Psychology > STUDY GUIDE > Nursing 402 PSYC | N3481 Final Exam Study Helps (All)
Nursing 402 PSYC | N3481 Final Exam Study Helps
Document Content and Description Below
1 N3481 Final Exam Study Helps • Compare and contrast individual and interpersonal factors influencing mental health, giving examples of each. o Stigma: a mark of shame, disgrace, or disapproval... that results in an individual being shunned or rejected by others § Self-stigma: type of stigma that occurs after individuals are publicly “marked” as being mentally ill § Public stigma: occurs after the individuals are publicly “marked” as being mentally ill. When individuals with mental illness act or say things that are odd or unusual or tell others that they have a mental illness, they are at risk of being publicly identified as having a mental illness and are subject to prejudice and discrimination • Being dangerous, unpredictable, and incapable of functioning independently § Label avoidance: avoiding treatment or care in order not to be labeled as being mentally ill • This is a reason so few people with mental health problems actually receive help § Cultural syndromes: cultural factors that represent a specific pattern of symptoms that occur within a specific cultural group or community • Ataque de nervios: frequent episodes of loss of control, uncontrollable crying, tremors, and severe anxiety and sadness with somatization symptoms including muscle and headache, nausea, loss of appeitite, insomnia, fatigue, and psychomotor agitation • Susto: fright characterized by symptoms of psychomotor agitation, anorexia, fever, diarrhea, confusion, apathy, depression, and introversion following an emotional trauma or witnessing a traumatic experience • Discuss the use of evidence-based care in making decisions about the care of your clients.\ o Evidence-based practice: the use of current best evidence in decision making; the search for and appraisal of the most relevant evidence to answer a clinical question – approach to the delivery of health care that integrates the best evidence from well-designed studies and patient care data and combines with it with patient preferences and values and nurse expertise § In an evidence-based approach, clinical questions are defined; evidence is discovered and analyzed; the research findings are applied in a practical manner and in collaboration with the patient; and outcomes are evaluated • Compare and contrast incidence, rate, prevalence and point prevalence giving examples of each. o Incidence: a rate that includes only new cases that have occurred within a clearly defined time period o Rate: the proportion of cases in the population when compared with the total population. § Rate = Cases in population / total population (cases and non-cases) o Prevalence: the total number of people who have the disorder within a given population at a specified time regardless of how long ago the disorder started o Point of prevalence: the basic measure that refers to the proportion of individuals in the population who have the disorder at a specified point in time. § This point can be a day on the calendar, such as April 1, 2012, or a point defined in relation to the study assessment, such as the day of the interview. It is also expressed as a fraction: • Point prevalence rate = Cases at t / Population at t • Compare and contrast mental disorders versus Mental health and give examples of each. o Mental health: the emotional and psychological well-being of an individual who has the capacity to interact with others, deal with ordinary stress, and perceive one’s surroundings realistically2 § Which the individual realizes his or her own abilities, can cope with life’s normal stresses, can work productively and fruitfully and can make a contribution to society o Mental disorders: health conditions characterized by alterations in thinking, mood, or behavior. They are associated with distress or impaired functioning § These include things like depression, bipolar 1 or 2, schizophrenia, etc. • Discuss the importance of epidemiology in understanding the effect of mental health disorders o Epidemiology: the study of patterns of disease distribution and determinants of health within populations § Contributes to the overall understanding of mental health status of population group, or aggregates, and associated factors / is important in understanding the distribution of mental illness and determinants of health within a given population • Discuss nonverbal communication and its implications with regards to behavior in various cultures. ???? o Nonverbal behavior varies from culture to culture. The nurse must, therefore, be careful to understand his or her own cultural context as well as that of the patient. For example, in some cultures, it is considered disrespectful to look a person straight in the eye. In other cultures, not looking a person in the eye may be interpreted as “hiding something” or as having low self-esteem. Whether one points with the finger, nose, or eyes and how much hand gesturing to use are other examples of nonverbal communication that may vary considerably among cultures. The nurse needs to be aware of cultural differences in communication in the context of each relationship and may need to consult with a cultural interpreter or use other learning opportunities to ensure that his or her communication is culturally congruent. § Nurses should use positive body language, such as sitting at the same eye level as the patient with a relaxed posture that projects interest and attention. Leaning slightly forward helps engage the patient. Generally, the nurse should not cross his or her arms or legs during therapeutic communication because such postures erect barriers to interaction. Uncrossed arms and legs project openness and a willingness to engage in conversation o Hispanic Americans § Tend to use all other resources before seeking help from mental health professionals – the reasoning behind this is unclear, but barriers for treatment include beliefs that mental health facilities do not accommodate their cultural needs (language, beliefs, values), cost of care, and concerns regarding immigration status. o African Americans § African Americans share many beliefs, attitudes, values, and behaviors, there are also many subcultural and individual differences based on social class, country of origin, occupation, religion, educational level, and geographical location. Many African Americans have extensive family networks in which members can be relied on for moral support, help with child rearing, provide financial aid, and help in crises. In many African American families, older members are treated with great respect – but African Americans with mental illness suffer from the stresses of double stigma – not only from their own cultural group but also from longtime racial discrimination. African Americans often have schizophrenia when compared to other groups. § A trusting, open, and collaborative therapeutic relationship during the diagnostic process is essential in order to conduct a meaningful assessment. o Asian Americans, Polynesians, and Pacific Islanders § Generally, Asian cultures have a tradition of denying or disguising the existence of mental illnesses. In many of these cultures, it is an embarrassment to have a family member treated for mental illness, which may explain the extremely low utilization of mental health services. § Asian Americans may experience a culture-bound syndrome, such as neurasthenia, which is characterized by fatigue, weakness, poor concentration,3 memory loss, irritability, aches/pains, and sleep disturbances. § Associated with the Korean culture, hwa-byung “suppressed anger syndrome” is characterized by subjective and expressed anger, sensations of eat, and feelings of gate. o Native Americans § Native American cultures emphasize respect and reverence for the earth and nature, from which come survival and comprehension of life and one’s relationships with a separate, higher spiritual being and with other human beings. Shamans, or medicine men, are central to most cultures. They are healers believed to possess psychic abilities. Healing treatments rely on herbal medicines and healing ceremonies with feasts. § In some tribes, mental illness is viewed as a supernatural possession, as being out of balance with nature. In certain groups, people with mental illness are stigmatized. However, this degree of stigmatization is not the same for all disorders – like suicide vs. mental/physical illnesses o Women of Minority Groups § Experience more conflicting feelings and psychological stressors than do men in trying to adjust to both their defined role in the culture and a different role in the larger predominant society. o Rural Cultures § Most mental health services are located in urban areas because most people live near these cities. Those living in rural areas have limited access to health care which leads to fewer people being diagnosed with a mental health problem. Even though rural residents are less likely than urban residents to suffer from mental health diagnoses or receive mental health care, the suicide rate is higher with firearms most commonly used. • Compare and contrast culture and ethnicity; define and give examples of each. o Culture: any group of people who identify or associate with each other on the basis of some common purpose, need, or similarity or background; the set of learned, socially transmitted beliefs, values, and behaviors that arise from interpersonal transactions among members of the cultural group § All cultural groups have sets of values, beliefs, and patterns of accepted behavior § Acculturation: is the term used to describe the socialization process by which minority groups learn and adopt selective aspects of the dominant culture § Cultural identity: set of cultural beliefs with which one looks for standards of behavior o Ethnicity: a person’s cultural background or where they came from § Nationality, regional culture, ancestry, and language – German, Spanish, Chinese ancestry • Compare, contrast and define autonomy, beneficence, non-maleficence, veracity, fidelity and justice and give examples of each. o Beneficence – the quality of doing good; can be described as charity o Autonomy – the clients right to make her own decisions. But the client must accept the consequences of those decisions. The client must also respect the decisions of others. o Non-maleficence – the duty to cause no harm, both individually and for all o Justice – fair and equal treatment for all o Fidelity – loyalty and faithfulness to the client and to one’s duty o Veracity – honesty when dealing with a client • Discuss HIPPA (the Health Insurance Portability and Accountability Act) confidentiality and protection/privacy of your patient’s health information in the inpatient mental health setting. o The Health Insurance Portability and Accountability Act of 1996 (HIPAA) provides legal protection in several areas of health care, including privacy and confidentiality. This act protects working Americans from losing existing health care coverage when changing jobs and increases opportunities for purchasing health care. It regulates the use and release of patient information, especially electronic transfer of health information.4 o HIPAA regulations require patient authorization for the release of information with the exception of that required for treatment, payment, and health care administrative operations. The release of information related to psychotherapy requires patient permission. § The underlying intent is to prevent the release of information to agencies not related to health care, such as employers, without the patient’s consent. When information is released, the patient must agree to the exact information that is being disclosed, the purpose of disclosure, the recipient of the information, and an expiration date for the disclosure of information • Compare and contrast the steps in the continuum of care giving example of each and identify how you would implement with your newly admitted client. o A continuum of care consists of an integrated system of settings, services, health care clinicians, and care levels, spanning illness-to-wellness states § The continuum facilitates the stability, continuity, and comprehensiveness of service to an individual and maximizes the coordination of care and services o The primary goal of the continuum of care is to provide treatment that allows patients to achieve the highest level of functioning in the least restrictive environment o Coordination of care is the integration of appropriate services so that individualized care is provided. Appropriated services are those that are tailored to address a client’s strengths and weaknesses, cultural context, service preferences, and recovery goals – including referral to community resources with others § Psychiatric–mental health nurses’ specific responsibilities vary according to the setting. In most settings, nurses function as members of a multidisciplinary team and assume responsibility for assessment and selection of level of care, education, evaluation of response to treatment, referral or transfer to a more appropriate level of care, and discharge planning. Discharge planning provides patients with all the resources they need to function effectively in the community and avoid re-hospitalization. • Discuss the focus of care for your client who has been admitted to an inpatient facility during a crisis. o During a crisis, the behaviors and verbalizations of a person may provide data that are indicative of mental illness. Nursing care should be prioritized according to the severity of responses. After the crisis has been resolved, assess whether the abnormal thoughts or feelings disappear. o The goal for people experiencing a crisis is to return to the pre-crisis level of functioning. The role of the nurse is to provide a framework of support systems that guide the patient through the crisis and facilitates development and use of positive coping skills. o Outcomes developed in cooperation with the person experiencing the crisis guide the evaluation. Once assessment data are clustered and prioritized the nursing diagnosis and the outcomes are determined. Once interventions are developed and implemented in cooperation with the individual in crisis, the person should come through the crisis with improved health, well-being, and social function. § Crisis intervention techniques involve listening for the emotional feeling message underlying the verbal message, especially when the patient presents as angry, hostile, and overwhelmed. The therapeutic alliance established with a patient is a dynamic, changeable interaction that may change between interactions. Thus, it must be constantly assessed and documented. The presence of the therapeutic alliance may be a protective factor, while the absence of a therapeutic alliance may be a risk factor for suicide. o THE GOAL IS TO RETURN THE CLIENT TO A PRE-CRISIS LEVEL o Crisis care requires an organized approach to treat individuals in crisis, including a mechanism for rapid access to care (within 24 hours), a referral for hospitalization, or access to outpatient services. o Crisis Intervention treatment – a specialized short-term, goal-directed therapy for those in acute distress – is brief, usually lasting fewer than 6 hours. This type of shirt-term care5 focuses on stabilization, symptom reduction, and prevention of relapse requiring inpatient services. § Patients in crisis demonstrate severe symptoms of acute mental illness, including labile mood swings, suicidal ideation, or self-injurious behaviors. Therefore, this treatment option commands a high degree of nursing expertise. Patients in crisis usually require medications such as anxiolytics or benzodiazepines for symptom management. Key nursing roles include assessment of short-term therapeutic interventions and medication administration. Nurses also facilitate referrals for admission to the hospital or for outpatient services. o Crisis Stabilization – is used when the immediate crisis does not resolve quickly. This type of care usually lasts fewer than 7 days. The primary purpose of stabilization is control of precipitating symptoms through medications, behavioral interventions, and coordination with other agencies for appropriate after-care. The major focus of nursing care in a short-term inpatient setting is symptom management. Ongoing assessment; short-term, focused interventions; and medication administration and monitoring of efficacy and side effects are main components. • Compare and contrast milieu therapy, biologic domain, psychological domain and social domains and give examples of each. o Milieu therapy”: an approach that provides a stable and coherent social organization to facilitate an individual’s treatment; often used interchangeably with therapeutic environment. The design of the physical surroundings, structure of patient activities, and promotion of a stable social structure and cultural setting enhance the setting’s therapeutic potential § Containment is the process of providing safety and security and involves the patient’s access to food and shelter § Validation is another process that affirms patient individuality § Structured interaction: which is purposeful interaction that allows patients to interact with others in a useful way (ex: daily community meetings) o The Biopsychosocial Model § Biologic Domain: The biologic domain consists of the biologic theories related to mental disorders and problems as well as all of the biologic activity related to other health problems. Biologic theories and concepts also relate to functional health patterns such as exercise, sleep, and adequate nutrition to mental health conditions. In addition, the neurobiologic theories also serve as a basis for understanding and administering pharmacologic agents § Psychological Domain: The psychological domain contains the theoretical basis of the psychological processes—thoughts, feelings, and behavior (intrapersonal dynamics) that influence one’s emotion, cognition, and behavior. The psychological and nursing sciences generate theories and research that are critical in understanding patients’ symptoms and responses to mental disorders. • Although there are neurobiologic changes in mental disorders, symptoms are psychological. For example, even though manic behavior is caused by dysfunction in the brain, there are no laboratory tests to confirm a diagnosis, only a pattern of behavior. § Social Domain: The social domain includes theories that account for the influence of social forces encompassing the patient, family, and community within cultural settings. Social and nursing sciences explain the connections within the family and communities that affect the mental health, treatment, and recovery of people with mental disorders. Psychiatric disorders are not caused by social factors, but their manifestations and treatment can be significantly affected by the society in which the patient lives. • Family support can actually improve treatment outcomes. Moreover, family factors, including origin, extended family, and other significant relationships, contribute to the total understanding and treatment of patients. Community forces, including cultural and ethnic groups within6 larger communities, shape the patient’s manifestation of disorders, response to treatment, and overall view of mental illness. o • Discuss the meaning of the concept of least restrictive environment and give examples. o Everything in regard to the incident or seclusion or restraint must be fully documented. If you suspect negligence or illegal activity on the part of a peer, carefully document the facts. o The psychiatric patient’s right to receive treatment and to have medical records kept confidential is protected under the Health Insurance Portability and Accountability Act (HIPPA). o Any discussion or consultation involving a patient should be conducted discreetly and only with individuals who have a need to know the information § The patient’s permission must be obtained to share information with persons who are not directly involved in his or her care o You cannot release information to a patient’s employer about the patient’s condition without the patient’s permission § You cannot divulge information after a person’s death that could not be shared before the patient died § In some states, direct care providers can warn a spouse if a partner tests HIV positive o Exceptions to confidentiality rule: § There is a duty to warn and protect third parties § Must notify Secret Service of threats against the President § Must report child and elder abuser o Patient’s Rights: § Right to vote § Right to enter into contractual agreement (contract) § Right to religious freedom and practice § Right to legal counsel § Right to be informed of research and right to refuse to participate § Right to send and receive mail and to be present for any inspection of packages received7 § Right to participate in planning treatment o Right to Refuse Treatment § A patient has the right to refuse treatment. You cannot administer psychotropic drugs without the patient’s informed consent • One can administer medications without the patient’s informed consent in two instances: o The patient’s behavior is out of control o A judge issues an order to administer medication without consent after a Medication Commitment hearing in Mental Health Court o Least Restrictive: the least drastic means be taken to achieve a specific purpose (a setting that provides the necessary care allowing the greatest personal freedom; more restrictive interventions should be used only after less restrictive interventions have been attempted to manage behavior and have been unsuccessful) § THINK SAFETY § De-escalating techniques are used first to try to talk to the patient and get him/her to calm down, if that doesn’t work, medication is used and if that doesn’t help much, restraints and seclusions are use but only if the patient is in danger to self or others. • Maintain the patient’s self-esteem and dignity, maintain calmness, assess the patient and situation, identify stressors and stress indicators, respond as early as possible, use a calm tone of voice, remain honest, be goal-oriented, give several options, be assertive. § When a patient is showing increased signs or symptoms of anxiety or agitation, it is perfectly appropriate to offer the patient a prn medication to alleviate symptoms. When used in conjunction with psychosocial interventions and deescalation techniques, this can prevent an aggressive or violent incident. During aggressive or violent incidents, HALOPERIDOL has historically been the most widely used antipsychotic, but with the introduction of IM 2nd generation antipsychotics, the use of olanzapine and ziprasidone has become more widespread-in part because of the severe side effects of haloperidol. A combination of antipsychotic (haloperidol or perphenazine) and a benzo (lorazepam) can be given IM. § Anger-control assistance: facilitation of the expression of anger in an adaptive, nonviolent manner; establish basic trust and rapport with patient, use calm, reassuring approach, determine appropriate behavioral expectations for expression of anger-given patient’s level of cognitive and physical functioning, limit access to frustrating situations until patient is able to express anger in an adaptive manner, encourage patient to seek assistance from nursing staff or responsible others during periods of increasing tension, monitor potential for inappropriate aggression and intervene before its expression, prevent physical harm if anger is directed at self or others, provide reassurance to patient that nursing staff will intervene to prevent patient from losing control, use external controls (physical or manual restraint, timeouts, and seclusions) as needed to calm patient who is expression anger in a maladaptive manner. • Compare and contrast unconditional positive regard, genuineness, empathetic understanding and self-actualization and give examples of each. o Genuineness means to be true, real, or authentic. When you’re discussing people, being genuine is about being sincere. § Genuineness also can be sincerity, honesty, integrity, and truthfulness. o Unconditional positive regard is a nonjudgmental caring for the client. In this therapy, the counselor’s attitude and nonverbal communication are crucial – emotional investment i.e., true caring in the client is also essential. o Empathetic Understanding – empathy is the ability to experience, in the present, a situation as another did at some point in the past; the ability to put oneself in another person’s circumstances and feelings.8 § For empathetic understanding to develop, there must be a giving of self to the other individual and a reciprocal desire to know each other personally. • Ex: “I know it’s not easy to lose weight because I myself have faced this problem.” o Self-Actualization is the realization or fulfillment of one’s talents and potentialities, especially considered as a drive or need present in everyone – growth of an individual toward fulfillment of the highest needs § The highest point in Maslow’s Hierarchy: • Compare and contrast psychoanalytic theory, behavioral theory, cognitive–behavioral theory, and client centered therapy and give examples of each. o Psychoanalytic Theory – Freud § The human mind is conceptualized in terms of conscious mental processes (an awareness of events, thoughts, and feelings with the ability to recall them) and unconscious mental processes (thoughts and feelings that are outside awareness and are not remembered) • Personality structure consists of three parts: the id, ego, and superego o The id is formed by unconscious desires, primitive instincts, and unstructured drives, including sexual and aggressive tendencies that arise from the body. o The ego consists of the sum of certain mental mechanisms, such as perception, memory, and motor control, as well as specific defense mechanisms (discussed below). The ego controls movement, perception, and contact with reality. The capacity to form mutually satisfying relationships is a fundamental function of the ego, which is not present at birth but is formed throughout the child’s development. o The superego is that part of the personality structure associated with ethics, standards, and self-criticism. § A child’s identification with important and esteemed people in early life, particularly parents, helps form the superego • Object relation is the psychological attachment to another person or object. For example: the child’s first love object is the mother, who is the source of nourishment and the provider of pleasure. As the child separates from the mother, the nature of this initial attachment influences future relationships. • Defense mechanisms are coping styles that protect a person from unwanted anxiety.9 • Psychoanalysis is the therapeutic process of accessing the unconscious conflicts that originate in childhood and then resolving the issues with a mature adult mild. Psychoanalysis attempts to reconstruct the personality by examining free associations (spontaneous, uncensored verbalizations of whatever comes to mind) and the interpretation of dreams. • Transference vs Countertransference: o Transference is when the client displaces feelings of another onto the nurse o Countertransference is when the nurse displaces feelings of another onto the client o Behavioral Theory § Attempt to explain how people learn and act. Behavioral theories never attempt to explain the cause of mental disorders; instead, they focus on normal human behavior. Two areas of behavioral theories are relevant to psychiatric nursing practice are stimulus-response theories and reinforcement theories. • Early-Stimulus Response Theories o Pavlovian Theory § Noticed that stomach secretions of dogs were stimulated by triggers other than food reaching the stomach. He found that the sight and smell of food triggered stomach secretions, and he became interested in this anticipatory secretion. Through his experiments, he was able to stimulate secretions with a variety of other laboratory non-physiologic stimuli. Thus, a clear connection was made between thought processes and physiologic responses. § In Pavlov’s model, there is an unconditioned stimulus (not dependent on previous training) that elicits an unconditioned (i.e., specific) response. In his experiments, meat is the unconditioned stimulus, and salivation is the unconditioned response. Pavlov taught the dog to associate a bell (conditioned stimulus) with the meat (unconditioned stimulus) by repeatedly ringing the bell before presenting the meat. Eventually, the dog salivated when he heard the bell. This phenomenon is called classical conditioning (or pavlovian conditioning) o John B Watson and the Behaviorist Revolution § Developed behaviorism – a learning theory that only focuses on objectively observable behaviors and discounts any independent activities of the mind. He developed two principles: frequency and recency • Frequency states that the more often a response is made to a stimulus, the more likely the response to that stimulus will be repeated • Recency states that the closer in time a response to a particular stimulus, the more likely the response will be repeated • Reinforcement Theories o Edward Thorndike § Found that animals gradually learn the correct response by “stamping in” the stimulus-response connection. Thorndike believed that reinforcement of positive behavior was important in learning – he was the first positive reinforcement theorist o B.F Skinner10 § Studied operant behavior or conditioning. In this type of learning, the focus is on the consequence of the behavioral response, not a specific stimulus. • If a behavior is reinforced or rewarded with success, praise, money, and so on, the behavior will probably be repeated. • If a behavior does not have a positive outcome, it is less likely that the behavior will be repeated. Nurses use this knowledge to create behavior management plans to reinforce healthy, positive behaviors. o Cognitive Theories § The initial behavioral studies focused on human actions without much attention to the internal thinking process. Cognitive theory includes the behavioral and the psychodynamic, attempted link internal thought processes with human behavior • Bandura’s Social Cognitive Theory o He developed his ideas after being concerned about television violence with children. He showed learning occurs by internalizing behaviors of others through a process of modeling – one person trying to be like another § He also developed self-efficacy – a person’s sense of his or her ability to deal effectively with the environment • The stronger the efficacy, the higher the goals people set for themselves and the firmer their commitment to them • Aaron Beck: Thinking and Feeling o Believed that people with depression have faulty informationprocessing systems that lead to biased cognitions. These faulty beliefs cause errors in judgment that become habitual errors in thinking. These individuals incorrectly interpret life situations, judge themselves too harshly, and jump to inaccurate negative conclusions. § A person may truly believe that he or she has no friends, and therefore no one cares. On examination, the evidence for the beliefs is based on the fact that there has been no contact with anyone because of moving from one city to another. Thus, a distorted belief is the basis of the cognition o Client-Centered Therapy – Rogers § Empathy is the capacity to assume the internal reference of the client in order to perceive the world the same way as the client, is used in the therapeutic process. The counselor is genuine but non-direct and also uses unconditional positive regard, a nonjudgmental caring for the client • In this therapy, the counselor’s attitude and nonverbal communication are crucial. The therapist’s emotional investment (true caring) in the client is essential in the therapeutic process • Discuss Peplau’s levels of anxiety and discuss how/when to best implement an education plan for your moderate to severely anxious client. o Hildegarde Peplau § Believed in the importance of the environment, defined as external factors considered essential to human development: cultural forces, presence of adults, secure economic status of the family, and a healthy prenatal environment. • Peplau emphasized the importance of empathic linkage: when one person feels an emotion (anxiety, panic, anger, disgust, envy) it can be communicated to others nonverbally and the emotion may be passed on.11 • Anxiety is a key concept for Peplau – according to her, anxiety is an energy that arises when expectations that are present are not met. o NOTE: Peplau’s model of anxiety continues to be an important concept in psychiatric nursing. Severe anxiety interferes with learning. Mild anxiety is useful for learning. § Levels of Anxiety: • Mild: awareness heightened • Moderate: awareness narrows • Severe: focused narrow awareness • Panic: unable to function • The self-system is another important concept in the model. Peplau defined the self as an anti-anxiety system and a product of socialization. The self-proceeds through personal development that is always open to revisions but tends toward stability. o Mild Anxiety – occurs in the normal experience of everyday living and allows an individual to perceive reality in sharp focus; YOU WANT TO TEACH DURING MILD ANXIETY § Sees, hears, and grasps more information § Problem solving becomes more effective § Physical symptoms may include slight discomfort, restlessness, irritability, or mild tension-relieving behaviors (nail biting, foot or finger tapping, fidgeting) o Moderate Anxiety – the perceptual field narrows, and some details are excluded from observation. § The person experiencing moderate anxiety sees, hears, and grasps less information and may demonstrate selective inattention, in which only certain things in the environment are seen or heard unless they are pointed out. § The ability to think clearly is hampered, but learning and problem solving can still take place although not at an optimal level. § Physical symptoms involve the sympathetic nervous system – tension, pounding heart, increased pulse, and respiratory rate, perspiration, and mild somatic symptoms (e.g., gastric discomfort, headache, urinary urgency. • Voice tremors and shaking may be noticed. § Mild or moderate anxiety levels CAN BE constructive because anxiety may be a signal that something in the person’s life needs attention is dangerous. o Severe Anxiety – the perceptual field of a person experiencing severe anxiety is greatly reduced. § A person with severe anxiety may focus on one particular detail or many scattered details and have difficulty noticing what is going on in the environment, even when another points out things. § Learning and problem solving are NOT POSSIBLE at this level, and the person may be dazed/confused. § Behavior at this level is automatic and aimed at reducing or relieving anxiety. § Physical symptoms: somatic symptoms (e.g., headache, nausea, dizziness, insomnia) often increase; trembling and a pounding heart are common and the person may experience hyperventilation and a sense of impending doom or dread. o Panic – is the most extreme level of anxiety and results in markedly disturbed behavior. § Someone in a state of panic is unable to process what is going on in the environment and may lose touch with reality. § The behavior that results may be manifested as pacing, running, shouting, screaming, or withdrawal. § Hallucinations, or false sensory perceptions (e.g., seeing people or objects not really there), may be experienced. Mild or moderate anxiety levels CAN BE constructive12 § Physical behavior may become erratic, uncoordinated, and impulsive. Automatic behaviors are used to reduce and relieve anxiety although such efforts may be ineffective. Acute panic may lead to exhaustion. • Identify, compare and contrast inhibitory versus excitatory neurotransmitters. o Dopamine (excitatory neurotransmitter) § Effect: involuntary muscle movement, stimulates reward pathways, influences emotion/judgment/insight, regulates attention, and impacts endocrine function • Decreased = Parkinson’s • Increased = Schizophrenia o Norepinephrine (excitatory neurotransmitter) § Effect: plays a role in memory/learning, has major role in sympathetic (fight or flight), major role in mood, and role in sleep/wake. • Decreased = depression and anxiety • Increased = mania o Serotonin (excitatory neurotransmitter) § Effect: involved with appetite, sleep, sex, and pain, major role in mood, and role in emotions/cognition • Decreased = depression and insomnia • Increased = mania o Acetylcholine (excitatory neurotransmitter) § Effect: plays role in memory/learning/emotions/cognitive function, has major role in autonomic system (primary cholinergic neurotransmitter; aids in communication for parasympathetic system) • Decreased = Alzheimer’s o GABA (inhibitory neurotransmitter) § Effect: plays a role in controlling anxiety/agitation • Decreased = seizures and anxiety o Glutamate (excitatory neurotransmitter) § Effect: plays a role in memory/learning • Increased = Alzheimer’s (chronic release of glutamate can lead to degeneration of neurons) • Compare and contrast the activities of the sympathetic versus the parasympathetic nervous system discussing the role each play in mental health and mental illness. o GAS: General Adaptation Syndrome consists of 3 stages o Sympathetic Nervous System: Alarm stage § Stage is initial, brief, and adaptive response to stressor (fight/flight) • Sympathetic: brain’s cortex and hypothalamus signal adrenals to release catecholamine adrenaline – increase sympathetic activity • Increase HR, RR, BP to enhance strength/speed; pupils dilate to broaden view on environment; blood shunts away from GI tract (dry mouth) and kidneys • Corticosteroids: hypothalamus sends message to adrenal cortex to produce corticosteroids to increase muscle endurance/stamina and reduce nonessential body functions o These inhibit 3 things: reproduction, growth and immunity • Endorphins: endorphins are released to reduce sensitivity to pain and injury-limit perception of pain § Decrease: salivary flow, arterioles, stomach motility and secretion, pancreas, intestinal motility, and bladder wall § Increase: pupil size, lacrimal glands, heart, bronchi, epinephrine o Parasympathetic Nervous System § Relaxation response – counteracts stress response by switching from SNS to PNS § Decrease: pupil size, lacrimal glands, heart, and bronchi § Increase: salivary flow, arterioles, stomach motility, pancreas, intestinal motility,13 bladder contraction o Impact on Stress § Acute Stress: uneasiness, concern, sadness, loss of appetite, immunosuppression, Increased metabolism, HTN, infertility, impotence, increased energy mobilization, decreased memory and learning, increased cardiovascular tone, increase risk of blood clots and stroke, increased cardiopulmonary tone § Chronic Stress: anxiety and panic attacks, depression or melancholia, anorexia/overeating, immunosuppression, insulin-resistant diabetes, amenorrhea, loss of libido, increased fatigue and irritability, increased risk for cardiac events, increased respiratory problems. • Which is a major differences between the atypical antipsychotics (such as clozapine) and the typical antipsychotics (such as haloperidol)? Typical (1st generation) • Used less in schizophrenia because of their minimal impact on negative symptoms and wide range of side effects. • Effective against positive symptoms • Cheaper in price than 2nd generation antipsychotics • Causes EPS • Divided into low or high potency categories: o Low potency = high sedation + high AcH + low EPS o High potency = low sedation + low AcH + high EPS • Adverse reactions including anticholinergic effects (dry mouth, urinary retention, constipation, blurred vision, photosensitivity, dry eyes, sexual dysfunction) and possible anticholinergic toxicity (dry mucous membranes, reduced or absent peristalsis, mydriasis, nonreactive pupils, hot/dry red skin, high fever without sweating, seizures) • Orthostatic hypotension • Sedation • Weight gain • In women-hyperprolactinemia • In men-gynecomastia • Compliance improves when EPS is minimized through dose lowering or in combination with other medications to relieve side effects such as: o Anti-parkinsonian drugs like: § Trihexyphenidyl (Artane) § Benztropine Mesylate (Cogentin) o Akathisia reducing: § Lorazepam o Others: § Diphenhydramine Hcl (Benadryl) Atypical (2nd/3rd generation) • Chosen as 1st line antipsychotics because they treat both positive and negative symptoms. • Produce minimal EPS effects – better side effects than typical antipsychotics • Clozapine causes agranulocytosis (cloza to death!) • Ziprasidone and Aripiprazole cause significant weight gain • May cause Metabolic syndrome which includes: o Weight gain (abdominal obesity) o Elevated BP o Altered glucose metabolism (elevated fasting glucose) o High serum triglycerides o Low HDL levels • There is increased risk of diabetes, hypertension, and atheroscleotic heart disease as a result of the above. • Aripiprazole (Abilify) is the ONLY 3rd generation drug. This drug: o Improves both positive and negative symptoms o Improves cognitive function o Is expensive o Produces little EPS or TDK o Has little AcH effect and does not appear to cause dysrhythmias • Since there are less EPS, Compliance is better than with 1st generation antipsychotics.14 § Amantadine Hcl (Symmetrel) • Compare, contrast, define and give examples of the following terms: transference; countertransference and boundary blurring, body space zones o Transference: patient unconsciously and inappropriately displaces onto nurse feelings and behaviors related to significant figures in patient’s past § Transference intensified in the relationships of authority o Countertransference: nurse displaces feelings related to people in nurse’s past onto patient § Patient’s transference to nurse often results in countertransference in nurse § Common signs of transference include a nurse over-identifying with the patient o Blurring of Boundaries: when relationships slip into social context; when nurse’s needs are met at the expense of patient’s needs o Body Space Zones: every individual is surrounded by four different body zones that provide varying degrees of protection against unwanted physical closeness during interactions. § 1. Intimate Zone: whispering and embracing • 15-46 cm / 6-18 in § 2. Personal Zone: close friends • 46cm-1.2m / 18-47 in § 3. Social Zone: acquaintances • 1.2-3.6m / 47in-3 yds § 4. Pubic Zone: interacting with strangers • >3.6m / >3 yds • Discuss the fundamental principles of therapeutic communication and the nurse’s role and focus in the therapeutic relationship. o Therapeutic communication is the ongoing process of interaction in which meaning emerges; may be verbal or non-verbal § Verbal communication – achieved by spoken words, includes the underlying emotion, context, and connotation of what is actually said § Non-verbal communication includes gestures, expressions, and body language. • Both the patient and the nurse use verbal and nonverbal communication15 o The nurse-patient relationship is a dynamic, time-limited interpersonal process that can be viewed in steps or phases with characteristic behaviors during each phase for the patient and the nurse § Self-awareness is the process of understanding one’s own beliefs, thoughts, motivations, biases, and limitations and recognizing how they affect others. Without self-awareness, nurses will find it impossible to establish and maintain therapeutic relationships with patients • Compare, contrast and discuss the concept of defense mechanisms, including their purpose and use. o Defense mechanisms are coping styles to help protect the individual against anxiety and creating awareness of internal or external dangers or stressors § Conversion occurs when cognitive tensions manifest themselves in physical symptoms (paralysis, blindness, deafness, becoming mute, and having a seizure) – man becoming deaf when wife tells him she wants a divorce § Projection occurs when one falsely attributes to another one’s own unacceptable feelings, impulses, or thoughts § Sublimation occurs when one channels potentially maladaptive feelings or impulses into socially acceptable behavior § Reframing consists of identifying and then disputing irrational or maladaptive thoughts § Denial is refusing to acknowledge some painful reality or subjective experience that would be apparent to others (psychotic denial used when there is gross impairment in reality testing). § Altruism: dealing with anxiety by reaching out to others § Suppression: voluntarily denying unpleasant thoughts and feelings § Repression: unconsciously putting unacceptable ideas, thoughts, and emotions out of awareness § Regression: sudden use of childlike or primitive behaviors that do not correlate with the person’s current developmental level § Displacement: shifting feelings related to an object, person, or situation to another less threatening object, person, or situation § Reaction formation: overcompensating or demonstrating the opposite behavior of what is felt § Undoing: performing an act to make up for prior behavior § Rationalization: creating reasonable and acceptable explanations for unacceptable behavior § Dissociation: creating a temporary compartmentalization or lack of connection between the person’s identity, memory, or how they perceive the environment § Compensation: emphasizing strengths to make up for weaknesses § Identification: conscious or unconscious assumption of the characteristics of another individual or group § Intellectualization: separation of emotions and logical facts when analyzing or coping with a situation or event § Splitting: demonstrating an inability to reconcile negative and positive attributes of self or others • Discuss therapeutic communication techniques to use in an initial assessment interview with your client who is seeking admission to the inpatient unit. o Therapeutic Communication Skills: § Acceptance: encouraging and receiving information in a nonjudgmental and interested manner. Used in establishing trust and developing empathy. § Confrontation: presenting the patient with a different reality of the situation. Used cautiously to immediately redefine the patient’s reality. However, it can alienate the patient if used inappropriately. A nonjudgmental attitude is critical for confrontation to be effective.16 § Doubt: expressing or voicing doubt when a patient relates a situation. Used carefully and only when the nurse feels confident about the details. It is used when the nurse wants to guide the patient toward other explanations. § Interpretation: putting into words what the patient is implying or feeling. Used in helping the patient identify underlying thoughts or feelings. § Observation: stating to the patient what the nurse is observing. Used when a patient’s behaviors (verbal or nonverbal) are obvious and unusual for that patient. § Open-ended statements: introducing an idea and letting the patient respond. Used when helping patient explore feelings or gain insight. § Reflection: redirecting the idea back to the patient for classification of important emotional overtones, feelings, and experiences; it gives patients permission to have feelings they may not realize they have. Used when patient is asking for the nurse’s approval or judgment; use of reflection helps nurse maintain a nonjudgmental approach. § Restatement: repeating the main idea expressed; lets patient know what was heard. Used when trying to clarify what the patient has said. § Silence: remaining quiet but nonverbally expressing interest during an interaction. Used when patient needs to express ideas but may not know quite how to do it; with silence, the patient can focus on putting thoughts together. § Validation: clarifying the nurse’s understanding of the situation. Used when nurse is trying to understand a situation the patient is trying to describe. o Non-Therapeutic Communication Skills: § Advice: telling a patient what to do. The nurse solves the patient’s problem, which may not be the appropriate solution and encourages dependency on the nurse. § Agreement: agreeing with a particular viewpoint of a patient. The patient is denied the opportunity to change his or her view now that the nurse agrees. § Challenges: disputing the patient’s beliefs with arguments, logical thinking, or direct order. The nurse belittles the patient and decreases the patient’s selfesteem. The patient will avoid relating to the nurse who challenges. § Reassurance: telling a patient that everything will be okay. The nurse makes a statement that may not be true. The patient is blocked from exploring his or her feelings. § Disapproval: judging the patient’s situation and behavior. The nurse belittles the patient. The patient will avoid the nurse. • Compare, contrast and give examples of components of the mental status exam including abstract reasoning, comprehension, affect, attention/concentration, mood/affect, thought content/process. o Level of Consciousness: described using the following terms, and observed behavior included in documentation § Alert: responsive and able to fully respond by opening her eyes and attending to a normal tone of voice and speech – answers questions spontaneously and appropriately § Lethargic: the client is able to open her eyes and respond but drowsy and falls asleep readily § Stuporous: requires vigorous or painful stimuli (pinching a tendon or rubbing the sternum) to elicit a brief response – may not be able to respond verbally § Comatose: the client is unconscious and does not respond to painful stimuli • May have abnormal posturing like… o Decorticate rigidity: flexion and internal rotation of upperextremity joints and legs o Decerebrate rigidity: neck and elbow extension, wrist and finger flexion o Physical Appearance: personal hygiene, grooming, and clothing choice § Expected findings include well-kempt, clean, and dressed appropriately for appearance17 o Behavior: voluntary and involuntary body movements § Mood: a client’s mood provides information about the emotion they’re feeling § Affect: a client’s affect is an objective expression of mood, such as a flat affect or a lack of facial expression o Cognitive and Intellectual abilities: Assess the client’s orientation to time, person, and place – assess the client’s memory – both recent and remote § Immediate: ask the client to repeat a series of numbers or a list of objects § Recent: ask the client to recall recent events, such as visitors from the current day, or the purpose of the current mental health appointment or admission § Remote: ask the client to state a fact from his past that is verifiable, like birth date or his mother’s maiden name • Assess the client’s level of knowledge like about their current illness/hospitalization • Assess the client’s ability to calculate – count backward from 100 • Assess client’s ability to think abstractly – like “a bird in the hand is worth two in the bush” • Assess client’s judgment – what would you do if there was a fire? • Assess the client’s rate and volume of speech – quality of his language • Discuss therapeutic communication techniques that enhance the effectiveness of an assessment interview giving examples of statements that reflect empathy. o Therapeutic Communication Skills: § Acceptance: encouraging and receiving information in a nonjudgmental and interested manner. Used in establishing trust and developing empathy. § Confrontation: presenting the patient with a different reality of the situation. Used cautiously to immediately redefine the patient’s reality. However, it can alienate the patient if used inappropriately. A nonjudgmental attitude is critical for confrontation to be effective. § Doubt: expressing or voicing doubt when a patient relates a situation. Used carefully and only when the nurse feels confident about the details. It is used when the nurse wants to guide the patient toward other explanations. § Interpretation: putting into words what the patient is implying or feeling. Used in helping the patient identify underlying thoughts or feelings. § Observation: stating to the patient what the nurse is observing. Used when a patient’s behaviors (verbal or nonverbal) are obvious and unusual for that patient. § Open-ended statements: introducing an idea and letting the patient respond. Used when helping patient explore feelings or gain insight. § Reflection: redirecting the idea back to the patient for classification of important emotional overtones, feelings, and experiences; it gives patients permission to have feelings they may not realize they have. Used when patient is asking for the nurse’s approval or judgment; use of reflection helps nurse maintain a nonjudgmental approach. § Restatement: repeating the main idea expressed; lets patient know what was heard. Used when trying to clarify what the patient has said. § Silence: remaining quiet but nonverbally expressing interest during an interaction. Used when patient needs to express ideas but may not know quite how to do it; with silence, the patient can focus on putting thoughts together. § Validation: clarifying the nurse’s understanding of the situation. Used when nurse is trying to understand a situation the patient is trying to describe. o Empathy is the ability to experience, in the present, a situation as another did at some point in the past; the ability to put oneself in another person’s circumstances and feelings. § For empathy to develop, there must be a giving of self to the other individual and a reciprocal desire to know each other personally. • Ex: “I know it’s not easy to lose weight because I myself have faced this problem.”18 • Compare and contrast benzo and nonbenzo antianxiety agents identifying best use and side/adverse effects. o Benzodiazepines – THINK LAM and PAM o Benzodiazepines are used to relieve anxiety (OCD, GAD, SAD, etc.) and treat insomnia § Alprazolam (Xanax) • Intermediate onset § Lorazepam (Ativan) • Slow-intermediate onset § Diazepam (Valium) • Very fast onset § Chlordiazepoxide (Librium) • Intermediate onset § Clonazepam (Klonopin) • Intermediate onset o Side Effects, Adverse Reactions, Toxicity § The most commonly reported side effects result from the sedative and CNS depression effects of these medications. Drowsiness, intellectual impairment, memory impairment, ataxia, and reduced motor coordination are common adverse reactions. • If used for sleep, long-acting benzodiazepines may cause a “hangover” effect § Individuals taking benzos should be instructed to not combine them with alcohol and to avoid driving or operating heavy machinery or other tasks that require mental alertness § Tolerance will most likely develop to these drugs and individuals who wish to experience the feeling of intoxication from these medications may be tempted to increase their own dosage • This leads to psychological dependence § Never stop benzos abruptly because it can cause recurrence of target symptoms like rebound insomnia or anxiety and can cause withdrawal symptoms: • Tremors, increased perspiration, palpitations, increased light sensitivity, abdominal discomfort, and rise in blood pressure. • These drugs should be tapered off slowly § Toxicity may develop in overdose or accumulation of the drug in the body from liver dysfunction. Symptoms include: • Worsening of the CNS depression, ataxia, confusion, delirium, agitation, hypotension, diminished reflexes, and lethargy. o Non-Benzodiazepines – just Buspirone o Useful in controlling symptoms of anxiety but has no effect on panic disorders and little on OCD – NOT ADDICTIVE!!*** § Effective for treating anxiety disorders without the CNS depressant effects or the potential for abuse and withdrawal syndromes § Buspirone • Very slow onset o Side Effects, Adverse Reactions, and Toxicity § Common side effects from buspirone include dizziness, drowsiness, nausea, excitement, and headache • Compare and contrast herbal supplements used in mental disorders identifying therapeutic use, side effect/adverse effects. o Herbal supplements popular for psychiatric disorders include: § St John’s Wort (SJW) • Used for depression, pain, anxiety, insomnia, and premenstrual syndrome19 • Said to modulate serotonin, dopamine, and norepinephrine – the risk for developing serotonin syndrome is increased with taking this with SSRIs/SNRIs § Kava • Used for anxiety reduction • Interacts with dopaminergic transmission • Said to carry risk for severe liver injury and can produce thrombocytopenia, leukopenia, and hearing impairment § Valerian • Used for insomnia and nervousness • Compare and contrast irrational beliefs and all-or-nothing thinking giving examples of each. o There are five themes common in irrational beliefs: § A demand: This MUST happen § Absolute thinking: all or nothing at all § Catastrophizing: exaggerating negative consequences of an event § Low frustration tolerance: everything should be easy § Global evaluations of human worth: people can be rated and some are better than others • Compare and contrast group norms, group cohesion, group think and group process giving examples of each. o A group develops norms which are rules and standards that establish acceptable behaviors. Some norms are formalized, such as beginning group on time, but others are never really formalized, such as sitting in the same place each session. § A member quickly learns the norms or is ostracized o Group behaviors can be challenging, frustrating, and problematic – overall group behaviors should support the integrity of the individual members and the group as a whole o Group cohesion: the ability of a group to stick together o Group think: the tendency of many groups to avoid conflict and adopt a normative pattern of thinking that is often consistent with the group leader’s ideas o Group process: the development and culmination of the session-to-session interactions of the members that move the group toward its goals. • Compare and contrast formal and informal roles of group members giving examples of each. o There are two official or formal group roles: the leader and the members § Leading a group involves many different functions, from obtaining and receiving information to testing and evaluating decisions. The leader should explain the rules of the group at the beginning of the group. • Leadership skills involve listening; tracking verbal and nonverbal behaviors; and maintaining a neutral, non-judgmental style o Informal group roles are positions with implicit rights and duties that can either help or hinder the groups process. § These roles are usually categorized according to purpose – task functions, maintenance functions, and individual roles. Members who assume task functions encourage the group members to stay focused on the groups task. Those who assume maintenance functions worry more about the group working together than the actual task itself. Individual roles can either enhance or detract from the work of the group. Individual roles are played by members to meet personal needs, such as feeling important or being an expert on a subject – these roles have nothing to do with the group’s purpose or cohesion – if individual roles predominate, the group may be ineffective. • Compare and contrast boundaries within the family system and give examples of each (rigid, diffuse, unclear, permeable). § Boundaries: are invisible barriers with varying permeabilities that surround each subsystem. They regulate the amount of contact a person has with others and protect the autonomy of the family and its subsystems. If family members do not20 take telephone calls at dinner, they are protecting themselves from outside intrusion. When parents do not allow children to interrupt them, they are establishing a boundary between themselves and their children. • The spouse subsystem must have a boundary that separates it from parents, children, and the outside world. A clear boundary between parent and child enables children to interact with their parents but excludes them from the spouse subsystem. • Boundaries vary from rigid to diffuse. If boundaries are too rigid and permit little contact from outside subsystems, disengagement results, and disengaged individuals are relatively isolated. o On the other hand, rigid boundaries permit independence, growth, and mastery within the subsystem, particularly if parents do not hover over their children. o Enmeshed subsystems result when boundaries are too diffuse. That is, when boundaries are too relaxed, parents may become too involved with their children, and the children learn to rely on the parents to make decisions, resulting in decreased independence. § If children see their parents as friends and treat them as they would their peers, then enmeshment exists. • Discuss the stages of the family life cycle giving examples of each stage. o Assessment of the family’s psychological domain focuses on the family’s developmental and life cycle, communication patterns, stress and coping abilities, and problem-solving skills. One aim of the assessment is to understand the relationships within the family. § The concept of family life cycle refers to stages that evolve based on significant events related to the arrival and departure of members, such as birth or adoption, child rearing, departure of children from home, occupational retirement, and death. Identifying the family life cycle is helpful in assessing family relationships, roles, and stresses § Transition times are the addition, subtraction, or change in status of family members. During transitions, family stresses are more likely to cause symptoms or dysfunction. Significant family events, such as the death of a member or the introduction of a new member, also affect the family’s ability to function. o Stages of the Family Life Cycle Family Life Cycle Stage Emotional Transition Required Family Changes Leaving home: emerging young adults Accepting emotional and financial responsibility for self Differentiation of self in relation to family of origin Development of intimate peer relationships Establishment of self in respect to work and financial independence Establishment of self in community and larger society Spirituality Joining of families through marriage or union Commitment to a new system Formation of partner systems Realignment of relationships with extended family, friends, and larger community to include new partners21 Families with young children Accepting new members into the system Adjustment of couple system to make space for children Collaboration in childrearing, financial, and housekeeping tasks Realignment of relationships with extended family to include parenting and grand-parenting roles Realignment of relationships with community and larger social system to include new family structure and relationships Families with adolescents Increasing flexibility of family boundaries to permit children’s independence and grandparents’ frailties Shift of parent–child relationships to permit adolescent to move into and out of system Refocus on midlife couple and career issues Begin shift toward caring for older generation Realignment with community and larger social system to include shifting family of emerging adolescent and parents in new formation pattern of relating Launching children and moving on at midlife Accepting a multitude of exits from and entries into the system Renegotiation of couple system as a dyad Development of adult-toadult relationships between parents and grown children Realignment of relationships to include inlaws and grandchildren Realignment of relationships with community and larger social system to include22 new structure and constellation of family relationships Exploration of new interests or career given the freedom from child care responsibilities Dealing with care needs, disabilities, and death of parents (grandparents) Families in late middle age Accepting the shifting generational roles Maintenance of own or couple functioning and interests in face of physiologic decline: exploration of new familial and social role options Supporting more central role of middle generations Realignment of system in relation to community and larger social system to acknowledge changed pattern of family relationships of this stage Making room in the system for the wisdom and experience of elders Supporting the older generation without overfunctioning for them Families nearing the end of life Accepting the realities of limitations and death and the completion of one cycle of life Dealing with loss of spouse, siblings, and other peers Making preparations for death and legacy Managing reversed roles in caretaking between middle and older generations Realignment of relationships with larger community and social system to acknowledge changing life-cycle relationships o23 • Discuss therapeutic approaches and protective factors that may help children who have been abused. o Children may need to learn a “violence vocabulary” that allows them to talk about their abuse and assign responsibility for abusive behavior. Children also need to learn that violence is not okay, and it is not their fault. Allowing children to discuss their abuse in the safety of a supportive, caring relationship may help alleviate anxiety and fear. o Reenacting the abuse through play is another technique that may be helpful in assisting children to express and work through their anxiety and fear. Play therapy uses dolls, human or animal figures, video games, or puppets to work though anxiety or fears. Other techniques include reading stories about recovery from abusive experiences (literal or metaphoric), using art or music to express feelings, and psychodrama. IN addition, teaching strategies to manage anxiety such as relaxation techniques, coping skills, and imagery, may give the child an added sense of mastering his or her fear. • Discuss children’s and adolescent’s responses to grief and loss based on developmental level. o Pre-School Aged § Limited ability to verbalize their feelings, they may need to express them through fantasy play and activities, such as mock funerals § As early as age 3 years, children have some concept of death. For example, the death of a goldfish provides an opportunity for the child to grasp the idea that the fish will never swim again. § Don’t tell child the person just fell asleep because they will fear sleeping o School Aged § Understand the permanence of death more clearly than do preschoolers, but they may still struggle to articulate their feelings § express their grief through somatic complaints, regression, behavior problems, withdrawal, and even anger toward their parents. § They may think that others expect them to cry and react with immediate emotional intensity to the death; when they do not react this way, they feel guilty o Adolescents § Piaget’s stage of formal operations, characterized by the ability to use abstract reasoning to conceptualize and solve problems, can better understand death as an abstract concept § Many teenagers become fascinated with morbid rock music, movies, and books. § Although they may be able to express their thoughts and feelings about death more clearly than younger children, they often are reluctant to do so for fear of being viewed as childish • Compare and contrast coping and adaptation giving examples of each. o Coping is a deliberate, planned, and psychological effort to maintain stressful demands. The coping process may inhibit or override the innate urge to act. Positive coping leads to adaptation, which is characterized by a balance between health and illness, a sense of well-being, and maximum social functioning. When a person does not cope well, maladaptations occur that can shift the balance toward illness, a diminished self-concept, and deterioration in social functioning. o There are two types of coping: § In problem-focused coping, the person attacks the source of stress and solves the problem (eliminating it or changing its effects), which changes the person– environment relationship. § In emotion-focused coping, the person reduces the stress by reinterpreting the situation to change its meaning o Adaptation is a person’s capacity to survive and flourish. Adaptation affects three important areas: health, psychological well-being, and social functioning § Health can be negatively affected by stress when coping is ineffective and the damaging condition or situation is not ameliorated or the emotional distress is not24 regulated. Examples of ineffective coping include using emotion-focused coping when a problem-focused approach is appropriate, such as if a woman reinterprets an abusive situation as her fault instead of getting help to remove herself from the environment. In addition, if a coping strategy violates cultural norms and lifestyle, stress is often exaggerated. Some coping strategies actually increase the risk for mortality and morbidity, such as the excessive use of alcohol, drugs, or tobacco. Many people use overeating, smoking, or drinking to reduce stress. They may feel better temporarily but are actually increasing their risk for illness. For people whose behaviors exacerbate their illnesses, learning new behaviors becomes important. Healthy coping strategies such as exercising and obtaining adequate sleep and nutrition contribute to stress reduction and the promotion of long-term health. § Psychological Well-Being: An ideal outcome to a stress response is feeling good about how stress is handled. Of course, outcome satisfaction for one person does not necessarily represent outcome satisfaction for another. For instance, suppose that two students receive the same passing score on an examination. One may feel a sense of relief, but the other may feel anxious because he appraises the score as too low. Understanding a person’s emotional response to an outcome is essential to analyzing its personal meaning. People who consistently have positive outcomes from stressful experiences are more likely to have positive self-esteem and self-confidence. Unsatisfactory outcomes from stressful experiences are associated with negative mood states, such as depression, anger, guilt leading to decreased self-esteem, and feelings of helplessness. Likewise, if the situation was appraised as challenging rather than harmful or threatening, increased self-confidence and a sense of well-being are likely to follow. If the situation was accurately appraised as harmful or threatening but viewed as manageable, the outcome may also be positive. § Social Functioning, the performance of daily activities within the context of interpersonal relations and family and community roles, can be seriously impaired during stressful episodes. For instance, a person who is experiencing the stress of a divorce may not be able to carry out job responsibilities satisfactorily. Social functioning continues to be impaired if the person views the outcome as unsuccessful and experiences negative emotions. If successful coping with a stressful encounter leads to a positive outcome, social functioning returns to normal or is improved. • Explain Walter Cannon’s fight-flight response including how triggered symptoms and how its related to the acute stress response. o The concept of homeostasis is the body’s tendency to resist physiological change and hold bodily functions relatively consistent, well-coordinated, and usualy stable § When the brain (amygdala and hippocampus) interprets an event as a threat, the hypothalamus and autonomic nervous system are signaled to secrete adrenaline, cortisol, and epinephrine. These hormones activate the sympathetic nervous system, physiological stability is challenged, and a “fight or flight” response occurs. Heart rate, blood pressure, and blood sugar increase. Energy is mobilized for survival. As the sympathetic system is activated, the parasympathetic is muted. After there is no longer a need for more energy and the threat is over, the body returns to a state of homeostasis o Chronic Stress and Kindling (Allostatic Load) § The role of an allostatic load or wear and tear on the body is thought to contribute to cognitive impairment, comorbidity, and eventual mortality of those with bipolar disorder. In this model, bipolar disorder is viewed as a disorder where the allostatic load increases as the number of mood episodes increases leading to an increase in physical and mental health problems. An interaction between stress and brain development is viewed as dynamic and individuals have different kinds of stress adaptation depending on their neurological responses.25 • The kindling theory posits that as genetically predisposed individuals experience repetitive, subthreshold stressors at vulnerable times, mood symptoms of increasing intensity and duration occur. Eventually a fullblown depressive or manic episode erupts. • Discuss and prioritize indicators of risk for and predictors of the potential for violence. o Neurologic Problems § Neurologic abnormalities are found in some persons who exhibit aggressive behavior. It is unclear how these abnormalities affect specific cognitive and affective processes, especially how they might be related to violence directed at partners, children, and older adults. Head injuries are associated with IPV as well as changes in personality, irritability, rage, and reduced impulse control – all of which may increase the risk of aggressive behaviors.26 o Alcohol and Other Drug Use § There is a strong association of AOD and IPV. The relationship between AOD use and IPV may be reciprocal and cyclical in nature. That is, AOD abuse increases the probability of perpetration and being the victim of violence which then increases the use of AOD to self-medicate emotional and physical sequelae of violence. AOD abuse plays a role in both perpetration of violence and in being a victim of violence. Women may be particularly vulnerable when under the influence of AOD. § The use of AODs increase the likelihood of IPV by disrupting thinking and interfering with processing social interactions. Distorted thinking contributes to developing paranoia, leading to impaired judgment. Crack, known to impair cognition and judgment, is often associated with violent subcultures, and the low social status of women in these cultures may give their partners a sense of entitlement to abuse them. Another explanation is that IPV leads to AOD use in attempt to self-medicate the pain associated with the violence. o Psychopathology § Three types of perpetrators have been identified according to their severity of violence, use of violence, and degree of psychopathology. The first group of family-only perpetrators engage in lower severity violent behaviors and exhibit the lowest levels of psychopathology. Next, those with borderline personality disorder characteristics or dysphoria engage in moderate to severe violence and demonstrate the highest levels of emotional volatility, dependency, and psychological distress. These perpetrators have a heightened sensitivity to emotional displays that predisposes them to interpret social situations as threatening and to respond with emotional dysregulation, verbal attacks, and physical violence. § Finally, the perpetrators who are generally violent and engage in moderate to severe violence, both inside and outside of the home, tend to meet criteria for antisocial personality disorder and are likely to have an extensive history of criminal behavior § Attachment styles are also used to explain violent behavior. According to attachment theory, the attachment avoidance style is characterized by pervasive discomfort with intimate closeness and a strong orientation toward being excessively self-reliant or socially withdrawn. Similar to those with antisocial personality disorder, they may be narcissistic, self-centered, and lack empathy for others, making them more prone to violence in intimate relationships. § An attachment anxiety style is characterized by low self-esteem, pervasive fears of partner rejection and abandonment, and either highly dependent or conflicted and disorganized relationship behaviors. Adults with anxious attachment who experience their partners as unavailable and have intense abandonment anxiety may respond with hostile, overt expressions of anger similar to those with borderline or dysphoric characteristics described above o Social Learning Theory (Intergenerational Transmission of Violence) § Violent families create an atmosphere of tension, fear, intimidation, and confusion about intimate relationships. Children in violent homes often learn that violent behavior is an approved and legitimate way to solve problems and to cope with difficulty. Social learning or intergenerational transmission of violence theory posits that children who witness or experience violence in their homes often perpetuate violent behavior. o Implicit Theories Held by Perpetrators § Are thoughts, core beliefs, or world views that support their offending behavior. Researchers have identified the following seven implicit theories held by male and female perpetrators: • (1) opposite sex is dangerous refers to emotions and beliefs that the opposite gender is deceitful, manipulative, controlling, and demanding; (2) general entitlement beliefs refer to beliefs that perpetrators consider27 themselves to be superior to others and that they are entitled to special privileges; (3) relationship entitlement beliefs are beliefs that one is superior to their partner and view their own needs as more important. Individuals with these beliefs expect their partners to behave according to their demands; (4) normalization of relationship violence is a belief that violence between partners is a normal and effective way of solving problems and dealing with undesired behavior of a partner. Additionally, individuals with this belief believe that the battered partner exaggerates the extent of the violence; (5) normalization of violence refers to beliefs that violence is acceptable, justifiable, and effective in solving conflicts and achieving personal goals, and controlling others outside of the intimate relationship; (6) it’s not my fault refers to beliefs that they deny responsibility for violence and attribute it to external factors such as alcohol and other drugs or attribute blame to the abused partner; (7) I am the man refers to stereotypical beliefs that men are superior to women in all aspects, that men are strong, dominant, authoritative, assertive, controlling, and aggressive and women are passive, dependent, and emotional • Identify neurotransmitters implicated in violent behaviors and aggressive behavior and identify indicators for violent behavior in your patient with anger control issues. o An aggression-related gene (monoamine oxidase A) which affects norepinephrine, serotonin, and dopamine, may play a significant role in the violence enacted by abused children § Low serotonin levels are also associated with irritability, increased pain sensitivity, impulsiveness, and aggression § Sex hormones also play a role in some aggressive behavior – make offenders have higher testosterone and female offenders act during the low progesterone phase of the menstrual cycle o Aggression assessment tools have been developed to assist in predicting violent behavior on inpatient psychiatric units. These tools can be beneficial but general risk identification includes the following: § A history of violence is the single best predictor of future violence § Patients who are delusional, hyperactive, impulsive, or predisposed to irritability are at a higher risk for violence. o Assess the patient for violence… § Does the patient have a wish or intent to harm? Does the patient have a plan? Does the patient have means able to carry out said plan? Does the patient match demographical risk factors such as male, 14-24, low socioeconomic status, inadequate support system, and prison time? • Define and provide examples of Traumatic Crisis; discuss expected nursing interventions for a patient experiencing a traumatic crisis § Traumatic (Adventitious) Crisis: a crisis initiated by unexpected, unusual events in which people face overwhelming hazards that entail injury, trauma, destruction, or sacrifice. May affect an individual or a multitude of people at once. • Things like natural disasters, national disasters, and crimes of violence. • May lead to psychological disorders needs crisis intervention, and debriefing28 • Discuss strategies and the goals and outcomes for crisis intervention address the immediate cause of the crisis, the definition of a crisis and restoration of emotional security and equilibrium. o During a crisis, the behaviors and verbalizations of a person may provide data that are indicative of mental illness. Nursing care should be prioritized according to the severity of responses. After the crisis has been resolved, assess whether the abnormal thoughts or feelings disappear. o The goal for people experiencing a crisis is to return to the pre-crisis level of functioning. The role of the nurse is to provide a framework of support systems that guide the patient through the crisis and facilitates development and use of positive coping skills. o Outcomes developed in cooperation with the person experiencing the crisis guide the evaluation. Once assessment data are clustered and prioritized the nursing diagnosis and the outcomes are determined. Once interventions are developed and implemented in cooperation with the individual in crisis, the person should come through the crisis with improved health, well-being, and social function. § Crisis intervention techniques involve listening for the emotional feeling message underlying the verbal message, especially when the patient presents as angry, hostile, and overwhelmed. The therapeutic alliance established with a patient is a dynamic, changeable interaction that may change between interactions. Thus, it must be constantly assessed and documented. The presence of the therapeutic alliance may be a protective factor, while the absence of a therapeutic alliance may be a risk factor for suicide. • Focus of crisis intervention: o 5 essential of mass trauma interventions that promotes o (1) sense of safety, (2) calming, (3) sense of self-efficacy and collective efficacy, (4) connectedness, and (5) hope o Goal of crisis intervention is to return the pt to at least precrisis level of functioning o Early intervention probably increases the chances for a good prognosis29 • Purpose of crisis debriefing o to assess the individual/family and the problem o More clearly the problem can be defined, more likely an effective solution can be identified o EX: what was happening in your life before you started to feel this way? • Importance of assessing coping mechanism o In order to evaluate the patient’s anxiety level & identifying the patient’s established patterns of coping o Common coping mechanism: overeating, drinking, smoking, seeking out to talk to someone, etc. o EX: what helped you thru difficult times in the past? • Discuss nursing management and risk assessment of a patient experiencing suicide ideation addressing degree of hopelessness, disorders, previous attempt, suicide planning and implementation, and availability and lethality of the suicide method. o Four main steps in preventing suicide and promoting long-term mental health: identification of those thinking about suicide (case finding), assessment to determine an imminent suicidal threat, intervening to change suicidal behavior associated with specific suicidal threat, and institution of effective interventions to prevent future episodes of suicidal behavior o Apply the assessment process that delineates the (1) intent to die, (2) severity of ideation, (3) availability of means, and (4) degree of planning § Questions to ask to ascertain suicidal ideation: • Have you ever tried to harm or kill yourself? • Do you have thoughts of suicide at this time? If yes, do you have a plan? If yes, can you tell me details about the plan? • Do you have the means to carry out this plan? • Have you made preparations for your death? (writing loved one’s notes, giving away possessions) • Has a significant episode in your life to cause you to think this way? • Compare and contrast lethality, parasuicide, suicidality and suicidal ideation giving examples of each. o Lethality: the probability that a person will successfully complete suicide; determined by the seriousness of the person’s intent and the likelihood that the planned method of death will succeed § Taking a bottle of pills vs. shooting oneself in the face with a gun/jumping off a bridge/jumping into traffic • A plan to use an accessible firearm to commit suicide has greather lethiality than a suicide plan that involves superficial cuts of the wrist o Parasuicide: deliberate, apparent attempt at suicide; commonly called a suicidal gesture, in which the aim is not death (taking a sublethal drug); also called parasuicidal behavior o Suicidality: all suicide-related behaviors and thoughts of completing or attempting suicide and suicide ideation o Suicidal ideation: thinking about and planning one’s own death without actually engaging in self-harm • Compare and contrast zyprexa and clozapine including therapeutic effects, side/adverse effects signs and important teaching for your client. o Both are antipsychotic medications that are indicated for schizophrenia, mania, and autism and to treat the symptoms of psychosis, such as hallucinations, delusions, bizarre behavior, disorganized thinking, and agitation. § These medications also reduce aggressiveness and inappropriate behavior associated with psychosis30 o Olanzapine (Zyprexa) O my goodness you’ll gain weight!! § Weight gain up to 20 lb within 1 year o Clozapine § Blood dyscrasias are rare but do occur with Clozapine • Agranulocytosis is an acute reaction that causes the individual’s white blood cell count to drop to very low levels, and concurrent neutropenia, a drop in total neutrophils in the blood, develops. • Weekly blood samples for the first 6 months of treatment and then every 2 weeks after that for as long as the drug is taken • Review the use of therapeutic communication during the assessment of your patient with Schizophrenia who is experiencing hallucinations, delusions, ideas of reference. o Hallucinations § Nurse should focus on understanding the patients experiences and responses § SAFETY MEASURES – specifically with suicidal or homicidal themes or commands § One-to-one supervision or transfer of the potential victim to another unit § The nurse should call the patient by name and speak simply and loudly enough to be understood amid the hallucinations and present in a non-threatening and supportive manner § Maintain eye contact and redirected the patient’s focus to your conversation as needed o Delusions § The nurse should attempt to see the world through the patient’s eyes § Acknowledge the patient’s experiences § Convey empathy § Avoid questioning the content of the delusion (aka FBI/Movie Star) § Label the patient’s feelings so they can be explored § Don’t focus too much on the material of the delusion § Do not debate with the patient or try to dissuade them from the delusion (HOWEVER – it is helpful to clarify misinterpretations of the environment and gently suggest a more reality-based perspective) § Engage patient in present activities and with people • Compare and contrast extrapyramidal side effects (EPS) pseudoparkinsons, dystonic reactions, akathisia and describe/identify best medications. Pseudoparkinsonism Symptoms: masklike facies, stiff and stooped posture, shuffling gait, drooling, tremor, “pill-rolling” Akinesia is associated with pseudoparkinsonism – it can be observed by the loss of spontaneous movements, such as the absence of the usual relaxed swing of the arms while walking. Onset: 5 hours - 30 days Nursing Interventions: - Administer prn antiparkinsonian agent (e.g., trihexyphenidyl (Artane) or benztropine (Cogentin)) - Towel or handkerchief for excess saliva. Teach how to reduce fall risk. Acute Dystonia Symptoms: acute contractions of tongue, face, neck, and back (usually tongue or jaw first), opisthotonos (tetanic heightening of entire body, head and belly up), oculogyric crisis (eyes locked upward/rolled into the back of the head), laryngeal dystonia Onset: 1 - 5 days Nursing Interventions: - Administer antiparkinsonian drugs like trihexyphenidyl (Artane) or benztropine (Cogentin) (IM for faster response) - Consider diphenhydramine hydrochloride (Benadryl) 25-50 mg IM/IV - Relief occurs usually in 5 - 15 minutes - Prevent further dystonia with antiparkinsonian drugs31 - Patient may fear choking; stay with patient and assist patient to understand what happened - Monitor airway Akathisia Symptoms: Motor inner-driven restlessness (tapping foot incessantly, rocking forward and backward in chair, shifting weight from side to side) Onset: 2 hours - 60 days Nursing Interventions: - Consider prescriber regarding possible medication change and give antiparkinsonian agent - Tolerance to akathisia does not develop, but akathisia usually subsides when antipsychotic is discontinued - Propranolol (Inderal), lorazepam (Ativan), or diazepam (Valium) may be used - May contribute to suicidality in severe cases so be aware. -Suicidal tendencies are due to the patient believing this is a permanent effect, not realizing it’s due to the medication. Tardive Dyskinesia Symptoms: Face: protruding and rolling tongue, blowing, smacking, licking, spastic facial distortion, smacking movements. Limbs: Choreic - rapid, purposeless, and irregular movements Athetoid - slow, complex, and serpentine movements Trunk: neck and shoulder movements, dramatic hip jerks and rocking, twisting pelvic thrusts Onset: Months to years Nursing Interventions: - No known treatment - Discontinuing drug rarely relieves symptoms - Nurses & doctors should screen for TD at least every 3 months - Onset may merit reconsideration of meds - Changes in appearance may lower self-esteem. Provide supports. - Teach patient actions to conceal involuntary movements (e.g., holding one hand with other) • Compare and contrast delusional disorder and schizoaffective disorder identifying best medications for each and what you would expect to expect to find in your clients diagnosed with these disorders. o Delusional Disorder is characterized by fixed, false delusions that could either occur in real life and are plausible in the context of the patient’s ethnic and cultural background or are completely implausible. These delusions may or may not interfere with an individual’s ability to function socially. Patients typically deny any psychiatric basis for their problem and refuse to seek psychiatric care. Patients whose delusions relate to somatic complaints are often seen in medical-surgical units of hospitals. Diagnosis otherwise is made only when patients act on the basis of their delusions and violate the law or social rules. § Delusional disorder is further classified as a particular subtype depending on the nature/content of patient’s delusions (erotomanic, grandiose, jealous, persecutory, somatic, mixed) • Erotomanic – that the patient is loved intensely by the loved object who is usually married, of a higher SES, or otherwise unattainable • Grandiose – have a great, unrecognized talent or have made an important discovery • Jealous – unfaithfulness or infidelity of a spouse or lover • Somatic – bodily functions or sensations • Persecutory – being conspired against, cheated, spied on, followed, poisoned, drugged, maliciously maligned, harassed, or obstructed32 • Mixed – no one delusional theme predominates – usually present with two or more types § Patient’s with delusional disorder usually do not experience functional difficulties or mental status impairment. Their thinking, orientation, affect, memory, perception, attention, and personality remain intact. § Sparse literature is available but antipsychotic agents are useful in improving acute symptoms by decreasing agitation and the intensity of the delusion o Schizoaffective Disorder (SAD) has symptoms typical of both schizophrenia and mood disorders but is a separate disorder. Although these patients experience mood problems most of the time, the diagnosis of SAD depends on the presence of positive symptoms (delusions/hallucinations) and mood symptoms at some time during the uninterrupted period of illness. § Many more mood responses and are very susceptible to suicide § To be diagnosed with SAD, a patient must have an uninterrupted period of illness when there is a major depressive, manic, or mixed episode along with two of the following symptoms of schizophrenia: delusions, hallucinations, disorganized speech, disorganized or catatonic behavior, or negative symptoms (e.g., diminished emotional expression, alogia, or avolition). In addition, the positive symptoms (delusions or hallucinations) must be present without the mood symptoms at some time during this period (for at least 2 weeks). • Two related subtypes of SAD have been identified: bipolar and depressive. In the bipolar type, the patient exhibits manic symptoms alone or a mix of manic and depressive symptoms. Patients with the depressive type display only symptoms of a major depressive episode § Atypical antipsychotic agents are generally prescribed because of their efficacy for psychosis and for their mood stabilizing properties. Clozapine, reported effective, can reduce risk for suicide and hospitalizations. • An antidepressant may be helpful if psychotic symptoms decrease but depressive symptoms still persist • Compare and contrast diagnostic criteria for depression including affect, vegetative signs, anhedonia, somatization, hopelessness, negative thinking and give examples of each and identify how you would address therapeutically. o Affect: an expression of mood manifest in a person’s outward emotional expression; varies considerably both within and among different cultures § Allow ample time for people who are depressed to answer questions and to respond to statements – it takes them a longer period of time to process what is being said o Vegetative signs: alterations in those activities necessary to support physical life and growth (eating, sleeping, elimination, sex) o Anhedonia: lack of interest in previously pleasurable activity; no pleasure o Somatization: experiencing multiple physical symptoms that are distressing and disruptive of daily life o Hopelessness: feelings of hopelessness/worthlessness; sometimes patients feel guilty. o Negative thinking: § Cognitive restructuring is a method of teaching the patient to restructure dysfunctional thought processes by defining and testing them. § The goal of cognitive reframing is to change the individual’s perceptions of stress by reassessing the situation and replacing irrational beliefs (“I can’t pass this course”) with more positive self-statements (“If I choose to study for this course, I will increase my chances of success”) • Cognitive distortions often include overgeneralizations (“He always…” or “I’ll never…) and “should” statements (“I should have done better” or “He shouldn’t have said that”.) • Create a teaching plan for your patient starting on an tricyclic antidepressant addressing symptoms they may experience from common side effects from this classification.33 TCAs – TRYPTYLINE & AMINE Medications Amitryptyline (Elavil), Nortrypriline (Pamelor), Imipramine (Tofranil), Clomipramine (Anafranil) Duration Inform the patient that TCAs may take several weeks for desired effects to take place (2 to 4 weeks) Neurotransmitters Block the reuptake of NE and serotonin at the presynaptic junction H1 receptor blockage = sedation AcH receptor blockage = anticholinergic effects Side Effects Hypotensive crisis, restlessness, weight gain, overdose is life-threatening, sedation, MI Anticholinergic Effects Dry mouth, difficulty voiding, dilated pupils, blurred vision, decreased GI motility, constipation Cardiac Effects Can cause cardiac toxicity: all patients should receive an ECG before and after treatment Therapeutic Effects Treat depression (however not first-line treatment due to side effect profile); reduction in seizures – helps with mood elevation Nursing Interventions/Teaching Patient and family should be informed that mood elevation may take 7 to 28 days. Family should reinforce this frequently to the depressed person because depressed people have trouble remembering and often respond to ongoing reassurance. If dose is missed, DO NOT double up, wait until next dose is due. Teach about side effects: drowsiness, dizziness, and hypotension. When taking, the patient should not operate heavy machinery. Instruct patient to take at bedtime. Abruptly stopping TCAs can cause nausea, altered heartbeat, and nightmares • Discuss important teaching regarding what to be aware of on initiation and when the medication reaches a therapeutic level for your client started on an antidepressant. o You should instruct your patient that many antidepressants take a couple weeks (2-4) before effects will be noticed § When patients have more energy and feel better they are more likely to commit suicide and follow through ?? • Compare and contrast Neuroleptic Malignant Syndrome with Agranulocytosis and discuss symptoms of each and best practice interventions and treatments. Neuroleptic Malignant Syndrome (NMS) Symptoms: Severe extrapyramidal - severe muscle rigidity, oculogyric crisis, dysphasia, flexor-extensor posturing, cogwheel-ing, decreased responsiveness. Hyperpyrexia is cardinal feature (temp over 103 F/39 C) Autonomic dysfunction - hypertension, tachycardia, diaphoresis, incontinence Agranulocytosis = CLOZAPINE Symptoms: Sore throat, fever, malaise, mouth sores, increased infections, and reduced WBC and neutrophil counts Onset: Usually during the first 12 weeks of antipsychotic therapy and occurs suddenly. After taking Clozapine.34 Delirium, stupor, & coma Onset: Can occur in first week of drug therapy but often occurs later and rapidly progressed over 2 to 3 days after initial manifestations. Risk factors: concomitant use of other psychotropics, older age, female gender (3:2), presence of mood disorder (40%), rapid dose titration Nursing Interventions: - Acute, life-threatening medical emergency - stop neuroleptic and transfer STAT to critical care unit - Bromocriptine (Parlodel) can relieve muscle rigidity and reduce fever - Dantrolene (Dantrium) may reduce muscle spasms - Cool body to reduce fever, maintain hydration, arrhythmias should be treated/ - Small doses of heparin may decrease possibility of pulmonary emboli. - Early detection increases survival chance. Nursing Interventions: - Potentially dangerous blood dyscrasia - Clozaril blood work usually done every week for 6 months then less frequently - Blood work may be ordered to determine leukopenia or agranulocytosis - If positive, drug discontinued and reverse isolation may be initiated - Morality high if drug is continued and treatment not initiated • Discuss the use of Lithium including therapeutic effects, side effects signs toxicity signs toxicity and important teaching for your client. o Mood stabilizers are primarily used for stabilization of mood swings particularly those of mania in bipolar disorders. Lithium is the oldest and the gold standard drug for treatment. § Lithium 0.4 to 1 mEq/L • Indications and MOA o Lithium is indicated for symptoms of mania characterized by rapid speech, flight of ideas (topic to topic), irritability, grandiose thinking, impulsiveness, and agitation. Lithium is used to treat depressive episodes of bipolar illness. o The exact MOA of Lithium isn’t know but it is thought to exert multiple neurotransmitter effects including enhancing serotonergic transmission, increasing synthesis of norepinephrine, and blocking postsynaptic dopamine. § It replaces sodium in the sodium-potassium pump and is retained more readily than sodium inside the cells § Lithium leads to increased storage of catecholamine’s within the cell, reduced dopamine neurotransmission, increased norepinephrine reuptake, increased GABA activity, and increased serotonin receptor sensitivity. • In conditions that cause sodium depletion, such as dehydration caused by fever, strenuous exercise, hot weather, increased perspiration, and vomiting, the kidneys attempt to conserve sodium – lithium is a salt so the kidneys hold on to it which leads to increased blood levels and potential toxicity35 • Side Effects, Adverse Reactions, and Toxicity o Side Effects: excessive thirst, increased frequency of urination, fine head tremor, drowsiness, and mild diarrhea o Toxicity: § Early signs of toxicity include severe diarrhea, vomiting, drowsiness, muscular weakness, and lack of coordination. § Comply with the requirements to have blood levels checked twice a week initially and every 2 months after achieving therapeutic levels. Mania poses a risk for dehydration, which can worsen with the use of lithium. Drink adequate fluids to maintain fluid balance. § Adherence to medication should be very important until instructured otherwise by physician. Plasma Level Side Effects/Symptoms of Toxicity <1.5 mEq/L Mild Side Effects Metallic taste in mouth, Fine hand tremor (resting), Nausea, Polyuria, Polydipsia, Diarrhea or loose stools, Muscular weakness or fatigue, Weight gain, Edema, Memory impairments 1.5-2.5 mEq/L Moderate toxicity Severe diarrhea, Dry mouth, Nausea and vomiting, Mild to moderate ataxia, Incoordination, Dizziness, sluggishness, giddiness, vertigo, Slurred speech, Tinnitus, Blurred vision, Increasing tremor, Muscle irritability or twitching, Asymmetric deep tendon reflexes, Increased muscle tone >2.5 mEq/L Severe toxicity Cardiac arrhythmias, Blackouts, Nystagmus, Coarse tremor, Fasciculation’s, Visual or tactile hallucinations, Oliguria, renal failure, Peripheral vascular collapse, Confusion, Seizures, Coma and death THERAPEUTIC EFFECTS: Therapeutic effects: Antimanic. • Can be given for anger control issues but not for acute anger (takes a long time to workantipsychotic IM). • First-line approach for treatment-resistant depression! • May balance biogenic amines of norepeniphrine, serotonin in CNS areas involved in emotional responses. • Decrease elation and mania. Mood stabilizer. SIDE EFFECTS OF LITHIUM Side effects: • increased urine output (polyuria) and thirst, headache, drowsy/dizzy, tremors, twitching, ataxia, • seizures, memory loss, clonic movements, fatigue, hypotension, ECG changes, • dysrhythmias, • circulatory Collapse, edema, tinnitus, blurred vision, goiter, hyperglycemia, hypo/hyperthyroidism, dry Ways to minimize side effects: • take with food to reduce GI upset! • Monitor lithium and sodium levels, blood pressure, thyroid levels, renal function and BMI (linked to metabolic syndrome). • Adequate fluids (2-3 L/day). • Avoid use with St. Johns wort, kava, and black/green tea. • Don’t change salt intake.36 mouth, anorexia, N/V, diarrhea, incontinence, leukocytosis, alopecia, rash, and muscle weakness. Dietary factors: LITHIUM • Eating too much salt can decrease effectiveness of lithium. • Lithium decreases reabsorption of sodium in kidneys and kidneys hold onto lithium when sodium levels are low (dehydration, low intake, diarrhea) which can cause toxicity • -DO NOT CHANGE YOUR SALT INTAKE (maintain it)!!!!! • Drink plenty of fluids (FVD= lithium ^ = toxicity). Adverse effects: • Long-term effects include hypothyroidism and decreased kidney concentrating ability (have kidneys and thyroid checked periodically). • Older adults should “start low and go slow” because of dec. kidney function up to 50%. • BAD FOR KIDNEYS- do not give to pt. w/ kidney problems. Toxic effects (how to address initial toxic effects): • Early mild toxicity= nausea/vomiting, diarrhea, poor coordination, FINE motor tremors, and muscle weakness, thirst, polyuria. • Advanced severe toxicity= COARSE hand tremors, severe thirst, tinnitus, muscular hyper agitation, severe hypotension (coma?), cardiac arrhythmia, diluted urine. NO ANTIDOTE FOR LITHIUM • -hemodialysis, induce emesis, or take substances to inc. rate of lithium excretion may be needed if toxicity occurs. • Toxicity also with: • diuretics, • NSAIDS (aspirin), • losartan, and • carbamezapine. • Diureticts and • antiHTN meds can lead to FVD can lead to toxicity! • Inc. neurotoxicty w/ haloperidol and thioridazine. • Beta-blockers used for tremor can mask toxicity Initial toxic effects: • similar to “early mild toxicity” (thirst, polyuria, weight gain, and tremor) tell patient to expect these when they first start the medicine but WILL GO AWAY W/IN 10 DAYS>IF it comes back later this is an EMERGENCY> • toxicity that can cause coma/death. Therapeutic index: • Narrow therapeutic range 0.5-1.5 mEq/L • blood levels must be monitored frequently at first, • then every 3 months. • 1.5 mEq = toxicity starts.37 • Discuss the use of Lamictal including therapeutic effects, side effects, signs toxicity and important teaching for your client. o Lamictal belongs to the group of anticonvulsants which are commonly used to treat individuals who have bipolar disorders, mania, or mixed episodes and are considered mood stabilizers § Patients should be taught about potential drug interactions, especially with herbal supplements. Oral contraceptives may become ineffective and female patients should be advised to use other forms of birth control § A benign skin rash, blurred or double vision, dizziness, nausea, vomiting, and other GI symptoms are side effects o Lamictal or Lamotrigine can produce a life-threatening side effect called Steven Johnson’s Syndrome (SJS) § This is usually within 2-8 weeks and has the highest risk in children • Immediately discontinue if a rash is noted and seek out healthcare provider immediately • Compare and contrast conversion, projection, sublimation and reframing giving examples of each. o Conversion occurs when cognitive tensions manifest themselves in physical symptoms (paralysis, blindness, deafness, becoming mute, and having a seizure) – man becoming deaf when wife tells him she wants a divorce o Projection occurs when one falsely attributes to another one’s own unacceptable feelings, impulses, or thoughts o Sublimation occurs when one channels potentially maladaptive feelings or impulses into socially acceptable behavior o Reframing consists of identifying and then disputing irrational or maladaptive thoughts • Compare and contrast benzodiazepines and non-benzodiazepines, discussing which are better for short term use and which one is better for long term use and why. o Benzodiazepines: LAMs and PAMs § Alprazolam (Xanax), Chlordiazepoxide (Librium), Clonazepam (Klonopin), Clorazepate (Tranxene), Diazepam (Valium), Lorazepam (Ativan), Oxazepam (Serax), & Halazepam (Paxipam) o Non-Benzodiazepines § Buspirone • LONG ACTING*** ONLY LONG ACTING REALLY • Compare, contrast and define patient behaviors/nursing interventions for patients diagnosed with personality disorders including: manipulation; limit setting; splitting; and discuss the importance of consistency. o Manipulation: try to prevent or reduce manipulation (flattery, seductiveness, instilling of guilt) by setting clear and realistic limits on specific behavior. Ensure that limits are adhered to by all staff. § Be aware that antisocial patients can instill guilt when they are not getting what they want; they will try to change behavior or perception of the nurse for their own gain – guard against being manipulated. o Limit Setting: establishing parameters of desirable and acceptable patient behavior § Discuss concerns about behaviors with patients and identify undesirable patient behavior. o Splitting: refers to the inability to view both positive and negative aspects of others as part of a whole. This results in viewing someone as either a wonderful person or a horrible person. This kind of dichotomous thinking and coping behavior is believed to be partially as a result of the person’s failed experiences with adult personality integration and likely is influenced by exposure to earlier psychological, sexual, or physical trauma. o Consistency: it’s just important obviously • Discuss the etiology and diagnostic characteristics of borderline personality.38 o Borderline Personality Disorder is characterized by a disruptive pattern of instability related to self-identity, interpersonal relationships, and affects combined with marked impulsivity and destructive behavior. o People with BPD have an extreme fear of abandonment as well as a history of unstable, insecure attachments. Most never experienced a consistently secure, nurturing relationship and are constantly seeking reassurance and validation. They often idealize others and establish intense relationships that violate others’ interpersonal boundaries, which lead to rejection. o These people are intensely emotional and have a poor sense of self, feel estranged from others and inadequate in the face of perceived social standards. § These feelings often result in self-injurious behaviors such as wrist cutting, selfburnings, or head banging. o In social situations, people with BPD use elaborate strategies to structure interactions. They restrict their relationships to ones in which they feel in control. They distance themselves from groups when feeling anxious (which is most of the time) and rarely use their social support system. They do not want to burden anyone; they fear rejection and assume people are tired of hearing them repeat the same issue. o Impulsivity is a characteristic of people with BPD. Because impulsive-driven people have difficulty delaying gratification or thinking through the consequences before acting on their feelings, their actions are often unpredictable. Gambling, spending money, binge eating, engaging in unsafe sex, abusing substances are all common of these individuals. They can also be physically/verbally aggressive. o The turmoil and unsuccessful interpersonal relationships and social experiences associated with BPD may lead the person to undermine him or herself when a goal is about to be reached. The most serious consequences are a suicide attempt or parasuicidal behavior (deliberate self-injury with intent to harm oneself). o Can be compulsive like hair pulling, episodic or repetitive like cutting oneself, and is more likely to occur when the individual with BPD is depressed; has highly unstable relationships; and is paranoid, hypervigilant, and resentful. • Compare and contrast the main characteristics of each the following personality disorders: avoidant, dependent, antisocial, narcissistic, histrionic, obsessivecompulsive, schizoid, schizotypal, paranoid, and borderline personality. Cluster A – Odd, Eccentric Cluster Involves personality disorders that portray social awkwardness and social withdrawal Cluster B – Dramatic, Overly Emotional Cluster Unpredictable behaviors and thinking are included – very dramatic and overdone Cluster C – Anxious, Fearful Cluster High levels of anxiety Paranoid, Schizoid, Schizotypal Antisocial, Borderline, Histrionic, Narcissistic Avoidant, Dependent, Obsessive-Compulsive o Antisocial Personality Disorder § Individuals are arrogant and self-centered and feel privileged and entitled. They are self-serving and they exploit and seek power over others. They can be interpersonally engaging and charming, which is often mistaken for a genuine sense of concern for other people. § They lack empathy; are unable to express human compassion; and tend to be insensitive, callous, and contemptuous of others. Deceit and manipulation for personal profit or pleasure are central features associated with this disorder. They are behaviorally impulsive and interpersonally irresponsible. • Many with this disorder perform acts that are grounds for arrest: destroying property, harassing others, or stealing/pursuing other illegal occupations.39 § they act hastily and spontaneously, are temperamentally aggressive and shortsighted; and fail to plan ahead or consider alternatives. § Associated Findings include: lacking empathy; callous, cynical, and contemptuous of the feelings, rights, and suffering of others; inflated and arrogant self-appraisal; excessively opinionated, self-assured, or cocky; glib, superficial charm; irresponsible and exploitative in sexual relationships; dysphoria – complaints of tension, inability to tolerate boredom, and depressed mood o Narcissistic Personality Disorder § Are grandiose, have an inexhaustible need for admiration, and lack empathy. Beginning in childhood, these individuals believe that they are superior, special, or unique and that others should recognize them in this way. They are often preoccupied with fantasies of unlimited success, power, beauty, or ideal love. They overvalue their personal worth, direct their affections toward themselves, and expect others to hold them in high esteem. They define the world through their own self-centered view. Their sense of entitlement is striking. People with narcissistic personality disorder are benignly arrogant and feel themselves above the conventions of their cultural group. They handle criticism poorly and may become enraged if someone dares to criticize them or else they may appear totally indifferent to criticism. They believe they are entitled to be served and that it is their inalienable right to receive special considerations. People with this disorder want to have their own way and are frequently ambitious to achieve fame and fortune. These individuals are often successful in their jobs but may alienate their significant others, who grow tired of their narcissism. They cannot show empathy, and they feign sympathy only for their own benefit to achieve their selfish ends. • Believed to be caused by parent overindulgence and overvaluation. o Histrionic Personality Disorder § “Attention seeking,” “excitable,” and “emotional” describe people with histrionic personality disorder. These individuals are lively and dramatic and draw attention to themselves by their enthusiasm, dress, and apparent openness. They are the “life of the party” and, on the surface, seem interested in others. Their insatiable need for attention and approval quickly becomes obvious. • There are two main ways their need to be “center stage” is exhibited: (1) their interests and topics of conversation focus on their own desires and activities, and (2) their behavior, including their speech, continually calls attention to themselves. § These needs are inflexible and persistent even after others attempt to meet them. Persons with histrionic personality disorders are quick to form new friendships and just as quick to become demanding. Because they are trusting and easily influenced by other opinions, their behavior often appears inconsistent. Their strong dependency need makes them overly trusting and gullible. They are moody and often experience a sense of helplessness when others are disinterested in them. They are sexually seductive in their attempts to gain attention and often are uncomfortable within a single relationship. Their appearance is provocative and their speech dramatic. They express strong opinions without supporting facts. Loyalty and fidelity are lacking • Gender Specific: Women dress seductively, may express dependency on selected men, and may “play” a submissive role. Men may dress in a very masculine manner and seek attention by bragging about athletic skills or successes in their jobs. Individuals with this disorder have difficulty achieving any true intimacy in interpersonal relationships. They seem to possess an innate sensitivity to the moods and thoughts of those they wish to please. This hyper-alertness enables them to maneuver quickly to gain their attention. Then they attempt to control relationships by their seductiveness at one level but become extremely40 dependent on their friends at another level. Their demand for constant attention quickly alienates their friends. o Paranoid Personality Disorder § Characterized by a long-standing suspiciousness and mistrust of persons in general. Individuals with these traits refuse to assume personal responsibility for their own feelings, assign responsibility to others, and avoid relationships in which they are not in control or lose power. These individuals are suspicious, guarded, and hostile. They are consistently mistrustful of others’ motives, even relatives and close friends. Actions of others are often misinterpreted as deception, deprecation, and betrayal, especially regarding loyalty or trustworthiness of friends and associate § People with paranoid personality disorder are unforgiving and hold grudges; their typical emotional responses are anger and hostility. They distance themselves from others and are outwardly argumentative and abrasive; internally, they feel powerlessness, fearful, and vulnerable. Other hallmark features of paranoid personality disorder are persistent ideas of self-importance and the tendency to be rigid and controlled. Blind to their own unattractive behaviors and characteristics, they often attribute these traits to others. Their outward demeanor often seems cold, sullen, and humorless. They want to appear controlled and objective, yet often they react emotionally, displaying signs of nervousness, anger, envy, and jealousy. Orderly by nature, they are hypervigilant to any environmental changes that may loosen their control on the world. o Schizoid Personality Disorder § Characterized as being impassive and interpersonally unengaged. They tend to be unable to experience the joyful and pleasurable aspects of life. They are introverted and reclusive and clinically appear distant, aloof, apathetic, and emotionally detached. Typically, lifelong loners, they have difficulty making friends, seem uninterested in social activities, and appear to gain little satisfaction in personal relationships. In fact, they appear to be incapable of forming social relationships. • Their interests are directed at objects, things, and abstractions. They may do well at solitary jobs other people might find difficulty to tolerate. Often people with schizoid personality disorders may daydream excessively and become attached to animals, and they frequently do not marry or even form long-lasting romantic relationships. As children, they engage primarily in solitary activities, such as stamp collecting, computer games, electronic equipment, or academic pursuits such as mathematics or engineering. In addition, they seem to have a cognitive deficit characterized by obscure thought processes, particularly about social matters. § Communication with others is confused and lacks focus. These individuals reveal minimum introspection and self-awareness, and interpersonal experiences are described in a very mechanical way. o Schizotypal Personality Disorder § Characterized by a pattern of social and interpersonal deficits. The term schizotypy refers to traits that are similar to the symptoms of schizophrenia but are less severe. Cognitive perceptual symptoms are a primary characteristic and include magical beliefs (similar to delusions) and perceptual aberrations (similar to hallucinations). Other common symptoms include referential thinking (interpreting insignificant events as personally relevant) and paranoia (suspicious of others). § Schizotypal personality disordered persons are more dramatically eccentric than those with schizoid personality disorder who are characteristically flat, colorless,41 and dull. These individuals are perceived as strikingly odd or strange in appearance and behavior, even to laypersons. They may have unusual mannerisms, an unkempt manner of dress that does not quite “fit together,” and inattention to usual social conventions (e.g., avoiding eye contact, wearing clothes that are stained or ill fitting, and being unable to join in the give-and-take banter of coworkers). Void of any close friends other than first-degree relatives, their mood is constricted or inappropriate, with excessive social anxieties. They usually exhibit an avoidant behavior pattern. § Persons with schizotypal personality disorder can respond to stress with transient psychotic episodes (lasting minutes to hours). Because of their short duration, the symptoms mirror but fall short of features that would justify the diagnosis of schizophrenia. Many individuals (30% to 50%) with schizotypal personality disorder also have a co-occurring major depressive disorder diagnosis when admitted to a hospital). Schizotypal personality disorders may be slightly more common in males. o Avoidant Personality Disorder § Characterized by avoiding social situations in which there is interpersonal contact with others. Individuals appear timid, shy, and hesitant, and they fear criticism and feel inadequate. These individuals are extremely sensitive to negative comments and disapproval and appraise situations more negatively than others do. The behavior becomes problematic when they restrict their social activities and work opportunities because of their extreme fear of rejection. § In childhood, they are shy, but instead of growing out of the shyness, it becomes worse in adulthood. They perceive themselves as socially inept, inadequate, and inferior, which in turn justifies their isolation and rejection by others. Vocationally, people with avoidant personality disorder often take jobs on the sidelines, rarely obtaining personal advancement or exercising much authority, but to employers, they seem shy and eager to please. They are reluctant to enter relationships unless they are given strong assurance of uncritical acceptances, so they consequently often have no close friends or confidants o Dependent Personality Disorder § Cling to others in a desperate attempt to keep them close. Their need to be taken care of is so great that it leads to doing anything to maintain the closeness, including total submission and disregard for themselves. § Decision making is difficult or nil. They adapt their behavior to please those to whom they are attached. They lean on others to guide their lives. They ingratiate themselves to others and denigrate themselves and their accomplishments. Their self-esteem is determined by others. Behaviorally, they withdraw from adult responsibilities by acting helpless and seeking nurturance from others. In interpersonal relationships, they need excessive advice and reassurance. They are compliant, conciliatory, and placating. They rarely disagree with others and are easily persuaded. Friends describe them as gullible. They are warm, tender, and noncompetitive. They timidly avoid social tension and interpersonal conflicts.42 However, these individuals are at risk for suicide and parasuicide, perpetration of child abuse, perpetration of domestic violence (in men), and victimization by a partner (in women). o Obsessive-Compulsive PERSONALITY Disorder § Stands out because it bears close resemblance to obsessive-compulsive disorder (OCD), and is closely related to anxiety disorder. Although these disorders have similar names, the clinical manifestations are quite different. • A distinguishing difference is that those with the OCD tend to use obsessive thoughts and compulsions when anxious but less so when anxiety decreases. o Persons with OCPD do not demonstrate obsessions and compulsions but rather a pervasive pattern of preoccupation with orderliness, perfectionism, and control. They also have the capacity to delay rewards; whereas those with OCD do not. § Individuals with this disorder attempt to maintain control by careful attention to rules, trivial details, procedures, and lists. They may be completely devoted to work, which typically has a rigid character, such as maintaining financial records or tracking inventory. They are uncomfortable with unstructured leisure time, especially vacations. Their leisure activities are likely to be formalized (season tickets to sports, organized tour groups). Hobbies are approached seriously. § Behaviorally, individuals with OCPD are perfectionists, maintaining a regulated, highly structured, strictly organized life. A need to control others and situations is common in their personal and work lives. They are prone to repetition and have difficulty making decisions and completing tasks because they become so involved in the details. They can be overly conscientious about morality and ethics and value polite, formal, and correct interpersonal relationships. They also tend to be rigid, stubborn, and indecisive and are unable to accept new ideas and customs. Their mood is tense and joyless. Warm feelings are restrained, and they tightly control the expression of emotions o Borderline Personality Disorder § Pattern of undermining self at the moment is a goal to be realized, possible psychotic-like symptoms during times of stress, recurrent job losses, interrupted education, broken marriages, history of sexual and physical abuse, neglect, hostile conflict, and early parental loss or separation. • Unstable interpersonal relationships, unstable self-image, unstable affects, cognitive dysfunctions (dichotomous thinking), impaired problem solving, impulsivity, and self-harm behaviors. • Emotional vulnerability, self-invalidation, unrelenting cries, inhibited grieving, active passivity, apparent competence. • Compare and contrast etiology, history, symptoms, assessment factors (what does patient present with) and associated behaviors (and the purpose of those behaviors) in patients diagnosed with: somatic symptom disorder; illness anxiety disorder (hypochondriasis); factitious disorder; factitious disorder imposed on another and conversion disorder o Somatic Symptom Disorder § Characterized by a combination of distressing symptoms and an excessive or maladaptive response or associated health concerns without significant physical findings and medical diagnosis. • Patients suffering is authentic (truthful and geniuine) and they typically experience a high level of functional impairment. § Common in women 16-25; included in the most common symptoms for visits to primary care providers are chest pain, fatigue, dizziness, headache, swelling, back pain, shortness of breath, insomnia, abdominal pain, and numbness. Health-related quality of life is frequently severely impaired, and patients43 appraise their bodily symptoms as unduly threatening, harmful, or troublesome, often fearing the worse about their health. o Illness Anxiety Disorder (Hypochonriasis) § Characterized by preoccupation with disease or illness. § The difference between Somatic Symptom Disorder and Illness Anxiety Disorder is that somatic symptoms are not present with Illness Anxiety Disorder, or if they are present, they are only mild. Illness anxiety can be quite obsessive as thoughts about illness may be intrusive and hard to dismiss even when the patients realize their fears are unrealistic. § People experience extreme worry and fear about the possibility of having a disease. Even normal bodily changes such as changes in heart rate or abdominal cramps, can be seen as red flags for serious illness – symptoms become amplified during times of increased stress. • Depression may also play a role in this disorder. o Factitious Disorder § People with factitious disorder consciously pretend to be ill to get emotional needs met and attain the status of patient § The term factitious is derived from the Latin word meaning “artificial or contrived”. Patients with this disorder artificially, deliberately, and dramatically fabricate symptoms or self-inflict injury, with the goal of assuming a sick role. • The illnesses can either be physical or psychiatric. Examples include: bleeding, fever, hypoglycemia, seizures, hallucinations, and even cancer/HIV § Munchausen Syndrome is associated with Factitious Disorder • Dramatically describes the illness using proper medical terminology and can be quite convincing. Reluctant for professionals to speak with family, friends, or previous doctors. • Often demand specific interventions and tests. If doctor sets limits with these patients or does not follow requests – the patient claims they are incompetent and will begin to shop for providers or hospitals for treatment § Factitious Disorder Imposed on Another (Manchusen by proxy) • This is when the caregiver deliberately feigns or invents illness on another to get a relationship with healthcare providers, and generally get attention and excitement. o The caregiver frequently is a health care worker or someone with extensive knowledge about the health care system. The disorder results in unnecessary medical visits and sometimes – harmful medical procedures. § Examples include premature delivery by rupturing the amniotic sac with a fingernail; infant apnea and SIDS; or introducing microorganisms into a child’s wound. § Malingering is mentioned as a condition related to Factitious disorders. Malingering is a consciously motivated act to device based on the desire for material gain. • It involves a process of fabricating an illness or exaggerating symptoms in order to become eligible for disability compensation, commit fraud against insurance companies, obtain prescription medications, evade military service, or receive a reduced prison sentence. o Body Dysmorphic Disorder § An obsessive-compulsive disorder that involves preoccupation with an imagined defective body part resulting in obsessional thinking and compulsive behaviors. o Conversion Disorder § Severe emotional distress or unconscious conflict is expressed through physical symptoms § Etiology44 • Neurological changes in the brain or childhood trauma § Symptoms • Impaired coordination or balance, paralysis, aphonia (inability to produce sound), difficulty swallowing or a sensation of a lump in the throat, and urinary retention • Loss of touch, vision problems, blind, deaf, hallucinations § Associated behavior (Purpose of behavior) • Nurse treats symptoms as real • Acknowledge the symptoms will help them deal with them • Compare and contrast Anorexia and Bulimia Nervosa with examples and identify the physiological criteria for hospitalization for each. o Anorexia Nervosa is a mixture of biopsychosocial symptoms that include significantly low body weight, intense fear of gaining weight or becoming fat, and a disturbance in experiencing body weight or shape (undue influence or distorted self-evaluation of body weight or shape or lack of recognition of the seriousness of low body weight). § Anorexia nervosa is further categorized into two major types: restricting (dieting and exercising with no binge eating or misuse of laxatives, diuretics, or enemas) and binge eating and purging (binge eating and misuse of laxatives, diuretics, or enemas). Malnutrition and semi-starvation result in a preoccupation with food, binge eating, depression, obsession, and apathy, as well as compromising several body systems, leading to medical complications and, in some instances, death § Body Distortion and body image (a mental picture of one’s own body) is a problem with anorexics – they severely distort the reality of their figure. § A drive for thinness is in place because of the body distortion. § Interoceptive Awareness or feelings of inadequacy and a fear of maturity is also a common characteristic. Weight loss becomes a way for these individuals to experience some sense of control and combat feelings of inadequacy and ineffectiveness. § Perfectionism – everything is symmetrical or objects are placed the same distance from one another is something that may be in place long before an eating disorder develops. • Symptoms: low weight, amenorrhea, lanugo (arm hair), cold extremities, muscle wasting, decreased bone density45 o Bulimia Nervosa involves binge and purge episodes – normally in secret o Patients with bulimia nervosa present as overwhelmed and overly committed individuals who have difficulty with setting limits and establishing appropriate boundaries. § Bulimia nervosa involves eating a large amount of food within a discrete period of time (e.g., 2 hours) and engaging in recurrent episodes of binge eating and compensatory purging in various forms such as vomiting or using laxatives, diuretics, or emetics or in non-purging compensatory behaviors, such as fasting or over-exercising in order to avoid weight gain. These episodes must occur at least once a week for a period of at least 3 months to meet the DSM-5 criteria. Self-evaluation is excessively and inappropriately influenced by body weight and shape. Unlike anorexia nervosa, there is little or no weight loss. § Binge eating is defined as rapid, episodic, impulsive, and uncontrollable ingestion of a large amount of food during a short period of time, usually 1 to 2 hours. Eating is followed by feelings of guilt, remorse, and often self-contempt, leading to purging. To assuage the out-of-control feeling, severe dieting is instituted, and these restrictions, referred to as dietary restraint, precipitate the next binge. The restrictions are viewed as “rules,” such as no sweets, no fats, and so forth. Each binge seems to influence stricter and stricter rules about what cannot be consumed, leading to more frequent binge eating. This cycle has prompted clinicians to focus treatment primarily on interventions related to dietary restraint.46 When dietary restraint is resolved, binge eating is decreased, and generally the purging that follows binge eating also is decreased. • Compare and contrast the following terms related to the normal sleep cycle: sleep latency; sleep architecture; sleep continuity; sleep fragmentation. o Sleep Latency: time period measured from lights out or bed time to initiation of sleep o Sleep architecture: pattern of non-rapid eye movement and rapid eye movement o Sleep continuity: unable to sleep through the night o Sleep hygiene: ways to promote the best sleep § Avoid napping, stimulants (alcohol, caffeine) § Exercise helps promote restful sleep – avoid 3 hours to bedtime § Avoid meals close to bed time § Ensure daily exposure to natural light § Reserve your bed for sleep and sex only – no other activities § Establish a regular routine for sleep habits o Sleep fragmentation: results in a sleep cycle that is typically short on slow-wave sleep and is often unrefreshing. Total time spent in sleep in any stage is also less than normal § Will wake up in the middle of the night with an inability to go back to sleep • Compare and contrast most effective specific medications for a patient experiencing problems with initiation versus effective medications for those patients experiencing sleep maintenance problems and discuss benefits and potential problems that each may cause. o Benzodiazepine receptor agonists, melatonin receptor agonists, sedating antidepressants, and OTC medications and supplements. § Benzodiazepine Receptor Agonists • Headache, dizziness, and residual sleepiness § Melatonin Receptor Agonists • Has been shown to shift circadian rhythm, decreases body temperature, alter reproductive rhythm, enhance immune function, and decrease alertness § Sedating Antidepressants § OTCs • Often are histamine receptor antagonists which cause side effects like sedation, diminished alertness, and slowing of reaction time. o They also produce anticholinergic effects like dry mouth, accelerated heart rate, urinary retention, and dilated pupils. • Propose the problem of “morning hangover” o ALL OF THESE HELP PATIENTS WITH INSOMNIA o Ramelteon (Rozerem), Lunesta (ezopiclone), Sonata (Zaleplon): Benzo-like (side effects) § Low abuse not controlled substance § Melatonin Receptor Agonist § Ramelteon should not be used by patients with severe hepatic impairment. It should not be used in combination with fluvoxamine. o ProSom (Estazolam), Ambien (zolpdem), Temazepam (restoril): Benzos § Benzo Receptor Agonist § Schedule IV controlled substance § Abuse and dependency potential § Be careful with withdrawal o Zaleplon (Sonate) § Sedative-hypnotic § Readily absorbed and metabolized § Warning • Shouldn’t be given to hepatic impairment • Potentiates psychomotor impairments of ethanol § Adverse Reactions • Ab pain, headache, dizzy, rash47 • Discuss symptoms of alcohol withdrawal and identify the best medications to ensure a safe withdrawal from alcohol. o Alcohol withdrawal syndrome: a syndrome that occurs after the reduction of alcohol consumption or when abstaining from alcohol after prolonged use, causing changes in vital signs, diaphoresis, and other adverse GI and CNS side effects o Delirium tremens: an acute symptom of alcohol withdrawal syndrome that is characterized by autonomic hyperarousal, disorientation, hallucinations, and tremors or grand mal (tonic-clonic) seizures § Signs of Alcohol Withdrawal: o Medications § Naltrexone (Vivitrol, injectable, ReVia, Depade, oral) – Withdrawal, relapse prevention, decrease cravings--nausea usually goes away after first month; headache, sedation, and pain at the injection site with each injection § Topiramate (Topamax) -- Withdrawal, works to decrease alcohol cravings by inhibiting the release of mesocorticolimbic dopamine § Diazepam (Valium)--Withdrawal--Alert patient to potential sedation. Educate about the signs and symptoms of withdrawal, including warnings of seizure activity. § Phenobarbital (Phenobarbital)--Withdrawal--produces sedation. vital signs should be checked frequently during withdrawal § Chlordiazepoxide (Librium)--Withdrawal--produces sedation, increases seizure threshold, reduce withdrawal agitation § Carbamazepine (Atretol, Tegretol) – Withdrawal--It works by decreasing nerve impulses that cause seizures and pain. May cause dizziness or drowsiness.48 Patient will need to take consistently and be tapered off to prevent seizures during detox. § Quetiapine fumarate (Seroquel)--Withdrawal, detoxification with reduced craving- -a drop in blood pressure may result when changing position from sitting to standing. May experience dry mouth and restlessness § **Disulfiram (Antabuse)—Maintenance – Helps prevent relapse of alcohol abuse. Ingested with alcohol will cause nausea, vomiting, headache, flushing, respiratory difficulties, and confusion. There is a metallic aftertaste; dermatitis; severe reaction or death could result from alcohol ingestion. For teaching, let the client know that any kind of alcohol will be harmful for example mouthwash and that they need to read labels § **Acamprosate calcium (Campral)—Maintenance—helps with alcohol cravings, possibly by reducing intensity of prolonged withdrawal syndrome. Benefit emerges after 30-90 days---Side effects include diarrhea, nausea, itching, intestinal gas, decreased libido. • Discuss the relationship between blood alcohol level (BAL), tolerance and normal/abnormal manifestations of BAL’s. o The level of CNS impairment while under the influence of alcohol depends on how much of it is consumed in a given period of time and how rapidly the body metabolizes it (tolerance). § People who use alcohol regularly usually develop alcohol tolerance, the ability to ingest an increasing amount of alcohol before they experience a high and show cognitive and motor effects. • Even though these individuals do not appear intoxicated, their BALs reflect the increased amount of alcohol Blood Alcohol Level Signs and Symptoms 20-100 mg percent Mood and behavioral changes, reduced coordination, impairment of ability to drive a car or operate machinery. 101-200 mg percent Reduced coordination of most activities, speech impairment, trouble walking, general impairment of thinking and judgment 201-300 mg percent Marked impairment of thinking, memory, and coordination; marked reduction in level of alertness; memory black outs; nausea and vomiting 301-400 mg percent Worsening of above symptoms with reduction of body temperature and blood pressure; excessive sleepiness; amnesia 401-800 mg percent Difficulty waking; serious decrease in pulse, temperature, blood pressure, and respirations; urinary and bowel incontinence; death • Compare and contrast medications that are used for maintenance of sobriety, including Antabuse, Campral, Revia and identify how each is used, potential adverse and common side effects and important teaching for each. o Disulfiram (Antabuse) – MAINTENANCE – helps prevent relapse of alcohol abuse. Must be taken consistently for aversion to alcohol to be consistent. Ingested with alcohol with cause nausea, vomiting, headache, flushing, respiratory difficulties, and confusion. There is a metallic aftertaste; dermatitis; severe reaction or death could result from alcohol ingestion. § Teach the client that any type of alcohol (even mouthwash or inhaling alcoholbased products) will be harmful and they need to read labels. o Acamprosate calcium (Campral) – MAINTENANCE – helps with alcohol cravings, possibly by reducing intensity of prolonged withdrawal syndrome by balancing49 neurotransmitters. Benefit emerges after 30-90 days. § Side effects include diarrhea, nausea, itching, intestinal gas, decreased libido. o Naltrexone (ReVia) – WITHDRAWAL/MAINTENANCE – relapse prevention, decreasing cravings § Side effects: nausea usually goes away after first month; headache, sedation, and pain at the injection site with each injection. o Suboxone – MAINTENANCE – injection used for active withdrawal and levels are adjusted over several days. Typically used for 9-12 months and then is tapered off. • Compare and contrast the type of questions used to elicit self-concept information in children and adolescents. o For young children, eliciting their view of themselves and the world is helpful. One technique is asking them what they would wish for if they had three wishes. Answers can be revealing. Whereas an inability to wish for anything beyond a nice meal or place to live may reflect hopelessness, wishes to conquer the world or put one’s teacher in jail may indicate feelings of grandiosity. Another technique is to tell a story and ask the child to make up an ending for it. For example, a baby bird fell out of a nest—what happened to it? The nurse may design stories to elicit particular fears or concerns that may be relevant for the individual child. o Drawings also provide an excellent window into the child’s internal world (Fig. 34.2). Asking the child to draw a picture of a person can provide data about the child’s selfconcept, sexual identity, body image, and developmental level. By age 3 years, children should be able to draw some facial features and limbs, but their drawings may have an “x-ray” quality, in which clothing is transparent and the body can be seen underneath. Older children should produce more sophisticated drawings unless they are resistant to the task. After the child has finished the drawing, the nurse can ask what the person in the drawing is thinking and feeling, using this device to assess the child’s mental processes. For example, one adolescent with school phobia drew a person fully dressed, in great detail, but with no feet. When asked about the drawing, he said that the boy could not go anywhere because his mother was afraid to let him leave home. o Other ways to assess children’s self-concepts include asking them what they want to do when they grow up, what their best subjects are in school, what things they are really good at, and how well-liked they are at school. Before concluding the individual interview with a child, the nurse should always ask if the child has any other information to share and whether he or she has any questions. § Self-concept: ask about play, favorite stories, and three wishes. Ask the child to draw a self-portrait, describe best and least liked qualities. Ask what he or she imagines doing for an occupation when grown up – also evaluate planning ability and sense of a future • Compare and contrast best interviewing/assessment techniques based on developmental levels of pre-school-aged, school-aged and adolescent children. o Pre-school § These children may have difficulty putting their feelings into words and that their thinking is very concrete § Join their world of play – it’s where they transform an experience from real life into a symbolic, nonliteral representation. • Play encourages verbalizations, promotes manual strength, teaches rules and problem solving, and helps children master control over their environment. • Drawings are also used to illuminate the child’s intellect, talents, deficits, body image difficulties, and perceptions of family life. § With children younger than 5 years of age, the nurse may conduct the assessment in a playroom. • While observing a child in the free play setting, the nurse should pay attention to the start of play, energy level, manipulation actions, tempo, themes of play, expression of emotions, and temperament are important to observe.50 § The nurse’s roles are to be a good listener; use appropriate vocabulary; tolerate a child’s anxious, angry, or sad behavior; and use reflective comments about the child’s play o School aged § Can use more constructs, provide longer descriptions, and make better inferences of others. § Competitive board games, such as checkers and playing cards § In this game, the clinician and child take turns drawing cards that pose hypothetical situations and ask what a person might think, feel, or do in such scenarios. For example, one card might say, “A boy has something on his mind that he is afraid to tell his father. What is he scared to talk about?” Another might read, “A girl heard her parents fighting. What were they fighting about? What was the girl thinking while she listened to her parents?” o Adolescent § Adolescents are likely to be defensive in front of their parents and concerned with confidentiality. • Often portray egocentrism – preoccupation with one’s own appearance, behavior, and thoughts. § Adolescents generally prefer a straightforward, candid approach to the interview because they often distrust those in authority. § Mentioning to adolescents that they do not have to discuss anything that they are not ready to reveal is also a good idea, so they will feel in control while they gradually build trust. • Describe realistic goals for a child diagnosed with mild, moderate and severe Intellectual disability disorder. o An intellectual disability is defined as limitation in intellectual functioning and adaptive behavior § Result from a variety of causes with the most common etiology related to genetic syndromes. Chromosomal changes or defects (down syndrome) and exposure to toxins during prenatal development (fetal alcohol syndrome), heredity, pregnancy and perinatal complications, medication conditions, and environmental influences are all associated with intellectual disabilities o There is literally nothing about mild moderate or severe in the book § The assessment of a child with an intellectual disability focuses on current adaptive skills, intellectual status, and social functioning. A developmental history is a useful way to gather information about past and current capacities. The nurse compares these data with normal growth and development. Developmentally delayed children who have not had a psychological evaluation should be considered for referral. These children also require evaluation for other comorbid psychiatric disorders, which may be a challenge because of the child’s cognitive limitations. Discussions about feelings and behavior may be too complex for these children. If children or adolescents with intellectual disabilities have a comorbid mental disorder or serious behavioral problems, a carefully constructed interdisciplinary behavioral plan will guide care and treatment. § Children and families may require varying levels of interventions at different times throughout the life cycle. When a child is young, the family requires special academic support and, for some, residential services. The need for psychiatric intervention varies according to the severity of disability, family functioning, and the existence of other disorders. Feelings of grief and loss in family members (especially parents) related to having a child with a disability may be relieved through family therapy. More specific parent training may be needed to deal with emerging maladaptive behaviors.51 • Discuss the diagnostic criteria for ADHD and give examples of Impulsivity, Hyperactivity and Inattention and give examples of behaviors you might see. o A persistent pattern of inattention, hyperactivity, and impulsiveness that interferes with functioning characterizes ADHD. A diagnosis is made based on school behavior, parents’ reports, and direct observation of inattention and hyperactivity-impulsivity that are inconsistent with developmental level. Parents and teachers describe children with ADHD as restless, always on the go, highly distractible, unable to wait their turn, heedless, and frequently disruptive. Indeed, it is often disruptive behavior that brings these children into treatment. § In ADHD, the person finds it difficult to attend to one task at a time and is easily distracted. For some, the lack of attention is related to being unable to filter incoming information, which leads to being unable to screen and select the important information. That is, all incoming stimuli are treated the same (e.g., directions from a teacher elicits the same importance as noise in the hallway). For others, the distractibility may be related to stimuli-seeking behavior. Given the heterogeneity of ADHD, either of these models explains problems of attention for subgroups of affected children. § Children with ADHD are prone to impulsive, risk-taking behavior and often fail to consider the consequences of their actions. They tend to exercise poor judgment and to have more than the usual lumps, bumps, and bruises because of their risk-taking behavior. They often require a high degree of structure and supervision o Impulsiveness is the tendency to act on urges, notions, or desires without adequately considering the consequences o Hyperactivity is excessive motor activity, as evidenced by restlessness, an inability to remain seated, and high levels of physical motion and verbal output • Describe the best environment and nursing care for a hospitalized child diagnosed with Autism Spectrum Disorder o Autism spectrum disorder is characterized by persistent impairment in social communication and social interaction with others. § Children with ASD may or may not have an intellectual disability, but they commonly show an uneven pattern of intellectual strengths and weaknesses • They are rigid in style, intolerant of change, and prone to behavioral outbursts in response to environmental demands or changes in routine. § A structured physical environment will most likely be important to a child with this disorder. Keeping furniture, dishes, and toys in the same place helps ease anxiety and fosters secure feelings. The nurse should identify the child’s specific needs for structure in the physical environment and what happens when the physical environment is changed. • Promoting Interaction: Structuring interventions for social isolation should fit the child’s cognitive, linguistic, and developmental levels. Interventions fostering nonverbal social interactions may be more useful than those based on speech. For higher functioning children, activities such as getting the mail, passing out snacks, or taking turns in the context of simple games can engage them in social activities without requiring the use of their limited language skills. Structuring social interactions so that the child shares a task with another, such as carrying a load of books, may help boost confidence in relating to others. • Ensuring Predictability and Safety: a consistent, structured environment with predictable routines for activities, mealtimes, and bedtimes—is necessary for successful treatment. Changes in routine may provoke disorganization in the child, leading to emotional disequilibrium and explosive behavior.52 • Discuss nursing care for a child diagnosed with ADHD and compare and contrast psychostimulant medications for children and adolescents experiencing ADHD, including therapeutic actions expected to be observed, common adverse reactions/side effects and important nursing teaching. o Background of ADHD § Show an inappropriate degree of inattention, impulsiveness, and hyperactivity. Some children can have attention deficit disorder without hyperactivity (ADD). § In order to diagnose a child with ADHD symptoms must be present in at least two settings (ex at home and school) and occur before age twelve. § In adults, fewer symptoms are necessary to gain a diagnosis. The disorder is most often detected when the child has difficulty adjusting to elementary school. § Attention problems and hyperactivity contribute to low frustration tolerance, temper outbursts, labile moods, poor school performance, peer rejection, and low self-esteem. § Children with ADHD are often diagnosed with comorbid disorders such as oppositional defiant disorder or conduct disorder. § The behaviors and symptoms associated with ADHD can include hyperactivity, difficulty taking turns or maintaining social relationships, high levels of impulsivity, poor social boundaries, intrusive behaviors, or frequently interrupting others. § Those with inattentive type of ADHD may exhibit high degrees of distractibility and disorganization; they may be unable to complete challenging or tedious tasks, become easily bored, lose things frequently, or require frequent prompts to complete tasks. o ADHD Medications § To control the aggressive behaviors found with these disorders, tried, including antipsychotics, lithium, anticonvulsants, and antidepressants. § **Psychostimulants must be used judiciously as they appear to have a dosedependent effect • low doses stimulate aggressive behaviors • moderate to high doses suppress aggression. This appears to be most effective in those patients with ADHD and associated aggressive behavior. § Methylphenidate (Ritalin) and amphetamine salts (Adderall) are the most widely used psychostimulants because of their relative safety and simplicity of use. As with any controlled substance, however, there is a risk of abuse and misuse such as the sale of medication on the street or the use by people for whom the medication was not intended. Insomnia is a common side effect while taking the stimulant ADHD medications. § Mood stabilizers such as lithium and anticonvulsants reduce aggressive behavior and are recommended for impulsivity, explosive temper, and mood lability. § Adrenolytic medications such as clonidine are also useful in reducing agitation and rage and in increasing frustration tolerance. § Antipsychotic medications have reduced violent behavior, hyperactivity, and social unresponsiveness. Due to the risk of tardive dyskinesia associated with long-term use, antipsychotic medications are recommended for use only in severely aggressive conduct disorder. § Treating with the minimum effective dose is essential, as is administering the medication no later than 4:00 in the afternoon. The extended-release formulations of these medications have improved dosing and scheduling, allowing for a morning administration with sustained release of the medication over the course of the day and with a decreased incidence of insomnia. • Other common side effects include appetite suppression, headache, abdominal pain, and lethargy. § *A non-stimulant selective norepinephrine reuptake inhibitor, atomoxetine (Strattera), is approved for childhood and adult ADHD (primarily inattentive)53 • Therapeutic responses develop slowly, and it may take up to 6 weeks for full improvement • Strattera should be used with extreme caution in those patients with comorbid depression or anxiety as its use has been associated with an increased incidence of suicidal ideation. § The most common side effects are gastrointestinal disturbances, reduced appetite, weight loss, urinary retention, dizziness, fatigue, and insomnia. It may also cause liver injury in some patients and a small increase in blood pressure and heart rate. • Ongoing monitoring of vital signs and regular screening of liver function are key aspects of assessment. Rarely, serious allergic reactions occur. Patients and their families should be clearly educated on the risks and benefits of treatment prior to starting this medication. o Psychostimulants are the most commonly used medication for the treatment of ADHD. These medications enhance dopamine and norepinephrine activity and thereby improve attention and focus, increase inhibition of impulsive actions, and quiet the noise associated with distractibility and shifting attention. § Methylphenidate (Ritalin) • Duration of action about 4 hours; when first dose wears off it is known as the rebound effect – can fix this problem by having the first and second dose closer to one another. • Longer acting preparations of methylphenidate such as Concerta, Ritalin LA, and Metadate or amphetamine–dextroamphetamine (Adderall) do not require frequent dosing and may be a better fit with a school day schedule. § Atomoxetine (Strattera) • A non-adrenergic reuptake inhibitor – not classified as a stimulant • Adverse effects include: headache, abdominal pain, decreased appetite, vomiting, somnolence, and nausea. § Concerta • Increased heart rate and chest pain are common side effects • Contraindications include glaucoma, tics/Tourette’s, severe anxiety, tension, or agitation • AVOID WITH MAOIs LAST 14 DAYS § Adderall • Side effects include bladder pain, bloody/cloudy urine, difficulty/burning/painful urination, fast/pounding heart rate, frequent urge to urinate, and lower back pain. • AVOID WITH MAOIs LAST 14 DAYS o One of the major concerns with the psychostimulants is the potential for abuse. With the increase in recognition of the ADHD, there has been an increase in psychostimulant prescriptions. There has also been an increase in teen and preteen abuse of amphetamine products. These abused prescription medications most often belong to the adolescents or a friend. Nurses should caution parents about the potential for abuse and prevent their child’s medication from being a source of recreational use. o ADHD Therapies § Cognitive Behavioral Therapy (CBT) is used to change the pattern of misconduct by fostering the development of internal controls and working with the family to improve coping and support. Development of problem solving, conflict resolution, empathy, and social skills are important components of the treatment program.54 • Compare and contrast psychotropic medications for Alzheimer’s that block NMDA channels versus those that are cholinesterase inhibitors. § Cholinesterase Inhibitors are the mainstay of pharmacologic treatment of dementia because they inhibit acetylcholinesterase, an enzyme necessary for the breakdown of acetylcholine. Inhibition of AChE results in an increase in cholinergic activity. Because these medications have been shown to delay the decline in cognitive functioning but generally do not improve functioning after it has declined, it is important that this medication be started as soon as the diagnosis is made. The primary side effects include: GI distress, N/V, and diarrhea. § Cholinesterase drugs increase the risk for developing stomach ulcers – prolonged use of NSAIDs with these medications should be monitored. o N-Methyl-D-Asparate Antagonists § Overstimulation of the N-methyl-D-aspartate (NMDA) receptor by glutamate (excitatory neurotransmitter) is considered to have a role in AD. In dementia, it is hypothesized that there is a chronic release of glutamate that causes a permanent increased intracellular calcium concentration that leads to neuronal degeneration. Memantine (Namenda XR) is an NMDA-receptor antagonist that has been shown to improve cognition and ADLs in patients with moderate to severe symptoms of dementia. • Compare, contrast and give examples of the following terms related to dementias: agnosia; apraxia, confabulation; perseveration; sundowning. o Agnosia: failure to recognize or identify objects despite intact sensory function o Apraxia: impaired ability to execute motor activities despite intact motor functioning. o Confabulation: telling a plausible but imagined scenario to compensate for memory gaps o Perseveration: repetition of a particular word/phrase/gesture o Sun-Downing: late delay or confusion – agitation gets worse throughout the day – less pronounced symptoms in the morning with dementia than later in the day o • Discuss barriers to successful treatment of homeless clients who are mentally ill and reasons contributing to lack of compliance with psychotropic medications. o Cost and lack of insurance are the biggest barriers to health and hospital care for homeless people. Another barrier is the inability of this population to carry out treatment55 recommendations; survival is their first priority. Compliance with medication and treatment regimens is difficult because successful treatment requires collaboration, monitoring, time for medication and other measures to be effective, and a secure place to keep medication. Mentally ill people who are homeless often cannot routinely get prescriptions filled. Medicines may be stolen. It is necessary for the person or family unit to have a place to keep medications that can be reached at the necessary times and have access to primary care services for regular check-ups, assessments for adverse drug responses, and necessary blood monitoring. • Compare and contrast intimate partner violence, stalking, sexual assault describing each, identifying motives for each and give characteristics and examples of each. o Intimate Partner Violence: defined by as psychological, physical, or sexual harm perpetrated by a current or former spouse or partner § Physical violence may be episodic, psychological abuse is frequent and unrelenting. Overtime, psychological abuse is devastating to an individual’s selfesteem and can lead to depression, anxiety, substance abuse, and other psychological disorders as well as other physical illnesses. • The varieties of abuse are used to exert power and control over romantic partners. § The most common type of abuse occurs as a result of domestic (family) violence; that is, the perpetrator is or once was a loved and trusted partner or family member. Many women are afraid or reluctant to identify their abuser, fearing retaliation against themselves or their children. Often, they continue to hold strong feelings for their partners despite the abuse. When medical care is required, women often attribute their injuries to other causes. § Examples may include violence and abuse during pregnancy; younger, single, divorced, and separated women are at a higher risk; and children of intimate partner violence are secondary victims. • Children who witness IPV are often overlooked as abused victims unless they demonstrate evidence of physical or sexual abuse themselves. Children who witness IPV may accept it as normal and a rational way to deal with problems. o Stalking: a pattern of repeated unwanted contact, attention, and harassment that often increases in frequency § Stalkers terrorize and harass their victims through behavior that causes fear or substantial emotional distress. Stalking may include such behaviors as following someone, showing up at the person’s home or workplace, vandalizing property, or sending unwanted gifts. § Cyberstalking is the use of the internet, email, or other telecommunication technology to harass or stalk another person.56 o Rape and Sexual Assault: includes any form of nonconsenting sexual activity, ranging from fondling to penetration. § The definition of rape, the most severe form of sexual assault, occurs when there is penetration, no matter how slight, or the vagina or anus with any body part or object, or oral penetration by a sex organ of another person, without the consent of the victim. § Less than half of rapes and sexual assaults against women are reported. Victims do not report sexual assault for the same reason that IPV is underreported – embarrassment, shame, concern about not being believed, and fear of being blamed for the assault. § Rapists use sexuality as a weapon to dominate, intimidate, and humiliate another person. Rapists can be classified into three categories: the power rapist, the anger rapist, and the sadistic rapist. • Power rapists account for over half of sexual assaults – they often attack people their own age and use intimidation and minimal physical force to control their victims. Their assaults are generally premediated. • Anger rapists tend to target either very young or very old victims. They may use extreme force and restraint that results in physical injury to the victim. • Sadistic rapists account for about 5% - they are the most dangerous. Their crimes are premediated and they often torture and kill their victims. Sadistic rapists derive erotic gratification from their victims’ suffering.57 • Review the phases in the cycle of violence and identify what occurs in each. o The cycle consists of three recurring phases that often increase in frequency and severity. § Phase 1: Tension Building • Minor incidents • Perpetrator establishes total control of victim by psychological and emotional means • Perpetrator demands total acquiescence of victim. Verbal abuse and accusations follow. • Perpetrator isolates victim by approving/disapproving social contacts and demands explanations • Perpetrator degrades and demoralizes victim by scrutinizing victim’s physical and mental characteristics (unattractive, stupid) and functions and assaulting victim’s self-esteem (worthless, no good) § Phase 2: Violence Erupts • Severe injury to victim and children • Victim may incite violence as a way to control mounting terror • Period of relative calm follows battering § Phase 3: Remorse Ensues • Perpetrator becomes kind, contrite, and loving – begging for forgiveness and promising to never inflict abuse again (until the next time) o Tension builds; the cycle repeat [Show More]
Last updated: 1 year ago
Preview 1 out of 57 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
May 16, 2021
Number of pages
57
Written in

Additional information
This document has been written for:
Uploaded
May 16, 2021
Downloads
0
Views
39
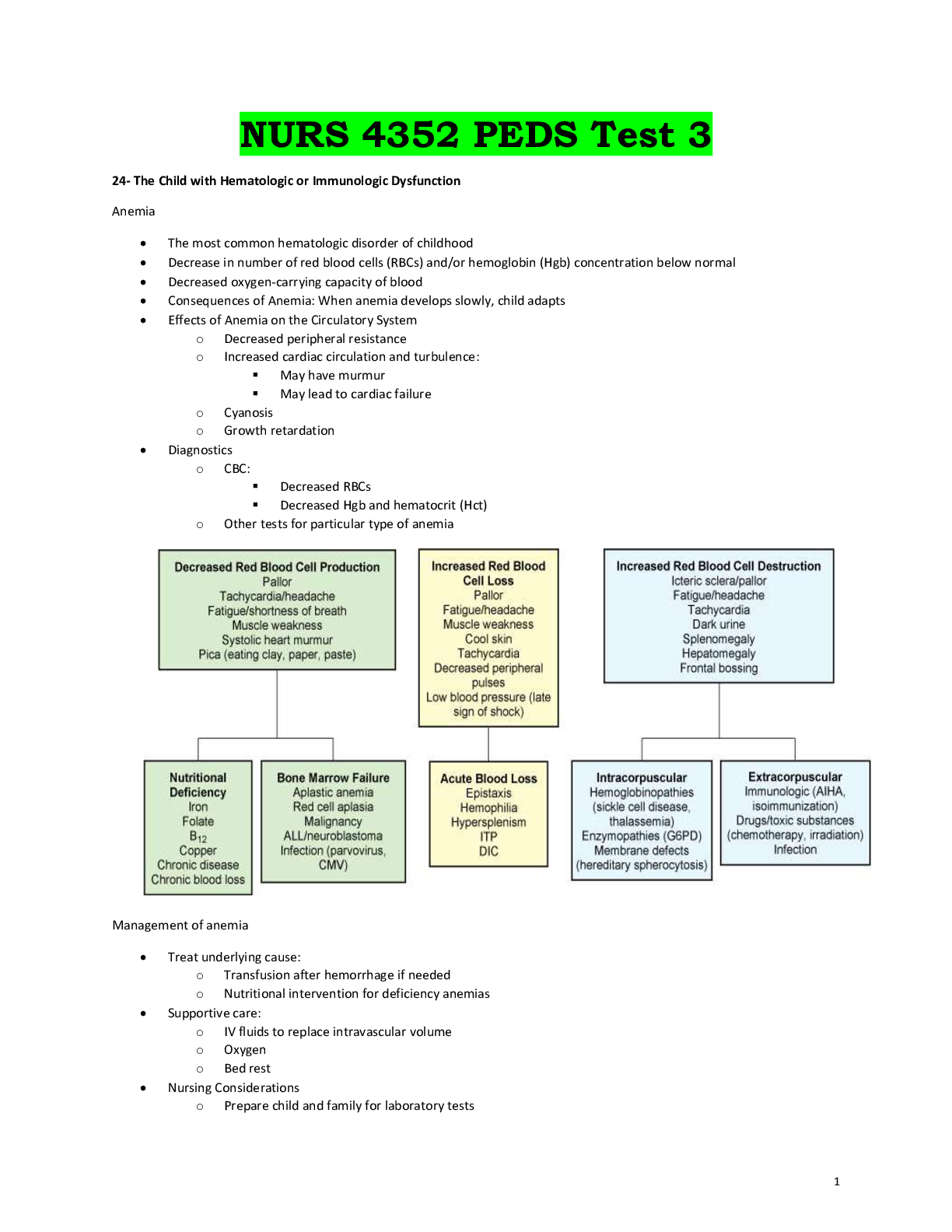
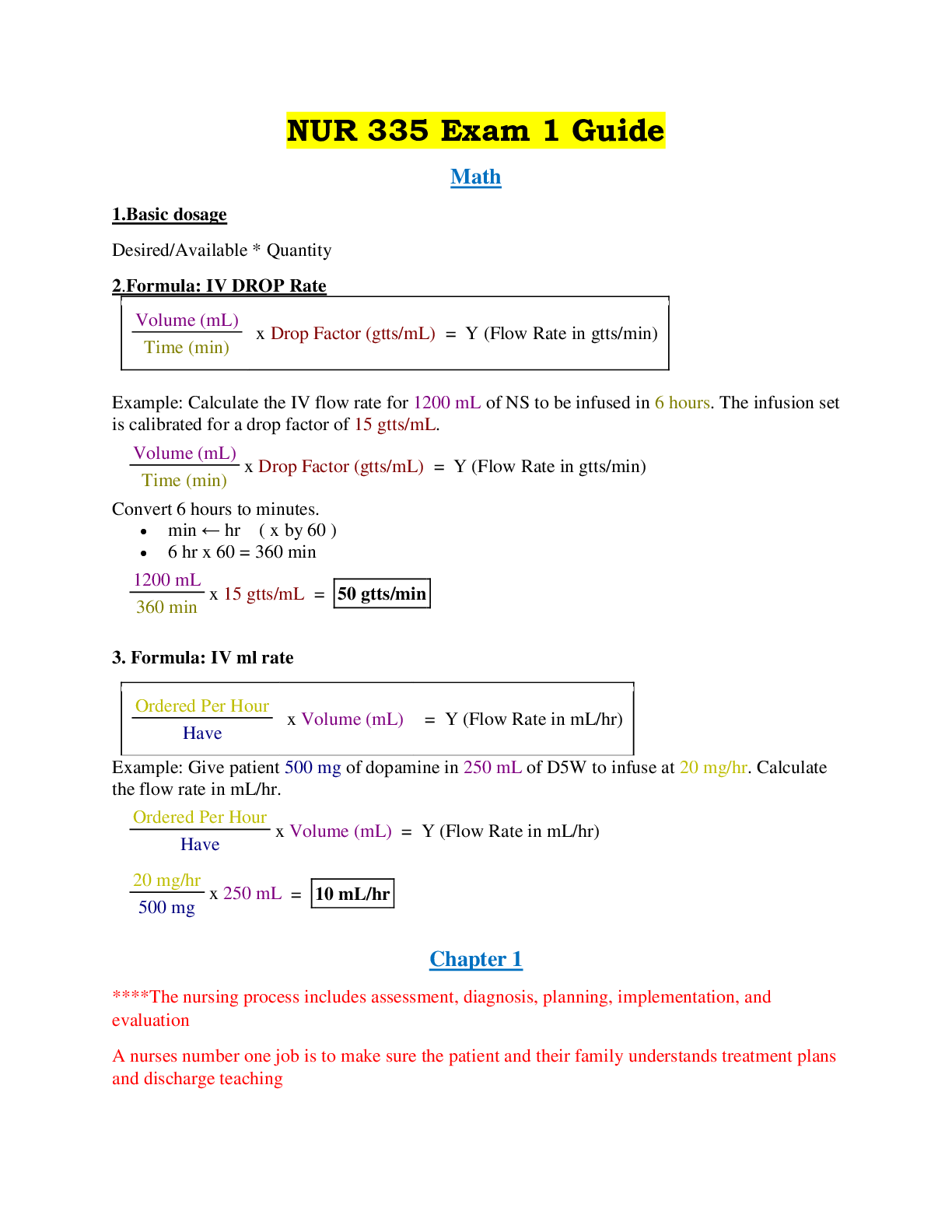


 (4).png)

 Rasmussen College.png)