*NURSING > CASE STUDY > NR 601 Case Study Chamberlain College of Nursing : Primary Care of the Maturing and Aged Family May (All)
NR 601 Case Study Chamberlain College of Nursing : Primary Care of the Maturing and Aged Family May, 2018
Document Content and Description Below
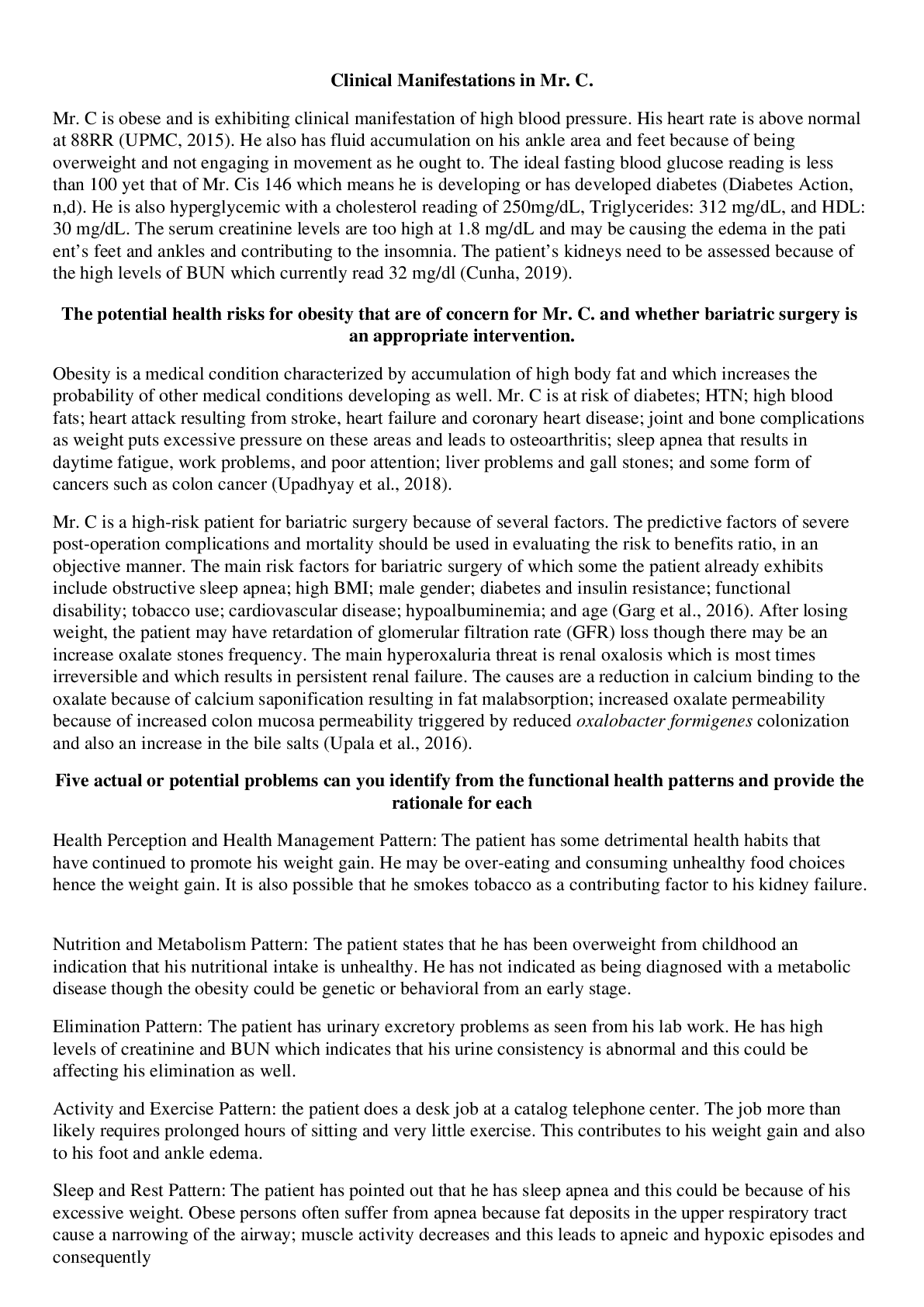
Introduction The purpose of this paper is to demonstrate the ability to analyze the subjective and objective information from the case study to formulate a management plan using evidenced based gui... delines. It also demonstrates the student’s ability to write SOAP note in chronological order. In this case study the assessment, treatment plan, medication and its cost, and SOAP note will be discussed in detailed. Assessment Based on the chief complaints, subjective, and objective findings patient’s primary diagnosis is type 2 diabetes mellitus (E11). The pathophysiologic mechanism of type 2 diabetes involves insulin resistance and decreased insulin secretion by beta cells of pancreas (McCance, Huether, Brashers, & Rote, 2013). The genetic, epigenetic, and environmental factors interfere the ability to sense increased blood glucose, insulin synthesis, and insulin secretion, which causes type 2 diabetes. The prevalence of type 2 diabetes increased with age, is higher among African American female, but obesity, hypertension, physical inactivity, and family history predominantly increased the risk of type 2 diabetes (McCance et al., 2013). Polyuria, polydipsia, and polyphagia are the classis symptoms of diabetes, but patient may present with nonspecific symptoms such as fatigue, pruritus, recurrent infection, visual change, paresthesia, or weakness (McCance et al., 2013). Based on the information given, the pertinent positive findings include very fatigued, no energy, weight gain, increased hunger and thrust, and increased frequency of urination for past 3 month. The polydipsia, polyuria, and polyphagia also known as 3P are the hallmark symptoms of diabetes (American Diabetes Association [ADA], 2017). The laboratory finding indicates her hemoglobin A1C is 6.9%, total cholesterol is 230 mg/dl, LDL 144mg/dl, VLDL 36 mg/dl, HDL 38mg/dl and triglycerides 232. The hemoglobin A1C of ≥ to 6.5% is one of the criteria that indicates diabetes (National Diabetes Education Initiative [NDEI], 2016). Mrs. G. blood glucose level of 126 which is at the meets the criteria for diabetes but has limited information on fasting status. The fasting plasma glucose of ≥ 126 is indicative to diabetes (NDEI, 2016).Her history of delivering a baby who weigh 9lb 2 oz is another risk factor of type 2 diabetes according to the ADA guidelines (NDEI, 2016). In addition, she has 1+ glucose and small protein on her UA. She weighs 185 pounds and her BMI based on her height and weight is 33.3 which is considered obese. Type 2 diabetes is most common in overweight or obese because excess weight causes some degree of insulin resistance (ADA, 2017). Other pertinent positive information that helps to diagnose type 2 diabetes includes obesity, dyslipidemia, and being Hispanic age greater than 50 years because risk of type 2 increases with age, obesity, lack of physical activity, dyslipidemia, and in certain racial or ethic groups such as Hispanic (ADA, 2017). The pertinent negative findings include no pruritus, recurrent infection, visual change, paresthesia, or weakness (McCance et al., 2013). Type 2 diabetes has a strong genetic predisposition, which Mrs. G is negative for this risk. The patient presenting symptoms such as 3P which are the hallmark symptoms of diabetes, her risk factors, and laboratory findings strongly suggest type 2 diabetes, thus it is a primary diagnosis of Mrs. G. Secondary Diagnosis Mixed hyperlipidemia (E78.2) is a secondary diagnosis that needs to be addressed during this visit. Hyperlipidemia is an acquired or genetic disorder that causes increased circulating lipids such as cholesterol, triglycerides, and fats in the blood (Moneta, n.d.). It is most commonly caused due to consumption of food high in saturated or trans fats, sedentary lifestyle, obesity, smoking, and diabetes. The familial hyperlipidemia is result from mutation in gene in a form of cholesterol called low density lipoprotein which causes atherosclerosis and cardiovascular diseases. The patient with type 2 diabetes often time have hypertriglyceridemia due to overproduction of lipoprotein in the liver which causes decrease high-density lipoprotein (HDL) and increased LDL, cholesterol, and triglycerides due to decrease lipoprotein activity (Karr, 2017). The role of race and gender in the development of hyperlipidemia is not clear, however, it is shown to be more prevalent in obese non-Hispanic black (Karr, 2017). The elevated blood lipids level doesn’t cause any symptoms, therefore patient remained asymptomatic and undiagnosed until they develop atherosclerosis plaques that reduce blood flow to the vital organ causing angina, heart attack, stroke, or pancreatitis (Karr, 2017). According to Kennedy-Malone, Fletcher, & Plank (2014), the physical finding may reveal xanthoma, xanthelasma, arterial bruits, or vascular claudication. Mrs. G did not have any symptoms related to hyperlipidemia. The pertinent positive data includes being obese, father has high cholesterol, and her laboratory finding of total cholesterol 230mg/dl which is borderline high (normal <200 mg/dl), LDL 144 mg/dl is at borderline high (normal <100mg/dl), VLDL 36mg/dl which is high (normal <30mg/dl), HDL 38mg/dl which is low (normal >40mg/dl) and triglycerides 232 which is high (normal <150mg/dl) (Kennedy-Malone, Fletcher, & Plank, 2014). Mrs. G. neither has symptoms nor has physical finding that indicates hyperlipidemia, but being obese, family history of hyperlipidemia, her laboratory test that showed borderline to high lipid profile, as well as her new onset of type 2 diabetes warrant the diagnosis and treatment of hyperlipidemia. The decision to add this problem into diagnosis is because abnormal lipid profile requires compressive assessment of risk for atherosclerotic cardiovascular disease (ASCVD) and early management. Multiple studies has shown that statin lowers total cholesterol and LDL which reduce the risk of cardiovascular disease as well as reduce mortality and disease progression among patient with clinical ASCVD (Karr, 2017). Obesity (E66.9) is another secondary diagnosis that needs to be addressed at this visit. Obesity is a condition that causes excess adipose tissue manifested by body mass index (BMI) of 30kg/m2 or weight above the 95th percentile in the growth chart (McCance et al., 2013). It is more common in women, African American women are likely to be obese, but the incidence is high among people with low socioeconomic status (McCance et al., 2013). Diet, sedentary lifestyle, inactivity, environmental factors, and genetic predisposition contributes to the incidence of obesity. Intake of calories that exceed the metabolic needs of the body remained the major cause of obesity. Symptoms of obesity includes fatigue, decreased energy, weakness, joint pain, shortness of breath, daytime sleepiness, and depression (McCance et al., 2013). BMI of 30-40 kg/m2 is diagnosed as obesity (McCance et al., 2013). Mrs. G. BMI is 33.6 kg/m2 which indicates obesity. Her complaints of being very fatigue and lack of energy are additional pertinent positive data which support the diagnosis. However, she did not report other symptoms such as weakness, shortness of breath, or feeling down or depressed. Obesity increased the risk of type 2 diabetes, coronary artery disease, stroke, death, and disability. The nonesterified fatty acid secreted from the adipose tissue in obese patient causes insulin resistance and impair β-cell function, thus leading to type 2 diabetes (Al-Goblan, Al-Alfi, & Khan, 2014). In order to better manage her diabetes, it is important to address the obesity problem at this visit. Obesity is one of the medical comorbidity that impact the health and wellbeing of the patient, thus needs to be addressed and managed on timely manner. Hypertension (I10) is another issue that can be address at this visit because early detection, prevention, and management has better outcome. Hypertension refers to elevation of blood pressure above normal. The imbalance in the vasodilator and vasoconstrictive substance produced by endothelium or renin production increase vascular resistance and rise in blood pressure (McCance et al., 2013). Age, sex, ethnicity, genetic, environmental factors, and lifestyle plays significant role. The diagnosis of hypertension is typically made on routine visit based on the BP reading because patient remained asymptomatic, but sometime may present with headache or change in vision (McCance et al., 2013). Mrs. G BP reading is 129/80 on this visit which is considered elevated BP according to new updated ACC/AHA blood pressure guidelines. The systolic blood pressure between 120-129 and diastolic <80 is categorized as elevated BP (American college of Cardiology, 2017).The patient has one BP reading which is elevated from normal, therefore she will need at least one more BP reading at separate occasion and home BP monitoring before treating hypertension () However, given her mother’s history of hypertension, her age, elevated glucose level, lipid panel, and obesity, I think it is important to address the elevated BP now and encourage her to modify her lifestyle. The diagnosis of hypertension was chosen because her BP reading of 129/80 is considered elevated as per the new ACC/AHA guidelines. Left knee arthritis (M17.12) is one of her past medical history. I think it is important to address this diagnosis because she is currently taking 500mg Tylenol every day for pain. Arthritis is one of the most common articular disease of older adults age 45 and older. Women tends to have higher chance of arthritis than men and obesity is one of a risk factors for knee arthritis. The biomechanical stresses and biochemical changes in articular cartilage and synovial membrane causes narrowing of joint space and osteophyte formation which leads to pain in the affected joint and impaired ability to perform activities of daily livings (McCance et al., 2013). The signs and symptoms include pain, morning stiffness, swelling, limited range of motion, cracking sound, or crepitus (McCance et al., 2013). The pertinent positive data found in the case study includes history of left knee arthritis and takes Tylenol to manage her pain. Overweight and age greater than 45 are her risk factors of arthritis. Patient came in with the prior history of arthritis and she is actively taking pills to manage her pain, therefore it is included as a secondary diagnosis. Differential Diagnosis Depression (F33.0) is a common psychosocial problem seen in the primary care setting. Most patient with depression present with complaints of severe feeling of sadness, apathy, unexplained fatigue, irritability, and anxiety. The exact pathophysiology of depression is unknown. The genetic and environmental factors play significant role in the etiology of mood disorder. Hypersecretion of cortisol may cause depression (McCance et al., 2013). A study indicated that a functional polymorphism in the serotonin transporter gene may interact with stressful life event increases the risk of depression (McCance et al., 2013). Alteration in sleep, appetite, sexual behavior as well as changes in endocrine, immunological, chronobiological abnormalities have a correlation with depression. Some of the signs and symptoms of depression includes irritability, low energy, fatigue, change in appetite or weight, insomnia, suicidal thoughts, helplessness, worthlessness, difficulty with memory and concentration (Ng, How, & Ng, 2016). Mrs. G complaint of very fatigue, low energy, recent weight gain, change in appetite, and feeling hungry are some of the pertinent positive finding for depression, therefore this diagnosis is added to the differential list. This patient neither report feeling of hopelessness, worthlessness, change in memory or concentration, restlessness, nor thoughts of suicide, therefore this is less likely to be her top most differential but given her symptoms it would still be considered as one of her differential diagnosis. Cushing’s disease (E24.9) is another differential diagnosis I will still consider for this patient. Increased circulating cortisol level due to excessive secretion of adrenocorticotropin hormone (ACTH) by pituitary adenoma is the most common cause of Cushing’s disease (Lonser,Nieman, & Oldfield, 2017). Cushing’s disease may lead to diabetes, hypertension, obesity, osteoporosis, and vascular disease if not treated appropriately. The signs and symptoms include obesity, diabetes, hypertension, moon facies, weight gain, increased thirst, fatigue, glucose intolerance, and facial plethora (Lonser et al., 2017). It can also may lead to depression, anxiety, panic attack, suicidal ideation, learning impairment, and memory deficit (Lonser et al., 2017). Mrs. G. presenting symptoms of weight gain, fatigue, obesity, elevated BP, and hyperglycemia could be associated with Cushing’s disease. This would require further laboratory assessment to confirms the diagnosis of endogenous hypercortisolism such as salivary cortisol, 24 hours urine free cortisol, or low dose dexamethasone suppression test (Lonser et al., 2017). Her presenting symptoms and laboratory data are consistent with Type 2 diabetes, but her subjective findings can be linked to Cushing’s syndrome, thus is a differential diagnose to consider if diabetes is ruled out. Plan The diagnostic test that I will consider ordering for this patient to diagnose type 2 diabetes includes fasting plasma glucose (FPG) or the 2 hours plasma glucose (2-h PG) level after a 75gram oral glucose tolerance test or the A1C level (ADA, 2017). The blood glucose results given in the case study doesn’t specify if it is fasting or not. Unless the patient has a clear clinical diagnosis such as classic symptoms of hyperglycemia or random plasma glucose of ≥ to 200mg/dl, a second test is required to confirm the diagnosis (ADA, 2017). The recommendation is to repeat the same test with new blood sample to confirm the diagnosis (ADA, 2017). The two- separate reading of A1C or FBG above the diagnostic threshold of >6.5% and ≥ 126 mg/dL respectively, can confirm the diagnosis (ADA, 2017). Anytime the result of one diagnostic test on two separate reading meets the criteria of diabetes, the diagnosis can be confirmed. Given that Mrs. G. first A1C came 6.9%, I will order her second A1C test. If her second A1C is ≥ 6.5%, diagnosis can be confirmed. Mrs. G lipid panel is abnormal. The fasting status is unknown, therefore fasting lipid panel need to be obtained before starting statin. The 2013 American College of Cardiology and American Heart Association (ACC/AHA) guideline recommended that fasting lipid panel is preferred, but not necessary to assess cardiovascular risk but is required before initiating statin therapy (Stone et al., 2014). The American Academy of Family Physicians [AANP] (2014) recommend moderate intensity statin therapy in adult age 40-75 years old with diabetes or moderate to high-intensity statin if LDL is 70-189 mg/dL without clinical ASCVD or diabetes. Mrs. G has meet the above criteria and needs to be treated with statin therapy, therefore a fasting lipid panel would be ordered. Mrs. G. elevated blood pressure reading must be confirmed by another elevated values on a separate day (). Home blood pressure monitoring or 24 hours ambulatory blood pressure monitoring along with another blood pressure reading on another visit is necessary to evaluate white-coat hypertension or other discrepancies (ADA, 2017). Mrs. G blood pressure is 120/80, which is elevated from normal but no need of antihypertensive therapy. Therefore, additional reading on next visit is recommended to keep good track of her BP. The diagnosis of obesity can be made based clinical evaluation, judgment and BMI, which measures the degree of adiposity. The BMI of 25-29.9 kg/m1 is considered overweight and ≥30 kg/m2 is considered obesity which is further classified as class I, II, and III (Garvey et al., 2016). If physical exam and BMI is questionable other test such as bioelectric impedance, air/water displacement plethysmography, or dual energy x-day absorptiometry can be ordered to further evaluate degree of obesity (Garver et al., 2016). Mrs. G. BMI is 33.6 kg/m2 which indicates class I obesity. At this visit I don’t consider ordering any test to diagnose obesity. It is important to consider the availability, cost, and outcomes of the data before using this diagnostic test. Mrs. G was previously diagnosed with arthritis and not presenting with arthritis complaints, therefore I don’t consider order any diagnostic test to examine her arthritis. The fast and preliminary screening for depression can be done by asking patient if she has felt down or hopeless and has little interest in doing things over past month. A positive response to one or both question may indicate positive depression. However, I will use the Patient Health Questionaire-2 (PHQ-2) to diagnose depression. The PHQ-2 is listed as key criteria for the diagnosis of major depression in the DSM-5 and is recommended the tool to screen major depression in the primary care setting (Ng, How, & Ng, 2016). Mrs. G. has classic symptoms of type 2 diabetes than Cushing’s disease, so my diagnostic test would focus to assess diabetes not Cushing’s disease at this time. If the diabetes is ruled out, then I will consider ordering late night salivary cortisol level and 24 hours urine free cortisol because these tests has high specificity and sensitivity. MRI can help to detect ACTH secreting pituitary adenoma by 15-30% and can be considered in patient with adenoma (Lonser et al., 2017). The above diagnostic test can be used to rule out Cushing’s disease. Medications Metformin 500 mg Sig: 1 tab PO daily disp# 30 RF: 0 Metformin monotherapy is a preferred initial agent in management of type 2 diabetes unless contraindicated (Crawford, 2017). It is shown to be effective in lowering hyperglycemia, linked to help loose weight, has fewer hypoglycemic occurrences, and is affordable and safe. The dose can be up titrated up to maximum dose of 2550mg/day or add second oral agent such as sulfonylurea, thoazolidinediones, dipeptidyl peptidase-4 inhibitor or SGLT2 inhibitor if targeted A1C level not met in 3 months (Crawford, 2017). Atorvastatin 40mg Sig: 1 tab PO daily disp# 30 RF: 0 The patient with diabetes aged 40 -75 with additional atherosclerotic cardiovascular disease risk factors are recommended high-intensity statin therapy (ADA, 2017). The clinical trial demonstrated significant reduction of ASCVD and CHD death in patient with diabetes treated with statin therapy (ADA, 2017). Tylenol 500 mg Sig: 2 tabs PO every 6 hours as needed for pain disp# 30 RF: 2 This is patient’s current medication. Acetaminophen helps to relieve mild to moderate pain due to arthritis and is relatively safer than nonsteroidal anti-inflammatory drugs (DiLonardo, n.d.). Multivitamin Sig: 1 tab PO daily disp#30 RF: 2 This is one of her current medication. Multivitamin daily provide supplement nutrients needed to support bone health. Education Type 2 diabetes is a condition characterized by deficient insulin secretion, impaired insulin function or combination of both which causes high blood sugar. It is a chronic condition that requires lifelong comprehensive health care. Lifestyle changes along with medication management is the key prevent complication and improve quality of life. The diagnosis of type 2 diabetes was confirmed based on the A1C results of ≥6.5%. in two separate tests. The risk of type 2 diabetes increases with aging, obesity, lack of physical activity, hypertension, hyperlipidemia, and racial and ethnic subgroups such as Hispanic/Latino (ADA, 2017). Your risk factors include obesity, increasing age, hyperlipidemia, and race/ethnicity. Along with lifestyle modification, metformin is the initial drug therapy. Some of the common side effects of metformin includes diarrhea, indigestion, nausea, vomiting, headache. It rarely causes hypoglycemia or lactic acidosis which can be fetal (Micromedex, 2017). The symptoms of hypoglycemia include shakiness, dizziness, sweating, lightheadedness, and fainting. It is important to carry snacks at all time especially during exercise due to change of hypoglycemia. Metformin is considered safe, affordable, and is shown to be effective in lowering your blood glucose level (Crawford, 2017). In addition, it will also help to lower your weight. Weight management is another important goal because it helps to reduce glucose, A1C, triglycerides, BP, LDL, TC, and increase HDL (Crawford, 2017). The weight loss of 5% or greater is beneficial but ≥ 7% is optimal to get desirable effects (Crawford, 2017). The combination of diet, physical activity, and behavioral therapy is recommended to help you manage your weight. It is important to cut down food high in calorie. Your recommended calorie per day is 1200 to 1500 kcal/day (Crawford, 2017). The patient with type 2 diabetes and obesity need more than 150min/week of moderate to vigorous physical activity, 2 to 3 session/week of resistance exercise, and reduce prolong sitting to no more than 90 minutes (Crawford, 2017). Microvascular complication such as nephropathy, retinopathy, and neuropathy are some of the common complication of diabetes. The renal function will be monitored periodically to evaluate kidney function. Baseline eye examination is recommended at the diagnosis of type 2 diabetes (Crawford, 2017). Diabetic neuropathy is one of the common and irreversible complication, therefore annual screening for peripheral neuropathy is recommended. Foot care is another important thing to consider because ulcers and amputation are quiet common complications. It is important to inspect feet daily, use proper fitting shoes, and proper nail care. Hyperglycemia, hypoglycemia, hyperglycemic hyperosmolar nonketotic syndrome (HHNS) and diabetic ketoacidosis are some of the warning signs that require immediate medical assistance. If you experience dry mouth, change in vision, nausea, fatigue, or increased urination or thirst, change in mental status, shortness of breath, or become sick, seek medical assistance right away. Be sure to wear necklace or bracelet that tells you are diabetic in case of medical emergency. Diabetes and hyperlipidemia increased the risk of ASCVD. Hyperlipidemia simply means high level of lipids such as cholesterol, triglycerides, and fat circulating in the blood. These fats can enter into the arteries and may develop plaque known as atherosclerosis which can lead to health disease and stroke (Moneta, n.d.). It is mostly caused due to high fat diet, sedentary lifestyle, obesity, diabetes (Moneta, n.d.). The lipid panel test can be using to confirm the diagnoses. Diet low in saturated fat, trans fat, increase viscous fiber, plant stanols, omega 3 fatty acid, daily exercise, weight loss, and diabetes management are important to reduce the risk of ASCVD risk (Crawford, 2017). The fasting lipid profile is recommended before starting statin therapy. Statin therapy is shown to be effective in lowering LDL, VLDL, and increase HDL. Atorvastatin is a high-potent statin drugs used to reduce total cholesterol, LDL, and familial hypercholesterolemia (Micromedex, 2018). Atorvastatin may cause diarrhea, indigestion, hepatitis, arthralgia, headache, insomnia, and urinary tract infection (Micromedex, 2018). Hyperlipidemia has no symptoms, but it increases the risk of heart disease and stroke. Any chest pain, shortness of breath, change in mental status, weakens of one side of body, change in vision must call 911 immediately. Obesity can cause insulin resistance. It is commonly caused due to excessive intake of calorie. The diagnosis of obesity can be made by calculating BMI. The BMI of 30.0-34.9 is classified as class I obesity (Crawford, 2017). The high intensity physical activity of 200- 300min/week, calorie restricted diet, and close monitoring of weight, and trained medical professional is recommended as an initiation therapy. There are FDA approved drugs that can be used to lose weight. Diet, exercise, and glucose-lowering agent can be used as an initial weight management therapy. The weight loss of 1 to 2 pound per week with the goal of reducing 10- 15% (Crawford, 2017). There is no identifiable warning sign of the diagnosis that need immediate attention. The patient with obesity may experience obstructive sleep apnea, therefore sleep study may be recommended. The blood pressure of 120-129 systolic and <80 diastolic is falls under elevated blood pressing as per the new ACC/AHA guidelines (American College of Cardiology, 2017). The guidelines recommend rechecking the blood pressure on a separate day. The elevated reading on minimum of two separate reading on two separate occasion is required to diagnose hypertension. The blood pressure of 130/80 is a targeted blood pressure for individual with risk of cardiovascular disease (American College of Cardiology, 2017). The patient with blood pressure of > 120/80 mmHg is recommended to modify lifestyle, lose weight, DASH diet, reduce sodium, and increase potassium intake, limit alcohol, increase physical activity, and (Crawford, 2017). No pharmacological therapy is required at this time. Referral After complete evaluation of Mrs. G and confirm the diagnosis of type 2 diabetes, she will be referred to nutritional therapist to help her prepare diabetic meal that has appropriate nutrients required for body. Diabetic retinopathy is one of the common complication of diabetes that requires initial evaluation, thus she will be referred to ophthalmology for eye exam (Crawford, 2017). Diabetes can cause periodontal disease so referral to dentist is recommended. Diabetic patient has 1.5 times more likely to develop foot ulceration or charcot foot which affects the midfoot joints which may require non-weight bearing cast or special braces (Centers for Disease Control and Prevention [CDC], n.d.) Therefore, referral to podiatrist to educate patient about foot complication and foot care can prevent complication and improve foot outcomes (CDC, n.d.). Diabetes increase the risk of anxiety and depression. About 25% patient with diabetes are reported to be depressed or has depressive symptoms (Crawford, 2017). Diabetes can be life changing. In order to combat with the lifechanging medical problem patient may benefits from early mental health support, counselling, and follow up. In addition, patient benefit from referral to community resources so that different community program can help to share and manage diabetes as well as obesity and hyperlipidemia. Diabetes self-management education and support group referral is important to increase self-awareness about the disease as well as to manage self at home (Crawford, 2017). Referral to diabetes educator for initial detail education about the diagnosis, discuss the importance of healthy eating, exercise, and review medication and ongoing education to support for long term management. Follow Up The follow up visit depends on the how patient tolerates the medication and response to therapy. The recommended visit for newly diagnosed patient would be 1 month and follow up A1C would be done in 3 months after initiation of therapy. Patient who tolerates therapy and respond well can have follow up visit in every 3 months (ADA, 2015). At 1 month follow up visit she will have recheck for her BP, weight, lipid panel as well as comprehensive history and physical exam. It is recommended to be in touch with patient every week if making any big changes to diabetes management plan (ADA, 2015). Once she is stabilized her regular visit would be every 3 months. Medication Cost Metformin $4/month (goodrx.com) Atorvastatin 10.11/month (goodrx.com) Tylenol Arthritis approximately 3.49/month- $10.47 for 100 CT (goodrx.com) Women’s daily multivitamin approximately 2.66/month- 7.97 for 100 CT (Walmart.com) An estimated monthly cost would be $20.26. It is important to assess her financial status and give patient a round figure of how much is she expected to spend on medication every month so that patient will be prepared which increases medication compliance. Goodrx.com is an excellent tool to use to determine cost of most of the drugs. There is some pharmacy that don’t take some insurance, or some insurance don’t cover every medication or brand medication, therefore it is important to talk to pharmacy before prescribing mediation to reduce financial burden on patient. I will explain patient that she can use goodrx.com to compare the price of the drugs. However, it is also important to consider one pharmacy to refill medication to prevent drug adverse reaction due to multiple medication as well as it is convenience. I think it is important inform patient about the prices and options and I can see myself using this price resources in the future with my patients. I strongly believe that patient will appreciate such discussion as well. SOAP Note Patient Information: MRS. G, 55, Female, Hispanic, S. CC: Patient presented with the complaints of fatigue, no energy for past 3 months. Her weight has gained since last year but noticed increased 3lb despite exercise, increase hunger and thirst, and frequency of bathroom trips during day and night. HPI: Onset: 3 months ago Location: Generalized Duration: continuous for past 3 month Characteristics: Associated with feeling fatigue, no energy, weight gain, increased hunger, thirst, and increased urinary frequency Aggravating Factors: Exercise worsen the hunger and thirst Relieving Factors: none reported Treatment: None reported Severity: fatigue and nausea and preventing participation in usual activities Current Medications: Tylenol 500mg, 2 tabs daily for knee pain and multivitamin 1 tab daily supplement. Allergies: NKDA, allergic to cats and pollen. No latex allergy PMHx: Left knee arthritis, chicken pox and mumps as a child. Immunization are up to date. Last tetanus date not available. GYN Hx: G2P1, 1 SAB, 1living child, full term weight 9lb 2 oz. LMP 15 months ago. Last PAP smear normal Soc Hx: She is a part time planning coordinator works from home. She is married. No history of tobacco use, or illicit drug use. She drinks 1-2 glasses of wine on the weekends. She reported to use seat belts all the time riding on car and have working smoke detectors in the house. Fam Hx: Both parents alive, mother has HTN, father has high cholesterol. She has a living child with no medical issue. No siblings. ROS: CONSTITUTIONAL: weight gain and fatigue. No fever, chills, and weakness HEENT: Eyes: No visual loss, blurred vision, double vision or yellow sclera. Ears, Nose, Throat: No hearing loss, sneezing, congestion, runny nose or sore throat. SKIN: No rash or itching. CARDIOVASCULAR: No chest pain, chest pressure or chest discomfort. No palpitations or edema. RESPIRATORY: No shortness of breath, cough or sputum. GASTROINTESTINAL: No anorexia, nausea, vomiting or diarrhea. No abdominal pain or blood. GENITOURINARY: Increased frequency, no burning. Last menstrual period, 03/03/2017. NEUROLOGICAL: No headache, dizziness, syncope, paralysis, ataxia, numbness or tingling in the extremities. No change in bowel or bladder control. MUSCULOSKELETAL: No muscle, back pain, joint pain or stiffness. HEMATOLOGIC: No anemia, bleeding or bruising. LYMPHATICS: No enlarged nodes. No history of splenectomy. PSYCHIATRIC: No history of depression or anxiety. ENDOCRINOLOGIC: No reports of sweating, cold or heat intolerance. Reported polyuria, polyphagia, and polydipsia. ALLERGIES: Allergic to cats and pollen. No history of asthma, hives, eczema or rhinitis. O. Physical exam: GENERAL: Obese female in no acute distress. Patient is well groomed, alert, oriented, and cooperative. VITAL SIGNS: BP, 129/80, pulse 80 regular; respirations 16, regular. Height 5’2.5”, weight 185 pounds. HEENT: Head normocephalic. Hair thick and distributed throughout the scalp. HEENT: Eyes without exudate, sclera white. Wears contacts. Tympanic membranes gray and intact with light reflex noted. Pinna and tragus nontender. Nares patent without exudate. Oropharynx moist without erythema. Teeth in good repair, no cavities noted. Neck supple. Anterior cervical lymph nontender to palpation. No lymphadenopathy. Thyroid midline, small and firm without palpable masses. SKIN: Pink, warm and dry. Hair on head is thick and equally disturbed. CARDIOVASCULAR: S1 and S2 RRR. No murmurs or rubs. LUNGS: Clear to auscultations bilaterally. Respirations unlabored. ABDOMEN: Soft, round, nontender. Positive bowel sounds present in all four quadrants. No bruits. No CVA tenderness. Diagnostic results: CBC: WBC 6,000/mm3, Hgb 12.5gm/dl, Hct 41%, RBC 4.6 million, MCV 88 fl, MCHC 34 g/dl, RDW 13.8% Ua: pH 5, SpGr 1.013, Leukocyte esterase negative, nitrites negative, 1+ glucose; small protein; negative for ketones CMP: Sodium 139, Potassium 4.3, Chloride 100, CO2 29, Glucose 126, BUN 12, Creatinine 0.7, GFR est non-AA 94 mL/min/1.73, GFR est AA 101mL/min/1.73, Calcium 9.5, Total protein 7.6, Bilirubin, total 0.6, Alkaline phosphatase 72, AST 25, ALT 29, Anion gap 8.10, Bun/Creat 17.7, Hemoglobin A1C: 6.9 %, TSH: 2.35, Free T4 0.8 ng/dL, Cholesterol: TC- 230mg/dl, LDL- 144mg/dl, VLDL- 36mg/dl, HDL- 38mg/dl, triglycerides- 232. EKG: Normal sinus rhythm A. Primary diagnosis: Type 2 diabetes mellitus (E11): Mrs. G. presenting symptoms of very fatigue, increased hunger, thirst, and urinary frequency, and weight gain are the classic symptoms of type 2 diabetes. The risk factors of type 2 diabetes that are pertinent to this patient includes obesity, age, Hispanic, obesity with the BMI of (), hyperlipidemia, and elevated blood pressure. The laboratory findings of blood glucose of 126, A1C 6.9%, and 1+ glucose in urine are pertinent positive to the primary diagnosis. Her A1C meet the criteria for diagnosis so as her BG of 126 if it was fasting, but fasting status is unknown (ADA, 2017). Secondary diagnosis (es): Mixed Hyperlipidemia (E78.2): Her total cholesterol is 230 ml/dL which falls under borderline high cholesterol, her HDL which is the good cholesterol should be >40mg/dl is low in 38 mg/dL, she has high triglycerides i.e., 232 ml/dL, LDL 144 mg/dL which is at borderline, and high VLDL. Her risk factors for hyperlipidemia includes obesity and family history of high cholesterol. The pertinent negative finding includes, xanthelasma, arterial bruits, or vascular claudication but patient with hyperlipidemia are usually asymptomatic. Obesity (E66.9): The pertinent positive finding that help to diagnose obesity is her BMI which is 33.3. The BMI of 30.0 to 34.9 is classified as class I BMI, as per the classification she has class I obesity (Al-Goblan, Al-Alfi, & Khan, 2014). HTN (I10): Her blood pressure of 129/80 is classified as elevated BP by ACC/AHA guidelines. Her positive risk factors include obesity, hyperlipidemia, family history of hypertension. Her pertinent negative finding includes no report of dizziness or lightheadedness. Left knee arthritis (M17.12): This is her past medical history and she currently takes pain medicine to help with her knee pain. No pertinent data reported. Differential Diagnoses: Depression (F33.0): Her complaints of being overly fatigue, tired, weight gain is pertinent positive information. She will need detailed examination as well as depression screening to consider this diagnosis. The pertinent negative findings includes no change in sleep and feeling of hopelessness, down or depression are not reported. Cushing's disease (E24.9): The signs and symptoms include obesity, diabetes, hypertension, moon facies, weight gain, increased thirst, fatigue, glucose intolerance, and facial plethora. Cushing’s disease may lead to diabetes, hypertension, obesity, osteoporosis, and vascular disease if not treated appropriately. Mrs. G obesity, hypertension, diabetes, fatigue could be related to Cushing’s disease. Pertinent negative finding include no moon face, red cheeks, excessive weight gain in torso, or excessive hair growth which are positive with Cushing’s disease, P. Diagnostics: Repeat A1C to confirm Type 2 diabetes. Fasting blood glucose and fasting lipids to ensure accuracy of results as well as to determine appropriate statin therapy for hyperlipidemia. Recheck BP on separate occasion along with home BP monitoring. Further diagnostic testing that measures skinfold thickness to classify her obesity. Depression screening and assessment to demine depression. 24 hours urine cortisol level or blood cortisol level to diagnosis Cushing’s. Medications: Metformin 500 mg BID PO daily for high blood sugar (Metformin is initial therapy of type 2 diabetes and it has less chance of developing hypoglycemia. Atorvastatin 40mg PO daily for hyperlipidemia (The ACC/AHA recommend moderate to high intensity statin for hyperlipidemia. Tylenol 500mg, 2 tab PO daily for knee pain. Continue home medication Multivitamin 1 tab PO daily. Continue home medication. Education: Type 2 diabetes is a chronic disease caused by deficiency in the beta cell insulin production or insulin resistance. It is diagnosed based on the clinical presentation as well as the A1C level of ≥ 6.5%. Obesity, hypertension, hyperlipidemia, age, genetic predisposition play role in the initiation and progression of the disease. Modifying lifestyle by increasing physical activity, control diet, and reduce weight. The goal of the treatment is to maintain A1C < 6.5 and maintain optimal health and quality of life. A weight reduction of 5% is recommended. It is important to stick with diet, exercise, and pharmacological therapy recommended to better control and prevent future complication. The complication of diabetes can be debilitating so it is important to educate to assess skin and feet daily and wear proper fitting shoes. Metformin is an initial pharmacological therapy to manage type 2 diabetes. It is relatively safe drugs but may cause hypoglycemia. So, look out of any dizziness, sweating, confusion, or change in mental status. It is important to visit doctor for even minor illness because not eating or change in eating habit, and illness may alter insulin needs and may cause hypoglycemia or diabetic ketoacidosis. Be sure to eat regularly, don’t skip meal, and carry snakes at all time. Hyperlipidemia is a condition in which the circulating fat increased leading to atherosclerotic plaque formation which may cause heart attack and strokes. Loosing weight is the key to lower the cholesterol which also beneficial for diabetes. Diet is the number one cause of hyperlipidemia and obesity, thus eat food low in saturated and trans-fat, increased exercise and physical activity helps to reduce cholesterol. Atorvastatin is a high potent statin used to treat hyperlipidemia. Some of the side effects includes muscle ache, arthralgia, diarrhea etc. Obesity is caused due to increased calorie intake. Limiting calorie intake to 1200 to 1500 Kcal per day and daily exercise is the key to reduce weight. The weight loss of 1 to 2 lb per week is safe. There are variety of weight watcher application that can be used to keep track of food and calorie intake. Limit prolong sitting, physical activity of 200 to 300 min/week, or finding trained professional are some tips to successfully loose weight. The BP is elevated from normal, but it needs to be rechecked at home as well as in the clinic on next visit. Modifying lifestyle, increased activity, DASH diet can help to lower BP. Referral/Consults: Referral to nutrition therapy to help plan appropriate diabetic meal. Diabetic educator can help to understand the disease, management, and ongoing education to support patient. Referral to ophthalmologist for initial and annual eye exam, podiatry to help fit shoe or braces, psychiatrist or behavioral counselor to prevent depression, anxiety, and provide ongoing mental support. Referral to local community services to help connect with people who are undergoing similar issue as well as to utilized resources to help manage their illness. Follow up: Follow in 1 month to check overall health, BP, medication side effects, and response to pharmacological and nonpharmacological therapies. Follow up laboratory test such as A1C, lipid panel, and blood pressure can be done. Adjust medicine and refill prescription as needed. Once adjustment to therapy maintenance follow up in every 3 months. References Al-Goblan, A. S., Al-Alfi, M. A., & Khan, M. Z. (2014). Mechanism linking diabetes mellitus and obesity. Diabetes, metabolic syndrome and obesity: targets and therapy, 7, 587. doi: 10.2147/DMSO.S67400 American Academy of Family Physicians. (2014). Treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults. Retrieved from https://www.aafp.org/patient- care/clinical-recommendations/all/cholesterol.html American College of Cardiology. (2017). New ACC/AHA high blood pressure guidelines lower definition of hypertension. Retrieved from https://www.acc.org/latest-in- cardiology/articles/2017/11/08/11/47/mon-5pm-bp-guideline-aha-2017 American Diabetes Association. (2017). Cardiovascular disease and risk management. Diabetes care, 40(1), S75-S87. https://doi.org/10.2337/dc17-s012 American Diabetes Association. (2017). Classification and diagnosis of diabetes. Diabetes Care, 40(1), S11-S24. https://doi.org/10.2337/dc17-S005 Atorvastatin. (2018). In Micromedex (Chamberlain College of Nursing Library ed.) [Electronic Version]. Greenwood Village, CO: Truven Health Analytics. Retrieved from http://www- micromedexsolutions-com Centers for Disease Control and Prevention. (n.d.). What podiatrist would like team members to know about foot health and diabetes. Retrieved from https://www.cdc.gov/diabetes/ndep/pdfs/ppod-guide-podiatrists.pdf Crawford, K. (2017). Review of 2017 diabetes standards of care. Nursing Clinics of North America, 52(4), 621-663. https://doi.org/10.1016/j.cnur.2017.07.010 DiLondardo, M. (n.d.). Taking acetaminophen safety: A popular drug for arthritis pain relief is safe, if you use it wisely. Arthritis Foundation. Retrieved from https://www.arthritis.org/living-with-arthritis/treatments/medication/drug- types/analgesics/acetaminophen-safety.php GoodRx. (2018). Medication search. Retrieved from https://www.goodrx.com/ Karr, S. (2017). Epidemiology and management of hyperlipidemia. The American Journal Of Managed Care, 23(9 Suppl), S139-S148. Kennedy-Malone, L., Fletcher, K., & Plank, L. (2014). Advanced practice nursing in the care of older adults. Retrieved from https://bookshelf.vitalsource.com Lonser, R. R., Nieman, L., & Oldfield, E. H. (2017). Cushing's disease: pathobiology, diagnosis, and management. Journal of neurosurgery, 126(2), 404-417. Doi: 10.3171/2016.1.JNS152119 McCance, K. L., Huether, S. E., Brashers, V. L., & Rote, N. S. (2013). Pathophysiology: The biologic basis for disease in adults and children (7th ed.). St. Louis, MO: Mosby. Metformin. (2018). In Micromedex (Chamberlain College of Nursing Library ed.) [Electronic Version]. Greenwood Village, CO: Truven Health Analytics. Retrieved from http://www- micromedexsolutions-com Moneta, G. L. (n.d.). Hyperlipidemia. Society for Vascular Surgery. Retrieved from https://vascular.org/patient-resources/vascular-conditions/hyperlipidemia National Diabetes Education Initiative. (2016). Diabetes management guidelines. Retrieved from http://www.ndei.org/ADA-2013-Guidelines-Criteria-Diabetes-Diagnosis.aspx.html Ng, C. W. M., How, C. H., & Ng, Y. P. (2016). Major depression in primary care: making the diagnosis. Singapore medical journal, 57(11), 591. Doi: 10.11622/smedi.2016174 Stone, N. J., Robinson, J. G., Lichtenstein, A. H., Merz, C. N. B., Blum, C. B., Eckel, R. H., ... & McBride, P. (2014). 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology, 63(25 Part B), 2889-2934. Wallmart. (2018). One a day multivitamin. Retrieved from https://www.walmart.com/ip/One-A- Day-Women-s-Multivitamin-Tablets-200-ct/10311437 [Show More]
Last updated: 1 year ago
Preview 1 out of 24 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Feb 07, 2023
Number of pages
24
Written in

Additional information
This document has been written for:
Uploaded
Feb 07, 2023
Downloads
0
Views
58

PSY 101 Week 9 Assignment Case Study 3.png)
Activity 1 Case Study 1.png)