*NURSING > STUDY GUIDE > NUR 2633 MATERNAL NEWBORN STUDY GUIDE 2020 WITH QUESTIONS,100% CORRECT (All)
NUR 2633 MATERNAL NEWBORN STUDY GUIDE 2020 WITH QUESTIONS,100% CORRECT
Document Content and Description Below
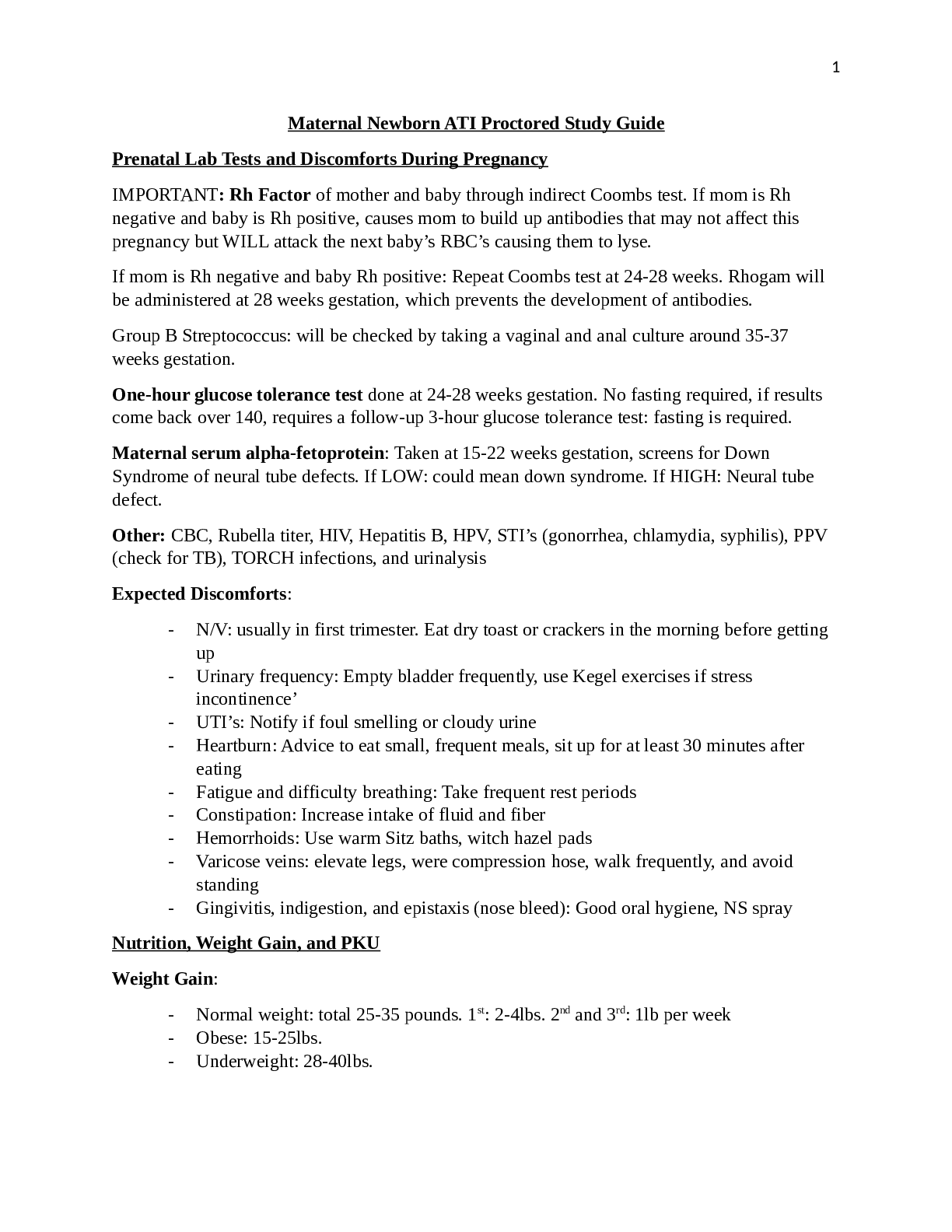
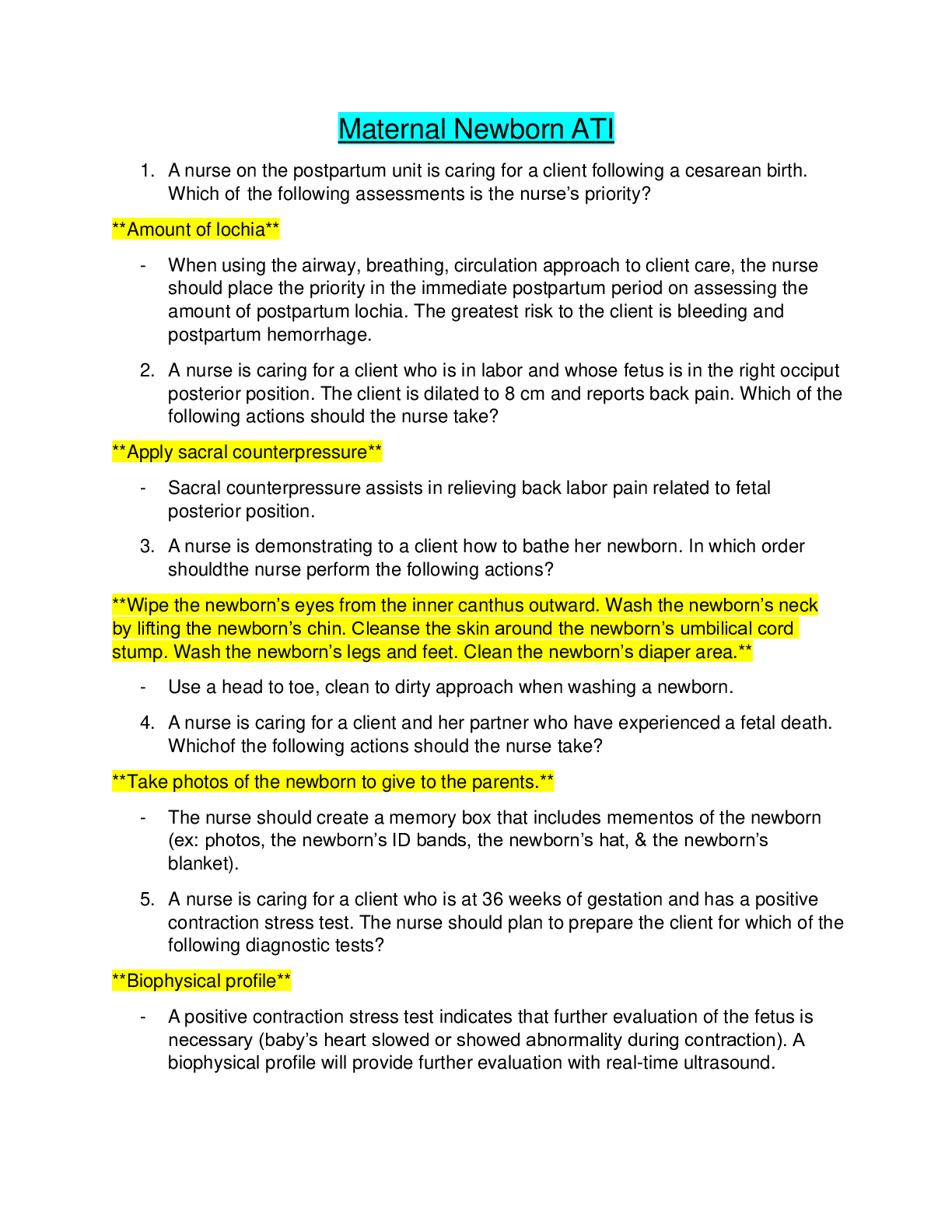
NUR 2633 MATERNAL NEWBORN STUDY GUIDE 2020 WITH QUESTIONS Women’s health encompasses breast care, GYN exams, and assessments. Be comfortable with the parameters of education for a. Breast educatio... n- b. Fluctuating hormone levels during the monthly cycle cause changes in breast tissue. i. Following menstruation, when hormone levels are at their lowest, the breast tissue is smooth and nontender. ii. As estrogen levels increase mid-cycle, breasts may become more sensitive. Also, just before menstruation, when progesterone is elevated, the breasts become swollen and tender, with palpable nodules. c. The area between the breasts has several oil and sweat glands, creating an atmosphere conducive to the growth of bacteria. d. Pregnancy darkens the color of the nipple, which is an enhancement for the breastfeeding baby. This darker color does not disappear after pregnancy. e. Mammography (mammogram) - is an MRI of the breast tissue used to detect abnormalities (tumors and cysts). i. Routine mammograms should be performed every 2 years for women ages 50-74 ii. Some gynecologists recommend mammograms begin a yearly mammogram screening at age 40. Self-breast exams- iii. Should be performed every 1-3 years for age 20-29 and every year for women over 40. iv. Technique: Breast Self-Examination (ACS, 2011d) p lxix 1) Lie down on your back and place your right arm behind your head. Remember, this step is done while lying down. In this position, the breast tissue spreads evenly over your chest wall and is as thin as possible. This makes it much easier to feel all of the breast tissue. 2) Use the pads of your three middle fingers on the left hand to feel for lumps in the right breast. Use overlapping dime-sized circular motions of the finger pads to feel all of the breast tissue. 3) When feeling the breast tissue, you will use three different levels of pressure. Light pressure is needed to feel the tissue closest to the skin. Medium pressure allows you to feel a little deeper, and firm pressure allows you to feel the tissue closest to your chest and ribs. o Remember, it is normal to feel a firm ridge in the lower curve of each breast. If you feel anything else out of the ordinary, be sure to tell your health-care practitioner. It is important to use each pressure level to feel all of the breast tissue before you move on to the next spot. 4) Move around the breast in an up and down pattern, starting at an imaginary line drawn straight down your side from the underarm and moving across the breast to the middle of the chest bone (sternum, breastbone). o Make sure that you check the entire breast area going down until you feel only your ribs and then up to the neck or collarbone (clavicle). Using the up and down, or vertical, pattern is probably the most effective way to examine the entire breast without missing any breast tissue. 5) Repeat step 4 on your left breast, putting your left arm behind your head and using the finger pads of your right hand to do the exam. 6) Stand before a mirror, place your hands on your hips, and press down firmly. In the mirror, look at your breasts for any changes of size, shape, contour, or dimpling or redness or scaliness of the nipple or breast skin. (Pressing down on your hips contracts the muscles of the chest wall and enhances any breast changes). 7) Sit or stand with your arm only slightly raised so that you can easily feel the underarm area. Do this on each side, feeling for lumps or thickened areas. (Raising the arm straight up causes a tightening of the tissue and makes it more difficult to examine). Normal menstrual cycle – v. Occurs approximately every 28 days (calculated from the first day of last period to the first day of the next), lasts for 2-7 days vi. Bleeding can be light to heavy, or variate between the two depending on stage of menstruation. What is the most common complaint with the menstrual cycle, and complications? vii. Dysmenorrhea-painful menstruation 1. Production of prostaglandins 2. Tx: NSAIDS—prohibit prostaglandins viii. PMS-fluctuation of estrogen/progesterone, hyperprolactinemia increased prolactin secondary to breast development. 1. Tx: exercise, rest, sleep, diet-decrease salt, sugar, caffeine ix. Endometriosis-growth of endometrial tissue outside of the uterus 1. During the ischemic menstrual cycle the misplaced tissue breaks down/bleeds into surrounding tissue—inflammation—gets trapped causes cysts. 2. Cycles of this result in scarring, fibrosis, and adhesions—binding organs together—increased abdominal pain, and infertility a. S/S: bleeding, pain b. Dx: palpation, vaginal ultrasound, laparoscopy c. Tx: pain meds, hormone therapy-shrinks endo tissue, surgery, oral contraception • Colorectal screenings, colonoscopy, fecal occult tests are all also important for women. STI’s and risks f. What is HPV? i. Human papilloma virus (HPV) in an STI which can cause cellular changes of the cervix- leading to cervical cancer. ii. HPV can also lead to the development of papillomas- benign growths of the genital and anal regions. iii. Vaccine = Gardasil 1. Protects against HPV types 6, 11, 16, and 18. Newly approved vaccine (Gardasil 9) covers HPV 6, 11, 16, and 18, as well as 31, 33, 45, 52, and 58- which are responsible for 1 in 5 cases of HPV-associated cervical cancer. 2. Consists of 3 IM injections given over 6 months at 1, 2, and 6 months 3. Can be given to females age 9-26 years old, boys can also receive the vaccine from age 9-15. 4. Nurses- teach the patient to be sure to return on time for each vaccine series, and continue to have routine cervical cancer screenings. Contraception - Forms of birth control – good subject for your postpartum patients as well – know them g. Natural family planning- h. Coitus interruptus- “pull out method” i. Abstinence j. Breast feeding—maintains progesterone levels, keep from ovulating k. Diaphragm- dome shaped, spermicide gel is placed inside the dome—inserted into vagina 6 hrs before intercourse and left in for 6 hrs after. l. Cervical cap- thimble shaped, spermicidal gel placed inside. Placed against cervix m. Condoms n. Spermicidal gels o. Hormonal methods i. Ethinyl estradiol (estrogen)-prevents the release of FSH from the anterior pituitary gland. When FSH levels are low the ovarian follicle doesn’t form and ovulation is prevented. ii. Progestins-inhibit LH surge-required for ovulation (used with estrogen) 1. Progesterone only-thickens cervical mucus which creates a hostile environment and endometrial atrophy so the egg wont implant. iii. Low-dose progestin only- (mini pill) thickens cervical mucus, can be taken while breast feeding—won’t enter breast milk. Patient teaching for birth control iv. Takes 7 days to start being effective with the initial pack. So will need to use a 2nd birth control method. v. Recheck in 3 months when first started vi. Take every day at roughly the same time vii. Begin a new pack on the same day (always) usually a Sunday. viii. If missed a dose, take 2 pills the following day. p. Patch-est/prog- 3 weeks patch on, 1 week patch off (in order to have menses). i. Placed on the abd, buttocks, outer arm, or upper torso (EXCEPT the breast area). 1. Patient education: a. Rotate sites (weekly or monthly depending on patch) b. If removed due to damage for longer than 24 hours, replace with a new patch and use 2nd birth control method x 7 days. q. Vaginal ring-est/prog- placed on the 5th day of the menstrual cycle. Leave in x3 weeks, remove x 1 week. Insert new ring at same time of day as the last ring. r. Emergency contraception- est/prog, or prog only (preferred) s. Plan B: (levonorgestrel – synthetic progestin) Emergency contraception – know education. i. 1 pill OTC, best used when taken within 72 hours, not effective after 120 hours 1. If implantation has occurred, this won’t work, patient can still become pregnant. 2. Won’t harm embryo if taken after fertilization has occurred. a. Side effects = N/V, breast tenderness, minor vaginal bleeding. ii. IUD-prevents implantation-can be used up to 5 days after unprotected intercourse. MD must insert 1. Don’t use if raped, or have risk for pelvic infections/STI’s 2. Only works if ovum has not implanted t. Injectable hormone- Depo-Provera (medroxyprogesterone acetate) i. Progestin only-lasts 3 months, first dose on day 5 of menses ii. Suppresses ovulation/alters cervical environment 1. Patient education: decreases bone density so need to increase calcium intake and do weight bearing exercises, Q3mo see MD for injection u. Subdermal hormone implant-Implanon—effective x 3 years. i. Single rod implanted into upper arm—progesterone only v. IUD-inserted into uterus, left in place~ i. Theory: causes a sterile inflammatory response that results in a spermicidal intrauterine environment. Few sperm are able to reach the fallopian tubes—if they do the IUD causes an unfavorable environment for implantation. 1. Mirena—progesterone only—replace Q5years 2. ParaGard- copper wire—replace Q10 years 3. Pt education: inserted during menses w. Sterilization-Permanent i. Female-tubal ligation ii. Male-vasectomy-vas deferens is cauterized/clipped/cut ***Remember birth control choice should be based on a patient’s lifestyle – if she cannot swallow pills do not offer oral contraception.*** Preconceptual care- is provided for a means to identify risks and provide education – not to establish who should become pregnant. Preconception-before pregnancy ❖ Menstrual/medical history, physical assessment, and pelvic exam. ❖ Labs, pap test, childhood illnesses, STI’s, genetic testing, lifestyle habits Please identify pregnancy history – G, T, P, A, L – know how to complete this given each women’s obstetrical history. • GTPAL a. G - Gravida. This is the number of times a woman has conceived, including any current pregnancy. b. T - Term births. This is the number of times a woman has carried a pregnancy to at least 37 weeks gestation and delivered. c. P - Preterm births. This is the number of times a woman has delivered before 37 weeks gestation, but after 20 weeks gestation. d. A - Abortions. This is the number of times a woman has lost a pregnancy, whether it was elective or spontaneous (miscarriage), before 20 weeks gestation. e. L - Living children. This term states 'living children,' but what it really is referring to is live births. GTPAL System G—Gravid T—Term pregnancies (#) P—Preterm deliveries (#) A— Abortions (spont/induced) (#)L— Living children (#) Example: A mom comes in for her monthly appointment. She is 32 weeks pregnant. She has with her, her two children. The boy was born at 28 weeks and is 7 years old, the girl was born at 41 weeks and is 3 years old. She denies any abortions. She had another baby girl born at 38 weeks, but died from SIDS at 3 months of age. Her GTPAL: G—4 (pregnant x1, living children x2, baby that died x1) T—2 (2nd child alive, and 3rd child that died) P—1 (first born) A—0 (denies any) L—2 (a 7 year old and a 3 year old) 4-2-1-0-2 Pregnancy Classification Gravid—being pregnant Gravidity--# of pregnancies (including current one) Nulligravid-0 no pregnancies Primigravid-1 pregnancy (first time pregnant) Secundigravid-2 pregnancies (second time pregnant) Multigravid-3+ pregnancies Parity-# of pregnancies carried to point of viability (~20 weeks) Signs of pregnancy: Presumptive~subjective Probable~objective Positive Amenorrhea Abdominal enlargement Fetal heart beat N/V (morning sickness) Uterine asymmetry Visualization of fetus Polyuria (uterus press on bladder) Hegars sign-softening of lower uterine segment Fetal movements palpated by practitioner Breast tenderness Goodell’s sign Quickening (2d trimester) Chadwick’s sign Stretch marks Braxton Hicks (2nd trimester) Fatigue Ballottement-passive movement of unengaged fetus Can you date a pregnancy using Naegele’s Rule? Estimate Date of Birth = EDB *each trimester is 14 weeks long* *3 trimesters* Term 37-42 weeks Preterm <37 weeks Post term >42 weeks Naegle’s Rule Based on 28 day cycle From date of last menstrual period (LMP) Minus (-) 3 months, Add (+) 7 days Add (+) 1 year if necessary Example: June (6) 3, 2017 -3 +7 +1 March (3) 10, 2018 Est. DOB Can you measure fundal height? Know the normal parameters of fetal growth. When does the uterus move out of the bony pelvis? At approximately 12 weeks gestation When does it reach the height of the umbilicus? At approximately 20 weeks gestation. When are fetal heart tones audible with a Doppler? Between 8-12 weeks gestation- ultrasound can allow for earlier detection than Doppler. What are the parameters and what does it mean if the fetus falls outside those parameters? ***Normal FHR = 110-160 BPM Assessment of fetus during pregnancy and labor a. Fetal HR HR tones best heard over fetal back when fetus is flexed. i. Baseline FHR: 110-160bpm ii. Tachy: >160 x 10min 1. Hypoxia, maternal fever, tocolytics, fetal anemia, infection iii. Brady: <110 x 10min 1. Hypoxia, beta blockers, maternal hypotension, prolonged umbilical cord compression iv. Variable: adequate oxygen neuro pathway from brain to heart. HR irregular pattern-interplay with SNS/PNS Leopold’s maneuvers: Assist mother in emptying her bladder first to avoid discomfort Fetal development from the conception through the embryonic (critical) period, to the placental development and beyond. – It is all about the placenta. f. Fertilization i. Ovary ovum ~ meets sperm ovum then forms a barrier to keep another sperm from entering. The zygote has formed! ii. Zygote goes into a morula then a blastocyte and implants in uterus (7-8 days later). iii. Blastocyst ~ inside is a mass of cells (embryoblast) (outer layer is trophoblast) iv. Chorion/Chorionic villi/Placenta develop from the trophoblast. v. Blood vessels begin to form~ week 3~ primitive fetoplacental circulation is established. vi. The placenta is well established by weeks 8-10. Fetal Growth and Development • Major organs formed during 1st 8 weeks of gestation • Weeks 0-8} embryo • Weeks 9-40} fetus Weeks 1-4 ❖ Neural tube develops—defective closure results in neural tube defects Weeks 17-20 ❖ Quickening-maternal awareness of fetal movements ❖ Vernix caseosa-thick, cheese like material on fetus skin. Protects fetus from amniotic fluid ❖ Lanugo-fine, downy hair. Present on fetus at 20th week ❖ Brown fat-keeps vital organs, spinal cord warm and protected Weeks 21-25 ❖ 24 weeks lungs secrete surfactant-substance decreases surface tension in alveoli. Necessary for survival after birth Weeks 26-29 ❖ Fetus may survive if born-lungs can breathe air ❖ CNS can regulate body temperature What risk factors will impede placental perfusion to the baby? Teratogens: (Chemicals that when ingested or used during pregnancy, can result in serious birth defects of the embryo or fetus) vii. Different teratogens can cause defects at different stages of development ❖ Fat soluble vitamins (A-retinol) CV agents ❖ Alcohol, smoking Retinoids- Accutane ❖ Caffeine Hormones ❖ Cocaine, heroin, opiates Antineoplastic agents ❖ Anticonvulsants Certain antibiotics ❖ Warfarin Thalidomide ❖ Mercury Medications Teratogens-affects cellular development in embryo/fetus. 3rd week-3rd month-greatest impact 3rd trimester-most vulnerable-cognitive impairment FDA Class A. Safe to take B. Fetal risk undetected C. Fetal risk undetected, Animals identified as a risk D. Risk identified~benefits need evaluated X. Don’t take, no benefit Know normal discomforts of pregnancy and what is not normal and how do nurses educate their patients on the difference: g. Uterus i. Estrogen-contraction-during labor ii. Braxton Hicks contractions-irregular pattern, lasts <60 seconds, begin at 16 weeks —serves to prep uterus for labor/delivery Look at each system. What a normal change means to her and what education you would give? Common Discomforts • Nausea-usually resolves 13-14 weeks of gestation • Vomiting-monitor for hyperemesis gravidarum • Excess salvation • Fatigue • Nasal congestion-increased levels of estrogen/progesterone cause nasal mucus membranes to swell, produce excess mucus/congestion • Backache • Leukorrhea-increased estrogen levels cause increased vaginal discharge • Urinary frequency-pressure on bladder 1st trimester; increased progesterone levels relax the urethra muscles 3rd trimester • Dyspepsia-progesterone induced cardiac sphincter relaxation and delayed gastric emptying • Gas • Constipation-increased progesterone-relaxes smooth muscles, also iron supplementation • Hypertrophied gums • Leg cramps • Dependent edema-increased progesterone relaxed blood vessels, pressure on pelvic veins • Varicosities • Dyspareuria-painful sex-pelvic congestion, impaired circulation • Nocturia • Insomnia • Round ligament pain-relaxin causes relaxtion/stretching on ligaments • SOB • Finger numbness • Supine hypotensive syndrome-pressure on the IVC while supine, patient should lie on her left side instead. Cervix ❖ Chadwicks sign-bluish/purple color—increased blood flow/engorgement (Chad is sad so he’s blue) ❖ Goodell’s sign-cervical softening (Gooey and soft) ❖ Mucus plug-est/prog. Causes proliferation of mucus producing cervical glands-mucus fills the endocervical canal/forms a ‘plug’—keeps harmful agents out of uterus Breasts ❖ Montgomery tubercles-on/around areola; enlarge-lubricate nipple ❖ Striae gravidarum-stretch marks ❖ Colostrum-creamy, whitish/yellowish liquid; can leak from nipples at 16 weeks Integument ❖ Linea nigra-brown line from umbilicus to mons pubis ❖ Chloasma-“mask of preg” dark, brown blotchy pigmentation to face Iron ❖ Need more to make RBC/Hgb ❖ Greatest need during the last 4 weeks (for fetal stores) Nose ❖ Congestion-progesterone-increased mucus GI ❖ Pyrosis-heartburn-prog. Causes relaxation of smooth muscle-cardiac sphincter UA ❖ Urinary frequency-progesterone relaxes the urethra/sphincter Pituitary Gland ❖ Prolactin-anterior pituitary—initiates lactation (* increased est/prog prohibit lactation) ❖ Oxytocin-uterine contractions as well as milk ejection from mammary ducts (*synthetic—pitocin) Adrenal Glands ❖ Cortisol-promote fetal lung maturation, stimulates labor at term MS System ❖ Diastasis recti-separation of rectus abdominal muscles secondary to abdominal wall weakening to accommodate growing fetus ❖ Lumbar lordosis—helps with center of gravity ❖ Relaxin-(hormone secreted by placenta) relaxes ligaments—pubic symphysis separates at 28-30 weeks. What activity is appropriate for the pregnant patient? Placenta is the ‘work horse’ organ of pregnancy – what does it provide/what it doesn’t provide? h. Placenta ❖ Responsible for providing oxygen, nutrition, waste elimination, and hormones necessary to maintain pregnancy. ❖ Also serves as protection to the fetus from pathogens and maternal rejection. 4 hormones produced by placenta 1. HCG 2. Human placental lactogen-regulates glucose availability for fetus; promotes fetal growth 3. Progesterone-decreases maternal immunity to decrease response to fetal antigens, decreases myometrial activity, constricts vessels, inhibits prolactin, secretin, relaxes smooth muscle 4. Estrogen-increases myometrial activity increases sensitivity of progesterone late in pregnancy, softens cervical fibers, increases pituitary secretion of prolactin Umbilical cord structure and function. i. Connects to the chorionic villi i. Contains AVA 2 arteries and 1 vein to provide circulation of blood and nutrients to the fetus throughout pregnancy. i. Wharton’s Jelly-surrounds umbilical cord. Help protect the cord from compression Amniotic fluid what is the purpose? j. Fetal Membranes 1. Chorion-thick membrane, encloses amnion, embryo, yolk sac; contains fingerlike projections 2. Amnion-thin protective membrane; contains amniotic fluid Amniotic Fluid Functions 1 Cushions fetus, protect against mechanical injury 2 Maintain normal body temp 3 Allows for symmetrical fetal growth 4 Prevents amnion from adhering to fetus 5 Aids in MS development—freedom to move 6 Essential for lung development • Amounts: 30 mls at 10 weeks; 800mls at 24 weeks, remains stable throughout pregnancy. Decreases when close to term. • Contains-antibacterial properties, albumin, uric acid, creatinine, bilirubin, lanugo- downy hairs. • Fetal urine/lung secretions are the primary fluid in late gestation (make up majority of amniotic fluid) What is the issue with oligohydramnios, and polyhydramnios? Amniotic Fluid Complications 1. Oligohydraminos: <300ml – deficiency of amniotic fluid a. Fetal renal abnormalities, decreased placental perfusion, PROM b. Can lead to cord compression during labor, variable heart decels i. Tx: amnioinfusion 2. Polyhydraminos: Excess of amniotic fluid - multiparous, fetal anomalies, DM a. Can cause malpresentation, prolapse of cord, PROM~infection Nutrition is a key factor in pregnancy outcome – what is essential to include. What do most women need additional supplements for? Nutrition/Weight Gain Normal/non-pregnant-1200-2400 kcal/day Pregnant-additional 300 kcalories per day (1500-2700kcal/day) Wt.gain-1st trimester-1-2.5kg/week 2nd trimester-0.4kg/week Total-25-35 pounds through entire pregnancy 1st/2nd trimester—maternal growth, 3rd trimester-fetal growth Protein-maternal growth (uterus/breast) fetal tissue/organs ❖ Modest increase is needed Water-8-10 glasses per day-needed to maintain CV health and maintain adequate blood supply ❖ Maternal blood volume increases by 1500mls ❖ Meet needs of hypertrophied uterus ❖ Adequate hydration of mom/fetus tissues ❖ Provide blood supply reserve for blood loss in birth Calcium/Vit D-1300 mg/day, needed to grow fetal skeleton/teeth Iron/Vit C-needed to maintain Hgb levels with the increase in blood volume ❖ Fetal iron stores increase during 3rd trimester—fetal iron stored in their immature Livers—stores are used during the first 4mo of life ❖ Mom should take 30mg/day to compensate for the insufficient amounts in breast milk Know Folic Acid is used to help prevent the development of the Neural Tube and the absence of openings. Folic Acid (Vit B9)-water soluble vitamin (need water to absorb*)-required for RBC development, Hgb development, essential in production of DNA/RNA, maintains normal brain function. ❖ Increased estrogen levels decrease absorption and metabolism ❖ F.A. deficient-neural tube defects (spina bifida, cleft lip/palate, anencephaly) ❖ Neural tube develops during 1st 4 weeks of pregnancy ❖ Consume-800mg/day ❖ Explore the vegetarian diet. ❖ Explore the problem of generalized nausea and vomiting – not severe – ❖ Explore food fads. ❖ What are the risks to the fetus if mom does not gain weight or does not eat properly? ❖ And keep in mind the questions regarding the use of alcohol in pregnancy – it is never acceptable. Prenatal testing - multiple tests are completed: Recognize the difference between a screening (routine) exam and a diagnostic (focused) exam. Include diagnostic tests such as ultrasounds too. k. When do we provide them and why? l. Specifically the labs drawn in the early pregnancy – MSAFP – or the Triple screen when and why drawn? m. Existence of some chromosomal abnormalities – ie: Down syndrome. Antepartum Fetal Assessment- What is fetal well- being and how do we measure it? Chorionic Villi Sample (CVS) Obtain fetal karyotype-villi arise from trophoblast cells, chromosomes similar to the fetus. Invasive procedure Performed at 10-12 weeks. Ultrasound guided Checks for chromosomal anomalies Percutaneous Umbilical Cord Sample (PUBS) Invasive procedure Ultrasound guided, needle into maternal abdomen into fetal umb. Cord. Checks for anemia, metabolic disorders, infection Amniocentesis Removal of amniotic fluid—needle into mom’s abdomen Invasive procedure Done at 12 weeks+ to monitor for chromosomal anomalies, infection, and bilirubin Done at 35 weeks+ to monitor for lung maturity Surfactant~ Lecithin/Sphingomyelin (L/S ratio) 2:1 accepted as lung maturity Kick Counts = Fetal Movement Counting Mom lies on side, counts number of fetal movements. 10 counts in 2 hours-WNL Non-Stress Test Mom in lateral tilt position, external fetal monitor. FHR observed 2 accelerations (FHR) of 15BPM x 15 sec over 20 min= Reactive test (WNL) Contraction Stress Test Evaluates FHR response to uterine contractions. Fetal monitor tracing for 20 minutes. If spontaneous uterus contractions don’t occur then stimulate uterine contractions with IV oxytocin, or nipple stimulation until 3 contractions of at least 40 sec long within 10 min occur. Watch for +/- late FHR decels. Negative result (normal) no evidence of late or significant variable decels. Don’t do this test if: 3rd trimester bleeding, placenta previa/abruption, C. Sections with vertical incision, PROM, cervical incompetent, multigestations. TORCH infections. T Toxoplasmosis Undercooked meats, cat feces Damage to eyes/brain of fetus, increased risk of fetal death O Other (varicella, HIV, syphilis) Blood, semen, respiratory droplets/contact (varicella) Mental retardation, muscle atrophy, premature birth, FTT, deafness R Rubella (German Measles) Respiratory droplets Deafness, blindness, ment. Retard. C CMV Bodily fluids Spont. Abort., microcephaly, H Herpes Contact Spont. Abort, preterm birth, dermal scarring Complications of pregnancy – bleeding can be normal or abnormal – what are the causes of both? Normal = Implantation bleeding – spotting within the first 6-12 days after conception, when the fertilized egg is implanting into the uterine lining. Cervical bleeding- Pap test or sexual intercourse can cause contact with the cervix and cause minor bleeding, no cause for concern. Bloody show- occurs a few days or weeks prior to labor - Loss of mucus plug may have blood in it - Should stop fairly quickly ▪ If bleeding continues- call Dr.- may be in preterm labor Abnormal = Miscarriage during 1st trimester – bleeding within the first 12 weeks of pregnancy can mean miscarriage, however, if the fetal heart rate can be heard or seen on ultrasound, 90% of these women will not miscarry. - Recommend bedrest - Intense cramping can indicate loss of pregnancy due to fetal tissue moving through the vagina. Ectopic pregnancy- a fertilized embryo implants itself outside of the uterus, usually in the fallopian tube. - Embryo must be removed (abortion) - If left to grow, it can cause rupture of the fallopian tube, resulting in infertility, and life-threatening consequences (hemorrhaging?) Molar pregnancy- Abnormal tissue grows inside of the uterus instead of a baby- tissue can be cancerous and spread. (This is a very rare condition) - Severe N/V - Rapid enlargement of the uterus Infection of the cervix- STI’s can cause bleeding in the first trimester Placenta Previa- can cause bleeding in the 2nd trimester = medical emergency Placental abruption- detachment of the placenta from the uterine wall - Very dangerous to both mother and baby - Can result in severe hemorrhage Uterine rupture- scar from a previous C-section reopens - Requires emergency C-section - Can be life-threatening Vasa Previa- blood vessels in the umbilical cord or placenta cross the opening to the birth canal. - Can be fatal for the baby if rupture occurs. - Extremely rare Premature labor- active labor prior to 37 weeks - Contractions - Vaginal discharge - Abdominal pressure - Lower back pain Signs and Symptoms of Danger during Pregnancy 1st Trimester ❖ N/V-excessive ❖ Vaginal bleeding-spontaneous abortion <20 weeks ❖ Infection 2nd Trimester Maternal ❖ Pre-eclampsia-increase in BP (140/90) >20 weeks gestation with proteinuria ❖ S/S-headache, visual changes, high blood pressure, edema ❖ Premature rupture of membranes ❖ Preterm labor-uterine contractions <37 weeks Fetal ❖ Hypoxia-due to maternal hypertension ❖ Irregular/absent heartbeat ❖ Preterm birth ❖ Infection ❖ Absence of fetal movements after quickening Tx: drink 2 glasses of water, rest on left side x2 hours; <10 movements consult MD 3rd Trimester Maternal ❖ Gestational DM-glucose challenge test 24-48 weeks if +, then 3 hour oral glucose tolerance test (OGTT) ❖ Placenta Previa-implantation of placenta in lower uterine segment near or over the cervical os S/S-painless, bright red bleeding as it thins/stretches ❖ Abruptio placentae-premature separation of a normally implanted placentae from uterine wall; results in hemorrhage-abd pain, vaginal bleeding Tx: bedrest, IV Fluids, delivery Know the difference between placenta Previa/placental abruption. What are the risk factors for both? Placenta Previa-implantation of the placenta in lower uterus near/over the cervical os. ❖ Complete (total): covers os, most serious risk, greatest amount of blood loss ❖ Partial: partially occludes os ❖ Marginal: encroachment of os S/S: painless bleeding profuse bleeding/shock Dx: ultrasound (2nd trimester) *No Vaginal exam-risk of perforation* Tx: active bleeding IVF, CBC, Rh/Blood type, transfusion, RhoGAM, bedrest Betamethasone-promotes fetal lung maturity Delivery if needed Placental Abruptio-premature separation of a normally implanted placenta from uterus. Causing hemorrhage in-between S/S: bleeding with abdominal pain-3rd trimester Uterine tenderness, abdominal, back pain, board-like abdomen and vaginal bleeding, abdominal contractions, increased uterine tone Fetal HR decels, detal demise Dx: *3rd trimester vaginal bleeding* ultrasound Tx: delivery, bedrest, monitoring Preterm labor – know signs and symptoms, treatment, nursing interventions. Premature labor- active labor prior to 37 weeks - Contractions - Vaginal discharge - Abdominal pressure - Lower back pain Know the drugs – that are used as a tocolytic (a drug that stops preterm labor) Tocolytics ❖ Magnesium sulfate-beta mimetics ❖ Indomethacin-prostaglandin inhibitor ❖ Nifedipine-calcium channel blocker ❖ Terbutaline sulfate-beta mimentic Pre – eclampsia – know signs and symptoms (subjective and objective), treatment and nursing interventions. Pre-eclampsia-Increased BP with proteinuria > 20 weeks gestation - Headache - HBP - Changes in vision - swelling Eclampsia- Increased BP, proteinuria and convulsions Convulsions are tonic-clonic-before onset patient will complain of headaches, visual disturbances, blurry vision. Monitor DTR’s. Assess for irritability/clonus, if hyperactive test ankle clonus— indicator of seizure onset. ***Women with preeclampsia who have seizures are considered to have eclampsia. Patho: vasopressive disease of the placenta, decreased placenta perfusion and placental hypoxia Risk factors: primigravida, DM, pre-existing hypertension, multiparous Tx: delivery is the only cure Mild: rest at home, side lying position as much as possible Severe: seizure prophylaxis with magnesium sulfate (CNS activity decreased), antihypertensive medications: labetalol, nifidepine, HCTZ, Lasix, sodium nitroprusside HELLP Syndrome- pre-eclampsia is a precursor to HELLP syndrome Hemolysis, Elevated Liver enzymes, Low Platelets Arterial vasospasms occur in pre-eclampsia Serious complication of pre-eclampsia Elevated Liver Enzymes Vasospasms decrease blood flow to liver—tissue ischemia and hemorrhagic necrosis Low Platelets Endothelial damage (vasospasms)—small holes develop in the vessels— platelets clump together at the sites and fibrin network develops leading to a decrease in circulating platelets. Hallmark S/S: rapidly deteriorating liver function and thrombocytopenia Tx: transfusion of FFP, platelets, delivery Know the medications used in pregnancy, both the normal supplementation and those used to manage preterm labor and preeclampsia. ❖ Manage HBP- BP meds o Methyldopa. o Nifedipine. ❖ Prevent seizures- magnesium sulfate can be used as an anticonvulsant ❖ Steroids to help speed fetal lung development ***Know specifically magnesium sulfate since it is used for both reasons – preterm labor and preeclampsia due to the effect – n. it is a smooth muscle relaxant – hence the uterus is a smooth muscle and will respond well to the drug – o. Blood vessels and the tissue surrounding relax hence having a hypotensive response if using Mag. p. Please know magnesium well. i. It is the first line defense in pre-eclampsia….not to prevent hypertension but to ***prevent muscle contraction and seizures*** Magnesium Sulfate Very potent~Anticonvulsant , resolution of eclampsia S.E.: warm feeling, blurred vision, headaches, drowsiness, decreased respiratory rate, blood pressure, heart rate, temperature, diarrhea, sweating Dosing: 40g in 1L LR—4-6g bolus over 20 min, then 1-3g/hr Nsg. Respon.: always use a pump to administer Initiate seizure precautions Check patellar reflexes—if absent then stop the infusion until a positive response returns Monitor urine output ❖ Antidote: Calcium gluconate 10% 10ml IV over 1-3 minutes. What are some things that can affect placental perfusion? ❖ Uterine contractions ❖ Smoking ❖ Maternal age ❖ Blood-clotting disorders ❖ Previous uterine surgeries or placental problems ❖ Multiple pregnancies or twin pregnancy ❖ HBP ❖ Premature rupture of membranes ❖ Substance abuse ❖ Abdominal trauma q. What is the effect on the baby of the risk factors that may impede placental perfusion? i. Baby is at risk for poor oxygenation and can be deprived of vital nutrients as it develops. What is Supine Hypotension Syndrome? How can an epidural affect mom and baby? Diabetes in pregnancy is a big problem. DM in Pregnancy-impairment of CHO metabolism Risk Factors: obesity, PCOS, Hx of GDM, Hx of DM2 Patho: mom can’t break down fat, protein, and CHO appropriately, increased insulin resistance develops (secondary to increased production of placental hormones (insulinase/HPL), cortisol, growth hormone acts as insulin antagonist. Leads to altered CHO metabolism and hyperglycemia. What is the risk to the baby? ❖ Congenital malformations ❖ Increased birth weight and increased fetal adipose tissue o Fetal hyperinsulinism secondary to maternal hyperglycemia ❖ Perinatal death ❖ Neonatal hypoglycemia Fetal Response Fetus continues to remove glucose from mom’s circulation. Insulin doesn’t cross the placenta—so baby has to increase its own production. Fetal hyperinsulinemia develops acts as growth hormone. (Macrosomia) increased fetal size, decreased in pulmonary surfactant production Dx: Glucose Challenge Test 50g oral glucose solution. Blood samples drawn 1 hour later. Ifresults over 140+ then need further evaluation 3 Hr Glucose Tolerate Test fasting patient ingests 100g glucose. Blood samples drawn once an hour x3H. +result if 2 values are above normal Fasting <95 1 hour <180 2 hour <155 3 hour <140 Hyperemesis Gravidarum – • a problem of extreme nausea and vomiting causing electrolyte imbalance, dehydration and severe weight loss – Hyperemesis gravidarum-extreme nausea/vomiting unresolved by 16 weeks; persistent, unresolved with treatment and weight loss (5%) What is the nursing intervention? Tx: rest, high protein foods, avoid irritating foods, IVF with dextrose/vitamins, NPO status, antiemetics (Phenergan, metoclopramide, Dramamine) Do you understand the concept of perfusion, oxygenation, the hormone feedback system, and the responses of the body under the hormone influences? RhoGam—why is it given and when is it given? What is the primary action? Rho Immunization-Hemolytic disease of the fetus condition in which the lifespan of RBC’s is shortened secondary to maternal antibodies against antigens. Antigens provoke reaction if incompatible blood cell enters circulation. Maternal antibodies form in Rh – moms after exposure to Rh + fetus. Tx: Rho (D) immune globulin (RHoGAM)-coats/destroys fetal cells in moms circulation. Must be given within 72 hours after birth. Effects last 3 months RHoGAM can be given during and after birth. Usually the first Rh+ baby unaffected Fetal issue: when antibodies to the Rh factor are present in the pregnant patient’s blood, they freely cross the placenta and destroy the RBC’s of the fetus. Over time the fetus develops RBC deficiency, fetal bilirubin levels rise and severe neuro disease develop. (Bilirubin encephalopathy) In the fetus this triggers rapid production of immature RBC’s unable to carry oxygen erythroblastosis fetalis. Fetal anemia and general edema (hydrops fetalis), CHF. Intrauterine resuscitation— VEAL CHOP MINE V = variable and may indicate >>>>>>> C = cord compression M = move (side left) E = early decal and may be indicate >>>>>>> H = head compression I = identify labor progress A = accelerations and is >>>>>> O = OK N = no action needed L = late decel’s may indicate >>>> P= placental insufficiency E = execute action immediately Stages of Labor True Labor False Labor Contractions regular Contractions irregular Contractions increase in freq/duration N/A Pain in low back radiates to abd Pain in abd region Dilation/effacement are progressive No change to cervix Walking increases pain Walking decreases pain First Stage 2. Stage of dilation, longest stage. Begins with onset of contractions, end with complete effacement/dilation a. 3 Phases Latent Active Transition Begins with establishment of regular contractions Contractions Q3-5min lasting 60 sec Most intense part Contractions 5 min apart lasting 30-45 sec. Mod/sev. Contractions Contractions Q2-3 min x60- 90 sec Cerv. Efface/dilation 0-3cm Cerv. Dilation advances quickly 1-1.5cm/hr Cerv. Dil. 1-1.5cm/hr 10-14 hours, may happen at home Rectal pressure, urge to bear down, increase in bloody show, spont. ROM b. Nursing responsibilities: monitor mom/fetus regularly. Comfort measures, positioning, being present. Changing pads, hygiene, mouth care, bladder elimination full bladder prevents fetal descent, void Q2hours/foley catheter Second Stage 1. Begins at full dilation ends with birth of infant a. Promoting effective pushing: urge to push stimulated by Ferguson reflex-presenting part stretches pelvic floor muscles-urge to push related to station rather than dilation of cervix. b. Laboring Down: women rests as fetus descends. Pushing postponed until urge to push starts again. c. Prepare for birth i. Crowning: fetal head is encircled by vaginal opening. Birth is imminent. May feel burning sensation—skin is stretching; intense pressure on bowels d. Episiotomy: surgical incision in perineum to enlarge vaginal orifice during 2nd stage. Midline: best, heals quickly. Mediolateral: some complications, tearing, increased pain e. Birth: head delivered in controlled manner-limit injury-under symphysis pubis i. anterior shoulder reaches pelvic outlet-rotates midline-delivered from under pelvic arch ii. Posterior shoulder guided over perineum-body follows Cardinal Movements Mechanism of labor, describes how fetus passes through birth canal & positional changes required to facilitate birth a. Descent: progression of fetal head into mom’s pelvis a. Pressure of amniotic fluid b. Direct pressure of fundus on fetal breech c. Contractions of mom’s abd muscles d. Extension/straightening of fetal body e. Measured by stations b. Flexion: fetal head descends/comes into contact with soft tissues of pelvis, pelvic flood muscles, cervix—resistance causes fetal chin to flex into chest—smallest distance to enter mom’s pelvis c. Internal rotation: fetal head must rotate to fit into mom pelvic cavity-occiput rotates~L to R, sagittal sutures align with long axis of mom’s pelvis d. Extension: fetal head passes under mom’s pubic symphysis, head pivots/extends with each push. Head is born in extension with face towards rectum e. Restitution: shoulders enter pelvis in oblique position after head is delivered in extension position it rotates to position it occupied when engaged in inlet. f. External rotation: as restitution continues, shoulders begin to align in the ant/post. Diameter. The head continues to turn further to one side. Fetal trunk moves through pelvis with anterior shoulders descending first. g. Expulsion: after external rotation, mom’s pushing efforts bring anterior shoulder under pubic symphasis. Lateral flexion of should and head-anterior then posterior shoulder is born, then body. Clamping the cord ❖ 2 Kelly clamps on umbilical cord then cuts between clamps. o Plastic clamp on cord 0.5-1in from newborns abd o Check cord for AVA—blood samples drawn for lab Third Stage ❖ Birth of baby to birth of placenta ❖ Lasts 5-10 min ~30 min ❖ Uterine cavity immediately gets smaller, resulting in decrease of size of placental attachment site. Leads to separation of placenta from uterus. Clinical Indications Separation Occurred a. Uterus spherical in shape b. Uterus rises up, placenta down c. Umbilical cord drops further through vagina d. Gush of blood occurs ❖ Placenta expelled either Schultze (shiny) or Duncan (dirty) o Shiny: placenta separated from the inside to the outer margins with shiny/fetal side presenting first o Dirty: separated from outer margins inward, rolls up, presents sideways with rough/mom’s side presenting first ❖ Important that uterus continues to contract-minimizes bleeding to assist with this oxytocin is administered (IV/IM) ❖ If 30 min pass between birth of baby to placenta then placenta is retained. ❖ Must check to see that all of placenta was expelled Fourth Stage o Birth of Placenta to 1-2 hours after o Assess mom’s uterus, cervix, perineum o Uterus: firmness, height, position o Left hand above pubic symphysis gently apply pressure downward o Right hand cupped around fundus o Expected: feel firm, positioned midline or just below umbilicus ▪ Full bladder/excessive blood: misplace uterus ▪ If feels soft/boggy: excess blood/clots have pooled, immediately massage uterus until firm. o Also monitor lochia: bloody vaginal discharge, noting color, amount, presence of clots o Lochia rubra: first lochia-bright red o Amount determined by soaking of pads/frequency of pad changes. o 1 pad within 1st hour=WNL/small clots=WNL o Small, steady trickle of blood=trauma o Check Vital signs Q 5-15 minutes! APGAR-1 and 5 min after birth o 5 signs of cardiopulmonary, neuromuscular function o HR: 0-<100=resuscitation o Resp. Effort: vigorous cry=WNL, wear/absent=intervention o Muscle tone: extension of extremity-return to flexion=WNL o Reflex: gentle stroking motion along spine/flicking soles/toes=cry WNL o Color: pallor/cyanosis at 1min 0 1 2 HR Absent Slow <100 >100 Resp. effort Absent Slow/irregular/weak cry Good strong cry Muscle tone Flaccid Some flexion or extension Well flexed Reflex irritability No response Grimace Vigorous Cry Color Blue/pale Pink body, blue extremities (acrocyanosis) Completely pink Scoring: 0-10 8-10=good condition <8=needs resuscitation measures [Show More]
Last updated: 1 year ago
Preview 1 out of 44 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jul 31, 2022
Number of pages
44
Written in

Additional information
This document has been written for:
Uploaded
Jul 31, 2022
Downloads
0
Views
46
.png)