*NURSING > STUDY GUIDE > Week 6 study guide: Labor complications and obstetrical emergencies (All)
Week 6 study guide: Labor complications and obstetrical emergencies
Document Content and Description Below
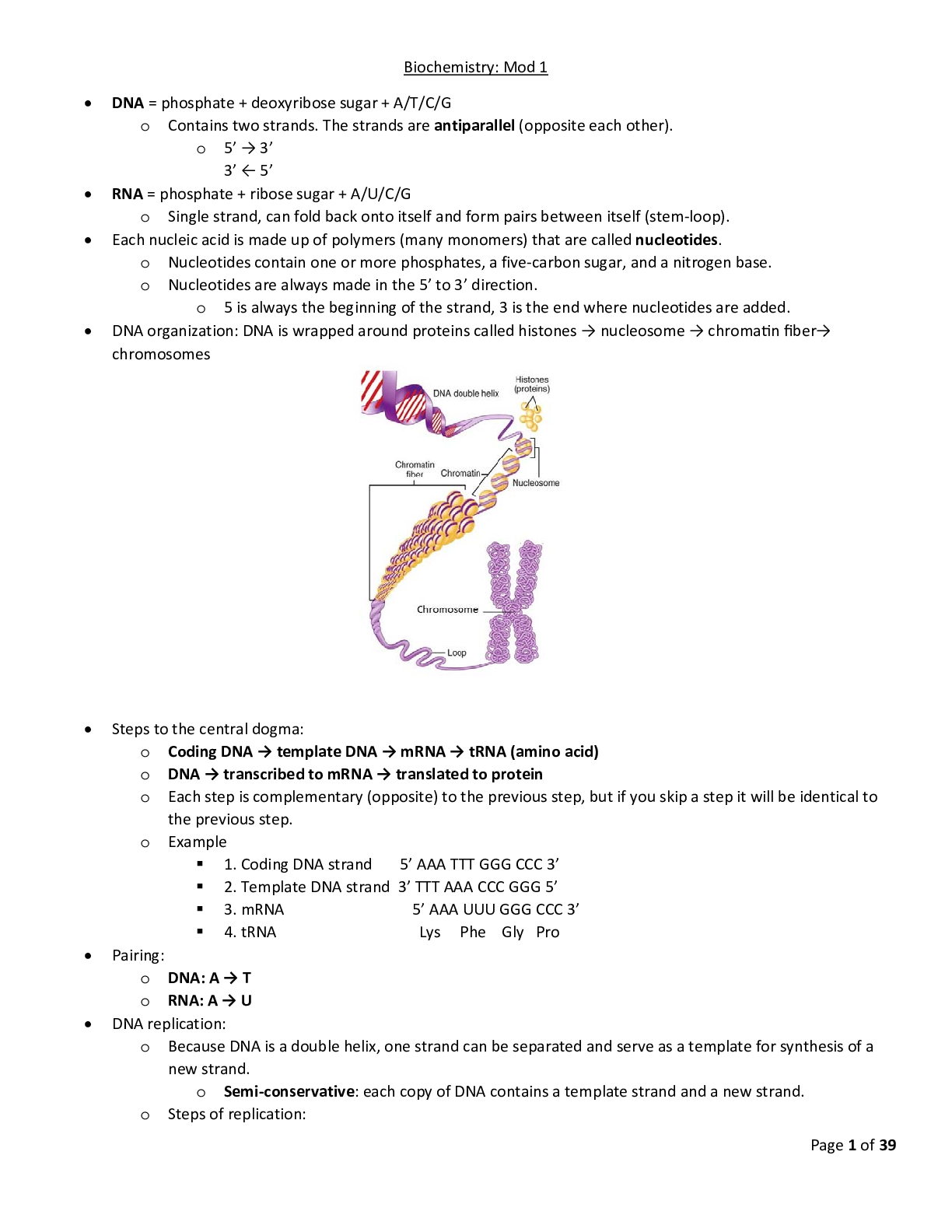
Week 6 study guide: Labor complications and obstetrical emergencies Dystocia (dysfunctional labor) Dystocia is abnormal labor that results from abnormalities of the power, the passenger, or the ... passage. Atypical uterine contractions patterns prevent the normal process of labor and its progression. Contractions can be hypotonic (weak, inefficient, or completely absent absent) or hypertonic (excessive frequent, uncoordinated, and of strong intensity with inadequate uterine relaxation) with failure to efface and dilate the cervix. Dystocia is the most common reason for primary cesarean sections. • Factors Influencing Labor: o Powers of labor (uterine contractions [UCs]) o Passenger (fetal position) o Passage (pelvic abnormality) • Risk Factors (Congenital abnormality with mom): o Cephalopelvic disproportion (CPD)- fetal head is larger than maternal pelvis. o Malpresentation or malposition of fetus- baby position. o bicornuate uterus- septum in the uterus (separation of the uterus that causes complications and can’t distend properly). o Tachysystole- contracting frequently every 1-2 minutes. Causing inadequate labor o Maternal fatigue or dehydration. o Pain medication too early. o Maternal fear. o Hormone release of large amount catecholamines that prevent oxytocin from releasing normally and causes abnormal contraction pattern. Hypertonic Uterine Dysfunction (precipitous labor risk factor) Hypertonic uterine dysfunction is nonproductive, uncoordinated, painful, uterine contractions during labor that are too frequent/ painful and too long in duration and do not allow for relaxation of the uterine muscle between contractions (uterine tetany). Hypertonic contractions do not contribute to the progression of labor (cervical effacement, dilation, and fetal descent). Hypertonic contractions can result uteroplacental insufficiency leading to hypoxia. • Uncoordinated Uterine Activity: frequent and painful, and not effective uterine contractions and not producing cervical dilations. Patient is at risk for severe exhaustion. • Risk Factors: Patient is at risk for severe exhaustion. Fetal intolerance. Efixia. Nulliparous woman are more subject to abnormal early labor. • Assessment Findings: o Painful, frequent UCs with inadequate uterine relaxation between UCs with little cervical changes. o May be Category II (indeterminate) or Category III (abnormal) fetal heart rate (FHR) related to prolonged labor and inadequate uterine relaxation • Medical Management: o Evaluate labor progress. o Evaluate cause of labor dysfunction. o Hydrate to improve uterine perfusion and coordination of UCs. o Provide pain management to allow the woman to sleep and prevent exhaustion. • Nursing Actions: o Promote rest to try to break the pattern of frequent but ineffective UCs. The pattern typically becomes effective when the woman sleeps for a period of several hours and awakens in a normal labor pattern of active labor. Methods used to promote uterine rest are: Administration of pain medication such as Demerol or morphine as per order to decrease labor contractions and allow the uterus to rest o Promotion of relaxation: Warm shower or tub bath, Quiet environment, Minimal interruptions to allow for long period of sleep o Hydrate the woman with IV or PO fluids if tolerated. Dehydration can result in dysfunctional labor. o Assess FHR and UCs o Evaluate labor progress with a sterile vaginal exam (SVE). ■ Inform the woman and family of the progress of labor and explain interventions o Inform the care provider of the woman’s response and progress in labor. Review: Hypertonic Uterine Dysfunction is uncoordinated uterine activity. Risk Factor: Nulliparous women are more subject to abnormal early labor. Hypotonic Uterine Dysfunction Hypotonic uterine dysfunction occurs when the pressure of the UC is insufficient (IUPC pressure <25 mm Hg) to pro- mote cervical dilation and effacement. Typically, the woman makes normal progress during the latent phase of labor, but during active labor the UCs become weaker and less effective for cervical changes and labor progress. The woman is at risk for exhaustion and infection related to the prolonged labor, and the fetus is at risk for fetal intolerance of labor and asphyxia. • Insufficient uterine contractions: Not sufficient enough in strength to produce cervical dilation. • Thus, insert the IUPC to determine to measure how strong the contractions are in mmHg. Only way to determine this is external palpation. This is utilized to measure the true intensity of the contraction enabling us to calculating Montevideo units. We want them to calculate between (<200; not adequate contractions)200-250 (>250; contractions that are too strong). ..................................................................continued......................................................................... [Show More]
Last updated: 1 year ago
Preview 1 out of 34 pages

Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
May 12, 2021
Number of pages
34
Written in

Additional information
This document has been written for:
Uploaded
May 12, 2021
Downloads
0
Views
33
.png)








.png)