*NURSING > DISCUSSION POST > NR 603 COMPARE AND CONTRAST DISCUSSION ON DEMENTIA AND DELIRIUM - DOWNLOAD TO SCORE A HIGH GRADE (All)
NR 603 COMPARE AND CONTRAST DISCUSSION ON DEMENTIA AND DELIRIUM - DOWNLOAD TO SCORE A HIGH GRADE
Document Content and Description Below
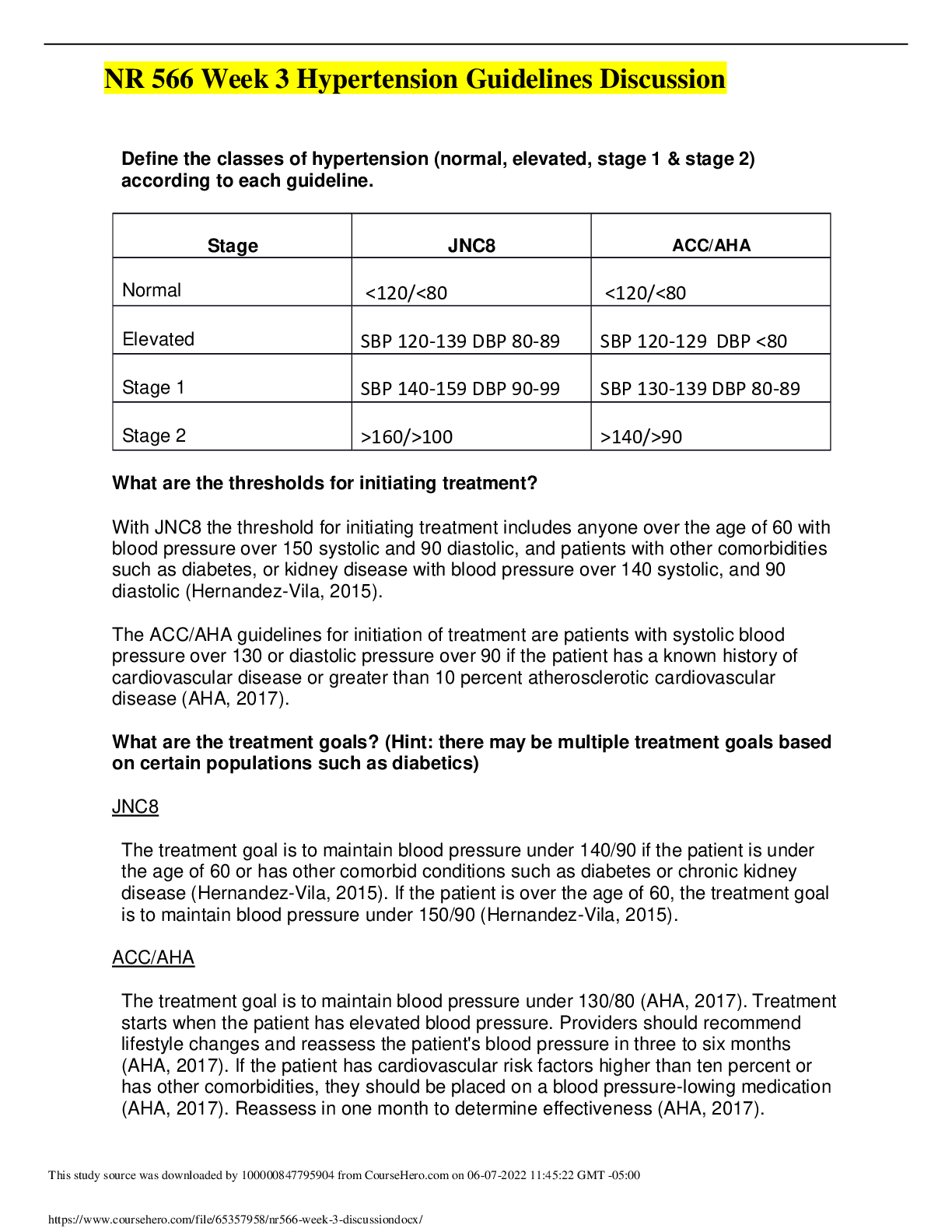
Dementia and Delirium – Compare and Contrast Presentation & Pathophysiology Dementia and delirium are both cognitive diseases that lead to poor health outcomes, increased morbidity, and increased m... ortality. Dementia typically presents in the older population, and age continues to be one of the greatest risk factors for dementia (Falk et al., 2018). Delirium is more likely to present in the older population but can present throughout the lifespan (Jackson et al., 2017). Per Jackson et al. 2017, 56% of dementia is undiagnosed or not recognized by health care providers. This is probably because the onset of dementia symptoms is slow. At first, the patient may start to have impaired instrumental activities of daily living (IADLS), such as remembering to take medications or difficulty managing their money (Falk et al., 2018). At this point, a health care provider may not recognize that a patient has dementia. The patient may also complain that routine tasks also take longer to complete, and the presence of multiple stimuli causes impaired attention and concentration (Falk et al., 2018). As the disease progresses, family members may be the ones to bring concerns of impaired cognition or memory. Dementia will cause difficulty completing multi-step activities, such as cooking a meal (Falk et al., 2018). Family members may say that the patient forgets that they’re cooking or will forget to turn off the stove after cooking. As the disease progresses, language, learning, memory, motor skills and social cognition will also be impaired (Falk et al., 2018). The disease will progress to impair activities of daily living (ADLS), such as bathing, toileting, and dressing (Falk et al., 2018). Unlike dementia, delirium presents as an acute, severe, and possibly life-threatening condition (Jackson et al., 2017). Wan and Chase (2017) state that delirium should be considered a medical emergency. Patients with delirium can present with incoherent thinking, auditory hallucinations, visual hallucinations, and agitation (Wan & Chase, 2017). Because the change in cognition is sudden and severe, delirium is diagnosed faster than dementia. The average survival rate after a diagnosis of dementia is 4.5 years, although this can vary depending on the age of the patient when he or she is diagnosed (Falk et al., 2018). If delirium continues to go untreated in an inpatient setting, the mortality rate can be as high as 76% (Wan & Chase, 2017). The cause of dementia is still unknown; besides age, other risk factors include a family history of dementia, a personal history of heart disease, diabetes, obesity, or cerebrovascular disease (Falk et al., 2018). Like dementia, the cause behind delirium is not yet fully recognized, but it is thought to be due to an inflammatory response and cholinergic neurotransmitter deficiencies (Wan & Chase, 2017). Risk factors for delirium include a medical event such as a major surgery or hip fracture (Wan & Chase, 2017; Cabrera & Kornusky, 2018). A patient with visual impairments, cognitive impairments, severe illnesses, and dehydration are more likely to develop delirium after being admitted to an inpatient setting (Wan & Chase, 2017). A previous history of cognitive impairment, such as having dementia, also puts a patient at higher risk for delirium (Wan & Chase, 2017). Medications can also put patients at a risk for delirium; up to 39% of cases of delirium are due to adverse effects of medications (Wan & Chase, 2017). It appears that there are identifiable causes, leading to an identifiable time period in which delirium starts. With dementia, it is less likely that the patient or family can identify the time that dementia started. This is most likely because the symptoms are subtle and do not impair normal life routines. Assessment, Diagnosis & Treatment Because these conditions are cognitive, there is no specific laboratory test that can be done to confirm delirium or dementia. Blood tests can help identify causes of delirium, such as electrolyte imbalances. Blood tests can also be ordered when assessing for dementia. Falk et al. (2017) recommends ordering a complete blood count, a comprehensive metabolic panel, thyroid levels, and vitamin B12 levels. Again, these tests will help rule out other conditions, but cannot definitively diagnose a cognitive disorder. Assessing and diagnosing dementia and delirium is done through screening tests. The Mini-Cog is a test that can done in the office to screen for dementia, however, it can only indicate if a patient has a cognitive impairment and is not specific for dementia (Falk et al., 2017). If a Mini-Cog is positive, a patient can be referred to a specialist for further cognitive testing. For patients presenting with possible delirium, a Confusion Assessment Method assessment tool can be used (Wan & Chase, 2017). A Mini-Cog would not be appropriate as the patient with delirium most likely will not be able to follow directions to complete the exam. A thorough neurological examination should be completed for both; however, this may prove difficult in the patient with delirium if they are uncooperative or unable to follow directions. A patient with delirium would also need a cardiac and respiratory exam, as other disease processes may affect these systems; for example, an electrolyte imbalance may cause ventricular arrythmias as well as delirium. For the elderly patient with dementia, a thorough skin examination may be needed to ensure there are no ulcers or wounds due to the inability to complete ADLs. A patient with delirium may also need a thorough skin assessment to ensure no unintentional, or perhaps intentional self-harm has occurred. Treatment of delirium involves treating the underlying cause; for example, if the patient presents with delirium due to an adverse effect from a medication, the medication should be stopped. Likewise, if a patient presents with delirium due to an infection, the infection should be treated. For patients with delirium, antipsychotic medications can be used to treat symptoms of agitation and aggression if verbal de-escalation fails (Wan & Chase, 2017). Unfortunately, we cannot treat the underlying cause of dementia, only the symptoms. Antipsychotic medications can be used in the dementia population if the patient is presenting with true psychosis; however, practice guidelines strongly encourage deprescribing of this class of medications for those with dementia (American Family Physicians, 2018). For dementia, cholinesterase inhibitors, memantine, and vitamin E are recommended for pharmacotherapy to help maintain cognitive functioning (Epperly et al., 2017). Nonpharmacological interventions for dementia include regular exercise and brain stimulating programs (Epperly et al., 2017). References American Family Physicians. (2018). Practice guidelines: deprescribing antipsychotics for behavioral and psychological symptoms of dementia and insomnia. American Family Physicians, 98(6), 394-395. Cabrera, G., & Kornusky, J. (2018). Evidenced-based care sheet: Delirium in older patients. In CINHAL Nursing Guide. EBSCO Publishing. Epperly, T., Dunay, M.A., & Boice, J.L. (2017) Alzheimer’s disease: Pharmacologic and nonpharmacologic therapies for cognitive and functional symptoms. American Family Physicians, 95(12), 771-778. Falk, N., Cole, A., & Meredith, T.J. (2018). Evaluation of suspected dementia. American Family Physician, 97(6), 398-405. Jackson, T.A., Gladman, J.R.F., Harwood, R.H., MacLullich, A.M.J., Sampson, E.L., Sheehan, B., & Davis, D.H.J. (2017). Challenges and opportunities in understanding dementia and delirium in the acute hospital. PLOS Medicine, 14(3): e1002247. https://doi.org/10.1371/journal.pmed.1002247 Wan, M., & Chase, J.M. (2017). Delirium in older adults: Diagnosis, prevention and treatment. BC Medical Journal, 59(3), 165-170. Discussion Board Response: Hi Reavis, Thank you for such an informative post on migraines and tension headaches. As you indicated, migraines are commonly seen in a health care setting. In fact, Buse et al. (2020) report that “second most disabling condition world-wide” is migraines (p 22). There are many co- morbidities that can be seen with migraines. Buse et al. (2020) found that patients with migraines were three times more likely to have anxiety, depression, and gastrointestinal ulcers. The increased prevalence of gastrointestinal ulcers in this group may be related to an increased use of non-steroidal anti-inflammatory agents (Buse et al., 2020). However, one group of medications that can be used to treat migraines prophylactically are anti- depressants; your post only mentioned beta blockers and anti-convulsant. Thus, if a patient has depression and/or anxiety, along with chronic migraines, an anti-depressant such as venlafaxine may be a good choice for a prophylactic medication. In our last courses together, we often discussed polypharmacy and over-prescribing. This is a great example of how we can treat two conditions with one medication and reduce the amount of prescription medications a patient takes. Patients may also want to seek out holistic care options; that is, they would prefer non- pharmaceutical methods of treatment. Acupuncture has been used to the treatment of headaches. Lemmon (2018) wrote that although the mechanism of action for acupuncture is still unclear, it is thought that stimulation of the central nervous system via needling of acupuncture points causes endorphins to be released, thus altering pain. Furthermore, magnetic resonance imaging shows that other stimulating specific points via acupuncture needling influences the serotonin levels in the brain (Lemmon, 2018). Lemmon (2018) goes on to write that a Cochrane review of literature found moderate evidence to support that acupuncture treatment can reduce headache frequency. While acupuncture may seem like a reasonable alternative to medications, health insurance companies may not provide coverage for the treatment. Health care coverage, or lack of, is another conversation for another time! Thanks again, Kue References Buse, D.C., Reed, M.L., Fanning, K.M., Bostic, R., Dodick, R., Schwedt, T.J., Munjal, S., Singh, P., & Lipton, B.J. (2020). Co-morbid and co-occurring conditions in migraine and associated risk of increasing headache pain intensity and headache frequency: Result of the migraine in America symptoms and treatment (MAST) study. The Journal of Headache and Pain, 21(1), 21-23. https://doi.org/10.1186/s10194-020-1084-y Lemmon, R. (2018). Acupuncture for pain: 7 questions answered. The Journal of Family Practice, 67(4), 224;226;228;230. Response to Instructor: What does that provider need to know about vitamin b12 deficiency and cognitive changes, hyponatremia, and hypothyroidism? Hello Dr. Martin, I’m not sure if I quite understand your question, but I am assuming that you’re asking the relationship between cognition and vitamin B12 deficiency, cognition and hyponatremia, and cognition and hypothyroidism. Vitamin B12 deficiency has been linked to cognitive impairment and other neurological disorders (Bailey et al., 2020). The aging process causes reduced gastric acid production, which is needed to digest and absorb vitamin B12 found in animal sources (Bailey et al., 2020). Furthermore, the long-term use of gastric acid reducing medications, such as omeprazole, will may lead to B12 deficiencies (Bailey et al., 2020). Vitamin B12 deficiencies are thought to elevate homocysteine; homocysteine is thought to negatively impair brain function, with the signs and symptoms manifesting as impaired cognitive functioning (Bailey et al., 2020). Hyponatremia is one the most common electrolyte imbalances (Fujisawa et al., 2016). Hyponatremia is frequently diagnosed in the elderly, but mild episodes may not be treated (Fujisawa, 2021). Chronic hyponatremia is difficult to detect as the body can adapt to the imbalance (Fujisawa et al., 2016). In the elderly, hyponatremia can also manifest as memory impairment, gait impairment, decreased attention spans, and frequent falls (Fujisawa et al., 2016; Fujisawa et al., 2021). Thus, the combination of memory loss and physical impairments may cause a provider to assume a cognitive process such as dementia. Finally, thyroid hormones have been shown to have an impact on memory and cognition. Hypothyroidism impairs the normal processes of utilizing glucose for energy, thus, affecting the brain functions such as memory (Bavarsad et al., 2019). Thyroid dysfunction can impair cognition throughout the entire lifespan (Bavarsad et al, 2019). For example, the lack of thyroid hormone to a developing fetus can result in cognitive impairment; infants are shown to have numerous brain changes, including a smaller hippocampus and reduced axonal density (Bavarsad et al., 2019). Bavarsad et al. (2019) write that although hypothyroidism is a reversible cause of cognitive impairment, not all cognitive impairments can be reversed by thyroid supplementation. For example, it is still unclear if Alzheimer’s disease results from thyroid imbalances, or if thyroid imbalances are the result of Alzheimer’s disease (Bavarsad et al., 2019). As I had indicated in my original post, blood tests for electrolyte imbalances, B12 levels and thyroid levels can help rule out other causes of cognitive impairment. Thus, it is essential that the provider order and review these results to further support a diagnosis such as dementia or delirium. Thank you, Kue Her Reference Bailey, R.L., Jun, S., Murphy, L., Green, R., Gahche, J.J., Dwyer, J.T., Pottischman, N., McCabe, G.P., & Miller, J.W. (2020). High folic acid or folate combined with low vitamin B12 status: potential but inconsistent association with cognitive function in a nationally representative cross- sectional sample of US older adults participating in the NHANES. The American Journal for Clinical Nutrition, 112, 1547-1557 Bavarsad, K., Hosseini, M., Hadjzahed, M., & Sahebkar, A. (2019). The effects of thyroid hormones on memory impairment and Alzheimer’s disease. Journal of Cellular Physiology, 234(9), 14633-14640. https://doi.org/10.1002/jcp.28198 Fujisawa, H., Sugimura, Y., Takagi, H., Mizoguchi, H., Takeuchi, H., Izumida, H., Nakashima, K., Ochiai, H., Takeuchi, S., Kiyota, A., Fukumoto, K., Iwama, S., Takagishi, Y., Arima, H., Komatsu, Murata, Y., & Osio, Y. (2016). Chronic hyponatremia causes neurological and psychologic impairments. Journal of American Society of Nephrology, 27(3), 766-780. https://doi.org/10.1681/ASN.2014121196 Fujisawa, C., Umegaki, H., Sugimoto, T., Samizo, S., Hsein Huang, C., Fujisawa, H., Sugimura, Y., Kuzyua, M., Toba, K., & Sakuri, T. (2021). Mild hyponatremia is associated with low skeletal muscle mass, physical function impairment, and depressed mood in the elderly. BMC Geriatrics, 21(1), 15. https://doi.org/10.1186/s12877-020-01955-4 [Show More]
Last updated: 1 year ago
Preview 1 out of 8 pages

Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Mar 03, 2023
Number of pages
8
Written in

Additional information
This document has been written for:
Uploaded
Mar 03, 2023
Downloads
0
Views
49
 (1).png)
.png)
.png)
.png)
.png)
