*NURSING > CASE STUDY > NR 511 WEEK 6 CASE STUDY DISCUSSION PART 2 WITH ANSWERS (All)
NR 511 WEEK 6 CASE STUDY DISCUSSION PART 2 WITH ANSWERS
Document Content and Description Below
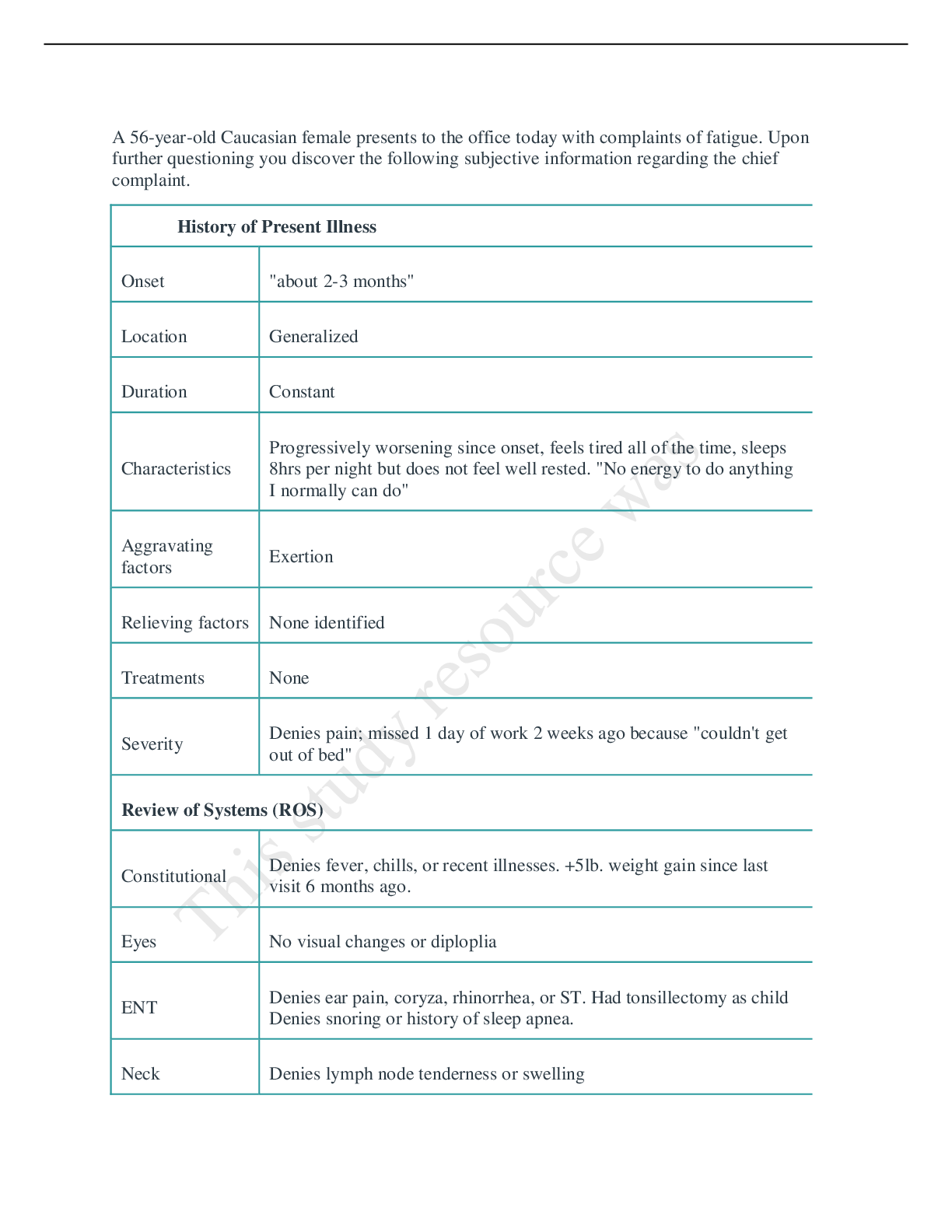
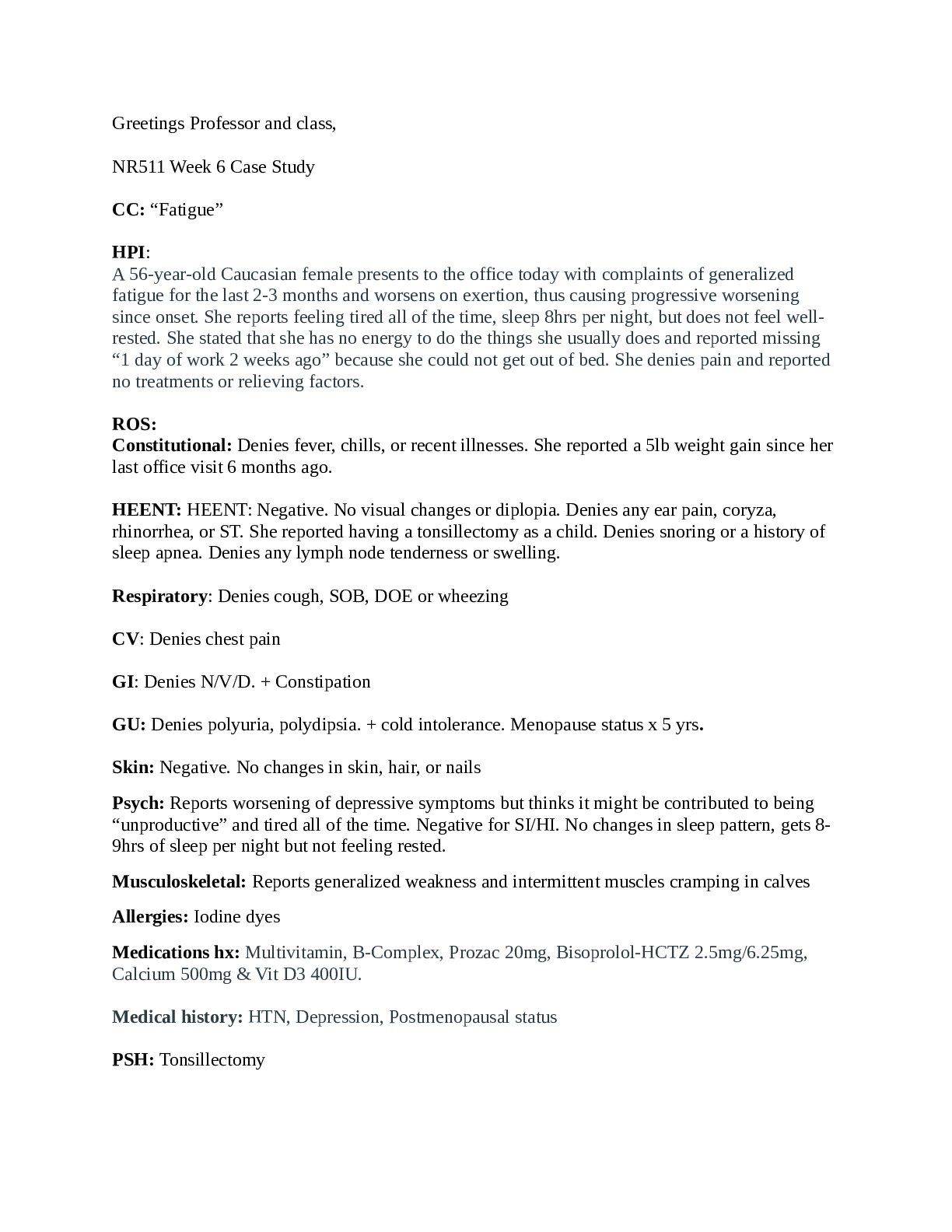
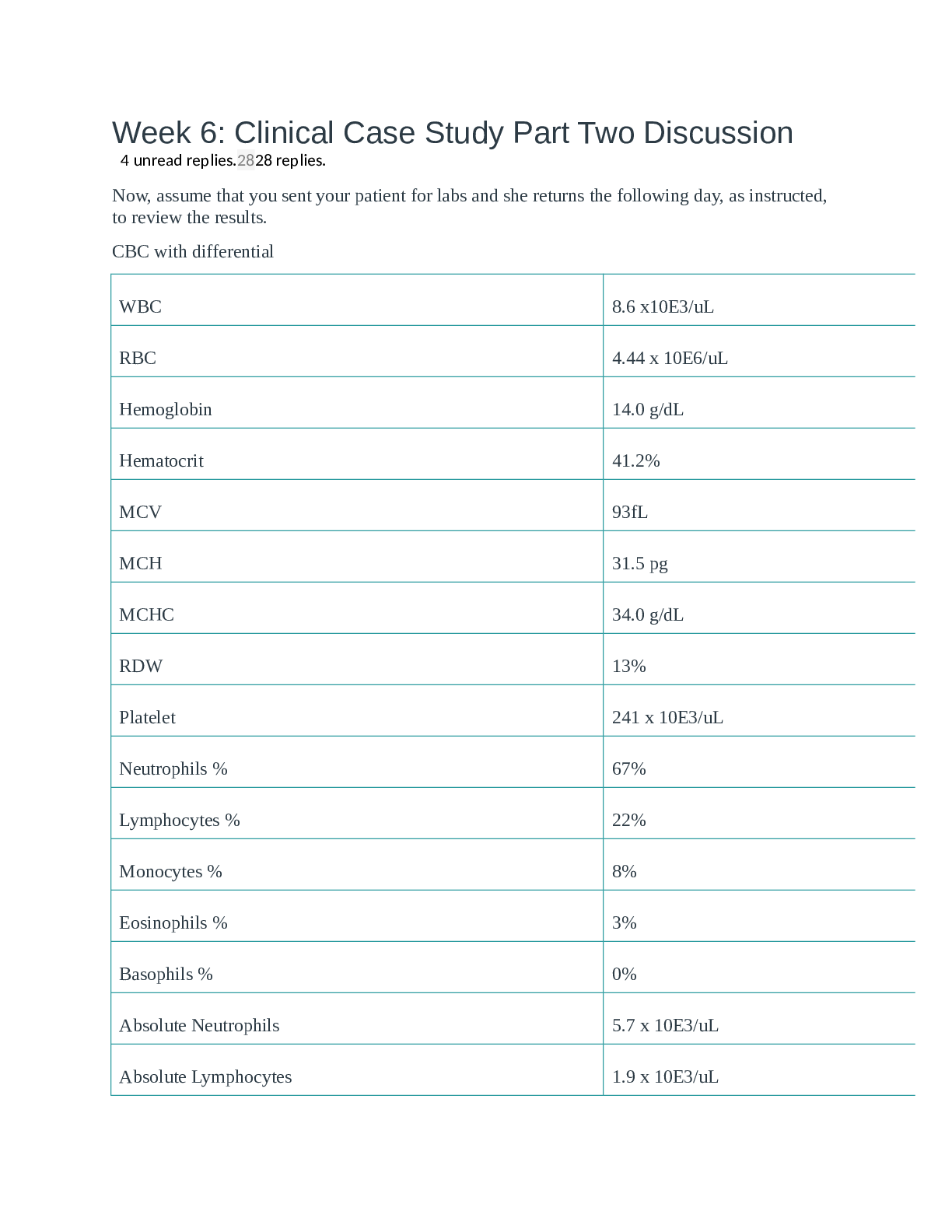
Week 6: Clinical Case Study Part Two Discussion 44 unread replies.2828 replies. Now, assume that you sent your patient for labs and she returns the following day, as instructed, to review the resul... ts. CBC with differential WBC 8.6 x10E3/uL RBC 4.44 x 10E6/uL Hemoglobin 14.0 g/dL Hematocrit 41.2% MCV 93fL MCH 31.5 pg MCHC 34.0 g/dL RDW 13% Platelet 241 x 10E3/uL Neutrophils % 67% Lymphocytes % 22% Monocytes % 8% Eosinophils % 3% Basophils % 0% Absolute Neutrophils 5.7 x 10E3/uL Absolute Lymphocytes 1.9 x 10E3/uL Absolute Monocytes 0.7 x 10E3/uL Eosinophils Absolute 0.3 x 10E3/uL Basophile Absolute 0.0 x 10E3/uL Immature Grans % 0% Absolute Immature Grans 0.0 x 10E3/uL TSH with Reflex to FT4 TSH 6.770 uIU/mL FT4 0.62 ng/dL PHQ-9 Depression Score=10 (previous was 5 at last visit 6 months ago) 1. What is your primary diagnosis for this patient as the cause for the CC of fatigue? (support your decision for your diagnosis with pertinent positives and negatives from the case) 2. Identify the corresponding ICD-10 code. 3. Provide a treatment plan for this patient's primary diagnosis which includes: o Medication* o Any additional testing necessary for this particular diagnosis* o Patient education* o Referral 4. Provide an active problem list for this patient based on the information given in the case. 5. Are there any changes that you would make to the patient's overall plan at this time? Must provide an evidence-based medicine (EBM) argument to support any treatments or testing decisions. 6. Provide an appropriate follow-up plan (include any additional testing that you feel is necessary and include an EBM argument). *If part of the plan does not warrant an action, you must explain why. ALL medication and testing decisions (or decisions not to treat with medication or additional testing) MUST be supported with an EBM argument. Over-the-counter (OTC) and RXs must be written in full as if handing a script to the patient in the office. Participation Guidelines Enters initial post to part one by 11:59 p.m. MT on Tuesday; initial post to part two by 11:59 p.m. MT on Thursday; responds substantively to at least one topic-related post of a peer including evidence from appropriate sources in parts one and two, AND all direct faculty questions in parts one and two by Sunday, 11:59 p.m. MT. **To see view the grading criteria/rubric, please click on the 3 dots in the box at the end of the solid gray bar above the discussion board title and then Show Rubric. This topic is closed for comments. Search entries or author Filter replies by unread Unread Collapse replies Expand replies Subscribed Collapse Subdiscussion Jaemee Nguyen Jaemee Nguyen Aug 13, 2019Aug 13 at 10:19pm Manage Discussion Entry Dr.Feehan and class, Week 6: Clinical Case Study Part Two Discussion Primary diagnosis and ICD-10 The U.S. Preventative Task Force (2015) also supports diagnosis of hypothyroidism based on elevated TSH and low T4 levels with or without clinical symptoms such as fatigue, weight gain or constipation. Pertinent positive findings: Generalized fatigue and weakness, weight gain as well as brittle nails and coarse hair, intolerance to cold, decreased DTRs in knees and ankles (+1), muscle cramping in calves, increased TSH level of 6.770 µIU/mL (normal range 0.5 – 4.70 µIU/mL), decreased FT4 level of 0.62 ng/dL (normal range 0.8 – 1.8 ng/dL). Review of the patient’s lab values indicates that her TSH is elevated and her FT4 is low which supports my primary diagnosis or of hypothyroidism with a corresponding ICD 10 code of E03.9. Treatment Plan While the patient’s lab values provide a diagnosis of hypothyroidism, there are conflicting recommendations regarding when medical management should begin. The most recent clinical guidelines provided by the American Association of Clinical Endocrinologists and the American Thyroid Association recommends medical therapy using levothyroxine when the patient’s TSH is greater that 10mIU/L. This same guideline states that the benefit in treating patients with a TSH between 4.5 to 10mIU/L is not clear. The decision to treat patients that have hypothyroidism as diagnosed by a TSH above 4.12mIU/L, but have a TSH less than 10mIU/L should be individualized based on the degree of symptoms, and risk of heart disease. With this in mind, consideration of the patient’s symptoms of ongoing fatigue that is interfering with her functional ability to work, increased depression symptoms, weight gain, constipation and cold intolerance supports the decision to start medical therapy at this time. Medications The medical treatment of hypothyroidism is the administration of an oral synthetic T4 hormone, or levothyroxine sodium to achieve resolution of symptoms and normal TSH and T4 levels. Dosage of levothyroxine is highly variable, and the recommended starting dose is 1.6 mcg/kg based on ideal body weight. The patient is 180 lbs = 81.8 kg. (1.6mcg/kg x 81.8kg=130) Levothyroxine (Synthroid) 125mcgDisp: # 30 tablets Sig: take one (1) tablet by mouth in the morning before breakfast for better absorption. Levothyroxine is the standard treatment for patients with hypothyroidism (Razvi & Peeters, 2019). Further Tests None. Patient education Educate the patient and family about the disorder and its management; reinforce that replacement therapy gradually restores proper metabolic function and quality of life. Iodine is a trace mineral and essential nutrient that is primarily necessary for synthesis of the thyroid hormones T4 and triiodothyronine (T3), the thyroid contains 80% of body iodine stores, T3 and T4 are necessary for proper brain development (especially during the first three years of life), physical growth, sexual development, and metabolism and energy regulation(Marcel & Pravikoff, 2018). Iodine must be consumed in the diet, since it is not manufactured within the body. Dietary sources of iodine include: iodized table salt,seafood (e.g., cod, bass, haddock, and perch), kelp,dairy products, eggs, and produce from regions with iodine-rich soil; the recommended daily iodine intake: Adults > 14 years of age: 150 mcg (Marcel & Pravikoff, 2018).Myxedema coma/crisis is a medical emergency that can necessitate mechanical ventilation, pivotal cardiac monitoring, and IV levothyroxine and corticosteroids until normal adrenal function is restored (Marcel & Pravikoff, 2018).Teach the patient and/or family to contact emergency services if S/S of myxedema coma/crisis develop. Most importantly, substituting between brand-name or generic levothyroxine can produce clinically significant differences in TSH and T4 levels. Referral There are situations in which an endocrinologist is needed since they are particularly knowledgeable about the function of the thyroid gland and the body’s other hormone-secreting glands. At least once when first diagnosed with hypothyroidism to review condition, test results, and treatment plan. Other times it's smart to see an endocrinologist are when: Symptoms of hypothyroidism does not get improved despite treatment, have a thyroid nodule or lump, enlarged thyroid gland, or goiter, a pituitary gland disorder is causing hypothyroidism, pregnant or are trying to conceive. Active problem list 1. Fatigue 8 2. Depression9 3. Overweight E66.3 Are there any changes that you would make to the patient's overall plan at this time? No changes that I would like to make to the patient’s overall plan at this time. Follow-up plan Subclinical hypothyroidism can be treated, and serum TSH levels are evaluated every 6–12 months to monitor disease progress (March & Pravikoff, 2018). References Hypothyroidism. Health Library: Evidence-Based Information, EBSCO Publishing, 2018 Nov 01 (patient education - condition), Database: Nursing Reference Center Plus Marcel C., & Pravikoff D. (2018). Hypothyroidism: Dietary Considerations. CINAHL Nursing Guide, EBSCO Publishing, 2017 Jun 16 (Evidence-Based Care Sheet), Database: Nursing Reference Center Plus. March P. & Pravikoff D. (2018). Hypothyroidism in Adults. CINAHL Nursing Guide, EBSCO Publishing, 2018 Jun 01 (Quick Lesson), Database: Nursing Reference Center Plus. Razvi S. & Peeters R. (2019). Thyroid Hormone Therapy for Subclinical Hypothyroidism. Pearce SHS, JAMA [JAMA], ISSN: 1538-3598, 2019 Feb 26; Vol. 321 (8), pp. 804; Publisher: American Medical Association; PMID: 30806683, Database: MEDLINE Complete Pubmed. 1. Collapse Subdiscussion Sharon Feehan Sharon Feehan Aug 16, 2019Aug 16 at 12:17am Manage Discussion Entry Great job on choosing the correct primary dx, Jaemee. Your treatment plan is appropriate. There were a few other things you also needed to include however. Remember, you always need to look at the TOTAL patient. Her B/P was elevated (in VS given in Part 1). and she's on treatment. So HTN should be on your problem list. You should be addressing you plan re: this. You could have chosen to increase her meds OR you could have very reasonably chosen to watch and wait, given B/P may come under better control once she reaches a euthyroid state. EITHER approach here would have been fine.....but you need to address the issue of her HTN in some fashion. Likewise, you needed to address what your plan for her depression would be. You're correct that she's already on treatment. Based on repeat the PHQ9 , she is objectively worse, though. You could have either chosen to increase the dose of her antidepressant, send her to Psych for med adjustment, or simply watch her, given the depression may improve once the thyroid issue is corrected. You needed to address it though, in some way. In your section discussing any plans for referral, you discuss all the possibilities of what is possible and what MIGHT be done. If this was your patient in your office right now, you need to make a decision, one way or another. What WILL you do, NOW? FYI - there wold be no reason to send her to endocrine at this juncture. She would likely only need to do go if she was not responding to standard therapy. Dr. Feehan Jaemee Nguyen Jaemee Nguyen Aug 16, 2019Aug 16 at 11:39pm Manage Discussion Entry Thank you Dr.Feehan, Hypertension I10 Constipation K59.0 For a BP 146/95, which is not substantbly high, I have chosen to monitor and wait, hoping the B/P may be better control once she has her hypothyroid situation resolved. In patients 18 to 59 years of age without major comorbidities, and in patients 60 years or older who have diabetes, chronic kidney disease (CKD), or both conditions, the new goal blood pressure level is <140/90 mm Hg. Based on repeat the PHQ-9 Depression Score=10, she is objectively worse due to not feeling well and not being able to work. Less medication is the route I had chosen, once again I would like to watch her and have high hopes that the depression may improve once the thyroid issue is corrected. If she needs someone to talk to, I can send her to a psychiatrist. However, before turning to laxatives, teach the patient to try these lifestyle changes to help with constipation: eat fiber-rich foods, such as wheat bran, fresh fruits and vegetables, and oats; drink plenty of fluids daily; exercise regularly (Schub, & Pravikoff, 2018). Bulk-forming laxatives, also referred to as fiber supplements, are the gentlest on the body and safest to use long term such as Metamucil and Citrucel. Reference Schub T., & Pravikoff D. (2018) [Show More]
Last updated: 1 year ago
Preview 1 out of 30 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
May 03, 2022
Number of pages
30
Written in

Additional information
This document has been written for:
Uploaded
May 03, 2022
Downloads
0
Views
80