*NURSING > CASE STUDY > Diana Humphries _ Diabetic Ketoacidosis (DKA)_Case Study Clinical Reasoning - 2022 | NR 466 Diabetic (All)
Diana Humphries _ Diabetic Ketoacidosis (DKA)_Case Study Clinical Reasoning - 2022 | NR 466 Diabetic Ketoacidosis_UNFOLDING Reasoning Case Study: STUDENT
Document Content and Description Below
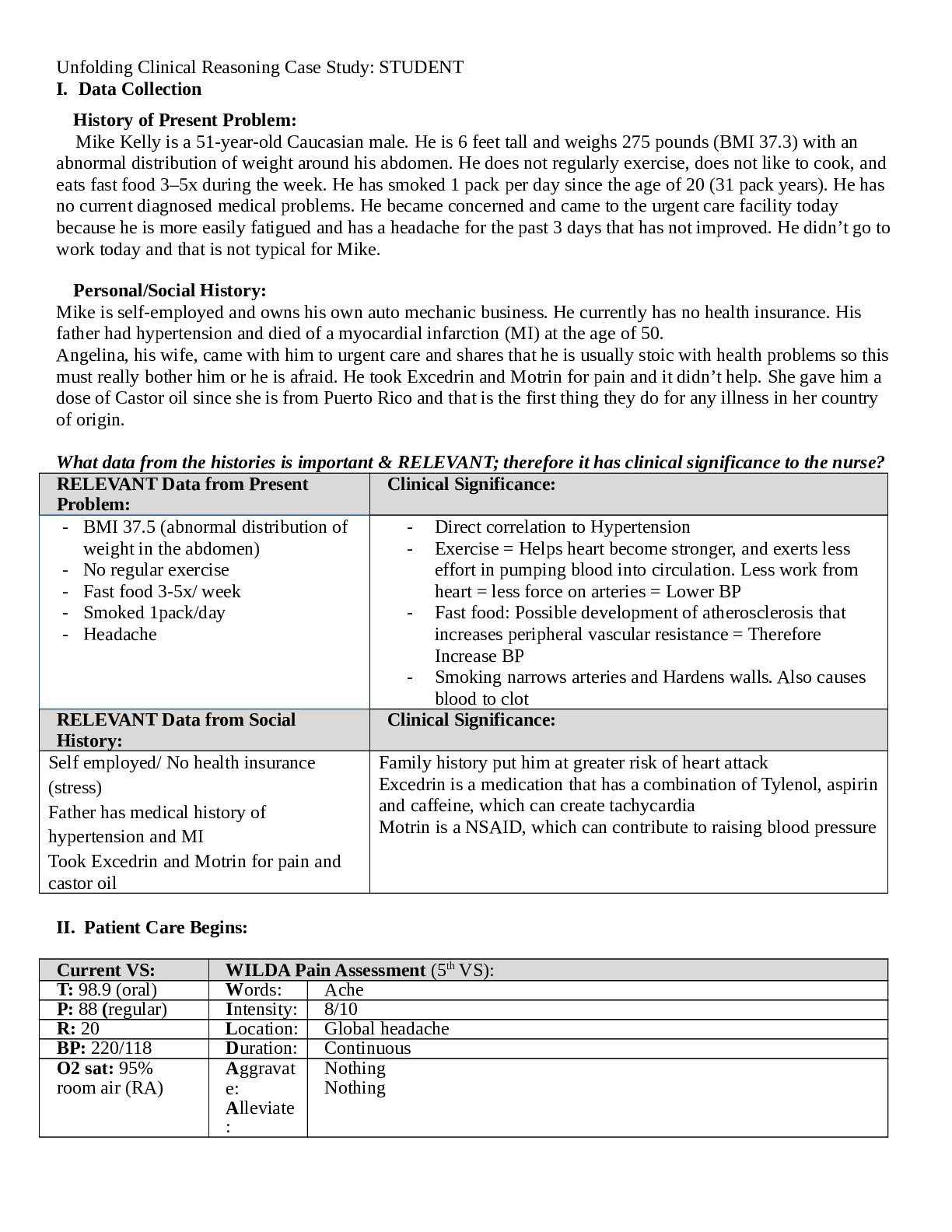
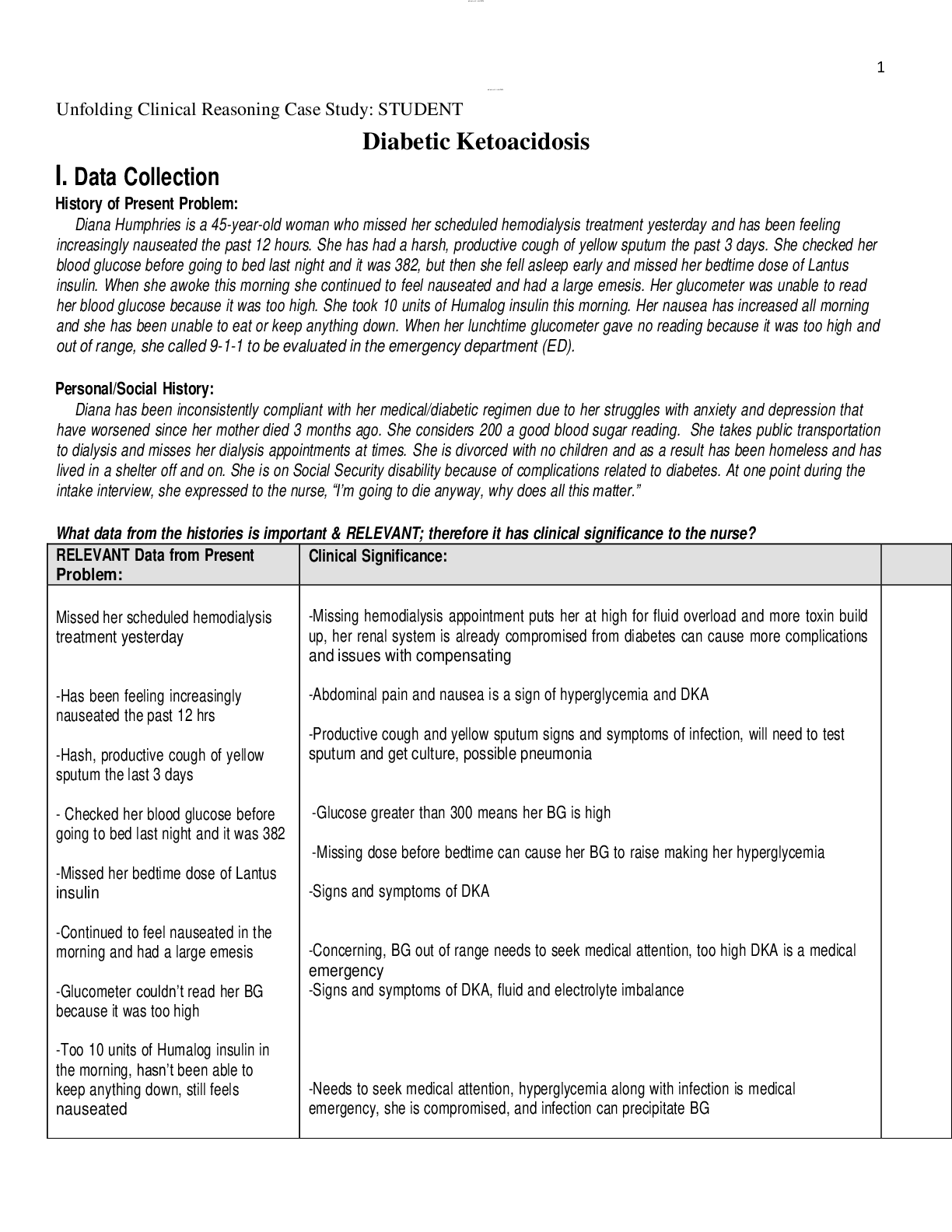
Diabetic Ketoacidosis (DKA) Diana Humphries, 45 years old Primary Concept Fluid and Electrolyte Balance Interrelated Concepts (In order of emphasis) 1. Acid-Base Balance 2. Glucose Regulation 3... . Infection 4. Pain 5. Clinical Judgment 6. Patient Education 7. Communication 8. Collaboration © 2016 Keith Rischer/www.KeithRN.com UNFOLDING Reasoning Case Study: STUDENT Diabetic Ketoacidosis (DKA) History of Present Problem: Diana Humphries is a 45-year-old woman with chronic kidney disease stage III and diabetes mellitus type1 who checks her blood sugar daily, or whenever she feels like it. She has been feeling increasingly nauseated the past 12 hours. She has had a harsh, productive cough of yellow sputum the past three days. She checked her blood glucose before going to bed last night and it was 382, but then she fell asleep early and missed her bedtime dose of glargine (Lantus) insulin. When she awoke this morning, she had generalized abdominal pain and continued to feel nauseated and had a large emesis. Her glucometer was unable to read her blood glucose because it was too high. She took 10 units of lispro (Humalog) insulin this morning. Her nausea has increased all morning and she has been unable to eat or keep anything down despite having an increased thirst and appetite. She also has had increased frequency of urination. When her lunchtime glucometer gave no reading because it was too high and out of range, she called 9-1-1 to be evaluated in the emergency department (ED). Personal/Social History: Diana has been inconsistently compliant with her medical/diabetic regimen due to her struggles with anxiety and depression that have worsened since her mother died three months ago. She considers 200 a good blood sugar reading. She is divorced with no children and has been homeless and has lived in a shelter off and on the past month. She is on Social Security disability because of complications related to diabetes. At one point during the intake interview, she expressed to the nurse, “I’m going to die anyway, why does all this matter?” What data from the histories is RELEVANT and has clinical significance to the nurse? RELEVANT Data from Present Problem: Clinical Significance: Chronic Kidney Disease Type 1 Diabetes and checks blood sugar whenever she feels like it Blood Sugar 383 before bed and didn’t take her bedtime Lantus Generalized abdominal pain, nausea, emesis Increased thirst, appetite, urination Lunchtime glucometer gave no reading because too high Decreased function of the kidneys and if patient is in DKA there is an increased load on kidneys due to polyuria Puts her at risk for developing DKA especially since she doesn’t check her blood sugar regularly Blood sugar already high before bed so we know it was high for a while before she called 911 Signs and symptoms of hyperglycemia Signs and symptoms of hyperglycemia Severe hyperglycemia RELEVANT Data from Social History: Clinical Significance: Inconsistently compliant with her medical/diabetic regimen Anxiety and Depression from her mother’s death Divorced with no children Homeless Inability to comply with medications increases risk for complications. Doesn’t have emotional support Due to her current financial hardship, she is unable to comply with her medications and her diabetes regimen. © 2016 Keith Rischer/www.KeithRN.com Receives social security disability benefits What is the RELATIONSHIP of your patient’s past medical history (PMH) and current meds? (Which medication treats which condition? Draw lines to connect) PMH: Home Meds: Pharm. Classification: Expected Outcome: • Chronic Kidney disease stage III (diabetic nephropathy) • Anemia • Diabetes mellitus type 1 since age 12 • Diabetic retinopathy • Neuropathy in lower legs • Hyperlipidemia • Hypertension • Coronary artery disease • Gastroesophageal reflux disease (GERD) • Anxiety • Depression 1. Aspirin 81mg PO daily 2 .Lisinopril 10 mg PO daily 3. Lorazepam 1mg PO bid prn 4. Citalopram 40 PO mg daily 5. Zolpidem 10 mg PO at HS prn 6. Gabapentin 300 mg PO bid 7. Labetalol 200 mg PO bid 8. Omeprazole 20 mg PO daily 9 .Simvastatin 40 mg PO HS 10. Glargine insulin 50 units SQ at HS 11. Lispro insulin SQ sliding scale AC and HS Salicylates ACE inhibitors Benzodiazepine SSRI Sedative Analgesic adjunct Beta Blocker Antilipidemia Pancreatics Pancreatics Aspirin will help with the pain caused by her neuropathy. Lisinopril will help manage her hypertension and with her kidney disease. Lorazepam will help calm down the patient and make her less anxiety. Zolpidem will allow the patient to sleep better. Gabapentin will help with nerve pain caused by her neuropathy. Labetalol will help with her hypertension and decrease her heart rate decreasing stress on the heart. Omeprazole will decrease the stomach acid h [Show More]
Last updated: 1 year ago
Preview 1 out of 16 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 14, 2022
Number of pages
16
Written in

Additional information
This document has been written for:
Uploaded
Apr 14, 2022
Downloads
0
Views
77

, Diana Humphries, 45 years old.png)
, Diana Humphries, 45 years old, (Latest 2021) Correct Study Guide, Download to Score A.png)

 Diana Humphries.png)
