*NURSING > CASE STUDY > NR 602 Week 3 Immunization Case Study Assignment (GRADED A+) (All)
NR 602 Week 3 Immunization Case Study Assignment (GRADED A+)
Document Content and Description Below
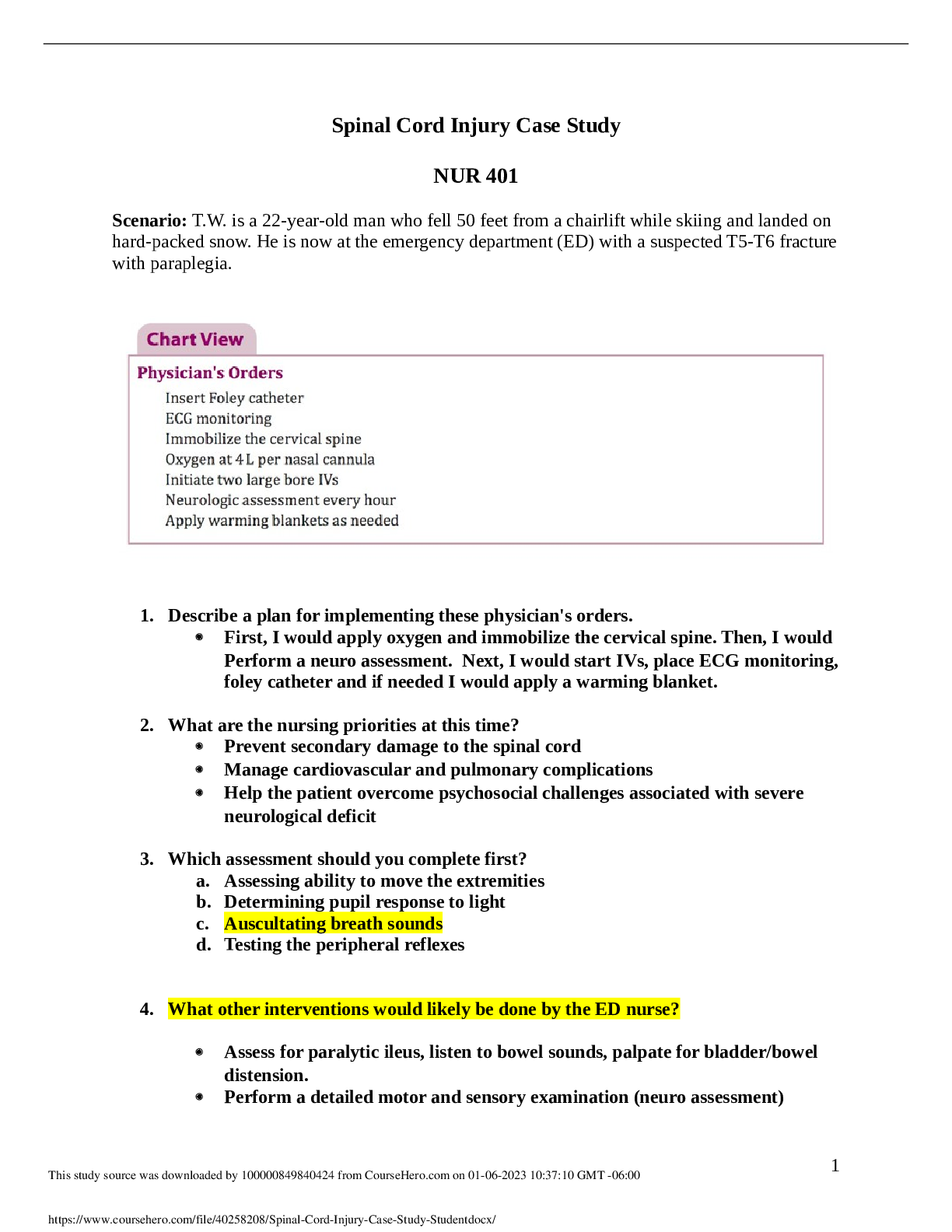
Week 3: Immunization Case Study Chamberlain University Week 3: Immunization Case Study The purpose of this assignment is to explore and identify vaccines available in the United States for pre... ventable diseases, understanding contraindications, precautions and recommendations from the Advisory Committee on Immunization Practice (ACIP). This paper will discuss 4 case studies related to childhood immunizations. Case Study 1 The first admission is a term newborn at 3.5 kg with normal labs and normal infant exam. The recommended vaccine that the newborn should receive is the Hepatitis B (Hep B) vaccine within the first 24 hours (CDC, 2019a). The 3-dose series should be initiated with a single dose antigen Hep B only as the first dose. The final dose should not be given before the baby reaches 24 weeks old (CDC, 2019a). This vaccine protects from Hep B and others positive with the disease, because children who have Hep B do not present with signs or symptoms. This vaccine also prevents the child from developing liver disease or cancers stemming from Hep B (CDC, 2019a). If mother was tested positive for Hep B there are other precautions that must be taken to protect the child. The recommended Hep B vaccine would still be administered as well as the Hepatitis B Immunoglobulin (HBIG) would be given within the first 12 hours of birth (CDC, 2019a). These injections would be administered at two different locations (separate extremities). A serologic test for anti-HB + HBsAg after the completion of the vaccine series between 9-12 months or during the next well visit after series is complete. Do not attempt serologic testing prior to 9 months because it may indicate passive anti-HB and HBIG administered from birth (CDC, 2019a). If the child comes back negative for their follow up serologic testing and the anti- HB level is ≤ 10 mIU/mL, then the child is protected and does not need further management. If > 10 mIU/mL, then it is recommended for revaccination with a single dose, then a serologic test 1-2 months later (CDC, 2019a). Women may continue to breast feed with child has received postexposure prophylaxis. If the mother’s Hepatitis B status is known, it is important to abide by the scheduled recommendations of administering the 3-dose Hep B series with the final dose to not be given prior to child turning 24 weeks (CDC, 2019a). It is also recommended for the mother to establish her Hep B status. Case Study 2 The second patient is a 2-month-old child present to the clinic for their follow up, who has already received their first Hep B dose. This is a term infant with no concerns from the parent. Examination was normal with no contraindications to vaccines. It is appropriate to administer the second Hep B dose, as well as the following: rotavirus (RV), Diphtheria/Tetanus/Pertussis (DTap), Haemophiles Influenzae (Hib), Pneumococcal Disease (PCV13), and Polio (IPV). Respectively, RV causes diarrhea, vomiting, and fever can cause a loss of body fluids leading to dehydration; the coating in the back of the nose or throat due to diphtheria can cause a blockage to the airway, resulting in difficulty breathing. The diphtheria toxin can affect the heart, causing an abnormal heart rhythms and even heart failure. It can also affect the nerves and lead to paralysis (unable to move parts of the body); painful muscle stiffness from tetanus can lead to muscle spasms can be strong enough to break a child’s spine or other bones (CDC, 2019a); whopping can result in a hospitalization from complications of pneumonia, seizures or brain damage; babies and children younger than 5 years old are most at risk for Hib and pneumococcal disease potentially causing a lifelong disability and possibly death (CDC, 2019a); lastly polio puts a child at risk for lifelong paralysis (CDC, 2019a). The child should return to the clinic in 2 months for their 4 months follow up to receive their second dose of DTap, Hib, IPV, PV13, and RV. Children immunizations are vital, but it also important to reduce the amount of trauma received from the injection. Vaccination combinations can be utilized to reduce the amount of injections. There are a few combination vaccinations available for children, they include: 1. Pediarix is a combination of DTap, Hep B and IPV 2. Proquad is a combination of MMR and Varicella 3. Kinrix is a combination of DTap and IPV 4. Pentacel is a combination of DTap, IPV and Hib The benefits of having combination vaccinations include decrease amount of injections, pain and discomfort, on time protection, as well as benefits for the parents such as decreased clinic visits and time off (CDC, 2019). Case Study 3. In this case study, a healthy 5-year-old child visits the clinic for a well-child checkup in November. All her routine immunizations are up to date. Examination is normal. It is recommended that the child receives the annual influenza vaccination (IIV or LAIV) (Grohskopf et al., 2020), MMR, Varicella, 5TH dose of DTaP, and 4th dose of IPV (CDC, 2019a). Anticipatory guidance for this child is to speak directly to child and ask them questions such as: do you feel healthy, what are favorite fruits and vegetables, or do you wash your hands after you use the bathroom. This will assess the child’s understanding as well as cognitive development. Other guidance that should be provided to the parents are possible side effects such as soreness, redness, and/or swelling at site of injection, headache, fever, nausea, and muscle aches (Grohskopf et al., 2020). During this visit, there are no contraindications for receiving the influenza vaccine. There are instances where it can be contraindicated to administer the influenza vaccine. They include, for the IIV, those who are less than 6 months old, allergies to egg; for the LAIV, is less than 2 years old, allergy to egg, a history of asthma and those who are on aspirin or salicylates due to an association of the development of Reyes Syndrome (Grohskopf et al., 2020). Other contraindications for the MMR, varicella, DTap, and IPV are related to previous severe allergy or those who have a history of being immunocompromised (CDC, 2019a). Case Study 4. In the final case study, we are introduced to an 11-year-old female for her routine well- child visit. Her immunizations are up to date and her exam was unremarkable. The following are recommended scheduled vaccinations for this child’s visit: annual influenza vaccine, 1st dose of HPV series, MenACWY vaccine, and Tdap. The two new vaccines are HPV and MenACWY; they are recommended to protect the child against Human Papillomavirus and MenACWY is to protect against meningococcal disease (CDC, 2019a). It is vital to educate the mother that these vaccines are pertinent to protecting the child infection or other potential exposures. As the child ages, the immunizations from childhood wear off and needs to have extended protection (CDC, 2019a). Once the education is provided to the mother, the second dose of HPV should be given to her 6–12 months after the first dose with a minimum interval of 5 months. If the follow up dose is given too soon, then another dose is to be given. The patient should also receive the second dose for the Meningococcal disease at age 16 (CDC, 2019a). Education to the child and parent is vital, as well as verbal feedback or teach back to assess patient and parent understanding about the vaccine, what it is for and anticipatory guidance. References Centers for Disease Control (CDC). (2019, August 01). Combination Vaccines – Fewer Shots Same Protection. Retrieved September 21, 2020, from https://www.cdc.gov/vaccines/parents/why-vaccinate/combination-vaccines.html Centers for Disease Control (CDC). (2019a, May 10). Vaccines for Your Children By Age. Retrieved September 19, 2020, from https://www.cdc.gov/vaccines/parents/by- age/index.html Grohskopf, L. A., Alyanak, E., Broder, K. R., Blanton, L. H., Fry, A. M., Jernigan, D. B., & Atmar, R. L. (2020). Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices — United States, 2020–21 Influenza Season. MMWR. Recommendations and Reports, 69(8), 1-24. doi:10.15585/mmwr.rr6908a1 Week 3: Immunization Case Study Chamberlain University Week 3: Immunization Case Study The purpose of this assignment is to explore and identify vaccines available in the United States for preventable diseases, understanding contraindications, precautions and recommendations from the Advisory Committee on Immunization Practice (ACIP). This paper will discuss 4 case studies related to childhood immunizations. Case Study 1 The first admission is a term newborn at 3.5 kg with normal labs and normal infant exam. The recommended vaccine that the newborn should receive is the Hepatitis B (Hep B) vaccine within the first 24 hours (CDC, 2019a). The 3-dose series should be initiated with a single dose antigen Hep B only as the first dose. The final dose should not be given before the baby reaches 24 weeks old (CDC, 2019a). This vaccine protects from Hep B and others positive with the disease, because children who have Hep B do not present with signs or symptoms. This vaccine also prevents the child from developing liver disease or cancers stemming from Hep B (CDC, 2019a). If mother was tested positive for Hep B there are other precautions that must be taken to protect the child. The recommended Hep B vaccine would still be administered as well as the Hepatitis B Immunoglobulin (HBIG) would be given within the first 12 hours of birth (CDC, 2019a). These injections would be administered at two different locations (separate extremities). A serologic test for anti-HB + HBsAg after the completion of the vaccine series between 9-12 months or during the next well visit after series is complete. Do not attempt serologic testing prior to 9 months because it may indicate passive anti-HB and HBIG administered from birth (CDC, 2019a). If the child comes back negative for their follow up serologic testing and the anti- HB level is ≤ 10 mIU/mL, then the child is protected and does not need further management. If > 10 mIU/mL, then it is recommended for revaccination with a single dose, then a serologic test 1-2 months later (CDC, 2019a). Women may continue to breast feed with child has received postexposure prophylaxis. If the mother’s Hepatitis B status is known, it is important to abide by the scheduled recommendations of administering the 3-dose Hep B series with the final dose to not be given prior to child turning 24 weeks (CDC, 2019a). It is also recommended for the mother to establish her Hep B status. Case Study 2 The second patient is a 2-month-old child present to the clinic for their follow up, who has already received their first Hep B dose. This is a term infant with no concerns from the parent. Examination was normal with no contraindications to vaccines. It is appropriate to administer the second Hep B dose, as well as the following: rotavirus (RV), Diphtheria/Tetanus/Pertussis (DTap), Haemophiles Influenzae (Hib), Pneumococcal Disease (PCV13), and Polio (IPV). Respectively, RV causes diarrhea, vomiting, and fever can cause a loss of body fluids leading to dehydration; the coating in the back of the nose or throat due to diphtheria can cause a blockage to the airway, resulting in difficulty breathing. The diphtheria toxin can affect the heart, causing an abnormal heart rhythms and even heart failure. It can also affect the nerves and lead to paralysis (unable to move parts of the body); painful muscle stiffness from tetanus can lead to muscle spasms can be strong enough to break a child’s spine or other bones (CDC, 2019a); whopping can result in a hospitalization from complications of pneumonia, seizures or brain damage; babies and children younger than 5 years old are most at risk for Hib and pneumococcal disease potentially causing a lifelong disability and possibly death (CDC, 2019a); lastly polio puts a child at risk for lifelong paralysis (CDC, 2019a). The child should return to the clinic in 2 months for their 4 months follow up to receive their second dose of DTap, Hib, IPV, PV13, and RV. Children immunizations are vital, but it also important to reduce the amount of trauma received from the injection. Vaccination combinations can be utilized to reduce the amount of injections. There are a few combination vaccinations available for children, they include: 1. Pediarix is a combination of DTap, Hep B and IPV 2. Proquad is a combination of MMR and Varicella 3. Kinrix is a combination of DTap and IPV 4. Pentacel is a combination of DTap, IPV and Hib The benefits of having combination vaccinations include decrease amount of injections, pain and discomfort, on time protection, as well as benefits for the parents such as decreased clinic visits and time off (CDC, 2019). Case Study 3. In this case study, a healthy 5-year-old child visits the clinic for a well-child checkup in November. All her routine immunizations are up to date. Examination is normal. It is recommended that the child receives the annual influenza vaccination (IIV or LAIV) (Grohskopf et al., 2020), MMR, Varicella, 5TH dose of DTaP, and 4th dose of IPV (CDC, 2019a). Anticipatory guidance for this child is to speak directly to child and ask them questions such as: do you feel healthy, what are favorite fruits and vegetables, or do you wash your hands after you use the bathroom. This will assess the child’s understanding as well as cognitive development. Other guidance that should be provided to the parents are possible side effects such as soreness, redness, and/or swelling at site of injection, headache, fever, nausea, and muscle aches (Grohskopf et al., 2020). During this visit, there are no contraindications for receiving the influenza vaccine. There are instances where it can be contraindicated to administer the influenza vaccine. They include, for the IIV, those who are less than 6 months old, allergies to egg; for the LAIV, is less than 2 years old, allergy to egg, a history of asthma and those who are on aspirin or salicylates due to an association of the development of Reyes Syndrome (Grohskopf et al., 2020). Other contraindications for the MMR, varicella, DTap, and IPV are related to previous severe allergy or those who have a history of being immunocompromised (CDC, 2019a). Case Study 4. In the final case study, we are introduced to an 11-year-old female for her routine well- child visit. Her immunizations are up to date and her exam was unremarkable. The following are recommended scheduled vaccinations for this child’s visit: annual influenza vaccine, 1st dose of HPV series, MenACWY vaccine, and Tdap. The two new vaccines are HPV and MenACWY; they are recommended to protect the child against Human Papillomavirus and MenACWY is to protect against meningococcal disease (CDC, 2019a). It is vital to educate the mother that these vaccines are pertinent to protecting the child infection or other potential exposures. As the child ages, the immunizations from childhood wear off and needs to have extended protection (CDC, 2019a). Once the education is provided to the mother, the second dose of HPV should be given to her 6–12 months after the first dose with a minimum interval of 5 months. If the follow up dose is given too soon, then another dose is to be given. The patient should also receive the second dose for the Meningococcal disease at age 16 (CDC, 2019a). Education to the child and parent is vital, as well as verbal feedback or teach back to assess patient and parent understanding about the vaccine, what it is for and anticipatory guidance. References Centers for Disease Control (CDC). (2019, August 01). Combination Vaccines – Fewer Shots Same Protection. Retrieved September 21, 2020, from https://www.cdc.gov/vaccines/parents/why-vaccinate/combination-vaccines.html Centers for Disease Control (CDC). (2019a, May 10). Vaccines for Your Children By Age. Retrieved September 19, 2020, from https://www.cdc.gov/vaccines/parents/by- age/index.html Grohskopf, L. A., Alyanak, E., Broder, K. R., Blanton, L. H., Fry, A. M., Jernigan, D. B., & Atmar, R. L. (2020). Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices — United States, 2020–21 Influenza Season. MMWR. Recommendations and Reports, 69(8), 1-24. doi:10.15585/mmwr.rr6908a1 [Show More]
Last updated: 1 year ago
Preview 1 out of 6 pages

Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Sep 06, 2021
Number of pages
6
Written in

Additional information
This document has been written for:
Uploaded
Sep 06, 2021
Downloads
0
Views
75