*NURSING > EXAM > NURSING 326 Psychiatric Mental Health Nursing Test Part 1, 2 and 3 BUNDLE | Chamberlain College of N (All)
NURSING 326 Psychiatric Mental Health Nursing Test Part 1, 2 and 3 BUNDLE | Chamberlain College of Nursing | Download To Score An A
Document Content and Description Below
Psychiatric Mental Health Nursing Test Part 1 All the questions in the quiz along with their answers are shown below. Your answers are bolded. The correct answers have a green background while th... e incorrect ones have a red background. 1. Your patient is very dependent and submissive. There are times that the patient is very clingy. This behavior reflects what type of personality disorder? ▪ a. Antisocial personality ▪ b. Dependent Personality ▪ c. Manic behavior ▪ d. Anxiety disorder Dependent personality is characterized by dependence, submission and being clingy. Antisocial personality is impulsive, aggressive and manipulative. 2. The appropriate therapeutic distance between you and a psychiatric patient is? ▪ a. 12 inches ▪ b. 35 inches ▪ c. 12 feet ▪ d. 4 feet Intimate zone: 0-18 inches. Parents with young children, people who mutually desire personal contact, or people whispering. Personal zone: 18-36 inches. Between family and friends talking. Social zone: 4-12 feet. Communication in social, work and business settings. Public zone: 12-25 inches. Speaker and an audience. Therapeutic distance: 3-6 feet. 3. Nurse Anna is instructing the new nurse to the psychiatric set-up. She also reminded her to use her therapeutic communication skills in dealing with clients. Which of the following techniques enlaces therapeutic communication? ▪ a. What are you thinking about? ▪ b. What made you think that way? ▪ c. Why did you say that? ▪ d. Let’s not talk about that. What do you think? This is using the therapeutic technique BROAD OPENING that allows the client to take the initiative to introduce a topic. 4. Mr. Juan is diagnosed with Alzheimer’s disease. The nurse’s intervention should focus on helping the client be oriented with the physical set-up and daily events. Which of the following is the most effective nursing intervention in orienting patients who has Alzheimer’s disease? ▪ a. Encourage the client to talk to family members to reminisce things ▪ b. Provide simple and easily understood directions ▪ c. Perform tasks with a variety of activities each day ▪ d. Have the client socialize with other patients Providing a daily routine and directions easily understood by the client would help orienting a client with Alzheimer’s disease. 5. A therapy that focuses on the remotivation of clients by directing their attention outside themselves to relieve preoccupation with personal thoughts, feelings, and attitudes is known as: ▪ a. Pharmacologic therapy ▪ b. Music therapy ▪ c. Occupational therapy ▪ d. Recreational therapy Recreational therapy- Focuses on remotivation of clients by directing their attention outside themselves to relieve preoccupation with personal thoughts, feelings, and attitudes. Clients learn to cope with stress through activity. Activities are planned to meet specific needs and encourage the development of leisure-time activities or hobbies. Recreational therapy is especially useful with those people who have difficulty relating to others (e.g., the regressed, withdrawn, or immobilized person). Examples of recreational activities include group bowling, picnics, sing-along, and bingo. 6. The 12-year old male patient looks like the nurse’s younger brother who is missing for years. During assessment and in the implementation of nursing care the nurse prioritizes this client. One day, when she found the boy crying in his room she hugged him and cried with him. This is an example of: ▪ a. Counter-transference ▪ b. Transference ▪ c. Resistance ▪ d. Denial When the nurse displays affection or emotion toward the client counter-transference is occurring. Transference is observed when the patient is displaying emotions towards the nurse. 7. A schizophrenic client is under your care. In reinforcing the functional behavior of this client what will the nurse do? ▪ a. Enumerate the symptoms of schizophrenia to the client ▪ b. Correct delusional thoughts to orient to reality ▪ c. Compliment the client for cessation of acting out behaviors ▪ d. Encourage the client to drink his medications religiously According to B.F. Skinner’s behavior medication technique, a client should be praise for good behaviors to help him modify his faulty actions. 8. A client was brought to the ER. Based on the significant others, the client had a history of shop stealing. However, no self-mutilating activities are committed by the client. During the interview, the client is very manipulative and aggressive and impulsive. What personality disorder most likely the client has? ▪ a. Antisocial ▪ b. Histrionic ▪ c. Narcissistic ▪ d. Borderline Antisocial P.D is characterized by aggression, manipulation and impulsivity. Histrionic people are emotional, dramatic and theatrical. Narcissistic people are boastful, egotistical and have superiority complex. Borderline PD is characterized by impulsivity, self-destruction and very unstable mood. 9. When the client told the nurse that he feels good when he mutilates or cuts himself the novice psychiatric nurse answered, “Do you know the risks involved when you cut yourself?” what type of nontherapeutic communication is the nurse using? ▪ a. Defending ▪ b. Testing ▪ c. Making stereotyped comments ▪ d. Disagreeing Testing is appraising a client’s degree of insight such as by asking the patient of the risks involved when he cut himself. This forces the client to recognize his problems. Defending is attempting to protect someone from a verbal attack. Stereotyped comments are meaningless clichés such as “it’s for your own good.” 10. A therapy that assists with discharge planning and rehabilitation, focusing on vocational skills and activities of daily living (ADL) to raise self-esteem and promote independence is called: ▪ a. Behavior modification ▪ b. Milieu therapy ▪ c. Recreational therapy ▪ d. Occupational therapy Occupational therapy - Assists with discharge planning and rehabilitation, focusing on vocational skills and activities of daily living (ADL) to raise self-esteem and promote independence 11. Nurse Marie is caring for a patient that underwent alcohol detoxification. Which of the following symptoms would Nurse Marie be most concern? ▪ a. Fever ▪ b. Delusions ▪ c. Excessive sweating ▪ d. Increase BP Once hallucinations and delusions are present; the client’s condition will most likely progress to delirium tremens. 12. The Distance that is observed when family members or friends are talking is under what zone: ▪ a. Intimate ▪ b. Therapeutic ▪ c. Personal ▪ d. Social Personal zone: 18-36 inches. Between family and friends talking. Intimate zone: 0-18 inches. Parents with young children, people who mutually desire personal contact, or people whispering. Social zone: 4-12 feet. Communication in social, work and business settings. Therapeutic distance: 3-6 feet. 13. The client is sharing Nurse Marie about his experiences. Suddenly, he paused, looked to the nurse and is hesitant to continue. The nurse responded, “Go on, and tell me about it.” What therapeutic communication technique is the nurse using? ▪ a. Exploring ▪ b. Focusing ▪ c. Encouraging expression ▪ d. General leads General leads indicate that the nurse is listening and following what the client is saying without taking away the initiative for the interaction. They also encourage the client to continue if he or she is hesitant or uncomfortable of the topic. Examples include, “Go on,” “Tell me about it,” and “And then?” 14. In a therapeutic communication, “why questions” are discouraged. For what reason is this question not useful? ▪ a. The question is intimidating and the client may be defensive in trying to explain him/herself. ▪ b. It forces the client to recognize his or her problems. The client’s acknowledgement that s/he doesn’t know things may be helpful to the nurse’s needs but not the client. ▪ c. It indicates that the client is right rather than wrong. ▪ d. It tends to make the client used and invaded. Using “why question” is asking to client the client to provide reasons for thoughts, feeling and behaviors. The question is intimidating and the client may be defensive in trying to explain him/herself. 15. An 18 year old client is brought to the ER due to a suicidal attempt. Her mother told the nurse that she has been drinking alcohol for the last 3 weeks and is depressed. In caring for this patient what is the most important consideration? ▪ a. Administering antidepressant medications ▪ b. Alcohol detoxification ▪ c. Allowing the client to participate in a therapy ▪ d. Close monitoring Safety is the most important consideration in client with a suicidal attempt. This is achieved by removing harmful objects around the client and monitoring the client closely. 16. In using a therapeutic communication technique interpreting client cues and signals is very important. Clear statements of intent such as the client saying that he wants to kill himself is a/an: ▪ a. Covert cues ▪ b. Abstract messages ▪ c. Concrete messages ▪ d. Overt cues Overt cues are clear statements of intent such as the client saying, “I want to die.” Covert cues are vague or hidden messages such as if a client verbalizes, “No one can help me.” Abstract messages are unclear patterns of words that often contain figures of speech that are difficult to interpret. Example is when the nurse asked the client, “What are you doing here?” Concrete messages are patterns of words that the nurse uses where words are explicit and does need an explanation. 17. A client was admitted due to self-mutilation. One day during one of the sessions, the client told the nurse that cutting himself feels great. What would be the nurse’s best response? ▪ a. “Do you know the risks involved when you cut yourself?” ▪ b. “I don’t want to hear about that!” ▪ c. “The behavior of cutting is not acceptable.” ▪ d. “Tell me more about that.” Presenting reality is the best in this situation as it is obvious that the client is misinterpreting the reality. Asking the client to tell the nurse more about is validating the actions of cutting himself. 18. A behavior that can indicate the speaker’s thoughts, feelings, needs and values that he or she acts out unconsciously is called: ▪ a. Verbal communication ▪ b. Communication ▪ c. Nonverbal communication ▪ d. Congruent message Nonverbal communication is the behavior that accompanies verbal content such as body language, eye contact, facial expression, tone of voice, speed and hesitations in speech, grunts and groans and distance from the listeners. This type of communication can indicate the speaker’s thoughts, feelings, needs and values that he or she acts out unconsciously. 19. Restraints are only used for a certain reason. Which of the following is an appropriate reason for placing a client in restraints? ▪ a. Punishment for stealing the other client’s things ▪ b. Self- harming behaviors ▪ c. Verbal abuse ▪ d. Not drinking medications One the patient attempts to harm himself, restraints is acceptable. 20. If a client is on restraints which of the following would the nurse do? ▪ a. Leave the client in the room for the whole 8 hours ▪ b. Do not allow the client to eat ▪ c. Take pictures of the client for evaluation ▪ d. monitor the extremity circulation When a client is placed on restraint, monitor the circulation to prevent physiologic damage of the extremity. 21. A client is scheduled for an electroconvulsive therapy (ECT). Which of the following medications can be given to the client before the procedure? ▪ a. Atropine ▪ b. Epinephrine ▪ c. Hydralazine ▪ d. Phenobarbital Before ECT atropine can be given to the client to decrease oral and respiratory function thereby preventing risks of aspiration. Atropine is antiarrythmic and at the same time an anticholinergic medication. 22. To ensure that your client knows about the procedure, risks and outcome and has been informed of the other alternative therapy. Which of the following must be accomplished? ▪ a. A signed informed consent by a client’s family member ▪ b. A signed informed consent by a 23-year old client who has voluntarily admitted himself in the unit. ▪ c. A signed informed consent of a 23-year old client’s parent ▪ d. A signed informed consent by a 17-year old client Clients of legal age can sign an informed consent. 23. The client says that he is hearing voices. What is nurse’s initial response? ▪ a. “I don’t hear any voices.” ▪ b. “From where are those voices coming from?” ▪ c. “What are the voices telling you?” ▪ d. “Are you sure about that?” Initially the nurse has to assess what the voices are telling the client to promote safety. Because if the voices are telling the client to kill himself or someone safety precautions must be implemented. 24. What is the most important criteria that must be accomplished by the nurse before dealing with psychiatric patients? ▪ a. Salary rate ▪ b. Self-awareness ▪ c. Self-understanding ▪ d. Standard of nursing practice Before a nurse can understand him/herself, being aware of what his/her strengths, weaknesses, limitations, belief and principles is very essential. A nurse who barely knows and understand herself cannot effectively establish a therapeutic communication with psychiatric clients. 25. If a client is a chain smoker, how should his medication dosage be adjusted? ▪ a. Same medication dose ▪ b. Increase the dose ▪ c. Decrease the dose ▪ d. Withhold the dose Smoking cigarettes increases the metabolism of some psychiatric medications, thus, medication dose should be increased. Psychiatric Mental Health Nursing Test Part 2 All the questions in the quiz along with their answers are shown below. Your answers are bolded. The correct answers have a green background while the incorrect ones have a red background. 1. Nurse Renalyn discovers that a male client with obsessive-compulsive disorder (OCD) is attempting to resist the compulsion. Based on this finding, the nurse should assess the client for: ▪ a. Feelings of failure ▪ b. Depression ▪ c. Excessive fear ▪ d. Increased anxiety An obsessive-compulsive client who attempts to resist the compulsion must be evaluated for increased anxiety. A compulsion is a repetitive, intentional behavior that the client performs in response to a certain obsession; it's aimed at neutralizing or decreasing anxiety. Resisting the compulsion may increase the client's anxiety. Although a client with OCD may have feelings of failure, depression, and excessive fear, these aren't responses to resisting the compulsion. 2. A female client comes to the emergency department while experiencing a panic attack. Nurse Jonathan can best respond to a client having a panic attack by: ▪ a. Staying with the client until the attack subsides ▪ b. Telling the client everything is under control ▪ c. Telling the client to lie down and rest ▪ d. Talking continually to the client by explaining what is happening The nurse should remain with the client until the attack subsides. If the client is left alone he may become more anxious. Giving false reassurance is inappropriate in this situation. The client should be allowed to move around and pace to help expend energy. The client may be so overwhelmed that he can't follow lengthy explanations or instructions, so the nurse should use short phrases and slowly give one direction at a time. 3. Nurse Krishna notices that a female client with obsessive-compulsive disorder dresses and undresses numerous times each day. Which comment by the nurse would be most therapeutic? ▪ a. "I saw you change clothes several times today. That must be very tiring." ▪ b. "Try to dress only once per day so you won't be so tired." ▪ c. "It bothers me to see you always so busy." ▪ d. "It's foolish to change clothes so many times in one day." Option A focuses on the client's feelings in an empathetic way, helping to reduce the intensity of the ritualistic behavior and promoting trust and rapport. Implying that the client's behavior is tiring, bothersome, or foolish would convey disapproval, impede trust and rapport, promote dysfunctional behavior, and worsen anxiety. 4. Nurse Luz is formulating a short-term goal for a client suffering from a severe obsessive-compulsive disorder (OCD). An appropriately stated short-term goal is that after 1 week, the client will: ▪ a. Demonstrate decreased anxiety. ▪ b. Participate in a daily exercise group. ▪ c. Identify the underlying reasons for rituals. ▪ d. State that the rituals are irrational. Participating in a daily exercise group refocuses the client's time toward adaptive activities and may reduce anxiety. Option A isn't stated specifically enough to allow for evaluation; for this goal to be measurable, specific objectives must be stated such as, "The client will verbalize feeling less anxious." Option C is incorrect because identifying the underlying reasons for rituals takes time and isn't a realistic goal after 1 week. Most clients with OCD are aware that the ritual is irrational but can't stop it, making option D inappropriate as well. 5. Because antianxiety agents such as chlordiazepoxide (Librium) can potentiate the effects of other drugs, nurse Raquel should incorporate which of the following instructions in her teaching plan? ▪ a. Avoid mixing antianxiety agents with alcohol or other central nervous system (CNS) depressants ▪ b. Avoid taking antianxiety drugs at bedtime ▪ c. Avoid taking antianxiety drugs on an empty stomach ▪ d. Avoid consuming aged cheese when taking antianxiety agents Potentiating effect refers to a drug's ability to increase the potency of another drug if taken together. Therefore, the client should be instructed to avoid alcohol while taking Librium because it potentiates the drug's CNS depressant effect. Taken at bedtime, this drug will induce sleep. Librium comes in capsule form and usually can be taken with water. Aged cheese is restricted with monoamine oxidase inhibitors, not Librium. 6. Danilo, arrives on the psychiatric unit exhibiting extreme excitement, disorientation, incoherent speech, agitation, frantic and aimless physical activity, and grandiose delusion. Which nursing diagnosis takes highest priority for the client at this time? ▪ a. Ineffective individual coping ▪ b. Hopelessness ▪ c. Risk for injury ▪ d. Disturbed identity This client is at increased risk for injury because of severe hyperactivity, disorientation, and agitation. Although the other options also are appropriate, the client's safety takes highest priority. The nurse should take immediate action to protect the client from injury. 7. Gina, age 18, is highly dependent on her parents and fears leaving home to go away to college. Shortly before the fall semester starts, she complains that her legs are paralyzed and is rushed to the emergency department. When physical examination rules out a physical cause for her paralysis, the physician admits her to the psychiatric unit where she is diagnosed with conversion disorder. The client asks nurse Rose, "Why has this happened to me?" What is the nurse's best response? ▪ a. "You've developed this paralysis so you can stay with your parents. You must deal with this conflict if you want to walk again." ▪ b. "It must be awful not to be able to move your legs. You may feel better if you realize the problem is psychological, not physical." ▪ c. "Your problem is real but there is no physical basis for it. We'll work on what is going on in your life to find out why it's happened." ▪ d. "It isn't uncommon for someone with your personality to develop a conversion disorder during times of stress." The nurse must be honest with the client by telling her that the paralysis has no physiologic cause while also conveying empathy and acknowledging that her symptoms are real. The client will benefit from psychiatric treatment, which will help her understand the underlying cause of her symptoms. After the psychological conflict is resolved, her symptoms will disappear. Saying that it must be awful not to be able to move her legs wouldn't answer the client's question; knowing that the cause is psychological wouldn't necessarily make her feel better. Telling her that she has developed paralysis to avoid leaving her parents or that her personality caused her disorder wouldn't help her understand and resolve the underlying conflict. 8. Dr. Luistro orders a new medication for a client with generalized anxiety disorder. During medication teaching, which statement or question by the nurse Kesselyn would be most appropriate? ▪ a. "Take this medication. It will reduce your anxiety." ▪ b. "Do you have any concerns about taking the medication?" ▪ c. "Trust us. This medication has helped many people. We wouldn't have you take it if it were dangerous." ▪ d. "How can we help you if you won't cooperate?" Providing an opportunity for the client to express concerns about a new medication and to make a choice about taking it can help the client regain a sense of control over his life. The client has the right to refuse the medication. Instead of simply ordering the client to take it, as in option A, the nurse should provide the information the client needs to make an informed decision. Attempting to make the client feel guilty, as in option C, or threatening the client, as in option D, would increase anxiety. 9. After seeking help at an outpatient mental health clinic, a client who was raped while walking her dog is diagnosed with posttraumatic stress disorder (PTSD). Three months later, the client returns to the clinic, complaining of fear, loss of control, and helpless feelings. Which nursing intervention is most appropriate for this client? ▪ a. Exploring the meaning of the traumatic event with the client ▪ b. Allowing the client time to heal ▪ c. Giving sleep medication, as prescribed, to restore a normal sleep-wake cycle ▪ d. Recommending a high-protein, low-fat diet The client with PTSD needs encouragement to examine and understand the meaning of the traumatic event and consequent losses. Otherwise, symptoms may worsen and the client may become depressed or engage in self- destructive behavior such as substance abuse. The client must explore the meaning of the event and won't heal without this, no matter how much time passes. Behavioral techniques, such as relaxation therapy, may help decrease the client's anxiety and induce sleep. The physician may prescribe antianxiety agents or antidepressants cautiously to avoid dependence; sleep medication is rarely appropriate. A special diet isn't indicated unless the client also has an eating disorder or a nutritional problem. 10. Jane is admitted to an inpatient psychiatric unit for treatment of obsessive-compulsive symptoms. Obsessive- compulsive disorder (OCD) is associated with: ▪ a. Physical signs and symptoms with no physiologic cause ▪ b. Apprehension ▪ c. Inability to concentrate ▪ d. Repetitive thoughts and recurring, irresistible impulses OCD is characterized by repetitive thoughts that the client can't control or exclude from consciousness, along with recurring, irresistible impulses to perform a particular action. Physical signs and symptoms with no physiologic cause typify somatoform disorder. Apprehension and inability to concentrate characterize anxiety disorders. 11. A client with obsessive-compulsive disorder and ritualistic behavior must brush the hair back from his forehead 15 times before carrying out any activity. Nurse Leo notices that the client's hair is thinning and the skin on the forehead is irritated — possible effects of this ritual. When planning the client's care, the nurse should assign highest priority to: ▪ a. Helping the client identify how the ritualistic behavior interferes with daily activities ▪ b. Exploring the purpose of the ritualistic behavior ▪ c. Setting consistent limits on the ritualistic behavior if it harms the client or others ▪ d. Using problem solving to help the client manage anxiety more effectively Client safety is the paramount concern and must be maintained. Therefore, setting consistent limits on potentially harmful ritualistic behavior takes highest priority. Although the other options are important, they take lower priority. For instance, helping the client identify how the ritualistic behavior interferes with daily activities increases the client's motivation for using more effective coping behavior. Exploring the purpose of the ritualistic behavior helps the client see this behavior as an attempt to control anxiety. As the client learns new ways to manage anxiety, the ritualistic behavior is likely to decrease. 12. During alprazolam (Xanax) therapy, nurse Rachel should be alert for which dose-related adverse reaction? ▪ a. Ataxia ▪ b. Hepatomegaly ▪ c. Urticaria ▪ d. Rash Dose-related adverse reactions to alprazolam include drowsiness, confusion, ataxia, weakness, dizziness, nystagmus, vertigo, syncope, dysarthria, headache, tremor, and a glassy-eyed appearance. These dose-related reactions diminish as therapy continues. Although hepatomegaly may occur with benzodiazepine use, this adverse reaction is rare and isn't dose-related. Idiosyncratic reactions to benzodiazepines may include a rash and acute hypersensitivity reactions; however, they aren't dose-related. 13. A client is admitted to the psychiatric unit with a diagnosis of conversion disorder. Since witnessing the beating of his wife at gunpoint, he has been unable to move his arms, complaining that they are paralyzed. When planning the client's care, nurse Jay should focus on: ▪ a. Helping the client identify and verbalize feelings about the incident ▪ b. Convincing the client that his arms aren't paralyzed ▪ c. Developing rehabilitation strategies to help the client learn to live with the disability ▪ d. Talking about topics other than the beating to avoid causing anxiety In conversion disorder, the client represses and converts emotional conflicts into motor, sensory, or visceral symptoms with no physiologic cause. Interventions should focus on helping the client identify the underlying emotional problem. A client with conversion disorder can't be convinced that the physical problem isn't real; attempts to convince him may lead him to seek other health care providers who may accept the reality of his symptoms. Treating the physical symptoms as long-term or permanent may encourage the client to maintain them. Ignoring the cause of the symptoms would prevent the client from dealing with his feelings about his wife's beating. 14. A male client with borderline personality disorder tells nurse Valerie, "You're the only nurse who really understands me. The others are mean." The client then asks the nurse for an extra dose of antianxiety medication because of increased anxiety. How should the nurse respond? ▪ a. "I'll talk to the physician right away. I don't think they give you enough medicine." ▪ b. "I'll have to discuss your request with the team. Can we talk about how you're feeling right now?" ▪ c. "I don't want to hear you say negative things about the other nurses." ▪ d. "You know you can't have extra medication. Why do you keep asking?" This response appropriately focuses on the emotional content of the client's message and helps the client identify feelings. Focusing on the request for extra medication would allow the client to ignore the underlying emotional issues. Clients with borderline personality disorder commonly divide the staff into "good guys" and "bad guys" to meet their needs; staff members must maintain consistency and a united front at all times. The nurse shouldn't take the client's statements personally because this would interfere with the ability to maintain a therapeutic relationship. 15. Angel, is admitted to the unit visibly anxious. When assessing her, the nurse would expect to see which of the following cardiovascular effects produced by the sympathetic nervous system? ▪ a. Syncope ▪ b. Decreased blood pressure ▪ c. Increased heart rate ▪ d. Decreased pulse rate Sympathetic cardiovascular responses to stress include increased heart rate, cardiac contractility, and cardiac output; increased blood pressure; and peripheral vasoconstriction. Syncope is a response to parasympathetic stimulation. 16. A male client with Alzheimer's disease has a nursing diagnosis of Risk for injury related to memory loss, wandering, and disorientation. Which nursing intervention should appear in this client's plan of care to prevent injury? ▪ a. Provide the client with detailed instructions ▪ b. Keep the client sedated whenever possible ▪ c. Remove hazards from the environment ▪ d. Use restraints at all times By removing environmental hazards, such as bottles of hydrogen peroxide and benzoin, the nurse can help prevent injury to the client. For a client with Alzheimer's disease, the nurse should provide single, simple instructions, rather than many detailed instructions. The nurse should administer medication as prescribed and as needed — not to keep the client sedated. The nurse should use restraints only when required to prevent self-harm by the client. 17. Rudy was found wandering in a local park is unable to state who or where he is or where he lives. He is brought to the emergency department, where his identification is eventually discovered. The client's wife states that he was diagnosed with Alzheimer's disease 3 years ago and has had increasing memory loss. She tells nurseAngelie she is worried about how she'll continue to care for him. Which response by the nurse would be most helpful? ▪ a. "Because of the nature of your husband's disease, you should start looking into nursing homes for him." ▪ b. "What aspect of caring for your husband is causing you the greatest concern?" ▪ c. "You may benefit from a support group called Mates of Alzheimer's Disease Clients." ▪ d. "Do you have any children or friends who could give you a break from his care every now and then?" The nurse should determine the specific concerns of the client's wife. Jumping to conclusions regarding the client's need for a nursing home or other care placement options would be inappropriate. The nurse must tailor care to the client and family, focusing on their needs. Although support groups, children, and friends may prove helpful to the client's wife, the nurse must establish a plan for continued care that addresses her specific concerns. 18. Nurse Agnes is aware that nursing action most appropriate when trying to diffuse a male client's impending violent behavior? ▪ a. Helping the client identify and express feelings of anxiety and anger ▪ b. Involving the client in a quiet activity to divert attention ▪ c. Leaving the client alone until he can talk about his feelings ▪ d. Placing the client in seclusion In many instances, the nurse can diffuse impending violence by helping the client identify and express feelings of anger and anxiety. Such statements as "What happened to get you this angry?" may help the client verbalize feelings rather than act on them. Close interaction with the client in a quiet activity may place the nurse at risk for injury should the client suddenly become violent. An agitated and potentially violent client shouldn't be left alone or unsupervised because the danger of the client's acting out is too great. The client should be placed in seclusion only if other interventions fail or the client requests this. Unlocked seclusion can be helpful for some clients because it reduces environmental stimulation and provides a feeling of security. 19. A male client has been taking imipramine (Tofranil), 125 mg by mouth daily, for 1 week. Now the client reports wanting to stop taking the medication because he still feels depressed. At this time, what is the best response of nurse Charlyn? ▪ a. "Imipramine may not be the most effective medication for you. You should call your physician for further evaluation." ▪ b. "Because imipramine must build to a therapeutic level, it may take 2 to 3 weeks to reduce depression." ▪ c. "The physician may need to increase the dosage for you to get the medication's maximum benefit." ▪ d. "Don't stop taking the medication abruptly because you may develop serious adverse effects." Antidepressant agents, such as imipramine, don't produce antidepressant effects until they reach a therapeutic level in the blood, usually about 2 to 3 weeks after the initial dose. Therefore, the nurse should encourage the client to continue therapy at least until the drug reaches that level. After this time, if the client's depression doesn't abate, the nurse may use the other responses. 20. A male client with Alzheimer's disease mumbles incoherently and rambles in a confused manner. To help redirect the client's attention, nurse Mark should encourage the client to: ▪ a. Fold towels and pillowcases ▪ b. Play cards with another client ▪ c. Participate in a game of charades ▪ d. Perform an aerobic exercise Folding towels and pillowcases is a simple activity that redirects the client's attention. Also, because this activity is familiar, the client is likely to perform it successfully. Cards, charades, and aerobic exercise are too complicated for a confused client. 21. Nurse Francis is aware that the nursing preparations for a client undergoing electroconvulsive therapy (ECT) resemble those used for: ▪ a. Physical therapy ▪ b. Neurologic examination ▪ c. General anesthesia ▪ d. Cardiac stress testing The nurse should prepare a client for ECT in a manner similar to that for general anesthesia. For example, the client should receive nothing by mouth for 8 hours before ECT to reduce the risk of vomiting and aspiration. Also, the nurse should have the client void before treatment to decrease the risk of involuntary voiding during the procedure; remove any full dentures, glasses, or jewelry to prevent breakage or loss; and make sure the client is wearing a hospital gown or loose-fitting clothing to allow unrestricted movement. Usually, these preparations aren't indicated for a client undergoing physical therapy, neurologic examination, or cardiac stress testing. 22. Nurse Hershey must administer activated charcoal before administering certain other drugs to a client who's taken an overdose. Which drug is rendered inactive when administered concomitantly with activated charcoal? ▪ a. Warfarin sodium (Coumadin) ▪ b. Ipecac syrup ▪ c. Simethicone (Phazyme) ▪ d. Famotidine (Pepcid) Ipecac syrup is rendered inactive when administered concomitantly with activated charcoal. 23. Dr. Tan orders electroconvulsive therapy (ECT) for a severely depressed client who fails to respond to drug therapy. When teaching the client and family about this treatment, nurse Bernadeth should include which most important point about ECT? ▪ a. An anesthesiologist will administer ECT ▪ b. ECT can cure depression ▪ c. ECT will induce a seizure ▪ d. The client will remember the shock of ECT but not the pain Reserved for clients with acute depression who don't respond to pharmacologic or psychiatric measures, ECT is the passage of an electrical current through the brain to induce a brief seizure. According to ECT proponents, the seizure causes desirable changes in neurotransmitters and receptor sites similar to those caused by antidepressant drugs. ECT is administered by a physician or an anesthesiologist. Although ECT may reduce the severity of depression, it doesn't necessarily cure it. Before ECT, the client receives a medication that provides short-term amnesia of the entire event. 24. Julius, an adolescent becomes increasingly withdrawn, is irritable with family members, and has been getting lower grades in school. After giving away a stereo and some favorite clothes, the adolescent is brought to the community mental health agency for evaluation. This adolescent is at risk for: ▪ a. Suicide ▪ b. Anorexia nervosa ▪ c. School phobia ▪ d. Psychotic break Changes in academic performance and familial communications, social withdrawal, and giving away of treasured possessions suggest that this adolescent is contemplating suicide. Anorexia nervosa would cause weight loss and other related symptoms. This adolescent's signs and symptoms don't suggest fear of school and typify depression, not psychosis. 25. Nurse Bea is aware the when preparing a client for electroconvulsive therapy (ECT), she should make sure that: ▪ a. The client sees family members immediately before the procedure ▪ b. The client is scheduled for a brain scan immediately after the procedure ▪ c. The client has undergone a thorough medical evaluation ▪ d. The client has received lithium carbonate (Lithonate) Before an ECT treatment, the nurse should ensure that the client has had a medical evaluation that includes an ECG, a chest X-ray, neurologic and laboratory tests, and spinal X-rays, if indicated. Although making sure that the client sees family members immediately before the procedure would be appropriate, it's unnecessary (unless the client requests this). A brain scan isn't required after ECT because it can't evaluate the therapeutic effects of this treatment. Lithium must be discontinued before ECT because it prolongs the effects of succinylcholine chloride (Anectine), a muscle relaxant given just before the shock is delivered. Psychiatric Mental Health Nursing Test Part 3 All the questions in the quiz along with their answers are shown below. Your answers are bolded. The correct answers have a green background while the incorrect ones have a red background. 1. A male adult client with bipolar disorder is being treated with lithium for the first time. Nurse Joy should observe the client for which common adverse effect of lithium? ▪ a. Sexual dysfunction ▪ b. Constipation ▪ c. Polyuria ▪ d. Seizures Polyuria commonly occurs early in the treatment with lithium and could result in fluid volume deficit. Sexual dysfunction isn't a common adverse effect of lithium; it's more common with sedatives and tricyclic antidepressants. Diarrhea, not constipation, occurs with lithium.Constipation can occur with other psychiatric drugs, such as antipsychotic drugs. Seizures may be a later sign of lithium toxicity. 2. Mr. Velasquez is brought to the crisis intervention center by his wife, who states that he has been increasingly listless and less involved with his family recently. She reports that he sleeps poorly, eats little, and can barely perform basic self-care activities. She also reveals that 3 months ago he was in a car accident in which his best friend was killed. After the physician diagnoses acute depression, the nurse should anticipate administering: ▪ a. paroxetine (Paxil), 20 mg by mouth (P.O.) every morning ▪ b. amitriptyline (Elavil), 20 mg P.O. daily ▪ c. doxepin (Sinequan), 500 mg daily ▪ d. imipramine (Tofranil), 500 mg daily All of the drugs listed are antidepressants that may be prescribed for this client. However, paroxetine, 20 mg P.O. every morning, is the only correct dosage. Amitriptyline is usually started at 75 to 150 mg P.O. daily in divided doses. Doxepin is started at 25 to 50 mg daily and may be titrated upward to a maximum daily dose of 300 mg. Imipramine is started at 50 to 75 mg daily and, if tolerated, titrated upward to a maximum daily dose of 300 mg. 3. Nurse Vanessa is administering venlafaxine (Effexor) 75 mg by mouth daily to a client diagnosed with depression. What type of agent is venlafaxine? ▪ a. Monoamine oxidase inhibitor ▪ b. Tricyclic antidepressant ▪ c. Second-generation antidepressant ▪ d. Lithium derivative Physicians prescribe venlafaxine to treat depressive disorders; the drug is a second-generation antidepressant agent 4. At night, Victor a geriatric client with senile dementia wanders into other clients' rooms, awakening them. What is the best nursing intervention for dealing with the client's insomnia and nocturnal roaming? ▪ a. Administer a benzodiazepine at bedtime as prescribed ▪ b. Administer a phenothiazine at bedtime as prescribed ▪ c. Administer a barbiturate at bedtime as prescribed ▪ d. Lock the client's door at bedtime In geriatric clients, phenothiazines are preferred for sedation and thought clearing. Benzodiazepines usually are avoided because of the risk of addiction, cardiovascular complications, and impaired motor coordination. Barbiturates also are avoided because they may cause delirium, confusion, excitement, and addiction. Locking the door is inappropriate and would violate the client's rights. 5. Catherine has received treatment for depression for 3 weeks. Which behavior suggests that the client is recovering from depression? ▪ a. The client talks about the difficulties of returning to college after discharge ▪ b. The client spends most of the day sitting alone in the corner of the room. ▪ c. The client wears a hospital gown instead of street clothes. ▪ d. The client shows no emotion when visitors leave. By talking about returning to college, the client is demonstrating an interest in making plans for the future, which is a sign of recovery from depression. Decreased socialization, lack of interest in personal appearance, and lack of emotion are all symptoms of depression. 6. Nurse Mary Anne is caring for a client who has been diagnosed with hypochondriasis. The client attributes his cough to tuberculosis. A chest X-ray and skin test are negative for tuberculosis. The client begins to complain about the sudden onset of chest pain. How should the nurse react initially? ▪ a. Let the client know the nurse understands his fears of serious illness. ▪ b. Encourage the client to discuss his fear of having a serious illness. ▪ c. Report the complaint of chest pain to the physician. ▪ d. Determine if the illness is fulfilling a psychological need for the client. Because of the risk of missing an actual medical problem, any new symptoms reported by a client with hypochondriasis should be reported to the physician. The other interventions are appropriate after the nurse has determined that the client doesn't have a serious medical disorder. 7. Linda, a 54-year-old was found unconscious on the floor of her bathroom with self-inflicted wrist lacerations. An ambulance was called and the client was taken to the emergency department. When she was stable, the client was transferred to the inpatient psychiatric unit for observation and treatment with antidepressants. Now that the client is feeling better, which nursing intervention is most appropriate? ▪ a. Observe for extrapyramidal symptoms. ▪ b. Begin a therapeutic relationship. ▪ c. Cancel any no-suicide contracts. ▪ d. Continue suicide precautions As antidepressants begin to take effect and the client feels better, she may have the energy to initiate and complete another suicide attempt. As the client's energy level increases, the nurse must continue to be vigilant to the risk of suicide. Extrapyramidal symptoms may occur with antipsychotics and aren't adverse effects of antidepressants. A therapeutic relationship should be initiated upon admission to the psychiatric unit, after suicide precautions have been instituted. It's through this relationship that the client develops feelings of self-worth and trust and problem-solving takes place. In a no-suicide contract, the client states verbally or in writing that she won't attempt suicide and will seek out staff if she has suicidal thoughts. When the time period for a contract has expired, a new contract should be obtained from the client. 8. Which of the following statements should be included when teaching a male client about monoamine oxidase inhibitor (MAOI) antidepressants? ▪ a. Don't take prescribed or over-the-counter medications without consulting the physician. ▪ b. Avoid strenuous activity because of the cardiac effects of the drug. ▪ c. Have blood levels screened weekly for leukopenia. ▪ d. Don't take with aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs). MAOI antidepressants when combined with a number of drugs can cause life-threatening hypertensive crisis. It's imperative that a client checks with his physician and pharmacist before taking any other medications. Activity doesn't need to be limited. Blood dyscrasias aren't a common problem with MAOIs. Aspirin and NSAIDs are safe to take with MAOIs. 9. Michael,a teenager was driving a car that slipped off an icy road, killing two of his friends. He repeatedly tells the nurse that he should be dead instead of his friends. The client's behavior is an example of: ▪ a. survivor's guilt ▪ b. denial ▪ c. anticipatory grief ▪ d. repression Individuals who survive a traumatic experience in which others have died commonly report powerful feelings of guilt that they survived and others didn't. This guilt is referred to as survivor's guilt. In denial, a person refuses to accept that a situation or feeling exists. Anticipatory grief occurs when an individual experiences grief before a loss occurs. In repression, an individual involuntarily blocks an unpleasant experience, memory, or feeling from consciousness. 10. Angelo with a diagnosis of major depression is prescribed clonazepam (Klonopin) for agitation in addition to an antidepressant. Client teaching would include which of the following statements? ▪ a. Klonopin may interact with organ meats. ▪ b. The medications shouldn't be taken together. ▪ c. Klonopin is a minor depressant and may aggravate symptoms of depression. ▪ d. The order needs to be clarified; call the physician. Klonopin is a central nervous system (CNS) depressant and can aggravate symptoms in depressed clients. It doesn't interact with organ meats and can be taken with antidepressant medication. There is no need to call the physician; the medications can be safely taken together. 11. A male client is about to be discharged with a prescription for the antipsychotic agent haloperidol (Haldol), 10 mg by mouth twice per day. During a discharge teaching session, nurse Ericka should provide which instruction to the client? ▪ a. Take the medication 1 hour before a meal. ▪ b. Decrease the dosage if signs of illness decrease. ▪ c. Apply a sunscreen before being exposed to the sun. ▪ d. Increase the dosage up to 50 mg twice per day if signs of illness don't decrease. Because haloperidol can cause photosensitivity and precipitate severe sunburn, the nurse should instruct the client to apply a sunscreen before exposure to the sun. The nurse also should teach the client to take haloperidol with meals — not 1 hour before — and should instruct the client not to decrease or increase the dosage unless the physician orders it. 12. For several years, a client with chronic schizophrenia has received 10 mg of fluphenazine hydrochloride (Prolixin) by mouth four times per day. Now the client has a temperature of 102° F (38.9° C), a heart rate of 120 beats/minute, a respiratory rate of 20 breaths/minute, and a blood pressure of 210/140 mm Hg. Because the client also is confused and incontinent, nurse Ronie suspects malignant neuroleptic syndrome. What steps should the nurse take? ▪ a. Give the next dose of fluphenazine, call the physician, and monitor vital signs. ▪ b. Withhold the next dose of fluphenazine, call the physician, and monitor vital signs. ▪ c. Give the next dose of fluphenazine and restrict the client to the room to decrease stimulation. ▪ d. Withhold the next dose of fluphenazine, administer an antipyretic agent, and increase the client's fluid intake. Malignant neuroleptic syndrome is a dangerous adverse effect of neuroleptic drugs such as fluphenazine. The nurse should withhold the next dose, notify the physician, and continue to monitor vital signs. Although an antipyretic agent may be used to reduce fever, increased fluid intake is contraindicated because it may increase the client's fluid volume further, raising blood pressure even higher. 13. During a group therapy session in the psychiatric unit, Joyce constantly interrupts with impulsive behavior and exaggerated stories that cast her as a hero or princess. She also manipulates the group with attention-seeking behaviors, such as sexual comments and angry outbursts. Nurse Joey realizes that these behaviors are typical of: ▪ a. paranoid personality disorder ▪ b. avoidant personality disorder ▪ c. histrionic personality disorder ▪ d. borderline personality disorder This client's behaviors are typical of histrionic personality disorder, which is marked by excessive emotionality and attention seeking. The client constantly seeks and demands attention, approval, or praise; may be seductive in behavior, appearance, or conversation; and is uncomfortable except when she is the center of attention. Typically, a client with paranoid personality disorder is suspicious, cold, hostile, and argumentative. Avoidant personality disorder is characterized by anxiety, fear, and social isolation. Borderline personality disorder is characterized by impulsive, unpredictable behavior and unstable, intense interpersonal relationships. 14. Nurse Jason is teaching a psychiatric client about her prescribed drugs, chlorpromazine and benztropine. Why is benztropine administered? ▪ a. To reduce psychotic symptoms ▪ b. To reduce extrapyramidal symptoms ▪ c. To control nausea and vomiting ▪ d. To relieve anxiety Benztropine is an anticholinergic medication, administered to reduce the extrapyramidal adverse effects of chlorpromazine and other antipsychotic medications. Benztropine doesn't reduce psychotic symptoms, relieve anxiety, or control nausea and vomiting. 15. Dr. Ryan would probably be ordered medication for the acutely aggressive schizophrenic client? ▪ a. chlorpromazine (Thorazine) ▪ b. haloperidol (Haldol) ▪ c. lithium carbonate (Lithonate) ▪ d. amitriptyline (Elavil) Haloperidol administered I.M. or I.V. is the drug of choice for acute aggressive psychotic behavior. Chlorpromazine is also an antipsychotic drug; however, it causes more pronounced sedation than haloperidol. Lithium carbonate is useful in bipolar or manic disorder, and amitriptyline is used for depression. 16. Joe is admitted to a psychiatric facility with a diagnosis of chronic schizophrenia. The history indicates that the client has been taking neuroleptic medication for many years. Assessment reveals unusual movements of the tongue, neck, and arms. Which condition should the nurse suspect? ▪ a. Tardive dyskinesia ▪ b. Dystonia ▪ c. Neuroleptic malignant syndrome ▪ d. Akathisia Unusual movements of the tongue, neck, and arms suggest tardive dyskinesia, an adverse reaction to neuroleptic medication. Dystonia is characterized by cramps and rigidity of the tongue, face, neck, and back muscles. Neuroleptic malignant syndrome causes rigidity, fever, hypertension, and diaphoresis. Akathisia causes restlessness, anxiety, and jitteriness. 17. Bryan, with a 5-year history of multiple psychiatric admissions is brought to the emergency department by the police. He was found wandering the streets disheveled, shoeless, and confused. Based on his previous medical records and current behavior, he is diagnosed with chronic undifferentiated schizophrenia. Nurse Tryzz should assign highest priority to which nursing diagnosis? ▪ a. Anxiety ▪ b. Impaired verbal communication ▪ c. Disturbed thought processes ▪ d. Self-care deficient: Dressing/grooming For this client, the highest-priority nursing diagnosis is Anxiety (severe to panic-level), manifested by the client's extreme withdrawal and attempt to protect himself from the environment. The nurse must act immediately to reduce anxiety and protect the client and others from possible injury. Impaired verbal communication, manifested by noncommunicativeness; Disturbed thought processes, evidenced by inability to understand the situation; and Self- care deficient: Dressing/grooming, evidenced by a disheveled appearance, are appropriate nursing diagnoses but aren't the highest priority. 18. Nurse Jeremiah formulates a nursing diagnosis of Impaired verbal communication for a client with schizotypal personality disorder. Based on this nursing diagnosis, which nursing intervention is most appropriate? ▪ a. Helping the client to participate in social interactions ▪ b. Establishing a one-on-one relationship with the client ▪ c. Establishing alternative forms of communication ▪ d. Allowing the client to decide when he wants to participate in verbal communication with the nurse By establishing a one-on-one relationship, the nurse helps the client learn how to interact with people in new situations. The other options are appropriate but should take place only after the nurse-client relationship is established. 19. Kris with schizophrenia is receiving antipsychotic medication. Which nursing diagnosis may be appropriate for this client? ▪ a. Ineffective protection related to blood dyscrasias ▪ b. Urinary frequency related to adverse effects of antipsychotic medication ▪ c. Risk for injury related to a severely decreased level of consciousness ▪ d. Risk for injury related to electrolyte disturbances Antipsychotic medications may cause neutropenia and granulocytopenia, life-threatening blood dyscrasias, that warrant a nursing diagnosis of Ineffective protection related to blood dyscrasias. These medications also have anticholinergic effects, such as urine retention, dry mouth, and constipation. Urinary frequency isn't an approved nursing diagnosis. Although antipsychotic medications may cause sedation, they don't severely decrease the level of consciousness, eliminating option C. These drugs don't cause electrolyte disturbances, eliminating option D. 20. Nurse Lea is providing care to a client with a catatonic type of schizophrenia who exhibits extreme negativism. To help the client meet his basic needs, the nurse should: ▪ a. ask the client which activity he would prefer to do first ▪ b. negotiate a time when the client will perform activities ▪ c. tell the client specifically and concisely what needs to be done ▪ d. prepare the client ahead of time for the activity The client needs to be informed of the activity and when it will be done. Giving the client choices isn't desirable because he can be manipulative or refuse to do anything. Negotiating and preparing the client ahead of time also isn't therapeutic with this type of client because he may not want to perform the activity. 21. Judah receiving haloperidol (Haldol) complains of a stiff jaw and difficulty swallowing. The nurse's first action is to: ▪ a. reassure the client and administer as needed lorazepam (Ativan) I.M. ▪ b. administer as needed dose of benztropine (Cogentin) I.M. as ordered. ▪ c. administer as needed dose of benztropine (Cogentin) by mouth as ordered. ▪ d. administer as needed dose of haloperidol (Haldol) by mouth. The client is most likely suffering from muscle rigidity due to haloperidol. I.M. benztropine should be administered to prevent asphyxia or aspiration. Lorazepam treats anxiety, not extrapyramidal effects. Another dose of haloperidol would increase the severity of the reaction. 22. Nurse Irma is aware that the most antipsychotic medications exert which of following effects on the central nervous system (CNS)? ▪ a. Stimulate the CNS by blocking postsynaptic dopamine, norepinephrine, and serotonin receptors. ▪ b. Sedate the CNS by stimulating serotonin at the synaptic cleft. ▪ c. Depress the CNS by blocking the postsynaptic transmission of dopamine, serotonin, and norepinephrine. ▪ d. Depress the CNS by stimulating the release of acetylcholine. The exact mechanism of antipsychotic medication action is unknown, but appear to depress the CNS by blocking the transmission of three neurotransmitters: dopamine, serotonin, and norepinephrine. They don't sedate the CNS by stimulating serotonin, and they don't stimulate neurotransmitter action or acetylcholine release. 23. Teresa with catatonic schizophrenia is mute, can't perform activities of daily living, and stares out the window for hours. What is the nurse's first priority? ▪ a. Assist the client with feeding. ▪ b. Assist the client with showering. ▪ c. Reassure the client about safety. ▪ d. Encourage socialization with peers. According to Maslow's hierarchy of needs, the need for food is among the most important. Other needs, in order of decreasing importance, include hygiene, safety, and a sense of belonging. 24. Aiza with paranoid schizophrenia has been experiencing auditory hallucinations for many years. One approach that has proven to be effective for hallucinating clients is to: ▪ a. take an as-needed dose of psychotropic medication whenever they hear voices. ▪ b. practice saying "Go away" or "Stop" when they hear voices. ▪ c. sing loudly to drown out the voices and provide a distraction. ▪ d. go to their room until the voices go away Researchers have found that some clients can learn to control bothersome hallucinations by telling the voices to go away or stop. Taking an as needed dose of psychotropic medication whenever the voices arise may lead to overmedication and put the client at risk for adverse effects. Because the voices aren't likely to go away permanently, the client must learn to deal with the hallucinations without relying on drugs. Although distraction is helpful, singing loudly may upset other clients and would be socially unacceptable after the client is discharged. Hallucinations are most bothersome in a quiet environment when the client is alone, so sending the client to his room would increase, rather than decrease, the hallucinations. 25. Nurse isabel is assigned to a client with catatonic schizophrenia. Which intervention should the nurse include in the client's plan of care? ▪ a. Meeting all of the client's physical needs ▪ b. Giving the client an opportunity to express concerns ▪ c. Administering lithium carbonate (Lithonate) as prescribed ▪ d. Providing a quiet environment where the client can be alone Because a client with catatonic schizophrenia can't meet physical needs independently, the nurse must provide for all of these needs, including adequate food and fluid intake, exercise, and elimination. This client is incapable of expressing concerns; however, the nurse should try to verbalize the message conveyed by the client's nonverbal behavior. Lithium is used to treat mania, not catatonic schizophrenia. Despite the client's mute, unresponsive state, the nurse should provide nonthreatening stimulation and should spend time with the client, not leave the client alone all the time. Although aware of the environment, the client doesn't interact with it actively; the nurse's support and presence can be reassuring. Nursing Board Review: Psychiatric Nursing Practice Test Part 1 All the questions in the quiz along with their answers are shown below. Your answers are bolded. The correct answers have a green background while the incorrect ones have a red background. 1. Before eating a meal, a female client with obsessive-compulsive disorder (OCD) must wash his hands for 18 minutes, comb his hair 444 strokes, and switch thebathroom lights 44 times. What is the most appropriate goal of care for this client? ▪ a. Omit one unacceptable behavior each day ▪ b. Increase the client’s acceptance of therapeutic drug use ▪ c. Allow ample time for the client to complete all rituals before each meal ▪ d. Systematically decrease the number of repetitions of rituals and the amount of time spent performing them. When caring for a client with OCD, the goal is to systematically decrease the undesirable behavior. (Therapy may not completely extinguish certain behaviors.) Expecting to omit one behavior each day is unrealistic because the client may have used ritualistic behavior would perpetuate the undesirable behavior. 2. The nurse closely observes the client who has been displaying aggressive behavior. The nurse observes that the client’s anger is escalating. Which approach is least helpful for the client at this time? ▪ a. Acknowledge the client’s behavior ▪ b. Maintain a safe distance from the client ▪ c. Assist the client to an area that is quiet ▪ d. Initiate confinement measures The proper procedure for dealing with harmful behavior is to first try to calm patient verbally. When verbal and psychopharmacologic interventions are not adequate to handle the aggressiveness, seclusion or restraints may be applicable. Options A, B and C are appropriate approaches during the escalation phase of aggression. 3. Clients who are suspicious primarily use projection for which purpose: ▪ a. deny reality ▪ b. to deal with feelings and thoughts that are not acceptable ▪ c. to show resentment towards others ▪ d. manipulate others Projection is a defense mechanism where one attributes ones feelings and inadequacies to others to reduce anxiety. Option A, is not true in all instances of projection. Options C and D focuses on the self rather than others. 4. A 26 year old writer is admitted for the second time accompanied by his wife. He is demanding, arrogant talked fast and hyperactive. Initially the nurse should plan this for a manic client: ▪ a. set realistic limits to the client’s behavior ▪ b. repeat verbal instructions as often as needed ▪ c. allow the client to get out feelings to relieve tension ▪ d. assign a staff to be with the client at all times to help maintain control The manic client is hyperactive and may engage in injurious activities. A quiet environment and consistent and firm limits should be set to ensure safety. Option B, clear, concise directions are given because of the distractibility of the client but this is not the priority. Option C, the manic client tend to externalize hostile feelings, however only non- destructive methods of expression should be allowed. Option D, nurses set limit as needed. Assigning a staff to be with the client at all times is not realistic. 5. A client with borderline personality disorder is admitted to the psychiatric unit. Initial nursing assessment reveals that the client's wrists are scratched from a recent suicide attempt. Based on this finding, the nurse should formulate a nursing diagnosis of: ▪ a. Ineffective individual coping related to feelings of guilt. ▪ b. Situational low self-esteem related to feelings of loss of control. ▪ c. Risk for violence: Self-directed related to impulsive mutilating acts. ▪ d. Risk for violence: Directed toward others related to verbal threats. The predominant behavioral characteristic of the client with borderline personality disorder is impulsiveness, especially of a physically self-destructive sort. The observation that the client has scratched wrists doesn't substantiate the other options. 6. Which assessment finding is most consistent with early alcohol withdrawal? ▪ a. Heart rate of 120 to 140 beats/minute ▪ b. Heart rate of 50 to 60 beats/minute ▪ c. Blood pressure of 100/70 mm Hg ▪ d. Blood pressure of 140/80 mm Hg Tachycardia, a heart rate of 120 to 140 beats/minute, is a common sign of alcohol withdrawal. Blood pressure may be labile throughout withdrawal, fluctuating at different stages. Hypertensiontypically occurs in early withdrawal. Hypotension, although rare during the early withdrawal stages, may occur in later stages. Hypotension is associated with cardiovascular collapse and most commonly occurs in clients who don't receive treatment. The nurse should monitor the client's vital signs carefully throughout the entire alcohol withdrawal process. 7. A client is admitted to the psychiatric clinic for treatment of anorexia nervosa. To promote the client's physical health, the nurse should plan to: ▪ a. severely restrict the client's physical activities. ▪ b. weigh the client daily, after the evening meal. ▪ c. monitor vital signs, serum electrolyte levels, and acid-base balance. ▪ d. instruct the client to keep an accurate record of food and fluid intake An anorexic client who requires hospitalization is in poor physical condition from starvation and may die as a result of arrhythmias, hypothermia, malnutrition, infection, or cardiac abnormalities secondary to electrolyte imbalances. Therefore, monitoring the client's vital signs, serum electrolyte level, and acid base balance is crucial. Option A may worsen anxiety. Option B is incorrect because a weight obtained after breakfast is more accurate than one obtained after the evening meal. Option D would reward the client with attention for not eating and reinforce the control issues that are central to the underlying psychological problem; also, the client may record food and fluid intake inaccurately. 8. Daisy Caparas is a 35 year old woman with two young children. She had been admitted withsevere depression. During the initial phase of the nurse-patient relationship, the most helpful nursing intervention for Mrs. Caparas is: ▪ a. alleviating symptoms ▪ b. assessing anxiety ▪ c. providing sympathy ▪ d. setting limits During the initial phase of the nurse-patient relationship in this situation, tasks include establishing boundaries of the relationship, identifying problems, assessing anxiety levels, and identifying expectations. All other responses aren’t part of this phase of the relationship. 9. The best way to promote communication with Mrs. Caparas is to: ▪ a. allow her to remain isolated in her room ▪ b. ask for clarification and restate or paraphrase her statements ▪ c. place strict time limits on her efforts at communication ▪ d. tell her what you think is going on Asking for clarification and restating or paraphrasing the patient’s statements are techniques used to further elicit and clarify the patient’s feelings. The other options aren’t recommended methods for promoting communication. 10. Techniques that may help Mrs. Caparas regain self-awareness include: ▪ a. discouraging comparison with other episodes in her life ▪ b. discouraging her assessment of emotions ▪ c. encouraging her to cry as frequently as needed ▪ d. encouraging reflection Encouraging the patient to reflect enables her to think about the events and feelings and reach a conclusion. This may be help her gain confidence in making assessments and decisions, and it may encourage self-reliance. 11. The nurse is assessing a 16-year-old female who is being admitted for treatment of anorexia nervosa. Which clinical manifestation is the nurse most likely to find? ▪ a. Tachycardia ▪ b. Warm, flushed extremities ▪ c. Parotid gland tenderness ▪ d. Coarse hair growth Frequent vomiting causes tenderness and swelling of the parotid glands. The reduced metabolism that occurs with severe weight loss produces bradycardia and cold extremities. Soft, downlike hair (called lanugo) may cover the extremities, shoulders, and face of an anorexic client. 12. The nurse formulates a nursing diagnosis of “impaired verbal communication” for a male patient with schizotypal personality disorder. Based on this nursing diagnosis, which nursing intervention is most appropriate? ▪ a. Helping the patient to participate in social interactions ▪ b. Establishing a one-on-one relationship with the patient ▪ c. Establishing alternative forms of communication ▪ d. Allowing the patient to decide when he wants to participate in verbal communication with you By establishing a one-to-one relationship, the nurse helps the patient learn how to interact with other people in new situations. The other options are appropriate but should take place only after the nurse-patient relationship is established. 13. A 27-year-old woman reports losing her sight in both eyes. She’s diagnosed as having conversion disorder and is admitted to the psychiatric unit. Which nursing intervention would be most appropriate for this client? ▪ a. Not focusing on his blindness ▪ b. Providing self-care for him ▪ c. Telling him that his blindness isn’t real ▪ d. Teaching eye exercises to strengthen his eyes Focusing on the client’s blindness can positively reinforce the blindness and further promote the use of maladaptive behaviors to obtain secondary gains. The client should be encouraged to participate in his own care as much as possible to avoid fostering dependency. To promote self-esteem, give positive reinforcement for what the client can do. Blindness and other physical symptoms in a conversion disorder aren’t under the client’s control and are real to him. Eye exercises won’t resolve the client’s blindness because no organic pathology is causing the symptoms. 14. The client is arrogant and manipulative. In ensuring a therapeutic milieu, the nurse does one of the following: ▪ a. Agree on a consistent approach among the staff assigned to the client. ▪ b. Suggest that the client take a leading role in the social activities ▪ c. Provide the client with extra time for one on one sessions ▪ d. Allow the client to negotiate the plan of care Agree on a consistent approach among the staff assigned to the client. A consistent firm approach is appropriate. This is a therapeutic way of to handle attempts of exploiting the weakness in others or create conflicts among the staff. Bargaining should not be allowed. Option B, this is not therapeutic because the client tends to control and dominate others. Option C, limits are set for interaction time. Option D, allowing the client to negotiate may reinforce manipulative behavior. 15. Jade Gomez is a 33 year old housewife. She has been diagnosed with clinical depression. In a therapeutic relationship, the nurse assumes which role with Mrs. Gomez? ▪ a. Doer ▪ b. Friend ▪ c. Helper ▪ d. Listener A therapeutic relationship is a helping relationship. 16. when beginning a therapeutic relationship with Mrs. Gomez, the first phase of nurse-patient interactions is known as the: ▪ a. helping phase ▪ b. orientation phase ▪ c. talking phase ▪ d. working phase During the orientation phase of the therapeutic relationship, the nurse and patient make an agreement that they will be working together to solve one or more of the patient’s problems. 17. Which statement about patient touch is true? ▪ a. Most patients prefer not to be touched. ▪ b. Most patients prefer to be touched. ▪ c. Nurse-patient touching is an issue that requires sensitivity on the part of the nurse. ▪ d. Patients should never be touched. Touch has many meanings to patients. Although many patients are eager for human touch, others may perceive touch as human-boundary violation. Therefore, touching requires sensitivity on the part of the nurse. 18. Tourette syndrome is characterized by the presence of multiple motor and vocal tics. A vocal tic that involves repeating one's own sounds or words is known as: ▪ a. echolalia. ▪ b. palilalia. ▪ c. apraxia. ▪ d. aphonia. Palilalia is defined as the repetition of sounds and words. Echolalia is the act of repeating the words of others. Apraxia is the inability to carry out motor activities, and aphonia is the inability to speak. 19. Anxiety is caused by: ▪ a. an objective threat ▪ b. a subjectively perceived threat ▪ c. hostility turned to the self ▪ d. masked depression Anxiety is caused by a subjectively perceived threat. Option A, Fear is caused by an objective threat. Option C, a depressed client internalizes hostility. Option D, mania is due to masked depression. 20. A 29 year old client newly diagnosed with breast cancer is pacing, with rapid speech headache and inability to focus with what the doctor was saying. The nurse assesses the level of anxiety as: ▪ a. Mild ▪ b. Moderate ▪ c. Severe ▪ d. Panic The client’s manifestations indicate severe anxiety. Option A, mild anxiety is manifested by slight muscle tension, slight fidgeting, alertness, ability to concentrate and capable of problem solving. Option B, moderate muscle tension, increased vital signs, periodic slow pacing, increased rate of speech and difficulty in concentrating are noted in moderate anxiety. Option D, panic level of anxiety is characterized immobilization, incoherence, feeling of being overwhelmed and disorganization 21. Winnie Cruz is a 33 year old woman who is admitted to the hospital for observation after she attempted suicide. The nurse includes a psychosocial assessment that includes Mrs. Cruz’s marital relationship, based on the nurse’s knowledge that: ▪ a. spouses are often the first to be aware of a potential suicide ▪ b. spouses may be able to intervene in future suicide attempts ▪ c. suicide attempts may adversely affect the marital relationship ▪ d. the number one risk factor for suicide in adult woman is spousal abuse Information regarding the patient’s relationship with her spouse is important because spousal abuse is the leading cause of attempted and actual suicides in adult women. 22. Psychiatric follow-up for Mrs. Cruz is essential because she: ▪ a. is definitely depressed ▪ b. is probably angry that she’ll still alive ▪ c. may try to commit suicide again ▪ d. obviously hates her life Patients who have attempted suicide are at much higher risk for repeat attempts in the future. 23. Kevin, a 21 year old college student fell from a train and sustained a spinal cord injury, leaving him paralyzed below the waist. He’s in a spinal cord rehabilitation program and is refusing to do things for himself or practices in his prescribed program. One of Kevin’s nursing diagnosis is self-esteem disturbance. Which of the following is the most therapeutic nursing intervention? ▪ a. asking his friends to encourage self-care ▪ b. enlisting him in the planning of his own care ▪ c. moving him to a different hospital environment ▪ d. teaching him to perform self-care measures Encouraging a patient to be as independent as possible will promote self-reliance and self-confidence, both of which are components of a healthy self-esteem. An effective means of encouraging this independence is enlisting the patient in the planning of his won care. Teaching self-care measures and eliciting his peers to encourage him will be beneficial, but they are not as focused on fostering a healthy self-esteem. Moving Mr. Kevin to a different hospital environment isn’t indicated based on the data given. 24. The nurse says to Kevin, “Tell me about your plans after hospitalization.” Mr. Kevin replies, “I think in a few months I’ll pick up where I left off- back in college doing what I was doing before.” Which stage of the grief process is Mr. Kevin demonstrating? ▪ a. Acceptance ▪ b. Anger ▪ c. Bargaining ▪ d. Denial Mr. Kevin is going through the grief-loss process because he has permanently lost the use of his legs due to paralysis. His comment suggests that he’s in denial, the first stage of the process. Denial is a coping mechanism that allows the individual time to assimilate the major changes associated with body function loss. 25. Which is the drug of choice for treating Tourette syndrome? ▪ a. fluoxetine (Prozac) ▪ b. fluvoxamine (Luvox) ▪ c. haloperidol (Haldol) ▪ d. paroxetine (Paxil) Haloperidol is the drug of choice for treating Tourette syndrome. Prozac, Luvox, and Paxil are antidepressants and aren't used to treat Tourette syndrome. Nursing Board Review: Psychiatric Nursing Practice Test Part 2 All the questions in the quiz along with their answers are shown below. Your answers are bolded. The correct answers have a green background while the incorrect ones have a red background. 1. A male client with a history of medication noncompliance is receiving outpatient treatment for chronic undifferentiated schizophrenia. The physician is most likely to prescribe which medication for this client? ▪ a. Chlorpromazine (Thorazine) ▪ b. Imipramine (Tofranil) ▪ c. Lithium carbonate (Lithane) ▪ d. Fluphenazine decanoate (Prolixin Decanoate) Fluphenazine decanoate is a long-acting antipsychotic agent given by injection. Because it has a 4-week duration of action, it’s commonly prescribed for outpatients with a history of medication noncompliance. Chlorpromazine, also an antipsychotic agent, must be administered daily to maintain adequate plasma levels, which necessitates compliance with the dosage schedule. Imipramine, a tricyclic antidepressant, and lithium carbonate, a mood stabilizer, are rarely used to treat clients with chronic schizophrenia. 2. Which of the following medications would the nurse in-charge expect the doctor to order to reverse a dystonic reaction? ▪ a. Procholorperazine (Compazine) ▪ b. Diphenhydramine (Benadryl) ▪ c. Haloperidol (Haldol) ▪ d. Midazolam (Versed) Diphenhydramine, 25 to 50 mg I.M. or I.V., would quickly reverse this condition. Prochlorperazine and haloperidol are both capable of causing dystonia, not reversing it. Midazolam would make this patient drowsy. 3. A nurse places a female client in full leather restraints. How often must the nurse check the client’s circulation? ▪ a. Once per hour ▪ b. Once per shift ▪ c. Every 10 to 15 minutes ▪ d. Every 2 hours Circulation as well as skin and nerve damage can occur within 15 minutes. Checking every hour, 2 hours, or 8 hours isn’t often enough and could result in permanent damage to the client’s extremities. Restraints should be removed every 2 hours, and range-of-motion exercises should be performed. 4. The client tells the nurse he was involved in a car accident while he was intoxicated. What would be the most therapeutic response from the nurse? ▪ a. "Why didn't you get someone else to drive you?" ▪ b. "Tell me how you feel about the accident." ▪ c. "You should know better than to drink and drive." ▪ d. "I recommend that you attend an Alcoholics Anonymous meeting." An open-ended statement or question is the most therapeutic response. It encourages the widest range of client responses, makes the client an active participant in the conversation, and shows the client that the nurse is interested in his feelings. Asking the client why he drove while intoxicated can make him feel defensive and intimidated. A judgmental approach isn't therapeutic. By giving advice, the nurse suggests that the client isn't capable of making decisions, thus fostering dependency. 5. A client is being admitted to the substance abuse unit for alcohol detoxification. As part of the intake interview, the nurse asks him when he had his last alcoholic drink. He says that he had his last drink 6 hours before admission. Based on this response, the nurse should expect early withdrawal symptoms to: ▪ a. begin after 7 days. ▪ b. not occur at all because the time period for their occurrence has passed. ▪ c. begin anytime within the next 1 to 2 days. ▪ d. begin within 2 to 7 days. Acute withdrawal symptoms from alcohol may begin 6 hours after the client has stopped drinking and peak 1 to 2 days later. Delirium tremens may occur 2 to 4 days — even up to 7 days — after the last drink. 6. Which is the highest priority in the post ECT care? ▪ a. Observe for confusion ▪ b. Monitor respiratory status ▪ c. Reorient to time, place and person ▪ d. Document the client’s response to the treatment A side effect of ECT which is life threatening is respiratory arrest. Options A and C, Confusion and disorientation are side effects of ECT but these are not the highest priority. 7. Which of the following medical conditions is commonly found in clients with bulimia nervosa? ▪ a. Allergies ▪ b. Cancer ▪ c. Diabetes mellitus ▪ d. Hepatitis A Bulimia nervosa can lead to many complications, including diabetes, heart disease, and hypertension. The eating disorder isn't typically associated with allergies, cancer, or hepatitis A. 8. A client tends to be insensitive to others, engages in abusive behaviors and does not have a sense of remorse. Which personality disorder is he likely to have? ▪ a. Narcissistic ▪ b. Paranoid ▪ c. Histrionic ▪ d. Antisocial These are the characteristics of an individual with antisocial personality. A. Narcissistic personality disorder is characterized by grandiosity and a need for constant admiration from others. B. Individuals with paranoid personality demonstrate a pattern of distrust and suspiciousness and interprets others motives as threatening. C. Individuals with histrionic have excessive emotionality, and attention-seeking behaviors. 9. The client on Haldol has pill rolling tremors and muscle rigidity. He is likely manifesting: ▪ a. tardive dyskinesia ▪ b. Pseudoparkinsonism ▪ c. akinesia ▪ d. dystonia Pseudoparkinsonism is a side effect of antipsychotic drugs characterized by mask-like facies, pill rolling tremors, muscle rigidity. Option A, Tardive dyskinesia is manifested by lip smacking, wormlike movement of the tongue. Option C, Akinesia is characterized by feeling of weakness and muscle fatigue. Option D, Dystonia is manifested by torticollis and rolling back of the eyes. 10. A client has approached the nurse asking for advice on how to deal with his alcohol addiction. The nurse should tell the client that the only effective treatment for alcoholism is: ▪ a. psychotherapy. ▪ b. total abstinence. ▪ c. Alcoholics Anonymous (AA). ▪ d. aversion therapy. Total abstinence is the only effective treatment for alcoholism. Psychotherapy, attendance at AA meetings, and aversion therapy are all adjunctive therapies that can support the client in his efforts to abstain. 11. The nurse is caring for a male client with schizophrenia. Which outcome is the least desirable? ▪ a. The client spends more time by himself ▪ b. The client doesn’t engage in delusional thinking ▪ c. The client doesn’t harm himself or others ▪ d. The client demonstrates the ability to meet his own self-care needs The client with schizophrenia is commonly socially isolated and withdrawn; therefore, having the client spend more time by himself wouldn’t be a desirable outcome. Rather, a desirable outcome would specify that the client spend more time with other clients and staff on the unit. Delusions are false personal beliefs. Reducing or eliminating delusional thinking using talking therapy and antipsychotic medications would be a desirable outcome. Protecting the client and others from harm is a desirable client outcome achieved by close observation, removing any dangerous objects, and administering medications. Because the client with schizophrenia may have difficulty meeting his or her own self-care needs, fostering the ability to perform self-care independently is a desirable client outcome. 12. The client says to the nurse ” Pray for me” and entrusts her wedding ring to the nurse. The nurse knows that this may signal which of the following: ▪ a. anxiety ▪ b. suicidal ideation ▪ c. Major depression ▪ d. Hopelessness The client’s statement is a verbal cue of suicidal ideation not anxiety. While suicide is common among clients with major depression, this occurs when their depression starts to lift. Hopelessness indicates no alternatives available and may lead to suicide, the statement and non verbal cue of the client indicate suicide. 13. The nurse asks a client to roll up his sleeves so she can take his blood pressure. The client replies, “If you want I can go naked for you.” The most therapeutic response by the nurse is: ▪ a. “You’re attractive but I’m not interested.” ▪ b. “You wouldn’t be the first that I will see naked.” ▪ c. “I will report you to the guard if you don’t control yourself.” ▪ d. “I only need access to your arm. Putting up your sleeve is fine.” “I only need access to your arm. Putting up your sleeve is fine.” The nurse needs to deal with the client with sexually connotative behavior in a casual, matter of fact way. Options A and B, these responses are not therapeutic because they are challenging and rejecting. Option C, threatening the client is not therapeutic. 14. Diana Gil is a 45 year old mother of three, is a patient on a burn unit. She received full thickness burn on 20% of her body in a house fire in which two of her children died. Which behavior would most suggest to the nurse that Mrs. Gil is still in the earliest stage of the grief process? ▪ a. Outburst of anger toward her family and the staff ▪ b. Questions about job retaining ▪ c. Statements that “it’s a dream” and “it didn’t really happen” ▪ d. Wanting to be left alone in a dark and quiet room Early grief involves shock, disbelief and denial; therefore, statements such as “it’s a dream” and “it didn’t really happen” are expected reactions in that stage. Job retaining questions are more suggestive of either the acceptance phase or dysfunctional grief, in which the individual is failing to grieve. Anger is the second phase of grief. Isolation is more suggestive of the depression phase of grief. 15. Shortly after midnight, Mrs. Gil is awakened by the sound of an arriving ambulance outside the window of her room. She exhibits screaming, crying, vigorous attempts to get out of the bed, and incoherent speech. These manifestations are most suggestive of which level of anxiety? ▪ a. Mild ▪ b. Moderate ▪ c. Panic ▪ d. Severe Extreme behaviors such as Mrs. Gil distorted response to the ambulance are indicative of panic. In the lesser degree of anxiety, the patient’s typical behavior is changed, but not exaggerated level that is seen in panic. 16. During this episode, which nursing intervention is most appropriate? ▪ a. Discuss appropriate coping mechanisms with Mrs. Gil. ▪ b. Encourage Mrs. Gil to express her feelings about the event. ▪ c. Have Mrs. Gil remain in bed and apply soft wrist restrains. ▪ d. Stay with Mrs. Gil and provide assurance and safety. When a patient is experiencing panic, it’s most important for the nurse to remain with the patient to provide physical and verbal assurance as well as to protect her from further injury. During panic, teaching her to discuss her feelings is less appropriate intervention because they can agitate the patient even more. Use of restrains requires a doctors order and can cause injury to the skin and joints. 17. A 26 year old unemployed woman seeks help because she feels depressed and abandoned and doesn't know what to do with her life. She says she has quit her last five jobs because her coworkers didn't like her and didn't train her adequately. Last week, her boyfriend broke up with her after she drove his car into a tree after an argument. The client's initial diagnosis is borderline personality disorder. Which nursing observations support this diagnosis? ▪ a. Flat affect, social withdrawal, and unusual dress ▪ b. Suspiciousness, hypervigilance, and emotional coldness ▪ c. Lack of self-esteem, strong dependency needs, and impulsive behavior ▪ d. Insensitivity to others, sexual acting out, and violence Borderline personality disorder is characterized by lack of self-esteem, strong dependency needs, and impulsive behavior. Instability in interpersonal relationships, mood, and poor self-image also is common. Typically, the client can't tolerate being alone and expresses feelings of emptiness or boredom. Flat affect, social withdrawal, and unusual dress are characteristic of schizoid personality disorder. Suspiciousness, hypervigilance, and emotional coldness are seen in paranoid personality disorders. In antisocial personality disorder, clients are usually insensitive to others and act out sexually; they may also be violent 18. How soon after chlorpromazine administration should the nurse in charge expect to see a patient’s delusion thoughts and hallucinations eliminated? ▪ a. Several minutes ▪ b. Several hours ▪ c. Several days ▪ d. Several weeks Although most phenothiazine produces some effects within minutes to hours, their antipsychotic effects may take several weeks to appear. 19. Dolores Moreno, a 21 year old mother of premature newborn, smoked cigarettes during her pregnancy. Her son is a patient in NICU and has a diagnosis of acute respiratory distress syndrome. Ms. Moreno is expressing guilt about her son’s illness. Which aspect of her role should the nurse most express when addressing Ms. Moreno’s guilt? ▪ a. Empathy ▪ b. Guidance ▪ c. Role modeling ▪ d. Teaching Empathy, the understanding of another’s perception of a situation, is key to establishing a therapeutic rapport with a patient. Empathy encourages a patient’s trust and promotes the patient’s self-expression. In this situation, it’s the most important aspect of the nursing role that should be expressed. 20. While pacing in the hall, a female patient with paranoid schizophrenia runs to the nurse and says, “Why are you poisoning me? I know you work for central thought control! You can keep my thoughts. Give me back my soul!” how should the nurse respond? ▪ a. “I’m a nurse, I’m not poisoning you. It’s against the nursing code of ethics.” ▪ b. “I’m a nurse, and you’re a patient in the hospital. I’m not going to harm you.” ▪ c. “I’m not poisoning you. And how could I possibly steal your soul?” ▪ d. “I sense anger, Are you feeling angry today?” The nurse should directly orient a delusional patient to reality, especially to place and person. Options A and C encourage further delusions by denying poisoning and offering information related to the delusion. Validating the patient’s feeling, as in option D, occurs during a later stage in the therapeutic process. 21. Conditions necessary for the development of a positive sense of self-esteem include: ▪ a. Consistent limits ▪ b. Critical environment ▪ c. Inconsistent boundaries ▪ d. Physical discipline A structured lifestyle demonstrates acceptance and caring provides a sense of security. A critical environment erodes a person’s esteem. Inconsistent boundaries lead to feelings of insecurity and lack of concern. Physical discipline can decrease self-esteem. 22. During which phase of alcoholism is loss of control and physiologic dependence evident? ▪ A. Prealcoholic phase ▪ B. Early alcoholic phase ▪ C. Crucial phase ▪ D. Chronic phase The crucial phase is marked by physical dependence. The prealcoholic phase is characterized by drinking to medicate feelings and for relief from stress. The early phase is characterized by sneaking drinks, blackouts, rapidly gulping drinks, and preoccupation with alcohol. The chronic phase is characterized by emotional and physical deterioration. 23. A client tells the nurse that he is having suicidal thoughts every day. In conferring with the treatment team, the nurse should make which of the following recommendations? ▪ a. A no-suicide contract ▪ b. Weekly outpatient therapy ▪ c. A second psychiatric opinion ▪ d. Intensive inpatient treatment Inpatient care is the best intervention for a client who is thinking about suicide every day. Implementing a no-suicide contract is an important strategy, but this client requires additional care. Weekly therapy wouldn't provide the intensity of care that this case warrants. Obtaining a second opinion would take time; this client requires immediate intervention. 24. During a private conversation, a client with borderline personality disorder asks the nurse to keep his secret and then displays multiple, self-inflicted, superficial lacerations on the forearms. What is the nurse's best response? ▪ a. "That's it! You're on suicide precautions." ▪ b. "I'm going to tell your physician. Do you want to tell me why you did that?" ▪ c. "Tell me what type of instrument you used. I'm concerned about infection." ▪ d. "The team needs to know when something important occurs in treatment. I need to tell the others, but let's talk about it first." This response informs the client of the nurse's planned actions and allows time to discuss the client's actions. Options A and B put the client on the defensive and may lead to a power struggle. Option C ignores the psychological implications of the client's actions. 25. Flumazenil (Romazicon) has been ordered for a client who has overdosed on oxazepam (Serax). Before administering the medication, the nurse should be prepared for which common adverse effect? ▪ a. Seizures ▪ b. Shivering ▪ c. Anxiety ▪ d. Chest pain Seizures are the most common serious adverse effect of using flumazenil to reverse benzodiazepine overdose. The effect is magnified if the client has a combined tricyclic antidepressant and benzodiazepine overdose. Less common adverse effects include shivering, anxiety, and chest pain. Psychiatric Nursing Practice Test Part 1 1. Marco approached Nurse Trish asking for advice on how to deal with his alcohol addiction. Nurse Trish should tell the client that the only effective treatment for alcoholism is: a. Psychotherapy b. Alcoholics anonymous (A.A.) c. Total abstinence d. Aversion Therapy 2. Nurse Hazel is caring for a male client who experience false sensory perceptions with no basis in reality. This perception is known as: a. Hallucinations b. Delusions c. Loose associations d. Neologisms 3. Nurse Monet is caring for a female client who has suicidal tendency. When accompanying the client to the restroom, Nurse Monet should… a. Give her privacy b. Allow her to urinate c. Open the window and allow her to get some fresh air d. Observe her 4. Nurse Maureen is developing a plan of care for a female client with anorexia nervosa. Which action should the nurse include in the plan? a. Provide privacy during meals b. Set-up a strict eating plan for the client c. Encourage client to exercise to reduce anxiety d. Restrict visits with the family 5. A client is experiencing anxiety attack. The most appropriate nursing intervention should include? a. Turning on the television b. Leaving the client alone c. Staying with the client and speaking in short sentences d. Ask the client to play with other clients 6. A female client is admitted with a diagnosis of delusions of GRANDEUR. This diagnosis reflects a belief that one is: a. Being Killed b. Highly famous and important c. Responsible for evil world d. Connected to client unrelated to oneself 7. A 20 year old client was diagnosed with dependent personality disorder. Which behavior isnot most likely to be evidence of ineffective individual coping? a. Recurrent self-destructive behavior b. Avoiding relationship c. Showing interest in solitary activities d. Inability to make choices and decision without advise 8. A male client is diagnosed with schizotypal personality disorder. Which signs would this client exhibit during social situation? a. Paranoid thoughts b. Emotional affect c. Independence need d. Aggressive behavior 9. Nurse Claire is caring for a client diagnosed with bulimia. The most appropriate initial goal for a client diagnosed with bulimia is? a. Encourage to avoid foods b. Identify anxiety causing situations c. Eat only three meals a day d. Avoid shopping plenty of groceries 10. Nurse Tony was caring for a 41 year old female client. Which behavior by the client indicates adult cognitive development? a. Generates new levels of awareness b. Assumes responsibility for her actions c. Has maximum ability to solve problems and learn new skills d. Her perception are based on reality 11. A neuromuscular blocking agent is administered to a client before ECT therapy. The Nurse should carefully observe the client for? a. Respiratory difficulties b. Nausea and vomiting c. Dizziness d. Seizures 12. A 75 year old client is admitted to the hospital with the diagnosis of dementia of the Alzheimer’s type and depression. The symptom that is unrelated to depression would be? a. Apathetic response to the environment b. “I don’t know” answer to questions c. Shallow of labile effect d. Neglect of personal hygiene 13. Nurse Trish is working in a mental health facility; the nurse priority nursing intervention for a newly admitted client with bulimia nervosa would be to? a. Teach client to measure I & O b. Involve client in planning daily meal c. Observe client during meals d. Monitor client continuously 14. Nurse Patricia is aware that the major health complication associated with intractable anorexia nervosa would be? a. Cardiac dysrhythmias resulting to cardiac arrest b. Glucose intolerance resulting in protracted hypoglycemia c. Endocrine imbalance causing cold amenorrhea d. Decreased metabolism causing cold intolerance 15. Nurse Anna can minimize agitation in a disturbed client by? a. Increasing stimulation b. limiting unnecessary interaction c. increasing appropriate sensory perception d. ensuring constant client and staff contact 16. A 39 year old mother with obsessive-compulsive disorder has become immobilized by her elaborate hand washing and walking rituals. Nurse Trish recognizes that the basis of O.C. disorder is often: a. Problems with being too conscientious b. Problems with anger and remorse c. Feelings of guilt and inadequacy d. Feeling of unworthiness and hopelessness 17. Mario is complaining to other clients about not being allowed by staff to keep food in his room. Which of the following interventions would be most appropriate? a. Allowing a snack to be kept in his room b. Reprimanding the client c. Ignoring the clients behavior d. Setting limits on the behavior 18. Conney with borderline personality disorder who is to be discharge soon threatens to “do something” to herself if discharged. Which of the following actions by the nurse would be most important? a. Ask a family member to stay with the client at home temporarily b. Discuss the meaning of the client’s statement with her c. Request an immediate extension for the client d. Ignore the clients statement because it’s a sign of manipulation 19. Joey a client with antisocial personality disorder belches loudly. A staff member asks Joey, “Do you know why people find you repulsive?” this statement most likely would elicit which of the following client reaction? a. Depensiveness b. Embarrassment c. Shame d. Remorsefulness 20. Which of the following approaches would be most appropriate to use with a client suffering from narcissistic personality disorder when discrepancies exist between what the client states and what actually exist? a. Rationalization b. Supportive confrontation c. Limit setting d. Consistency 21. Cely is experiencing alcohol withdrawal exhibits tremors, diaphoresis and hyperactivity. Blood pressure is 190/87 mmhg and pulse is 92 bpm. Which of the medications would the nurse expect to administer? a. Naloxone (Narcan) b. Benzlropine (Cogentin) c. Lorazepam (Ativan) d. Haloperidol (Haldol) 22. Which of the following foods would the nurse Trish eliminate from the diet of a client in alcohol withdrawal? a. Milk b. Orange Juice c. Soda d. Regular Coffee 23. Which of the following would Nurse Hazel expect to assess for a client who is exhibiting late signs of heroin withdrawal? a. Yawning & diaphoresis b. Restlessness & Irritability c. Constipation & steatorrhea d. Vomiting and Diarrhea 24. To establish open and trusting relationship with a female client who has been hospitalized with severe anxiety, the nurse in charge should? a. Encourage the staff to have frequent interaction with the client b. Share an activity with the client c. Give client feedback about behavior d. Respect client’s need for personal space 25. Nurse Monette recognizes that the focus of environmental (MILIEU) therapy is to: a. Manipulate the environment to bring about positive changes in behavior b. Allow the client’s freedom to determine whether or not they will be involved in activities c. Role play life events to meet individual needs d. Use natural remedies rather than drugs to control behavior 26. Nurse Trish would expect a child with a diagnosis of reactive attachment disorder to: a. Have more positive relation with the father than the mother b. Cling to mother & cry on separation c. Be able to develop only superficial relation with the others d. Have been physically abuse 27. When teaching parents about childhood depression Nurse Trina should say? a. It may appear acting out behavior b. Does not respond to conventional treatment c. Is short in duration & resolves easily d. Looks almost identical to adult depression 28. Nurse Perry is aware that language development in autistic child resembles: a. Scanning speech b. Speech lag c. Shuttering d. Echolalia 29. A 60 year old female client who lives alone tells the nurse at the community health center “I really don’t need anyone to talk to”. The TV is my best friend. The nurse recognizes that the client is using the defense mechanism known as? a. Displacement b. Projection c. Sublimation d. Denial 30. When working with a male client suffering phobia about black cats, Nurse Trish should anticipate that a problem for this client would be? a. Anxiety when discussing phobia b. Anger toward the feared object c. Denying that the phobia exist d. Distortion of reality when completing daily routines 31. Linda is pacing the floor and appears extremely anxious. The duty nurse approaches in an attempt to alleviate Linda’s anxiety. The most therapeutic question by the nurse would be? a. Would you like to watch TV? b. Would you like me to talk with you? c. Are you feeling upset now? d. Ignore the client 32. Nurse Penny is aware that the symptoms that distinguish post traumatic stress disorder from other anxiety disorder would be: a. Avoidance of situation & certain activities that resemble the stress b. Depression and a blunted affect when discussing the traumatic situation c. Lack of interest in family & others d. Re-experiencing the trauma in dreams or flashback 33. Nurse Benjie is communicating with a male client with substance-induced persisting dementia; the client cannot remember facts and fills in the gaps with imaginary information. Nurse Benjie is aware that this is typical of? a. Flight of ideas b. Associative looseness c. Confabulation d. Concretism 34. Nurse Joey is aware that the signs & symptoms that would be most specific for diagnosis anorexia are? a. Excessive weight loss, amenorrhea & abdominal distension b. Slow pulse, 10% weight loss & alopecia c. Compulsive behavior, excessive fears & nausea d. Excessive activity, memory lapses & an increased pulse 35. A characteristic that would suggest to Nurse Anne that an adolescent may have bulimia would be: a. Frequent regurgitation & re-swallowing of food b. Previous history of gastritis c. Badly stained teeth d. Positive body image 36. Nurse Monette is aware that extremely depressed clients seem to do best in settings where they have: a. Multiple stimuli b. Routine Activities c. Minimal decision making d. Varied Activities 37. To further assess a client’s suicidal potential. Nurse Katrina should be especially alert to the client expression of: a. Frustration & fear of death b. Anger & resentment c. Anxiety & loneliness d. Helplessness & hopelessness 38. A nursing care plan for a male client with bipolar I disorder should include: a. Providing a structured environment b. Designing activities that will require the client to maintain contact with reality c. Engaging the client in conversing about current affairs d. Touching the client provide assurance 39. When planning care for a female client using ritualistic behavior, Nurse Gina must recognize that the ritual: a. Helps the client focus on the inability to deal with reality b. Helps the client control the anxiety c. Is under the client’s conscious control d. Is used by the client primarily for secondary gains 40. A 32 year old male graduate student, who has become increasingly withdrawn and neglectful of his work and personal hygiene, is brought to the psychiatric hospital by his parents. After detailed assessment, a diagnosis of schizophrenia is made. It is unlikely that the client will demonstrate: a. Low self esteem b. Concrete thinking c. Effective self boundaries d. Weak ego 41. A 23 year old client has been admitted with a diagnosis of schizophrenia says to the nurse “Yes, its march, March is little woman”. That’s literal you know”. These statement illustrate: a. Neologisms b. Echolalia c. Flight of ideas d. Loosening of association 42. A long term goal for a paranoid male client who has unjustifiably accused his wife of having many extramarital affairs would be to help the client develop: a. Insight into his behavior b. Better self control c. Feeling of self worth d. Faith in his wife 43. A male client who is experiencing disordered thinking about food being poisoned is admitted to the mental health unit. The nurse uses which communication technique to encourage the client to eat dinner? a. Focusing on self-disclosure of own food preference b. Using open ended question and silence c. Offering opinion about the need to eat d. Verbalizing reasons that the client may not choose to eat 44. Nurse Nina is assigned to care for a client diagnosed with Catatonic Stupor. When Nurse Nina enters the client’s room, the client is found lying on the bed with a body pulled into a fetal position. Nurse Nina should? a. Ask the client direct questions to encourage talking b. Rake the client into the dayroom to be with other clients c. Sit beside the client in silence and occasionally ask open-ended question d. Leave the client alone and continue with providing care to the other clients 45. Nurse Tina is caring for a client with delirium and states that “look at the spiders on the wall”. What should the nurse respond to the client? a. “You’re having hallucination, there are no spiders in this room at all” b. “I can see the spiders on the wall, but they are not going to hurt you” c. “Would you like me to kill the spiders” d. “I know you are frightened, but I do not see spiders on the wall” 46. Nurse Jonel is providing information to a community group about violence in the family. Which statement by a group member would indicate a need to provide additional information? a. “Abuse occurs more in low-income families” b. “Abuser Are often jealous or self-centered” c. “Abuser use fear and intimidation” d. “Abuser usually have poor self-esteem” 47. During electroconvulsive therapy (ECT) the client receives oxygen by mask via positive pressure ventilation. The nurse assisting with this procedure knows that positive pressure ventilation is necessary because? a. Anesthesia is administered during the procedure b. Decrease oxygen to the brain increases confusion and disorientation c. Grand mal seizure activity depresses respirations d. Muscle relaxations given to prevent injury during seizure activity depress respirations. 48. When planning the discharge of a client with chronic anxiety, Nurse Chris evaluates achievement of the discharge maintenance goals. Which goal would be most appropriately having been included in the plan of care requiring evaluation? a. The client eliminates all anxiety from daily situations b. The client ignores feelings of anxiety c. The client identifies anxiety producing situations d. The client maintains contact with a crisis counselor 49. Nurse Tina is caring for a client with depression who has not responded to antidepressant medication. The nurse anticipates that what treatment procedure may be prescribed? a. Neuroleptic medication b. Short term seclusion c. Psychosurgery d. Electroconvulsive therapy 50. Mario is admitted to the emergency room with drug-included anxiety related to over ingestion of prescribed antipsychotic medication. The most important piece of information the nurse in charge should obtain initially is the: a. Length of time on the med. b. Name of the ingested medication & the amount ingested c. Reason for the suicide attempt d. Name of the nearest relative & their phone number Answers and Rationale Psychiatric Nursing Practice Test Part 1 1. C. Total abstinence is the only effective treatment for alcoholism. 2. A. Hallucinations are visual, auditory, gustatory, tactile or olfactory perceptions that have no basis in reality. 3. D. The Nurse has a responsibility to observe continuously the acutely suicidal client. The Nurse should watch for clues, such as communicating suicidal thoughts, and messages; hoarding medications and talking about death. 4. B. Establishing a consistent eating plan and monitoring client’s weight are important to this disorder. 5. C. Appropriate nursing interventions for an anxiety attack include using short sentences, staying with the client, decreasing stimuli, remaining calm and medicating as needed. 6. B. Delusion of grandeur is a false belief that one is highly famous and important. 7. D. Individual with dependent personality disorder typically shows indecisivenesssubmissiveness and clinging behavior so that others will make decisions with them. 8. A. Clients with schizotypal personality disorder experience excessive social anxiety that can lead to paranoid thoughts. 9. B. Bulimia disorder generally is a maladaptive coping response to stress and underlying issues. The client should identify anxiety causing situation that stimulate the bulimic behavior and then learn new ways of coping with the anxiety. 10. A. An adult age 31 to 45 generates new level of awareness. 11. A. Neuromuscular Blocker, such as SUCCINYLCHOLINE (Anectine) produces respiratory depression because it inhibits contractions of respiratory muscles. 12. C. With depression, there is little or no emotional involvement therefore little alteration in affect. 13. D. These clients often hide food or force vomiting; therefore they must be carefully monitored. 14. A. These clients have severely depleted levels of sodium and potassium because of their starvation diet and energy expenditure, these electrolytes are necessary for cardiac functioning. 15. B. Limiting unnecessary interaction will decrease stimulation and agitation. 16. C. Ritualistic behavior seen in this disorder is aimed at controlling guilt and inadequacy by maintaining an absolute set pattern of behavior. 17. D. The nurse needs to set limits in the client’s manipulative behavior to help the client control dysfunctional behavior. A consistent approach by the staff is necessary to decrease manipulation. 18. B. Any suicidal statement must be assessed by the nurse. The nurse should discuss the client’s statement with her to determine its meaning in terms of suicide. 19. A. When the staff member ask the client if he wonders why others find him repulsive, the client is likely to feel defensive because the question is belittling. The natural tendency is to counterattack the threat to self image. 20. B. The nurse would specifically use supportive confrontation with the client to point out discrepancies between what the client states and what actually exists to increase responsibility for self. 21. C. The nurse would most likely administer benzodiazepine, such as lorazepan (ativan) to the client who is experiencing symptom: The client’s experiences symptoms of withdrawal because of the rebound phenomenon when the sedation of the CNS from alcohol begins to decrease. 22. D. Regular coffee contains caffeine which acts as psychomotor stimulants and leads to feelings of anxiety and agitation. Serving coffee top the client may add to tremors or wakefulness. 23. D. Vomiting and diarrhea are usually the late signs of heroin withdrawal, along with muscle spasm, fever, nausea, repetitive, abdominal cramps and backache. 24. D. Moving to a client’s personal space increases the feeling of threat, which increases anxiety. 25. A. Environmental (MILIEU) therapy aims at having everything in the client’s surrounding area toward helping the client. 26. C. Children who have experienced attachment difficulties with primary caregiver are not able to trust others and therefore relate superficially 27. A. Children have difficulty verbally expressing their feelings, acting out behavior, such as temper tantrums, may indicate underlying depression. 28. D. The autistic child repeat sounds or words spoken by others. 29. D. The client statement is an example of the use of denial, a defense that blocks problem by unconscious refusing to admit they exist. 30. A. Discussion of the feared object triggers an emotional response to the object. 31. B. The nurse presence may provide the client with support & feeling of control. 32. D. Experiencing the actual trauma in dreams or flashback is the major symptom that distinguishes post traumatic stress disorder from other anxiety disorder. 33. C. Confabulation or the filling in of memory gaps with imaginary facts is a defense mechanism used by people experiencing memory deficits. 34. A. These are the major signs of anorexia nervosa. Weight loss is excessive (15% of expected weight). 35. C. Dental enamel erosion occurs from repeated self-induced vomiting. 36. B. Depression usually is both emotional & physical. A simple daily routine is the best, least stressful and least anxiety producing. 37. D. The expression of these feeling may indicate that this client is unable to continue the struggle of life. 38. A. Structure tends to decrease agitation and anxiety and to increase the client’s feeling of security. 39. B. The rituals used by a client with obsessive compulsive disorder help control the anxiety level by maintaining a set pattern of action. 40. C. A person with this disorder would not have adequate self-boundaries. 41. D. Loose associations are thoughts that are presented without the logical connections usually necessary for the listening to interpret the message. 42. C. Helping the client to develop feeling of self worth would reduce the client’s need to use pathologic defenses. 43. B. Open ended questions and silence are strategies used to encourage clients to discuss their problem in descriptive manner. 44. C. Clients who are withdrawn may be immobile and mute, and require consistent, repeated interventions. Communication with withdrawn clients requires much patience from the nurse. The nurse facilitates communication with the client by sitting in silence, asking open-ended question and pausing to provide opportunities for the client to respond. 45. D. When hallucination is present, the nurse should reinforce reality with the client. 46. A. Personal characteristics of abuser include low self-esteem, immaturity, dependence, insecurity and jealousy. 47. D. A short acting skeletal muscle relaxant such as succinylcholine (Anectine) is administered during this procedure to prevent injuries during seizure. 48. C. Recognizing situations that produce anxiety allows the client to prepare to cope with anxiety or avoid specific stimulus. 49. D. Electroconvulsive therapy is an effective treatment for depression that has not responded to medication. 50. B. In an emergency, lives saving facts are obtained first. The name and the amount of medication ingested are of outmost important in treating this potentially life threatening situation. Psychiatric Nursing Practice Test Part 2 1. Nurse Tony should first discuss terminating the nurse-client relationship with a client during the: a. Termination phase when discharge plans are being made. b. Working phase when the client shows some progress. c. Orientation phase when a contract is established. d. Working phase when the client brings it up. 2. Malou is diagnosed with major depression spends majority of the day lying in bed with thesheet pulled over his head. Which of the following approaches by the nurse would be the most therapeutic? a. Question the client until he responds b. Initiate contact with the client frequently c. Sit outside the clients room d. Wait for the client to begin the conversation 3. Joe who is very depressed exhibits psychomotor retardation, a flat affect and apathy. The nurse in charge observes Joe to be in need of grooming and hygiene. Which of the following nursing actions would be most appropriate? a. Waiting until the client’s family can participate in the client’s care b. Asking the client if he is ready to take shower c. Explaining the importance of hygiene to the client d. Stating to the client that it’s time for him to take a shower 4. When teaching Mario with a typical depression about foods to avoid while taking phenelzine(Nardil), which of the following would the nurse in charge include? a. Roasted chicken b. Fresh fish c. Salami d. Hamburger 5. When assessing a female client who is receiving tricyclic antidepressant therapy, which of the following would alert the nurse to the possibility that the client is experiencing anticholinergic effects? a. Urine retention and blurred vision b. Respiratory depression and convulsion c. Delirium and Sedation d. Tremors and cardiac arrhythmias 6. For a male client with dysthymic disorder, which of the following approaches would the nurse expect to implement? a. ECT b. Psychotherapeutic approach c. Psychoanalysis d. Antidepressant therapy 7. Danny who is diagnosed with bipolar disorder and acute mania, states the nurse, “Where is my daughter? I love Louis. Rain, rain go away. Dogs eat dirt.” The nurse interprets these statements as indicating which of the following? a. Echolalia b. Neologism c. Clang associations d. Flight of ideas 8. Terry with mania is skipping up and down the hallway practically running into other clients.Which of the following activities would the nurse in charge expect to include in Terry’s plan of care? a. Watching TV b. Cleaning dayroom tables c. Leading group activity d. Reading a book 9. When assessing a male client for suicidal risk, which of the following methods of suicide would the nurse identify as most lethal? a. Wrist cutting b. Head banging c. Use of gun d. Aspirin overdose 10. Jun has been hospitalized for major depression and suicidal ideation. Which of the following statements indicates to the nurse that the client is improving? a. “I’m of no use to anyone anymore.” b. “I know my kids don’t need me anymore since they’re grown.” c. “I couldn’t kill myself because I don’t want to go to hell.” d. “I don’t think about killing myself as much as I used to.” 11. Which of the following activities would Nurse Trish recommend to the client who becomes very anxious when thoughts of suicide occur? a. Using exercise bicycle b. Meditating c. Watching TV d. Reading comics 12. When developing the plan of care for a client receiving haloperidol, which of the following medications would nurse Monet anticipate administering if the client developed extra pyramidal side effects? a. Olanzapine (Zyprexa) b. Paroxetine (Paxil) c. Benztropine mesylate (Cogentin) d. Lorazepam (Ativan) 13. Jon a suspicious client states that “I know you nurses are spraying my food with poison as you take it out of the cart.” Which of the following would be the best response of the nurse? a. Giving the client canned supplements until the delusion subsides b. Asking what kind of poison the client suspects is being used c. Serving foods that come in sealed packages d. Allowing the client to be the first to open the cart and get a tray 14. A client is suffering from catatonic behaviors. Which of the following would the nurse use to determine that the medication administered PRN have been most effective? a. The client responds to verbal directions to eat b. The client initiates simple activities without direction c. The client walks with the nurse to her room d. The client is able to move all extremities occasionally 15. Nurse Hazel invites new client’s parents to attend the psycho educational program for families of the chronically mentally ill. The program would be most likely to help the family with which of the following issues? a. Developing a support network with other families b. Feeling more guilty about the client’s illness c. Recognizing the client’s weakness d. Managing their financial concern and problems 16. When planning care for Dory with schizotypal personality disorder, which of the following would help the client become involved with others? a. Attending an activity with the nurse b. Leading a sing a long in the afternoon c. Participating solely in group activities d. Being involved with primarily one to one activities 17. Which statement about an individual with a personality disorder is true? a. Psychotic behavior is common during acute episodes b. Prognosis for recovery is good with therapeutic intervention c. The individual typically remains in the mainstream of society, although he has problems in social and occupational roles d. The individual usually seeks treatment willingly for symptoms that are personally distressful. 18. Nurse John is talking with a client who has been diagnosed with antisocial personality about how to socialize during activities without being seductive. Nurse John would focus the discussion on which of the following areas? a. Discussing his relationship with his mother b. Asking him to explain reasons for his seductive behavior c. Suggesting to apologize to others for his behavior d. Explaining the negative reactions of others toward his behavior 19. Tina with a histrionic personality disorder is melodramatic and responds to others and situations in an exaggerated manner. Nurse Trish would recommend which of the following activities for Tina? a. Baking class b. Role playing c. Scrap book making d. Music group 20. Joy has entered the chemical dependency unit for treatment of alcohol dependency. Which of the following client’s possession will the nurse most likely place in a locked area? a. Toothpaste b. Shampoo c. Antiseptic wash d. Moisturizer 21. Which of the following assessment would provide the best information about the client’s physiologic response and the effectiveness of the medication prescribed specifically for alcohol withdrawal? a. Sleeping pattern b. Mental alertness c. Nutritional status d. Vital signs 22. After administering naloxone (Narcan), an opioid antagonist, Nurse Ronald should monitor the female client carefully for which of the following? a. Respiratory depression b. Epilepsy c. Kidney failure d. Cerebral edema 23. Which of the following would nurse Ronald use as the best measure to determine a client’s progress in rehabilitation? a. The way he gets along with his parents b. The number of drug-free days he has c. The kinds of friends he makes d. The amount of responsibility his job entails 24. A female client is brought by ambulance to the hospital emergency room after taking an overdose of barbiturates is comatose. Nurse Trish would be especially alert for which of the following? a. Epilepsy b. Myocardial Infarction c. Renal failure d. Respiratory failure 25. Joey who has a chronic user of cocaine reports that he feels like he has cockroaches crawling under his skin. His arms are red because of scratching. The nurse in charge interprets these findings as possibly indicating which of the following? a. Delusion b. Formication c. Flash back d. Confusion 26. Jose is diagnosed with amphetamine psychosis and was admitted in the emergency room.Nurse Ronald would most likely prepare to administer which of the following medication? a. Librium b. Valium c. Ativan d. Haldol 27. Which of the following liquids would nurse Leng administer to a female client who is intoxicated with phencyclidine (PCP) to hasten excretion of the chemical? a. Shake b. Tea c. Cranberry Juice d. Grape juice 28. When developing a plan of care for a female client with acute stress disorder who lost her sister in a car accident. Which of the following would the nurse expect to initiate? a. Facilitating progressive review of the accident and its consequences b. Postponing discussion of the accident until the client brings it up c. Telling the client to avoid details of the accident d. Helping the client to evaluate her sister’s behavior 29. The nursing assistant tells nurse Ronald that the client is not in the dining room for lunch.Nurse Ronald would direct the nursing assistant to do which of the following? a. Tell the client he’ll need to wait until supper to eat if he misses lunch b. Invite the client to lunch and accompany him to the dining room c. Inform the client that he has 10 minutes to get to the dining room for lunch d. Take the client a lunch tray and let the client eat in his room 30. The initial nursing intervention for the significant-others during shock phase of a grief reaction should be focused on: a. Presenting full reality of the loss of the individuals b. Directing the individual’s activities at this time c. Staying with the individuals involved d. Mobilizing the individual’s support system 31. Joy’s stream of consciousness is occupied exclusively with thoughts of her father’s death.Nurse Ronald should plan to help Joy through this stage of grieving, which is known as: a. Shock and disbelief b. Developing awareness c. Resolving the loss d. Restitution 32. When taking a health history from a female client who has a moderate level of cognitive impairment due to dementia, the nurse would expect to note the presence of: a. Accentuated premorbid traits b. Enhance intelligence c. Increased inhibitions d. Hyper vigilance 33. What is the priority care for a client with a dementia resulting from AIDS? a. Planning for remotivational therapy b. Arranging for long term custodial care c. Providing basic intellectual stimulation d. Assessing pain frequently 34. Jerome who has eating disorder often exhibits similar symptoms. Nurse Lhey would expect an adolescent client with anorexia to exhibit: a. Affective instability b. Dishered, unkempt physical appearance c. Depersonalization and derealization d. Repetitive motor mechanisms 35. The primary nursing diagnosis for a female client with a medical diagnosis of major depression would be: a. Situational low self-esteem related to altered role b. Powerlessness related to the loss of idealized self c. Spiritual distress related to depression d. Impaired verbal communication related to depression 36. When developing an initial nursing care plan for a male client with a Bipolar I disorder (manic episode) nurse Ron should plan to? a. Isolate his gym time b. Encourage his active participation in unit programs c. Provide foods, fluids and rest d. Encourage his participation in programs 37. Grace is exhibiting withdrawn patterns of behavior. Nurse Johnny is aware that this type of behavior eventually produces feeling of: a. Repression b. Loneliness c. Anger d. Paranoia 38. One morning a female client on the inpatient psychiatric service complains to nurse Hazel that she has been waiting for over an hour for someone to accompany her to activities. Nurse Hazel replies to the client “We’re doing the best we can. There are a lot of other people on the unit who needs attention too.” This statement shows that the nurse’s use of: a. Defensive behavior b. Reality reinforcement c. Limit-setting behavior d. Impulse control 39. A nursing diagnosis for a male client with a diagnosed multiple personality disorder is chronic low self-esteem probably related to childhood abuse. The most appropriate short term client outcome would be: a. Verbalizing the need for anxiety medications b. Recognizing each existing personality c. Engaging in object-oriented activities d. Eliminating defense mechanisms and phobia 40. A 25 year old male is admitted to a mental health facility because of inappropriate behavior.The client has been hearing voices, responding to imaginary companions and withdrawing to his room for several days at a time. Nurse Monette understands that the withdrawal is a defense against the client’s fear of: a. Phobia b. Powerlessness c. Punishment d. Rejection 41. When asking the parents about the onset of problems in young client with the diagnosis of schizophrenia, Nurse Linda would expect that they would relate the client’s difficulties began in: a. Early childhood b. Late childhood c. Adolescence d. Puberty 42. Jose who has been hospitalized with schizophrenia tells Nurse Ron, “My heart has stopped and my veins have turned to glass!” Nurse Ron is aware that this is an example of: a. Somatic delusions b. Depersonalization c. Hypochondriasis d. Echolalia 43. In recognizing common behaviors exhibited by male client who has a diagnosis of schizophrenia, nurse Josie can anticipate: a. Slumped posture, pessimistic out look and flight of ideas b. Grandiosity, arrogance and distractibility c. Withdrawal, regressed behavior and lack of social skills d. Disorientation, forgetfulness and anxiety 44. One morning, nurse Diane finds a disturbed client curled up in the fetal position in the corner of the dayroom. The most accurate initial evaluation of the behavior would be that the client is: a. Physically ill and experiencing abdominal discomfort b. Tired and probably did not sleep well last night c. Attempting to hide from the nurse d. Feeling more anxious today 45. Nurse Bea notices a female client sitting alone in the corner smiling and talking to herself.Realizing that the client is hallucinating. Nurse Bea should: a. Invite the client to help decorate the dayroom b. Leave the client alone until he stops talking c. Ask the client why he is smiling and talking d. Tell the client it is not good for him to talk to himself 46. When being admitted to a mental health facility, a young female adult tells Nurse Mylene that the voices she hears frighten her. Nurse Mylene understands that the client tends to hallucinate more vividly: a. While watching TV b. During meal time c. During group activities d. After going to bed 47. Nurse John recognizes that paranoid delusions usually are related to the defense mechanism of: a. Projection b. Identification c. Repression d. Regression 48. When planning care for a male client using paranoid ideation, nurse Jasmin should realize the importance of: a. Giving the client difficult tasks to provide stimulation b. Providing the client with activities in which success can be achieved c. Removing stress so that the client can relax d. Not placing any demands on the client 49. Nurse Gerry is aware that the defense mechanism commonly used by clients who are alcoholics is: a. Displacement b. Denial c. Projection d. Compensation 50. Within a few hours of alcohol withdrawal, nurse John should assess the male client for the presence of: a. Disorientation, paranoia, tachycardia b. Tremors, fever, profuse diaphoresis c. Irritability, heightened alertness, jerky movements d. Yawning, anxiety, convulsions Answers and Rationale Psychiatric Nursing Practice Test Part 2 1. C. When the nurse and client agree to work together, a contract should be established, the length of the relationship should be discussed in terms of its ultimate termination. 2. B. The nurse should initiate brief, frequent contacts throughout the day to let the client know that he is important to the nurse. This will positively affect the client’s self-esteem. 3. D. The client with depression is preoccupied, has decreased energy, and is unable to make decisions. The nurse presents the situation, “It’s time for a shower”, and assists the client with personal hygiene to preserve his dignity and self-esteem. 4. C. Foods high in tyramine, those that are fermented, pickled, aged, or smoked must be avoided because when they are ingested in combination with MAOIs a hypertensive crisis will occur. 5. A. Anticholinergic effects, which result from blockage of the parasympathetic (craniosacral) nervous system including urine retention, blurred vision, dry mouth & constipation. 6. B. Dysthymia is a less severe, chronic depression diagnosed when a client has had a depressed mood for more days than not over a period of at least 2 years. Client with dysthymic disorder benefit from psychotherapeutic approaches that assist the client in reversing the negative self image, negative feelings about the future. 7. D. Flight of ideas is speech pattern of rapid transition from topic to topic, often without finishing one idea. It is common in mania. 8. B. The client with mania is very active & needs to have this energy channeled in a constructive task such as cleaning or tidying the room. 9. C. A crucial factor is determining the lethality of a method is the amount of time that occurs between initiating the method & the delivery of the lethal impact of the method. 10. D. The statement “I don’t think about killing myself as much as I used to.” Indicates a lessening of suicidal ideation and improvement in the client’s condition. 11. A. Using exercise bicycle is appropriate for the client who becomes very anxious when thoughts of suicidal occur. 12. C. The drug of choice for a client experiencing extra pyramidal side effects from haloperidol (Haldol) is benztropine mesylate (cogentin) because of its anti cholinergic properties. 13. D. Allowing the client to be the first to open the cart & take a tray presents the client with the reality that the nurses are not touching the food & tray, thereby dispelling the delusion. 14. B. Although all the actions indicate improvement, the ability to initiate simple activities without directions indicates the most improvement in the catatonic behaviors. 15. A. Psychoeducational groups for families develop a support network. They provide education about the biochemical etiology of psychiatric disease to reduce, not increase family guilt. 16. C. Attending activity with the nurse assists the client to become involved with others slowly. The client with schizotypal personality disorder needs support, kindness & gentle suggestion to improve social skills & interpersonal relationship. 17. C. An individual with personality disorder usually is not hospitalized unless a coexisting Axis I psychiatric disorder is present. Generally, these individuals make marginal adjustments and remain in society, although they typically experience relationship and occupational problems related to their inflexible behaviors. Personality disorders are chronic lifelong patterns of behavior; acute episodes do not occur. Psychotic behavior is usually not common, although it can occur in either schizotypal personality disorder or borderline personality disorder. Because these disorders are enduring and evasive and the individual is inflexible, prognosis for recovery is unfavorable. Generally, the individual does not seek treatment because he does not perceive problems with his own behavior. Distress can occur based on other people’s reaction to the individual’s behavior. 18. D. The nurse would explain the negative reactions of others towards the client’s behaviors to make the clients aware of the impact of his seductive behaviors on others. 19. B. The nurse would use role-playing to teach the client appropriate responses to others and in various situations. This client dramatizes events, drawn attention to self, and is unaware of and does not deal with feelings. The nurse works to help the client clarify true feelings & learn to express them appropriately. 20. C. Antiseptic mouthwash often contains alcohol & should be kept in locked area, unless labeling clearly indicates that the product does not contain alcohol. 21. D. Monitoring of vital signs provides the best information about the client’s overall physiologic status during alcohol withdrawal & the physiologic response to the medication used. 22. A. After administering naloxone (Narcan) the nurse should monitor the client’s respiratory status carefully, because the drug is short acting & respiratory depression may recur after its effects wear off. 23. B. The best measure to determine a client’s progress in rehabilitation is the number of drug- free days he has. The longer the client is free of drugs, the better the prognosis is. 24. D. Barbiturates are CNS depressants; the nurse would be especially alert for the possibility of respiratory failure. Respiratory failure is the most likely cause of death from barbiturate over dose. 25. B. The feeling of bugs crawling under the skin is termed as formication, and is associated with cocaine use. 26. D. The nurse would prepare to administer an antipsychotic medication such as Haldol to a client experiencing amphetamine psychosis to decrease agitation & psychotic symptoms, including delusions, hallucinations & cognitive impairment. 27. C. An acid environment aids in the excretion of PCP. The nurse will definitely give the client with PCP intoxication cranberry juice to acidify the urine to a ph of 5.5 & accelerate excretion. 28. A. The nurse would facilitate progressive review of the accident and its consequence to help the client integrate feelings & memories and to begin the grieving process. 29. B. The nurse instructs the nursing assistant to invite the client to lunch & accompany him to the dinning room to decrease manipulation, secondary gain, dependency and reinforcement of negative behavior while maintaining the client’s worth. 30. C. This provides support until the individuals coping mechanisms and personal support systems can be immobilized. 31. C. Resolving a loss is a slow, painful, continuous process until a mental image of the dead person, almost devoid of negative or undesirable features emerges. 32. A. A moderate level of cognitive impairment due to dementia is characterized by increasing dependence on environment & social structure and by increasing psychologic rigidity with accentuated previous traits & behaviors. 33. C. This action maintains for as long as possible, the clients intellectual functions by providing an opportunity to use them. 34. A. Individuals with anorexia often display irritability, hospitality, and a depressed mood. 35. D. Depressed clients demonstrate decreased communication because of lack of psychic or physical energy. 36. C. The client in a manic episode of the illness often neglects basic needs, these needs are a priority to ensure adequate nutrition, fluid, and rest. 37. B. The withdrawn pattern of behavior presents the individual from reaching out to others for sharing the isolation produces feeling of loneliness. 38. A. The nurse’s response is not therapeutic because it does not recognize the client’s needs but tries to make the client feel guilty for being demanding. 39. B. The client must recognize the existence of the sub personalities so that interpretation can occur. 40. D. An aloof, detached, withdrawn posture is a means of protecting the self by withdrawing and maintaining a safe, emotional distance. 41. C. The usual age of onset of schizophrenia is adolescence or early childhood. 42. A. Somatic delusion is a fixed false belief about one’s body. 43. C. These are the classic behaviors exhibited by clients with a diagnosis of schizophrenia. 44. D. The fetal position represents regressed behavior. Regression is a way of responding to overwhelming anxiety. 45. B. This provides a stimulus that competes with and reduces hallucination. 46. D. Auditory hallucinations are most troublesome when environmental stimuli are diminished and there are few competing distractions. 47. A. Projection is a mechanism in which inner thoughts and feelings are projected onto the environment, seeming to come from outside the self rather than from within. 48. B. This will help the client develop self-esteem and reduce the use of paranoid ideation. 49. B. Denial is a method of resolving conflict or escaping unpleasant realities by ignoring their existence. 50. C. Alcohol is a central nervous system depressant. These symptoms are the body’s neurologic adaptation to the withdrawal of alcohol. Psychiatric Nursing Practice Test Part 3 1. Francis who is addicted to cocaine withdraws from the drug. Nurse Ron should expect to observe: a. Hyperactivity b. Depression c. Suspicion d. Delirium 2. Nurse John is aware that a serious effect of inhaling cocaine is? a. Deterioration of nasal septum b. Acute fluid and electrolyte imbalances c. Extra pyramidal tract symptoms d. Esophageal varices 3. A tentative diagnosis of opiate addiction, Nurse Candy should assess a recently hospitalized client for signs of opiate withdrawal. These signs would include: a. Rhinorrhea, convulsions, subnormal temperature b. Nausea, dilated pupils, constipation c. Lacrimation, vomiting, drowsiness d. Muscle aches, papillary constriction, yawning 4. A 48 year old male client is brought to the psychiatric emergency room after attempting to jump off a bridge. The client’s wife states that he lost his job several months ago and has been unable to find another job. The primary nursing intervention at this time would be to assess for: a. A past history of depression b. Current plans to commit suicide c. The presence of marital difficulties d. Feelings of excessive failure 5. Before helping a male client who has been sexually assaulted, nurse Maureen should recognize that the rapist is motivated by feelings of: a. Hostility b. Inadequacy c. Incompetence d. Passion 6. When working with children who have been sexually abused by a family member it is important for the nurse to understand that these victims usually are overwhelmed with feelings of: a. Humiliation b. Confusion c. Self blame d. Hatred 7. Joy who has just experienced her second spontaneous abortion expresses anger towards her physician, the hospital and the “rotten nursing care”. When assessing the situation, the nurse recognizes that the client may be using the coping mechanism of: a. Projection b. Displacement c. Denial d. Reaction formation 8. The most critical factor for nurse Linda to determine during crisis intervention would be the client’s: a. Available situational supports b. Willingness to restructure the personality c. Developmental theory d. Underlying unconscious conflict 9. Nurse Trish suggests a crisis intervention group to a client experiencing a developmental crisis. These groups are successful because the: a. Crisis intervention worker is a psychologist and understands behavior patterns b. Crisis group supplies a workable solution to the client’s problem c. Client is encouraged to talk about personal problems d. Client is assisted to investigate alternative approaches to solving the identified problem 10. Nurse Ronald could evaluate that the staff’s approach to setting limits for a demanding, angry client was effective if the client: a. Apologizes for disrupting the unit’s routine when something is needed b. Understands the reason why frequent calls to the staff were made c. Discuss concerns regarding the emotional condition that required hospitalizations d. No longer calls the nursing staff for assistance 11. Nurse John is aware that the therapy that has the highest success rate for people with phobias would be: a. Psychotherapy aimed at rearranging maladaptive thought process b. Psychoanalytical exploration of repressed conflicts of an earlier development phase c. Systematic desensitization using relaxation technique d. Insight therapy to determine the origin of the anxiety and fear 12. When nurse Hazel considers a client’s placement on the continuum of anxiety, a key in determining the degree of anxiety being experienced is the client’s: a. Perceptual field b. Delusional system c. Memory state d. Creativity level 13. In the diagnosis of a possible pervasive developmental autistic disorder. The nurse would find it most unusual for a 3 year old child to demonstrate: a. An interest in music b. An attachment to odd objects c. Ritualistic behavior d. Responsiveness to the parents 14. Malou with schizophrenia tells Nurse Melinda, “My intestines are rotted from worms chewing on them.” This statement indicates a: a. Jealous delusion b. Somatic delusion c. Delusion of grandeur d. Delusion of persecution 15. Andy is admitted to the psychiatric unit with a diagnosis of borderline personality disorder.Nurse Hilary should expects the assessment to reveal: a. Coldness, detachment and lack of tender feelings b. Somatic symptoms c. Inability to function as responsible parent d. Unpredictable behavior and intense interpersonal relationships 16. PROPRANOLOL (Inderal) is used in the mental health setting to manage which of the following conditions? a. Antipsychotic – induced akathisia and anxiety b. Obsessive – compulsive disorder (OCD) to reduce ritualistic behavior c. Delusions for clients suffering from schizophrenia d. The manic phase of bipolar illness as a mood stabilizer 17. Which medication can control the extra pyramidal effects associated with antipsychotic agents? a. Clorazepate (Tranxene) b. Amantadine (Symmetrel) c. Doxepin (Sinequan) d. Perphenazine (Trilafon) 18. Which of the following statements should be included when teaching clients about monoamine oxidase inhibitor (MAOI) antidepressants? a. Don’t take aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs) b. Have blood levels screened weekly for leucopenia c. Avoid strenuous activity because of the cardiac effects of the drug d. Don’t take prescribed or over the counter medications without consulting the physician 19. Kris periodically has acute panic attacks. These attacks are unpredictable and have no apparent association with a specific object or situation. During an acute panic attack, Kris may experience: a. Heightened concentration b. Decreased perceptual field c. Decreased cardiac rate d. Decreased respiratory rate 20. Initial interventions for Marco with acute anxiety include all except which of the following? a. Touching the client in an attempt to comfort him b. Approaching the client in calm, confident manner c. Encouraging the client to verbalize feelings and concerns d. Providing the client with a safe, quiet and private place 21. Nurse Jessie is assessing a client suffering from stress and anxiety. A common physiological response to stress and anxiety is: a. Uticaria b. Vertigo c. Sedation d. Diarrhea 22. When performing a physical examination on a female anxious client, nurse Nelli would expect to find which of the following effects produced by the parasympathetic system? a. Muscle tension b. Hyperactive bowel sounds c. Decreased urine output d. Constipation 23. Which of the following drugs have been known to be effective in treating obsessive-compulsive disorder (OCD)? a. Divalproex (depakote) and Lithium (lithobid) b. Chlordiazepoxide (Librium) and diazepam (valium) c. Fluvoxamine (Luvox) and clomipramine (anafranil) d. Benztropine (Cogentin) and diphenhydramine (benadryl) 24. Tony with agoraphobia has been symptom-free for 4 months. Classic signs and symptoms of phobia include: a. Severe anxiety and fear b. Withdrawal and failure to distinguish reality from fantasy c. Depression and weight loss d. Insomnia and inability to concentrate 25. Which nursing action is most appropriate when trying to diffuse a client’s impending violent behavior? a. Place the client in seclusion b. Leaving the client alone until he can talk about his feelings c. Involving the client in a quiet activity to divert attention d. Helping the client identify and express feelings of anxiety and anger 26. Rosana is in the second stage of Alzheimer’s disease who appears to be in pain. Which question by Nurse Jenny would best elicit information about the pain? a. “Where is your pain located?” b. “Do you hurt? (pause) “Do you hurt?” c. “Can you describe your pain?” d. “Where do you hurt?” 27. Nursing preparation for a client undergoing electroconvulsive therapy (ECT) resemble those used for: a. General anesthesia b. Cardiac stress testing c. Neurologic examination d. Physical therapy 28. Jose who is receiving monoamine oxidase inhibitor antidepressant should avoid tyramine, a compound found in which of the following foods? a. Figs and cream cheese b. Fruits and yellow vegetables c. Aged cheese and Chianti wine d. Green leafy vegetables 29. Erlinda, age 85, with major depression undergoes a sixth electroconvulsive therapy (ECT) treatment. When assessing the client immediately after ECT, the nurse expects to find: a. Permanent short-term memory loss and hypertension b. Permanent long-term memory loss and hypomania c. Transitory short-term memory loss and permanent long-term memory loss d. Transitory short and long term memory loss and confusion 30. Barbara with bipolar disorder is being treated with lithium for the first time. Nurse Clint should observe the client for which common adverse effect of lithium? a. Polyuria b. Seizures c. Constipation d. Sexual dysfunction 31. Nurse Fred is assessing a client who has just been admitted to the ER department. Which signs would suggest an overdose of an antianxiety agent? a. Suspiciousness, dilated pupils and incomplete BP b. Agitation, hyperactivity and grandiose ideation c. Combativeness, sweating and confusion d. Emotional lability, euphoria and impaired memory 32. Discharge instructions for a male client receiving tricyclic antidepressants include which of the following information? a. Restrict fluids and sodium intake b. Don’t consume alcohol c. Discontinue if dry mouth and blurred vision occur d. Restrict fluid and sodium intake 33. Important teaching for women in their childbearing years who are receiving antipsychotic medications includes which of the following? a. Increased incidence of dysmenorrhea while taking the drug b. Occurrence of incomplete libido due to medication adverse effects c. Continuing previous use of contraception during periods of amenorrhea d. Instruction that amenorrhea is irreversible 34. A client refuses to remain on psychotropic medications after discharge from an inpatient psychiatric unit. Which information should the community health nurse assess first during the initial follow-up with this client? a. Income level and living arrangements b. Involvement of family and support systems c. Reason for inpatient admission d. Reason for refusal to take medications 35. The nurse understands that the therapeutic effects of typical antipsychotic medications are associated with which neurotransmitter change? a. Decreased dopamine level b. Increased acetylcholine level c. Stabilization of serotonin d. Stimulation of GABA 36. Which of the following best explains why tricyclic antidepressants are used with caution in elderly patients? a. Central Nervous System effects b. Cardiovascular system effects c. Gastrointestinal system effects d. Serotonin syndrome effects 37. A client with depressive symptoms is given prescribed medications and talks with his therapist about his belief that he is worthless and unable to cope with life. Psychiatric care in this treatment plan is based on which framework? a. Behavioral framework b. Cognitive framework c. Interpersonal framework d. Psychodynamic framework 38. A nurse who explains that a client’s psychotic behavior is unconsciously motivated understands that the client’s disordered behavior arises from which of the following? a. Abnormal thinking b. Altered neurotransmitters c. Internal needs d. Response to stimuli 39. A client with depression has been hospitalized for treatment after taking a leave of absence from work. The client’s employer expects the client to return to work following inpatient treatment. The client tells the nurse, “I’m no good. I’m a failure”. According to cognitive theory, these statements reflect: a. Learned behavior b. Punitive superego and decreased self-esteem c. Faulty thought processes that govern behavior d. Evidence of difficult relationships in the work environment 40. The nurse describes a client as anxious. Which of the following statement about anxiety is true? a. Anxiety is usually pathological b. Anxiety is directly observable c. Anxiety is usually harmful d. Anxiety is a response to a threat 41. A client with a phobic disorder is treated by systematic desensitization. The nurse understands that this approach will do which of the following? a. Help the client execute actions that are feared b. Help the client develop insight into irrational fears c. Help the client substitutes one fear for another d. Help the client decrease anxiety 42. Which client outcome would best indicate successful treatment for a client with an antisocial personality disorder? a. The client exhibits charming behavior when around authority figures b. The client has decreased episodes of impulsive behaviors c. The client makes statements of self-satisfaction d. The client’s statements indicate no remorse for behaviors 43. The nurse is caring for a client with an autoimmune disorder at a medical clinic, where alternative medicine is used as an adjunct to traditional therapies. Which information should the nurse teach the client to help foster a sense of control over his symptoms? a. Pathophysiology of disease process b. Principles of good nutrition c. Side effects of medications d. Stress management techniques 44. Which of the following is the most distinguishing feature of a client with an antisocial personality disorder? a. Attention to detail and order b. Bizarre mannerisms and thoughts c. Submissive and dependent behavior d. Disregard for social and legal norms 45. Which nursing diagnosis is most appropriate for a client with anorexia nervosa who expresses feelings of guilt about not meeting family expectations? a. Anxiety b. Disturbed body image c. Defensive coping d. Powerlessness 46. A nurse is evaluating therapy with the family of a client with anorexia nervosa. Which of the following would indicate that the therapy was successful? a. The parents reinforced increased decision making by the client b. The parents clearly verbalize their expectations for the client c. The client verbalizes that family meals are now enjoyable d. The client tells her parents about feelings of low-self esteem 47. A client with dysthymic disorder reports to a nurse that his life is hopeless and will never improve in the future. How can the nurse best respond using a cognitive approach? a. Agree with the client’s painful feelings b. Challenge the accuracy of the client’s belief c. Deny that the situation is hopeless d. Present a cheerful attitude 48. A client with major depression has not verbalized problem areas to staff or peers since admission to a psychiatric unit. Which activity should the nurse recommend to help this client express himself? a. Art therapy in a small group b. Basketball game with peers on the unit c. Reading a self-help book on depression d. Watching movie with the peer group 49. The home health psychiatric nurse visits a client with chronic schizophrenia who was recently discharged after a prolong stay in a state hospital. The client lives in a boarding home, reports no family involvement, and has little social interaction. The nurse plan to refer the client to a day treatment program in order to help him with: a. Managing his hallucinations b. Medication teaching c. Social skills training d. Vocational training 50. Which activity would be most appropriate for a severely withdrawn client? a. Art activity with a staff member b. Board game with a small group of clients c. Team sport in the gym d. Watching TV in the dayroom Answers and Rationale Psychiatric Nursing Part 3 1. B. There is no set of symptoms associated with cocaine withdrawal, only the depression that follows the high caused by the drug. 2. A. Cocaine is a chemical that when inhaled, causes destruction of the mucous membranes of the nose. 3. D. These adaptations are associated with opiate withdrawal which occurs after cessation or reduction of prolonged moderate or heavy use of opiates. 4. B. Whether there is a suicide plan is a criterion when assessing the client’s determination to make another attempt. 5. A. Rapists are believed to harbor and act out hostile feelings toward all women through the act of rape. 6. C. These children often have nonsexual needs met by individual and are powerless to refuse.Ambivalence results in self-blame and also guilt. 7. B. The client’s anger over the abortion is shifted to the staff and the hospital because she is unable to deal with the abortion at this time. 8. A. Personal internal strength and supportive individuals are critical factors that can be employed to assist the individual to cope with a crisis. 9. D. Crisis intervention group helps client reestablish psychologic equilibrium by assisting them to explore new alternatives for coping. It considers realistic situations using rational and flexible problem solving methods. 10. C. This would document that the client feels comfortable enough to discuss the problems that have motivated the behavior. 11. C. The most successful therapy for people with phobias involves behavior modificationtechniques using desensitization. 12. A. Perceptual field is a key indicator of anxiety level because the perceptual fields narrow as anxiety increases. 13. D. One of the symptoms of autistic child displays a lack of responsiveness to others. There is little or no extension to the external environment. 14. B. Somatic delusions focus on bodily functions or systems and commonly include delusion about foul odor emissions, insect manifestations, internal parasites and misshapen parts. 15. D. A client with borderline personality displays a pervasive pattern of unpredictable behavior, mood and self image. Interpersonal relationships may be intense and unstable and behavior may be inappropriate and impulsive. 16. A. Propranolol is a potent beta adrenergic blocker and producing a sedating effect, therefore it is used to treat antipsychotic induced akathisia and anxiety. 17. B. Amantadine is an anticholinergic drug used to relive drug-induced extra pyramidal adverse effects such as muscle weakness, involuntary muscle movements, pseudoparkinsonism and tar dive dyskinesia. 18. D. MAOI antidepressants when combined with a number of drugs can cause life-threatening hypertensive crisis. It’s imperative that a client checks with his physician and pharmacistbefore taking any other medications. 19. B. Panic is the most severe level of anxiety. During panic attack, the client experiences a decrease in the perceptual field, becoming more focused on self, less aware of surroundings and unable to process information from the environment. The decreased perceptual field contributes to impaired attention and inability to concentrate. 20. A. The emergency nurse must establish rapport and trust with the anxious client before using therapeutic touch. Touching an anxious client may actually increase anxiety. 21. D. Diarrhea is a common physiological response to stress and anxiety. 22. B. The parasympathetic nervous system would produce incomplete G.I. motility resulting in hyperactive bowel sounds, possibly leading to diarrhea. 23. C. The antidepressants fluvoxamine and clomipramine have been effective in the treatment of OCD. 24. A. Phobias cause severe anxiety (such as panic attack) that is out of proportion to the threat of the feared object or situation. Physical signs and symptoms of phobias include profuse sweating, poor motor control, tachycardia and elevated B.P. 25. D. In many instances, the nurse can diffuse impending violence by helping the client identify and express feelings of anger and anxiety. Such statement as “What happened to get you this angry?” may help the client verbalizes feelings rather than act on them. 26. B. When speaking to a client with Alzheimer’s disease, the nurse should use close-ended questions. Those that the client can answer with “yes” or “no” whenever possible and avoid questions that require the client to make choices. Repeating the question aids comprehension. 27. A. The nurse should prepare a client for ECT in a manner similar to that for general anesthesia. 28. C. Aged cheese and Chianti wine contain high concentrations of tyramine. 29. D. ECT commonly causes transitory short and long term memory loss and confusion, especially in geriatric clients. It rarely results in permanent short and long term memory loss. 30. A. Polyuria commonly occurs early in the treatment with lithium and could result in fluid volume deficit. 31. D. Signs of anxiety agent overdose include emotional lability, euphoria and impaired memory. 32. B. Drinking alcohol can potentiate the sedating action of tricyclic antidepressants. Dry mouth and blurred vision are normal adverse effects of tricyclic antidepressants. 33. C. Women may experience amenorrhea, which is reversible, while taking antipsychotics.Amenorrhea doesn’t indicate cessation of ovulation thus, the client can still be pregnant. 34. D. The first are for assessment would be the client’s reason for refusing medication. The client may not understand the purpose for the medication, may be experiencing distressing side effects, or may be concerned about the cost of medicine. In any case, the nurse cannot provide appropriate intervention before assessing the client’s problem with the medication. The patient’s income level, living arrangements, and involvement of family and support systems are relevant issues following determination of the client’s reason for refusing medication. The nurse providing follow-up care would have access to the client’s medical record and should already know the reason for inpatient admission. 35. A. Excess dopamine is thought to be the chemical cause for psychotic thinking. The typical antipsychotics act to block dopamine receptors and therefore decrease the amount of neurotransmitter at the synapses. The typical antipsychotics do not increase acetylcholine, stabilize serotonin, stimulate GABA. 36. B. The TCAs affect norepinephrine as well as other neurotransmitters, and thus have significant cardiovascular side effects. Therefore, they are used with caution in elderly clients who may have increased risk factors for cardiac problems because of their age and other medical conditions. The remaining side effects would apply to any client taking a TCA and are not particular to an elderly person. 37. B. Cognitive thinking therapy focuses on the client’s misperceptions about self, others and the world that impact functioning and contribute to symptoms. Using medications to alter neurotransmitter activity is a psychobiologic approach to treatment. The other answer choices are frameworks for care, but hey are not applicable to this situation. 38. C. The concept that behavior is motivated and has meaning comes from the psychodynamic framework. According to this perspective, behavior arises from internal wishes or needs. Much of what motivates behavior comes from the unconscious. The remaining responses do not address the internal forces thought to motivate behavior. 39. C. The client is demonstrating faulty thought processes that are negative and that govern his behavior in his work situation – issues that are typically examined using a cognitive theory approach. Issues involving learned behavior are best explored through behavior theory, not cognitive theory. Issues involving ego development are the focus of psychoanalytic theory. Option 4 is incorrect because there is no evidence in this situation that the client has conflictual relationships in the work environment. 40. D. Anxiety is a response to a threat arising from internal or external stimuli. 41. A. Systematic desensitization is a behavioral therapy technique that helps clients with irrational fears and avoidance behavior to face the thing they fear, without experiencing anxiety. There is no attempt to promote insight with this procedure, and the client will not be taught to substitute one fear for another. Although the client’s anxiety may decrease with successful confrontation of irrational fears, the purpose of the procedure is specifically related to performing activities that typically are avoided as part of the phobic response. 42. B. A client with antisocial personality disorder typically has frequent episodes of acting impulsively with poor ability to delay self-gratification. Therefore, decreased frequency of impulsive behaviors would be evidence of improvement. Charming behavior when around authority figures and statements indicating no remorse are examples of symptoms typical of someone with this disorder and would not indicate successful treatment. Self- satisfaction would be viewed as a positive change if the client expresses low self-esteem; however this is not a characteristic of a client with antisocial personality disorder. 43. D. In autoimmune disorders, stress and the response to stress can exacerbate symptoms. Stress management techniques can help the client reduce the psychological response to stress, which in turn will help reduce the physiologic stress response. This will afford the client an increased sense of control over his symptoms. The nurse can address the remaining answer choices in her teaching about the client’s disease and treatment; however, knowledge alone will not help the client to manage his stress effectively enough to control symptoms. 44. D. Disregard for established rules of society is the most common characteristic of a client with antisocial personality disorder. Attention to detail and order is characteristic of someone with obsessive compulsive disorder. Bizarre mannerisms and thoughts are characteristics of a client with schizoid or schizotypal disorder. Submissive and dependent behaviors are characteristic of someone with a dependent personality. 45. D. The client with anorexia typically feels powerless, with a sense of having little control over any aspect of life besides eating behavior. Often, parental expectations and standards are quite high and lead to the clients’ sense of guilt over not measuring up. 46. A. One of the core issues concerning the family of a client with anorexia is control. The family’s acceptance of the client’s ability to make independent decisions is key to successful family intervention. Although the remaining options may occur during the process of therapy, they would not necessarily indicate a successful outcome; the central family issues of dependence and independence are not addresses on these responses. 47. B. Use of cognitive techniques allows the nurse to help the client recognize that this negative beliefs may be distortions and that, by changing his thinking, he can adopt more positive beliefs that are realistic and hopeful. Agreeing with the client’s feelings and presenting a cheerful attitude are not consistent with a cognitive approach and would not be helpful in this situation. Denying the client’s feelings is belittling and may convey that the nurse does not understand the depth of the client’s distress. 48. A. Art therapy provides a nonthreatening vehicle for the expression of feelings, and use of a small group will help the client become comfortable with peers in a group setting. Basketball is a competitive game that requires energy; the client with major depression is not likely to participate in this activity. Recommending that the client read a self-help book may increase, not decrease his isolation. Watching movie with a peer group does not guarantee that interaction will occur; therefore, the client may remain isolated. 49. C. Day treatment programs provide clients with chronic, persistent mental illness training in social skills, such as meeting and greeting people, asking questions or directions, placing an order in a restaurant, taking turns in a group setting activity. Although management of hallucinations and medication teaching may also be part of the program offered in a day treatment, the nurse is referring the client in this situation because of his need for socialization skills. Vocational training generally takes place in a rehabilitation facility; the client described in this situation would not be a candidate for this service. 50. A. The best approach with a withdrawn client is to initiate brief, nondemanding activities on a one-to-one basis. This approach gives the nurse an opportunity to establish a trusting relationship with the client. A board game with a group clients or playing a team sport in the gym may overwhelm a severely withdrawn client. Watching TV is a solitary activity that will reinforce the client’s withdrawal from others. [Show More]
Last updated: 1 year ago
Preview 1 out of 65 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Aug 31, 2021
Number of pages
65
Written in

Additional information
This document has been written for:
Uploaded
Aug 31, 2021
Downloads
0
Views
36
.png)

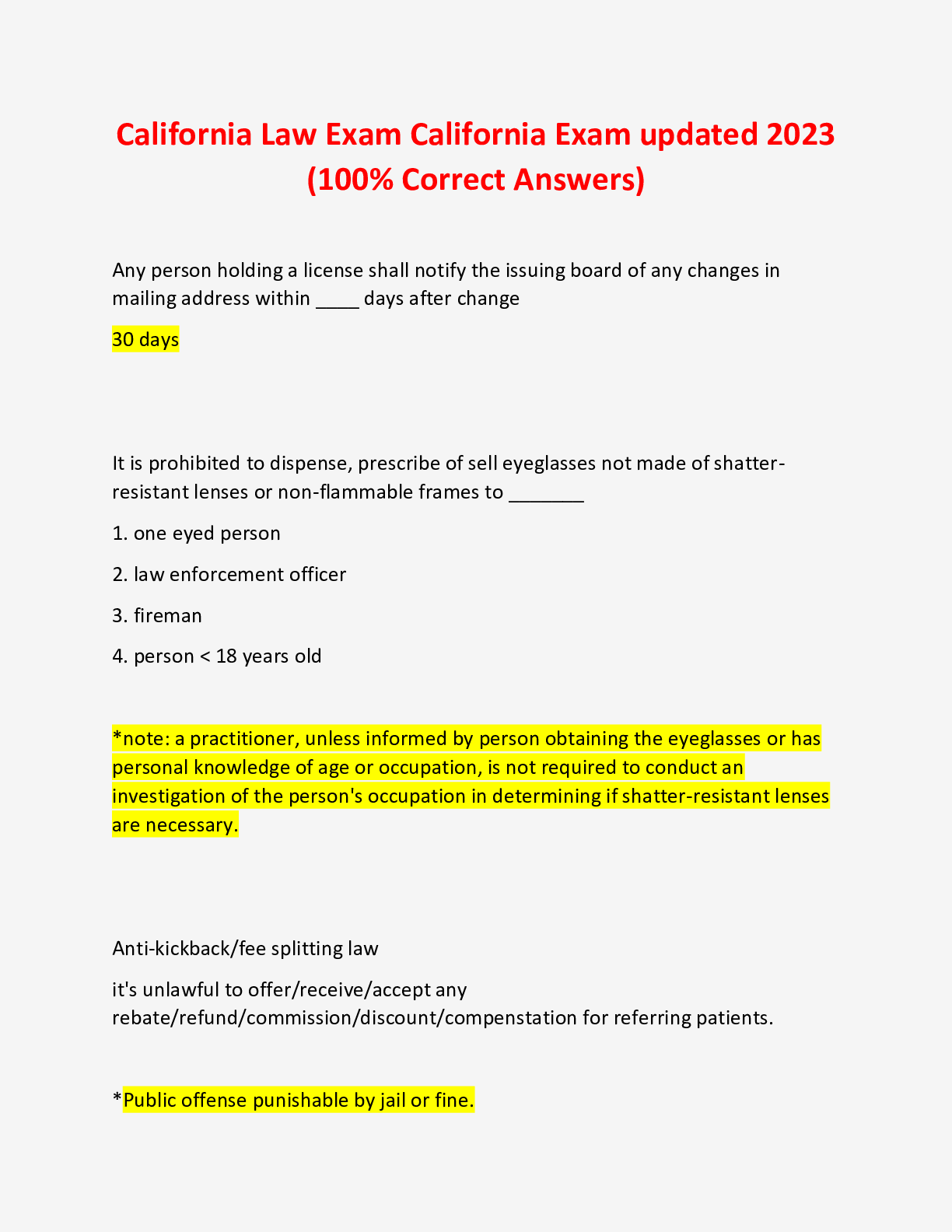
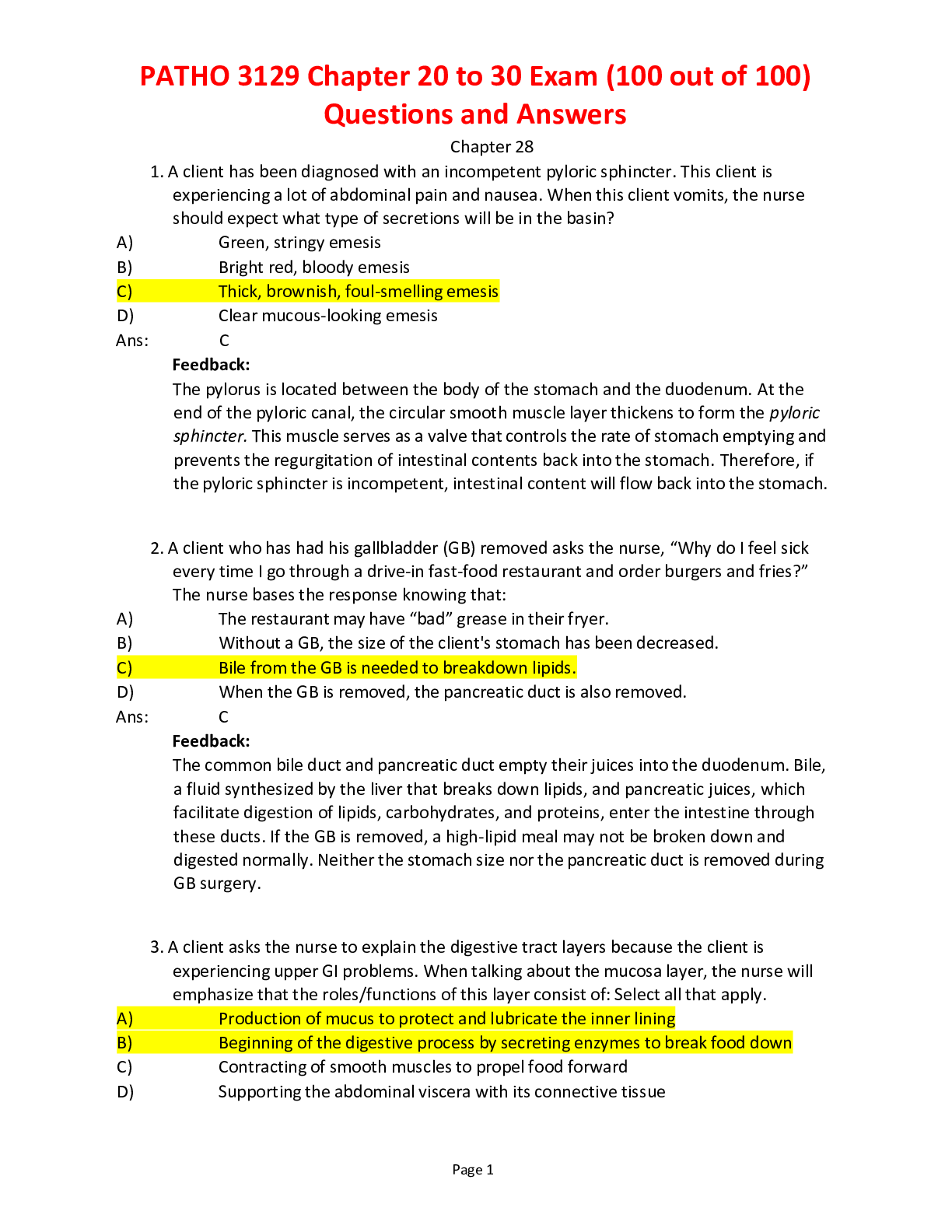
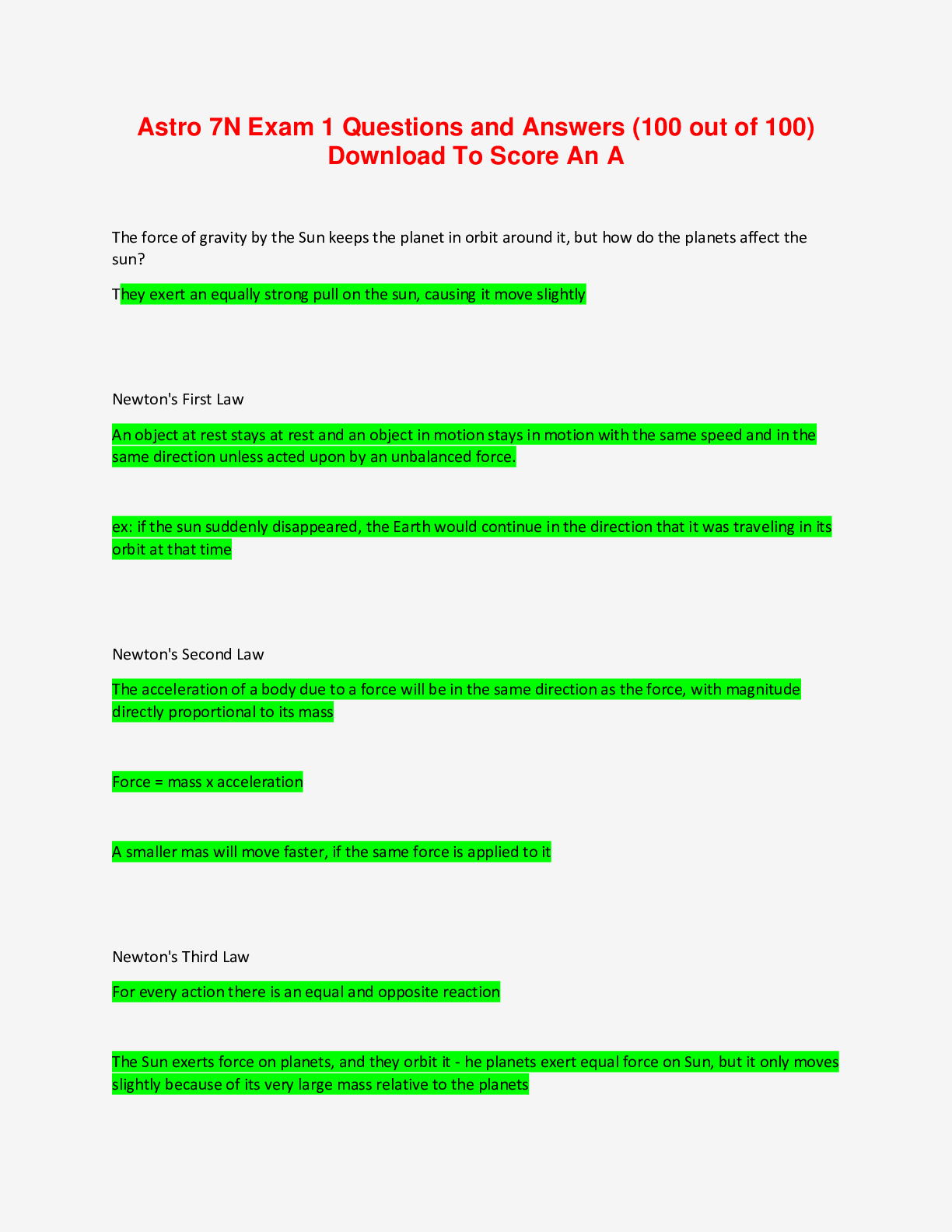
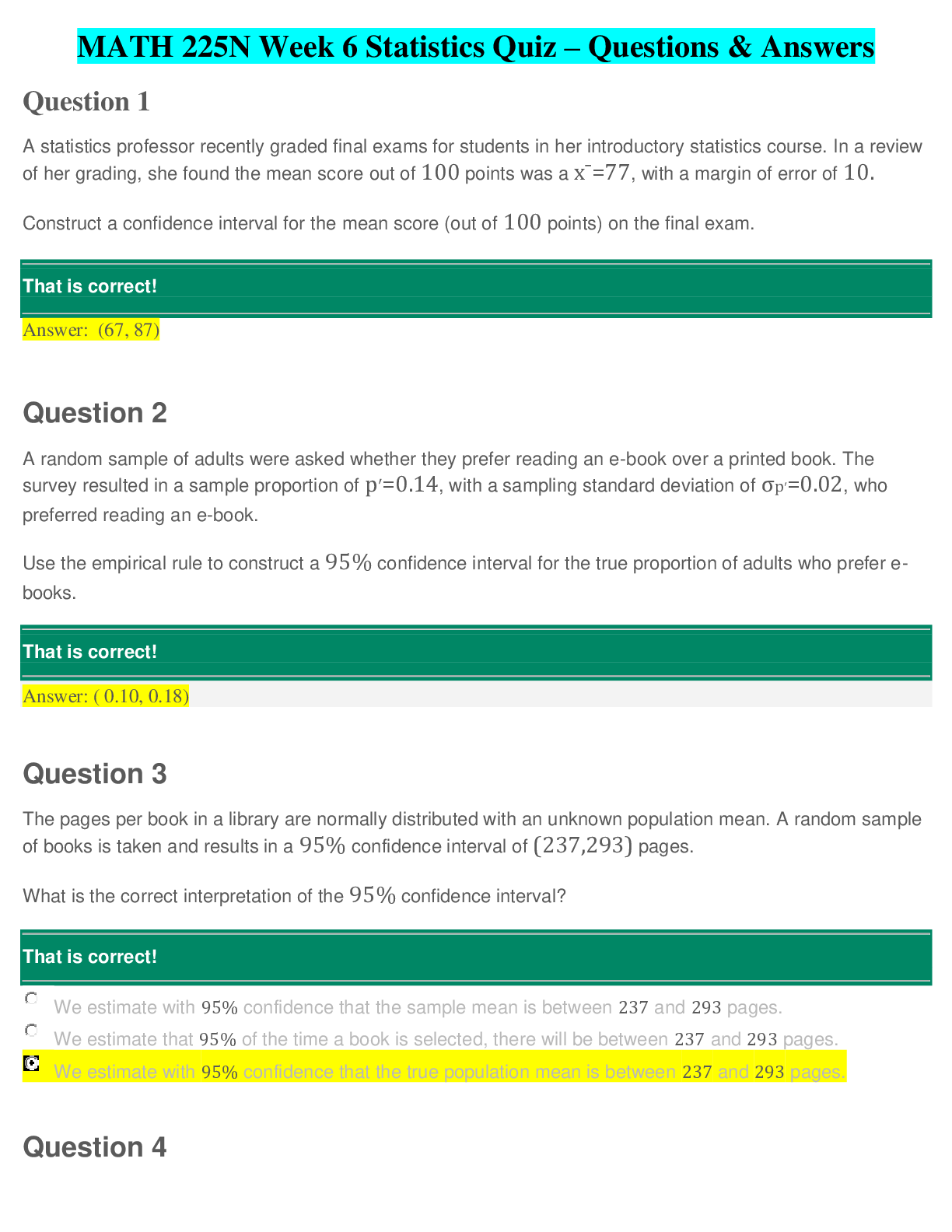
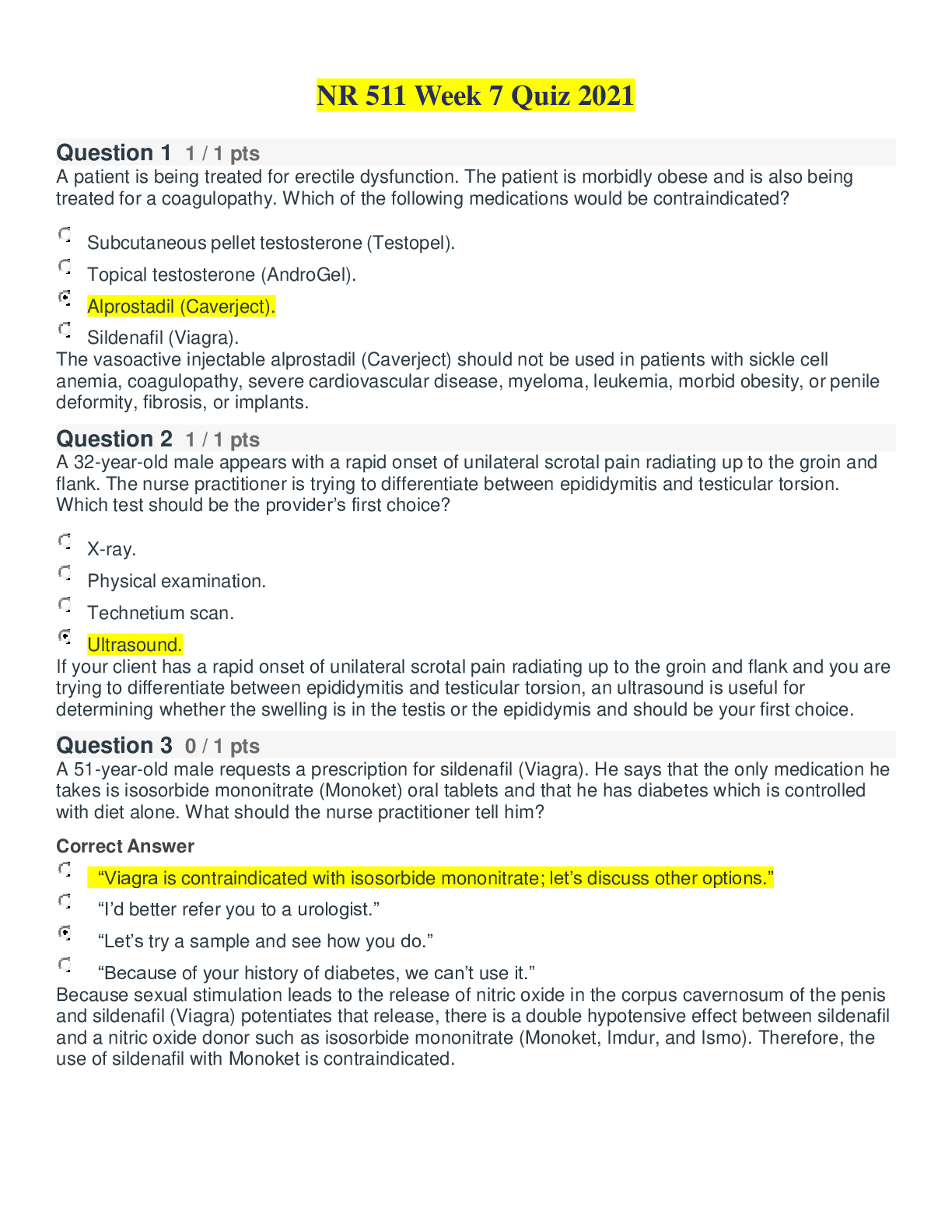
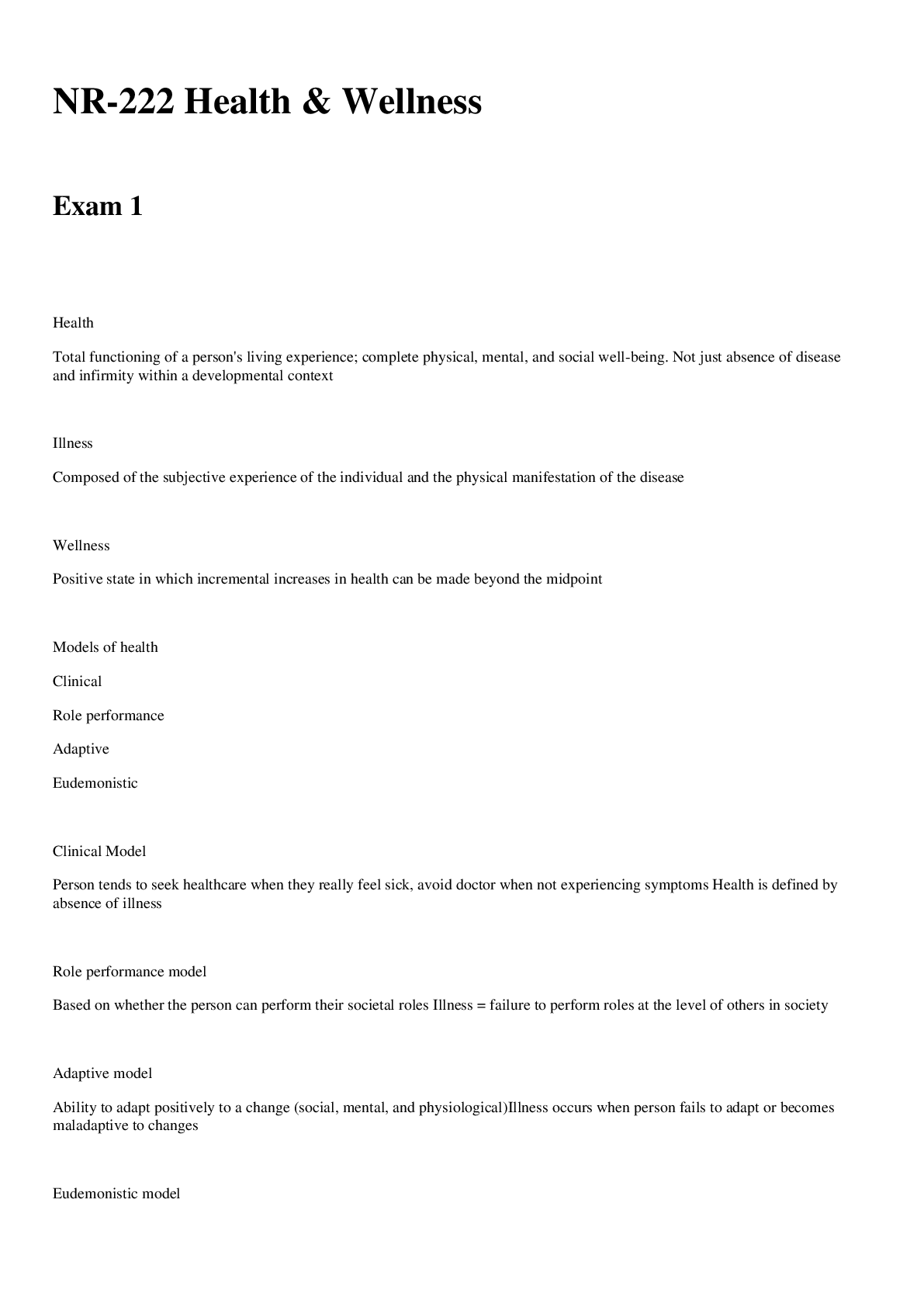
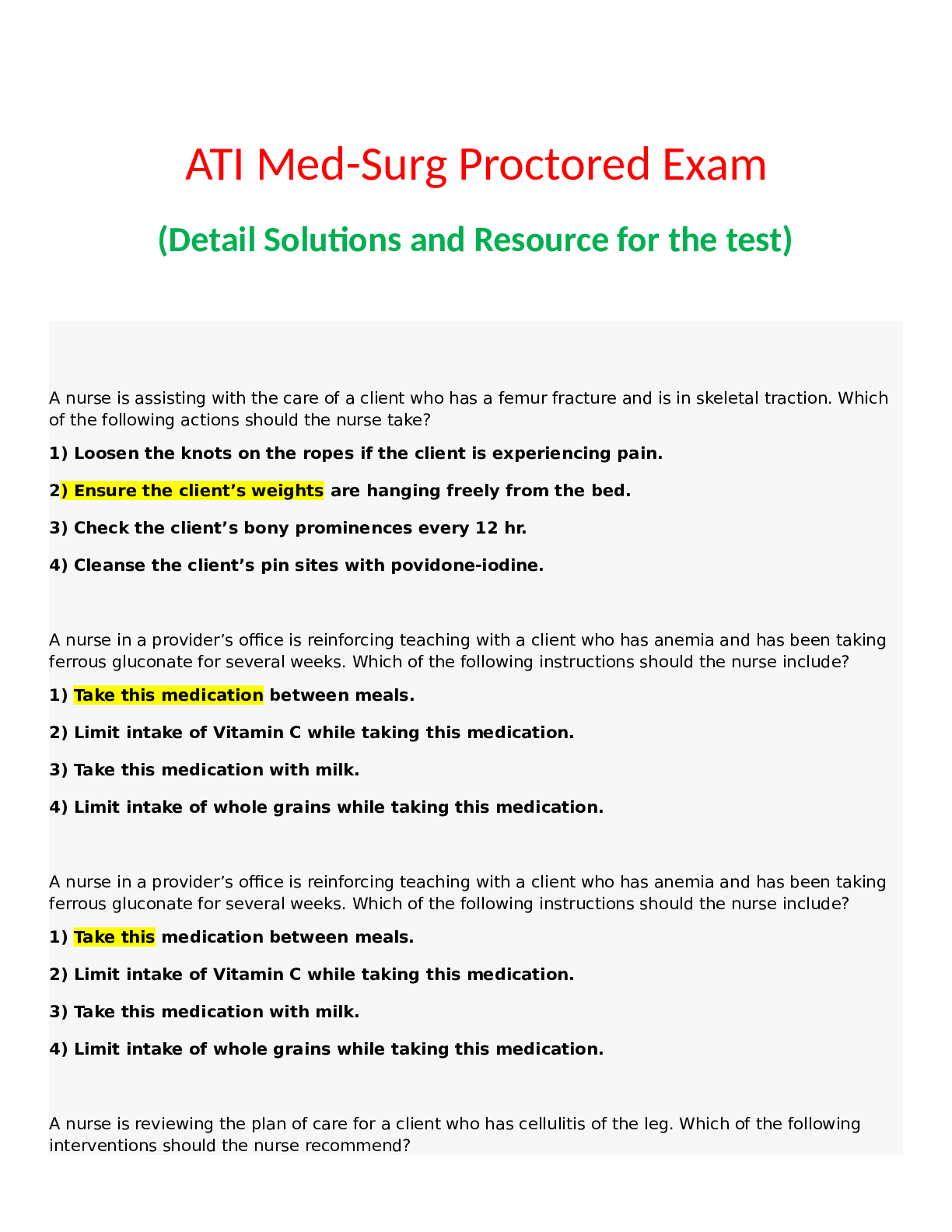
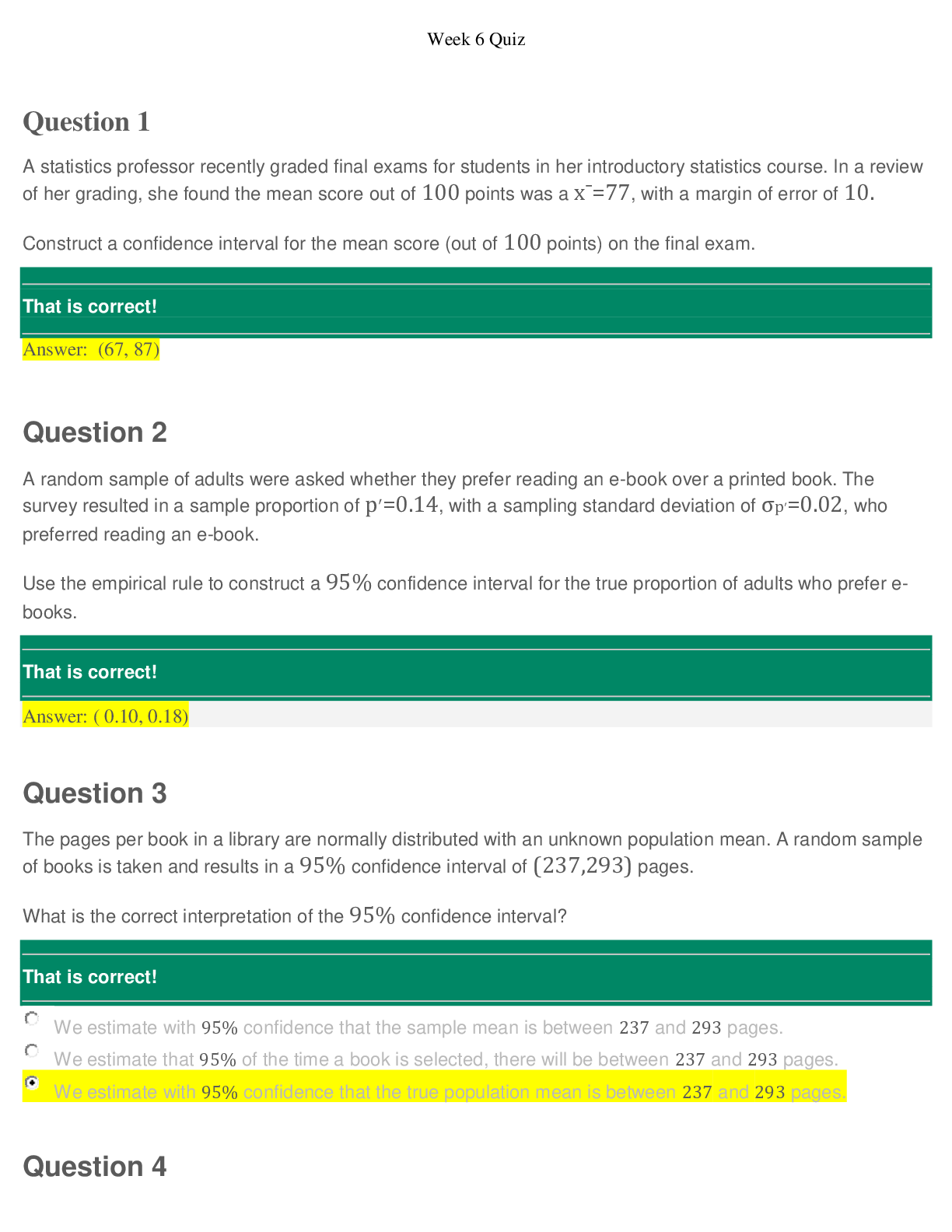
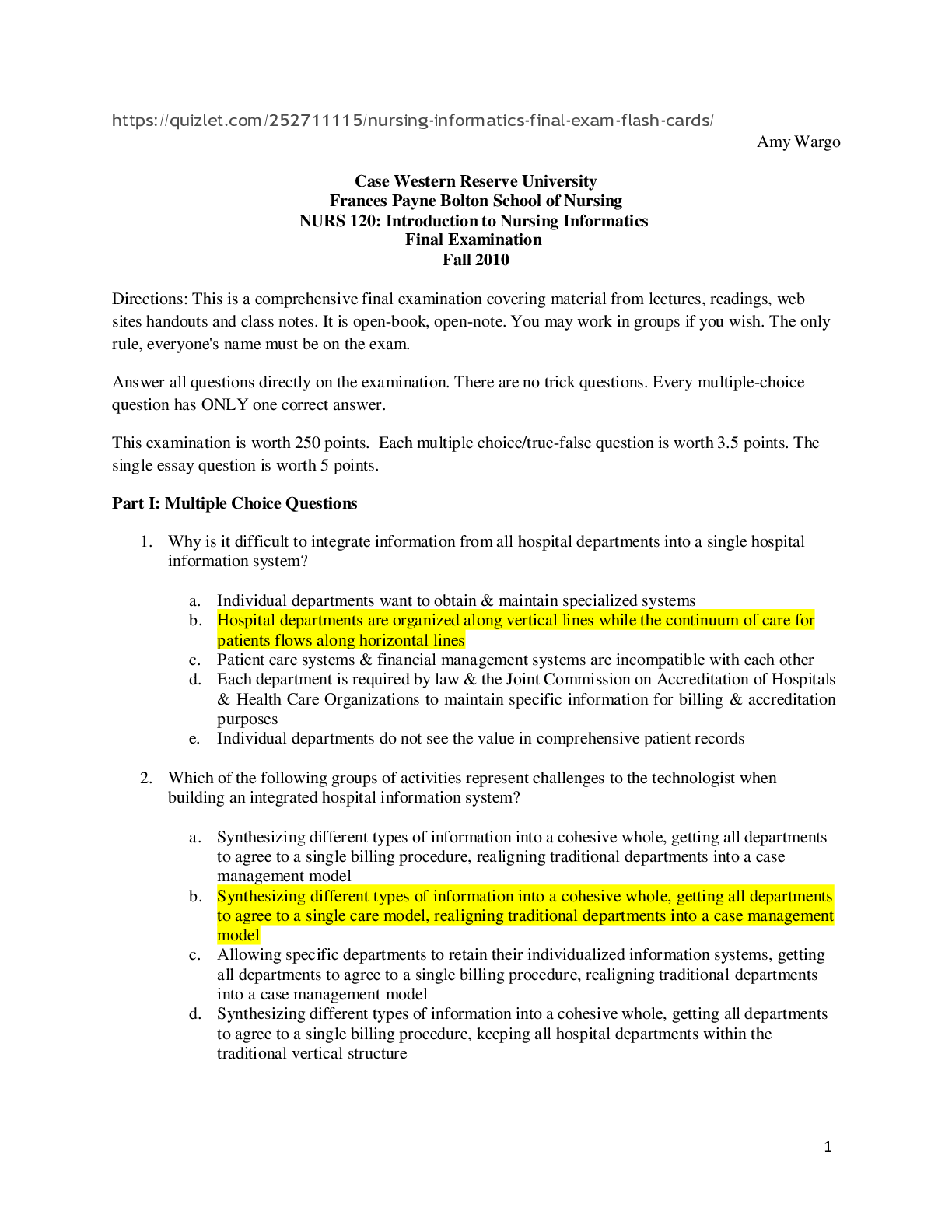
 – CHAMBERLAIN COLLEGE OF NURSING.png)