*NURSING > EXAM > Test Bank for Medical Surgical Nursing 7th Edition by Linton (All Chapters Questions And Answers ) (All)
Test Bank for Medical Surgical Nursing 7th Edition by Linton (All Chapters Questions And Answers )
Document Content and Description Below
Chapter 01: Aspects of Medical-Surgical Nursing Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What provides direction for individualized care and assures the delivery of ac... curate, safe care through a definitive pathway that promotes the client’s and the support persons’ progress toward positive outcomes? a. Physician’s orders b. Progress notes c. Nursing care plan d. Client health history ANS: C The nursing care plan provides direction for individualized care and assures the delivery of accurate, safe care through a definitive pathway that promotes the client’s and the support persons’ progress toward positive outcomes. DIF: Cognitive Level: Comprehension REF: p. 2 OBJ: 1 TOP: Nursing Care Plan KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Reduction of Risk 2. The nurse is performing behaviors and actions that assist clients and significant others in meeting their needs and the identified outcomes of the plan of care. What is the correct term for these nursing behaviors? a. Assessments b. Interventions c. Planning d. Evaluation ANS: B Caring interventions are those nursing behaviors and actions that assist clients and significant others in meeting their needs and the identified outcomes of the plan of care. DIF: Cognitive Level: Comprehension REF: p. 3 OBJ: 1 TOP: Interventions KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Reduction of Risk 3. The nurse understands the importance of being answerable for all actions and the possibility of being called on to explain or justify them. What term best describes this concept? a. Reliability b. Maturity c. Accountability d. Liability ANS: C Accountability means that a person is answerable for his or her actions and may be called on to explain or justify them. DIF: Cognitive Level: Comprehension REF: pp. 6-7 OBJ: 3 | 5 | 7 TOP: Accountability KEY: Nursing Process Step: N/A MSC: NCLEX: Physiological Integrity: Reduction of Risk MULTIPLE RESPONSE 1. The nurse manager is providing an inservice about conflict resolution. What modes of conflict resolution should be addressed? (Select all that apply.) a. Suppression b. Accommodation c. Compromise d. Avoidance e. Collaboration f. Competition ANS: B, C, D, E, F The modes of conflict resolution include accommodation, collaboration, compromise, avoidance, and competition. DIF: Cognitive Level: Knowledge REF: p. 7|p. 8|Table 1.1 OBJ: 7 TOP: Conflict Resolution KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. What are the characteristics of an effective leader? (Select all that apply.) a. Effective communication b. Rigid rules and regulations c. Delegates appropriately d. Acts as a role model e. Consistently handles conflict f. Focuses on individual development ANS: A, C, D, E Characteristics of an effective leader include effective communication, consistency in managing conflict, knowledge and competency in all aspects of delivery of care, effective role model for staff, uses participatory approach in decision making, shows appreciation for a job well done, delegates work appropriately, sets objectives and guides staff, displays caring, understanding, and empathy for others, motivates and empowers others, is proactive and flexible, and focuses on team development. DIF: Cognitive Level: Comprehension REF: p. 6 OBJ: 5 TOP: Leadership KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. is defined as the process by which information is exchanged between individuals verbally, nonverbally, and/or in writing or through information technology. ANS: Communication Communication is defined as the process by which information is exchanged between individuals verbally, nonverbally, and/or in writing or through information technology. DIF: Cognitive Level: Knowledge REF: p. 2 OBJ: 2 TOP: Communication KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. is the collection and processing of relevant data for the purpose of appraising the client’s health status. ANS: Assessment Assessment is the collection and processing of relevant data for the purpose of appraising the client’s health status. DIF: Cognitive Level: Knowledge REF: p. 2 OBJ: 1 | 2 TOP: Assessment KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 3. is concerned with the ethical questions that arise in the context of health care. ANS: Bioethics Bioethics is concerned with the ethical questions that arise in the context of health care. DIF: Cognitive Level: Knowledge REF: p. 4 OBJ: 3 TOP: Bioethics KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 4. Place the corresponding letter to each stage of conflict in the correct order. (Place the events in the appropriate sequence with capital letters. Do not separate answers with a space or punctuation. Example: ABCD.) a. Outcomes b. Conceptualization c. Frustration d. Action ANS: CBDA The stages of conflict in order are frustration, conceptualization, action, and outcomes. DIF: Cognitive Level: Comprehension REF: p. 7 OBJ: 7 TOP: Conflict KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 5. Place the corresponding letter to each key step in solving an ethical dilemma in the correct order. (Place the events in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Negotiate a plan. b. Clarify values. c. Ask if it is an ethical dilemma. d. Verbalize the problem. e. Gather information. f. Identify possible courses of action. g. Evaluate the plan over time. ANS: CEBDFAG The key step of solving an ethical dilemma in order are ask the question, is it an ethical dilemma, gather information, clarify values, verbalize the problem, identify possible course of action, negotiate a plan, and evaluate the plan over time. DIF: Cognitive Level: Analysis REF: p. 4 OBJ: 3 TOP: Ethical Dilemma KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 02: Medical-Surgical Practice Settings Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. While a home health nurse is making the entry to a service assessment on a homebound patient, the spouse of the patient asks whether Medicare will cover the patient’s ventilator therapy and insulin injections. What is the best response by the nurse? a. “Yes, Medicare will cover both the ventilator therapy and the insulin injections.” b. “No, Medicare will not cover either of these ongoing therapies.” c. “Medicare will cover the ventilator therapy, but it does not cover the insulin injections.” d. “Medicare will cover the ongoing insulin therapy, but it does not cover a highly technical skill such as ventilator therapy.” ANS: C Medicare will cover skilled nursing tasks such as ventilator therapy, but common tasks that can be taught to the family or the patient are not covered. DIF: Cognitive Level: Application REF: pp. 12-13 OBJ: 3 | 4 TOP: Medicare Coverage for Home Health KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 2. The wife of a patient asks the nurse whether her husband would be considered for placement in a skilled nursing care facility when he is discharged from the general hospital. The patient is incontinent, has mild dementia but is able to ambulate with a walker, and must have help to eat and dress himself. What is the nurse’s most appropriate response? a. “Yes, your husband would qualify for a skilled care facility because of his inability to feed and dress himself.” b. “No, your husband’s disabilities would not qualify him for a skilled facility.” c. “Yes, your husband qualifies for placement in a skilled care facility because of his dementia.” d. “Yes, anyone who is willing to pay can be placed in a skilled nursing facility.” ANS: B Placement in a skilled nursing facility must be authorized by a physician. A clear need for rehabilitation must be evident, or severe deficits in self-care that have a potential for improvement and require the services of a registered nurse, a physical therapist, or a speech therapist must exist. DIF: Cognitive Level: Analysis REF: p. 13 OBJ: 6 TOP: Placement Qualifications for Skilled Nursing Facility KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment 3. A nurse has noted that a newly admitted resident to an extended care facility stays in her room, does not take active part in activities, and leaves the meal table after having eaten very little. The nurse should analyze this relocation response as a. regression. b. social withdrawal. c. depersonalization. d. passive aggressive. ANS: B Social withdrawal is a frequent response to relocation. DIF: Cognitive Level: Application REF: p. 21 OBJ: 10 TOP: Relocation Response KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 4. A nurse clarifies to a new patient in a rehabilitation center what rehabilitation means. What statement made by the patient indicates a correct understanding? a. “I will return to my previous level of functioning.” b. “I will be counseled into a new career.” c. “I will develop better coping skills to accept his disability.” d. “I will attain the greatest degree of independence possible.” ANS: D The rehabilitation process works to promote independence at whatever level the patient is capable of achieving. DIF: Cognitive Level: Comprehension REF: p. 15 OBJ: 7 TOP: Rehabilitation Goals KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Coordinated Care 5. A nurse assesses a patient who needs to be reminded to take premeasured oral medications, wash, go to meals, and undress and come to bed at night, but coming and going as he pleases is considered safe for him. What facility placement would be most appropriate for this patient? a. Skilled care b. Intermediate care c. Sheltered housing d. Domiciliary care ANS: D Domiciliary care provides room, board, and supervision, and residents may come and go as they please. Sheltered housing does not provide 24-hour care. DIF: Cognitive Level: Comprehension REF: p. 19 OBJ: 3 | 9 TOP: “Levels of Care, Criteria for Domiciliary Residence” KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 6. A nurse is making a list of the members of the rehabilitation team, so the different types of services available to patients may be taught to a group of families. Which lists should be used? a. Physical therapist, nurse, family members, and personal physician b. Occupational therapist, dietitian, nurse, and patient c. Rehabilitation physician, laboratory technician, patient, and family d. Vocational rehabilitation specialist, patient, and psychiatrist ANS: A The rehabilitation team usually consists of all of the choices except the laboratory technician, dietitian, and psychiatrist. (The mental health role is represented by the psychologist.) DIF: Cognitive Level: Comprehension REF: p. 17 OBJ: 7 TOP: Rehabilitation Team Members KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 7. A nurse explains the level of disability to a patient who was injured in a construction accident that resulted in the loss of both his right arm and right leg. This loss has affected his quality of life and ability to return to previous employment. At what level should the client be classified as being disabled? a. I b. II c. III d. IV ANS: B The patient is limited in the use of his right arm for feeding himself, dressing himself, and driving his car, which are three main activities of daily living. He may be able to work if workplace modifications are made. DIF: Cognitive Level: Application REF: p. 15 OBJ: 8 TOP: Levels of Disability KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 8. A nurse explains that in 1990, the Americans with Disabilities Act (ADA) was passed. For which extended services for the disabled persons did this act provide? a. Covering the costs for the rehabilitation of disabled World War I servicemen by providing job training b. Extending protection to the disabled in the military sector, such as wheelchair ramps on military bases c. Extending protection to the disabled in private areas, such as accessibility to public restaurant bathrooms and telephones d. Affording disabled persons full access to all health care services ANS: C The ADA of 1990 extended the previous legislative Acts of 1920, 1935, and 1973. The ADA now covers private sector individuals and public businesses in particular. DIF: Cognitive Level: Comprehension REF: p. 16 OBJ: 8 TOP: Americans with Disabilities Act (ADA) of 1990 KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 9. A frail patient in a long-term care facility asks the nurse if a bath is to be given this morning. What is the best reply by the nurse to encourage independence and give the patient the most flexibility? a. “Based on your room number, you get bathed on Monday, Wednesday, and Friday. Today is Tuesday.” b. “If you want to eat breakfast in the dining room with the others, you may sponge yourself off in your bathroom.” c. “When your daughter comes this evening, ask her if she can give you a bath.” d. “I will bring a basin of water for a sponge off for right now. After breakfast, we will talk about a bath schedule.” ANS: D The resident should be provided as much flexibility as possible and support for independence. DIF: Cognitive Level: Application REF: p. 22 OBJ: 11 TOP: Maintenance of Autonomy in Extended Care Facility KEY: Nursing Process Step: Implementation MSC: NCLEX Physiological Integrity: Basic Care and Comfort 10. A computer programmer who lost both legs is being retained by his employer, who has made arrangements for a ramp and a special desk to accommodate the patient’s wheelchair. What is the disability level of the computer programmer? a. I b. II c. III d. IV ANS: B Level II allows for workplace accommodation, which is the desk modification in this case. DIF: Cognitive Level: Analysis REF: p. 15 OBJ: N/A TOP: Reasonable Accommodation KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 11. A partially paralyzed forklift operator is to be retrained by vocational rehabilitation services for less demanding office work. What law provides for this rehabilitation? a. Vocational Rehabilitation Act of 1920 b. Social Security Act of 1935 c. Rehabilitation Act of 1973 d. Americans with Disabilities Act of 1990 ANS: C The Rehabilitation Act of 1973 provided a comprehensive approach and expanded resources for public vocational training. DIF: Cognitive Level: Comprehension REF: p. 16 OBJ: 7 TOP: Rehabilitation Legislation KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 12. The home health care nurse performs all the following actions. Which is the only action that is reimbursable under Medicare payment rules? a. Observing a spouse cleaning and changing a dressing b. Taking a frail couple for a walk to provide exercise c. Watching a patient measure out all medications d. Teaching a patient to self-administer insulin ANS: D Medicare reimburses skilled techniques that are clearly spelled out; these include teaching but not return demonstration–type actions by patient or family. DIF: Cognitive Level: Comprehension REF: pp. 12-13 OBJ: 4 TOP: Medicare Reimbursable Actions KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 13. A patient with multiple sclerosis must be fed, bathed, and dressed. How should the nurse assess this patient? a. Disabled b. Disadvantaged c. Handicapped d. Impaired ANS: D Feeding oneself, dressing, and bathing are activities of daily living. The patient is impaired in this scenario. DIF: Cognitive Level: Analysis REF: p. 15 OBJ: 7 TOP: Principles of Rehabilitation | Defining Levels of Loss of Functioning Independently KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity 14. Which law initially provided for rehabilitation of disabled Americans? a. Vocational Rehabilitation Act of 1920 b. Social Security Act of 1935 c. Rehabilitation Act of 1973 d. Americans with Disabilities Act of 1990 ANS: A The U.S. government has passed four pieces of legislation to identify and meet the needs of disabled individuals with each one being more inclusive. The first one was passed in 1920. DIF: Cognitive Level: Knowledge REF: p. 16 OBJ: 8 TOP: Rehabilitation Legislation KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 15. A client was admitted to a long-term residential care facility. On what should the admitting nurse tell the family the concepts of long-term care are based? a. Amount of activities the resident can do for herself b. Maintenance care with an emphasis on incontinence c. Successful adaptation to the regulations of the home d. Maintenance of as much function as possible ANS: D Maintenance of function and encouraging autonomy and independence are some of the basic concepts of long-term care. DIF: Cognitive Level: Comprehension REF: p. 18 OBJ: 11 TOP: Principles of Nursing Home Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 16. A 58-year-old patient with diabetes is recuperating from a broken hip and is concerned about how to pay for rehabilitation. The nurse should inform this patient that funds for rehabilitation are available from which resource? a. Vocational Rehabilitation Act of 1920 b. Rehabilitation Act of 1973 c. Disabled American Veterans Act of 1990 d. Title V, Health of Crippled Americans 1935 ANS: B The Rehabilitation Act of 1973 assists in paying for rehabilitation for those who are younger than 65 years of age and who will benefit from vocational rehabilitation through teaching. DIF: Cognitive Level: Comprehension REF: p. 16 OBJ: 8 TOP: Legislation for Funding Health Care KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 17. What is an example of a description of community health nursing? a. Visiting patients in their homes after hospital discharge to assess their personal health status b. Asking a nursing assistant (NA) to identify the health services most needed in the patient’s personal life c. Meeting with residents of low-income housing to identify their health care needs d. Developing a hospital-based home health care service ANS: C Whereas community-based nursing looks at identified community needs and provides care at all levels of wellness and illness, community health nursing seeks to provide services to groups to modify or create systems of care. DIF: Cognitive Level: Comprehension REF: pp. 10-11 OBJ: 2 TOP: Defining Community-Based Nursing versus Community Health Nursing KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Coordinated Care 18. Home health nurses have some different nursing activities than those of community health nurses. Which statement best describes the home health nurse’s activities? a. Conducting health education classes in a senior citizens’ common residence building b. Conducting blood pressure screening on a regular basis at a local mall c. Visiting and assessing the home care and further teaching needs of a patient who has been recently discharged from the hospital d. Acting as a nurse consultant to a chronic psychiatric section in a state institution ANS: C The home health nurse works with individuals in the home; the other descriptors are community nurse activities. DIF: Cognitive Level: Comprehension REF: p. 13 OBJ: 1 | 5 TOP: Activities of the Home Health Nurse KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 19. Based on guidelines from the Americans with Disability Act (ADA), which question is an appropriate choice for the director of nurses to ask a nurse with an artificial leg who is applying for a staff position in an extended care facility? a. “How long have you had your prosthesis?” b. “How many flights of stairs are you able to climb without assistance?” c. “Are you able to lift a load of 45 lb?” d. “Has your disability caused you to miss work?” ANS: C Queries to disabled job applicants can be made relative to specific job functions, but they cannot be asked relative to the severity of the disability or the degree of disability in general. DIF: Cognitive Level: Application REF: p. 16 OBJ: 7 | 8 TOP: ADA KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 20. A nurse reminds a resident in a long-term care facility that he has autonomy in many aspects of his institutionalization. What is an example of autonomy? a. Selection of medication times b. Availability of his own small electrical appliances c. Smoking in the privacy of his own room d. Application of advance directives ANS: D The application of advance directives is an autonomous decision. Agency protocols relative to medication times, access to private electrical devices, and smoking are rarely waived; these policies are not in the control of the resident. DIF: Cognitive Level: Comprehension REF: p. 22 OBJ: 10 TOP: Autonomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation MULTIPLE RESPONSE 1. What care skills are safe and appropriate for the licensed practical nurse (LPN) to teach family members in the home health care setting? (Select all that apply.) a. Insulin injection b. Sterile dressing changes c. Venipunctures d. Periodic Foley catheter insertions e. Instillation of eye drops f. Changing dressings on small wounds ANS: A, E, F Insulin injections, instillation of eye drops, and small wound dressing changes are safe to teach a nonprofessional caregiver. Sterile dressings, venipunctures, and inserting Foley catheters are considered skilled, and the costs for these are reimbursed by Medicare. DIF: Cognitive Level: Comprehension REF: p. 13 OBJ: 3 TOP: Skills Taught by Home Health Nurse KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 2. The nursing care plan in a long-term care facility calls for the documentation of regressive behavior of a newly admitted 82-year-old resident who has had congestive heart failure and osteoarthritis. Of these behaviors observed by the nurse, which should be documented as regression? (Select all that apply.) a. Talks nonstop to staff and other residents. b. Wets and soils self several times a day. c. Wakes in the middle of the night and is unable to return to sleep. d. Wears the same clothes day after day. e. Cries frequently for no apparent reason. ANS: B, D, E Behaviors that are infantile or immature in the absence of dementia are considered regressive. Frequent episodes of crying and inattention to personal hygiene are regressive in nature. Excessive talking and wakefulness may be related to relocation anxiety, but they are not considered regressive. DIF: Cognitive Level: Analysis REF: pp. 20-21 OBJ: 10 TOP: Impact of Relocation KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 3. From what do most quality-of-care problems in home health care result? (Select all that apply.) a. Patient’s noncompliance b. Family’s reluctance to participate in the care c. Inadequate documentation d. Limited funding e. Defective communication among care team members ANS: C, E Inadequate communication and incomplete documentation create most of the quality-of-care problems. DIF: Cognitive Level: Comprehension REF: pp. 11-12 OBJ: 2 TOP: Communication in Home Health Setting KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 4. An 80-year-old man is newly admitted to a long-term care facility and suddenly becomes incontinent of urine at night. What nursing interventions should be used to help restore self-toileting? (Select all that apply.) a. Waking the resident every 2 hours and escorting him to the bathroom b. Leaving a night-light on c. Discouraging the use of long-legged pajama bottoms d. Placing a urinal at the bedside e. Keeping the room uncluttered ANS: B, C, D, E Providing light in an uncluttered room, encouraging clothing that does not impede self-toileting, and making the urinal available increase independence and alleviate situations that make self-toileting difficult. Waking a resident not only disturbs his or her rest, but doing so also increases dependency on the staff. DIF: Cognitive Level: Application REF: pp. 11-12 OBJ: 10 | 11 TOP: Independence in Long-Term Care Center KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. The nurse clarifies that an impairment that creates a measurable diminished capacity to work is a(n) . ANS: disability When there is a measurable impairment that changes the individual’s lifestyle, it is referred to as a disability. DIF: Cognitive Level: Knowledge REF: p. 15 OBJ: N/A TOP: Rehabilitation Concepts KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Coordinated Care 2. What should the home health nurse do when teaching a family member the skill of injecting insulin effectively? Prioritize these nursing interventions for this situation. (Place the events in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Offer instruction at an appropriate pace. b. Write down the steps of the procedure. c. Assess the level of knowledge of the family member. d. Inquire about the preferred learning style. e. Evaluate the family member’s performance. ANS: CBDAE Effective teaching depends on assessing the level of knowledge, breaking down the skill in steps, offering instruction in the preferred style, pacing the instruction appropriately, and evaluating the performance. DIF: Cognitive Level: Application REF: p. 14 OBJ: 1 TOP: Home Health Teaching KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 3. Prioritize the steps in solving an ethical dilemma. (Place the events in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Evaluate the outcome. b. Plan an approach. c. Visualize the consequences. d. Take action. e. Identify the problem. ANS: EBCDA To solve an ethical dilemma, one must clearly identify the problem, plan an approach, visualize the consequences, take action, and evaluate the outcome. DIF: Cognitive Level: Comprehension REF: p. 11 OBJ: 7 TOP: Solving an Ethical Dilemma KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 03: Medical-Surgical Patients: Individuals, Families, and Communities Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What should be included in a patient’s care plan in consideration of cultural similarities? a. Family, educational background, and economic level should all be considered. b. Subtle communication involving languages should be considered. c. Families have strong patriarchal leaders. d. Culture is learned, shared, and expressed similarly among members. ANS: D Different cultures have some similarities and some differences. How the culture is expressed in health care settings will be diverse. DIF: Cognitive Level: Comprehension REF: p. 26 OBJ: 4 TOP: Similarities among Cultures KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Coordinated Care 2. What is the basis for the health–illness continuum? a. Prevention of acute illness b. Individual response to health or illness c. Promotion of health and wellness d. Variation in degree of health or illness ANS: D Currently, health and illness are viewed as relative states along a continuum. Individuals are at neither absolute health nor absolute illness but are in an ever-changing state of being. DIF: Cognitive Level: Comprehension REF: pp. 25-26 OBJ: 5 TOP: Current View of Health-Illness Continuum KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 3. What is the current concern of the health care system? a. Treating illness b. Preventing illness c. Promoting optimal function in the chronically ill d. Caring for patients with acute and chronic illness ANS: B Health promotion activities are directed toward maintaining or enhancing well-being as a protection against illness. DIF: Cognitive Level: Knowledge REF: pp. 25-26 OBJ: 2 | 5 TOP: Health Promotion KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 4. What is the primary reason that family is an important unit in society? a. Offers unconditional love and acceptance. b. Provides emotional support and security. c. Is essential to life and society. d. Promotes cultural values and attitudes. ANS: B A family is defined as being joined together by bonds of sharing and emotional closeness. DIF: Cognitive Level: Comprehension REF: p. 33 OBJ: 8 TOP: The Family Unit KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 5. What should a nurse assess when a patient comes from an extended family? a. Multiple wage earners b. Three generations living together c. Children from previous marriages d. Parents of different ethnic origins ANS: B The extended family consists of relatives of either spouse who live with the nuclear family. Children, regardless of their parentage, are considered part of the nuclear family. DIF: Cognitive Level: Comprehension REF: p. 33 OBJ: 8 TOP: Types of Families KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 6. A nurse is designing a home care plan for a child with a congenital disease and is assessing the family values regarding home care. What is the best resource for the nurse to use? a. Current literature on congenital deformities b. General knowledge of the culture c. Patient’s family d. Written survey ANS: C Determining the family’s values, beliefs, customs, and behaviors that influence health needs and health care practice is important. The best source is the family itself. DIF: Cognitive Level: Comprehension REF: p. 34 OBJ: 11 TOP: Cultural Aspects KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 7. A nurse counsels a family regarding the stage of families with adolescents. Which developmental task is appropriate for the nurse to include? a. Maintaining relationships with the extended family b. Developing parental roles to meet the needs of children c. Maintaining a satisfying marital relationship d. Maintaining open communication between parent and children ANS: D The family developmental tasks at this stage include balancing freedom with responsibility and maintaining communication between parents and children. DIF: Cognitive Level: Comprehension REF: p. 34|Table 3.3 OBJ: 8 TOP: Family Life Cycles KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 8. Which developmental task should families master in later life? a. Becoming role models for their grandchildren b. Making a significant contribution to society c. Abandoning the parental role to grown children d. Maintaining a satisfactory living arrangement ANS: D The last stage of the family life cycle includes families in later life who are adjusting to retirement, the aging process, decreased self-esteem, and changes in status and health issues. Maintaining a satisfactory living arrangement is the primary developmental task. DIF: Cognitive Level: Comprehension REF: p. 34|Table 3.3 OBJ: 8 TOP: Family Life Cycles KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 9. Culture and social class usually set a precedent for different roles and responsibilities of each family member. Which example best demonstrates the healthiest family? a. The father assumes the role as breadwinner. b. The mother assumes the role as homemaker. c. The father or mother shares the roles of breadwinner and homemaker. d. The roles of breadwinner or homemaker can be shifted as needed. ANS: D A healthy family is one in which the opportunity to shift roles occurs easily from time to time. DIF: Cognitive Level: Comprehension REF: p. 34 OBJ: 8 TOP: Family Role StructureKEY: Nursing Process Step: N/A MSC: NCLEX: N/A 10. During a family counseling session, a patient, a mother of a 5-year-old son, states, “I don’t understand why my husband continually tries to get our son involved in T-ball. My son said the coach and his dad yelled at him and told him the game was lost because he couldn’t catch the ball.” What is the most important family interaction to maintain a healthy family unit? a. Maintain open communication among all family members. b. Encourage self-acceptance and self-esteem for all family members. c. Encourage all family members to participate in community events. d. Realize that not all family members may be able to fulfill assigned roles. ANS: B The most important influence on family interaction is the self-esteem of each member. DIF: Cognitive Level: Comprehension REF: p. 35 OBJ: 9 TOP: Family Interaction KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 11. For the past three evenings, shortly after their arrival in the hospital unit, the parents of a 14-year-old daughter begin to argue about the cost of the hospitalization and the time required to come to the hospital. The patient begins to cry and complains about her abdominal pain. What role is the patient assuming? a. Caretaker b. Martyr c. Blocker d. Scapegoat ANS: D A scapegoat usually assumes the role to maintain homeostasis, serving to divert attention from marital conflict between spouses. DIF: Cognitive Level: Analysis REF: p. 34 OBJ: 9 | 10 TOP: Family Role StructureKEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 12. A patient, a 36-year-old mother of four children, is crying. She relates to you that her best friend just told her, “You are a good mother and you do everything perfectly, but I don’t think you enjoy it.” What role is the patient assuming? a. Caretaker b. Martyr c. Contributor d. Harmonizer ANS: B A martyr sacrifices everything for the sake of the family. DIF: Cognitive Level: Analysis REF: p. 34 OBJ: 9 | 10 TOP: Family Role StructureKEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 13. What is the basis for the roles children assume in families? a. Obligation b. Instinct c. Observation d. Rewards ANS: D Parents reward children for fulfilling certain roles, which children adopt and maintain as they mature. DIF: Cognitive Level: Comprehension REF: p. 34|p. 35 OBJ: 9 TOP: Family Role StructureKEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 14. A patient confides that her husband shares only the incidental happenings of his day at work as he reads the paper, and he never tells her that he loves her anymore. She is beginning to wonder if their marriage is getting stale. What communication pattern should the nurse recognize? a. Affective b. Affectional c. Functional d. Dysfunctional ANS: D One type of dysfunctional communication involves using chitchat about unimportant daily occurrences to avoid discussing meaningful issues or expressing feelings. DIF: Cognitive Level: Analysis REF: p. 35 OBJ: 9 TOP: Functional Communication KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 15. What should a nurse consider when discussing the communication patterns of families with the patient? a. Cultural aspects of the family b. Age of the family members c. Role adopted by each family member d. Number of members in the family ANS: A Although each option has significance, cultural aspects must be considered in determining the functioning level of the family as it affects the roles taken. DIF: Cognitive Level: Comprehension REF: p. 35 OBJ: 9 TOP: Functional Communication KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 16. A patient states that her 5-year-old daughter is always running up to relatives and friends and wants to give them a big hug and kiss. The patient asks if her daughter is appropriate in her actions. What is the most appropriate reply based on the concepts of functional communication? a. “Your daughter’s actions are definitely dysfunctional.” b. “Your daughter is just being a ‘little girl’ and will outgrow being so affectionate.” c. “Your daughter is going through a normal developmental phase.” d. “Does your mother-in-law show signs of affection toward your daughter?” ANS: C Physical expression of emotion usually dominates in early childhood and is normal in the developmental pattern. DIF: Cognitive Level: Application REF: p. 35 OBJ: 9 TOP: Functional Communication KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 17. For what should functional patterns of communication in the family setting provide a means? a. Nurturing b. Information c. Closeness d. Openness ANS: A Functional patterns of communication include emotional and affective communication that deals with the expression of feelings and nurturing. A healthy family is able to demonstrate a wide range of emotions and feelings. DIF: Cognitive Level: Comprehension REF: p. 35 OBJ: 9 TOP: Functional Communication KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 18. What does the manner in which a family unit adapts to stress affect? a. Ability to communicate and function b. Health and function c. Level of affective communication d. Ability to adapt and function ANS: B The manner in which a family handles stress can affect the health of the family. DIF: Cognitive Level: Comprehension REF: pp. 36-37 OBJ: 11 TOP: Stress and Adaptation KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 19. A patient who was recently diagnosed with cancer tells the nurse that she is so grateful for her children and family because she does not know what she would do without them. Which coping response is being exhibited? a. Internal family b. External family c. Family communication d. Social support ANS: A The internal family coping responses are those that the family relationships use as support. DIF: Cognitive Level: Comprehension REF: p. 36 OBJ: 10 TOP: Coping Strategies KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 20. What is the main role of the nurse when assessing families and their coping strategies? a. Emotional support and reassurance b. Information and reassurance c. Emotional support and referral d. Elimination of the stressor ANS: B Families need information and reassurance. DIF: Cognitive Level: Comprehension REF: pp. 36-37 OBJ: 10 TOP: Role of the Nurse KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 21. What is the best description of the current view of the family as a unit? a. Functioning together to provide security and support to its members b. Functioning to meet the needs of society and support its members c. A unit of two or more that shares common goals and mutual support d. A unit of two or more joined together by mutual bonds and identity ANS: D Friedman (1997) defined the family as “…two or more persons joined together by bonds of sharing and emotional closeness and who identify themselves as being part of the family.” DIF: Cognitive Level: Comprehension REF: p. 34 OBJ: 8 TOP: Family Role StructureKEY: Nursing Process Step: N/A MSC: NCLEX: N/A 22. A nurse reminds a patient that communication in the family unit involves continual exchange of information. Which is the best example of this concept? a. Determining the intent of the communication being sent b. Determining whether the communication is functional or dysfunctional c. Accepting individual differences d. Excluding emotional responses ANS: C Clear communication is a way of fostering a nurturing environment. Communication patterns in a functional family demonstrate an acceptance of individual differences, openness, honesty, and recognition of needs. DIF: Cognitive Level: Comprehension REF: p. 35 OBJ: 9 TOP: Family Communication KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 23. What is the basis for the health–illness continuum? a. Prevention of acute illness b. Individual response to health or illness c. Promotion of health and wellness d. Variation in degree of health or illness ANS: D Currently, health and illness are viewed as relative states along a continuum. Individuals are at neither absolute health nor absolute illness but are in an ever-changing state of being. DIF: Cognitive Level: Comprehension REF: p. 25 OBJ: 2 | 5 TOP: Current View of Health-Illness Continuum KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 24. What should a nurse take into consideration regarding developmental tasks when planning patient care? a. All of the activities performed throughout life. b. Activities learned primarily in the middle years of life. c. Things to be learned and accomplished in each stage of life. d. All actions taken when confronted with specific problems. ANS: C Developmental processes are changes that present challenges that must be undertaken and mastered for a person to go on to the next stage successfully. DIF: Cognitive Level: Comprehension REF: p. 30 OBJ: 8 TOP: Developmental Tasks KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 25. Which behavior is not characteristic of a young adult’s developmental task? a. Living in his or her own apartment b. Accepting a place on the board of a community agency c. Interacting with a large group of friends d. Dating many different young women ANS: D As young adults enter their 30s and 40s, their focus is directed mainly toward raising a family and furthering their career. A heterosexual intimate relationship is not in keeping with developmental tasks. DIF: Cognitive Level: Comprehension REF: pp. 30-31 OBJ: 8 TOP: Developmental Tasks: Young Adulthood KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Growth and Development MULTIPLE RESPONSE 1. What is included in the functional communication styles in a family? (Select all that apply.) a. Openness b. Subtlety c. Chitchat d. Spontaneity e. Self-disclosure ANS: A, D, E Functional communication is open and honest and has no subtlety or superficial chitchat. DIF: Cognitive Level: Comprehension REF: p. 35 OBJ: 9 TOP: Functional Communication KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 2. A nurse makes a patient referral to a community resource. What benefit(s) will this referral provide? (Select all that apply.) a. Provision of helpful literature b. Ongoing and consistent assistance c. Reassurance to the family members that they are not alone d. A variety of free services e. Organization of a support group ANS: A, B, C, E Community resources can provide assistance, literature, and support in an ongoing and consistent manner, but the services are not always free. DIF: Cognitive Level: Comprehension REF: p. 37 OBJ: 12 TOP: Community Resources KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care COMPLETION 1. The process in which children mature and take on the values of their families and their society is called . ANS: enculturation Enculturation is the process of learning to be part of a culture. DIF: Cognitive Level: Comprehension REF: p. 26|p. 27|p. 33 OBJ: 3 TOP: Enculturation KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. A nurse congratulates a patient for successfully coping with a family crisis. The state of having used coping strategies effectively is classified as . ANS: mastery Mastery is attained when coping skills are successful in coping with a crisis. DIF: Cognitive Level: Comprehension REF: p. 36 OBJ: 10 TOP: Mastery KEY: Nursing Process Step: Evaluation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 3. The nurse includes the family in patient care to maintain the family’s . ANS: self-esteem Self-esteem is supported and maintained when family is given opportunity to contribute to the planning of patient care. DIF: Cognitive Level: Comprehension REF: p. 37 OBJ: 8 TOP: Maintenance of Self-Esteem KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation Chapter 04: Health, Illness, Stress, and Coping Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What is the traditional view of health? a. Promotes optimal function. b. Views health and illness as separate concepts. c. Defines health as an absence of illness. d. Emphasizes the prevention of disease. ANS: B Traditionally, health and illness have been viewed as separate entities with a focus on the illness and not in attaining the highest quality of life possible when a cure is not possible. DIF: Cognitive Level: Comprehension REF: pp. 41-42 OBJ: 1 TOP: Traditional View of Health and Illness KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 2. What is the current view of health? a. Promotes the highest quality of life possible, both mentally and socially. b. Includes mental, physical, social, and emotional adaptation to the environment. c. Includes the basic physiologic needs and self-actualization. d. Relies on alternative therapies for the treatment and cure of diseases. ANS: B A healthy person maintains stability and comfort by adapting physically, mentally, emotionally, and socially to internal and external events. DIF: Cognitive Level: Comprehension REF: pp. 41-42 OBJ: 1 TOP: Current View of Health and Illness KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 3. During the initial gathering of data, a patient reveals a weight loss of 17 lb since the death of his spouse 5 weeks earlier. He says that he is not sleeping and has no appetite. What category of unmet needs should be considered by the nurse according to Maslow’s hierarchy of needs? a. Physiologic b. Safety and security c. Love and belonging d. Self-actualization ANS: A Physiologic needs include oxygen, fluids, and nutrition and must be met before the higher levels of needs are provided. DIF: Cognitive Level: Application REF: p. 41 OBJ: 2 TOP: Maslow’s Basic Human Needs KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 4. What is the major advantage of using Maslow’s hierarchy of needs when planning nursing care for patients? a. Establishes a nursing diagnosis. b. Improves problem-solving techniques. c. Prioritizes patient care. d. Establishes priorities of care. ANS: C Priorities for nursing care can be based on the level of human needs; physical needs take priority over security needs. DIF: Cognitive Level: Comprehension REF: p. 41 OBJ: 2 TOP: Maslow’s Basic Human Needs KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 5. A nurse points out that a physiologic response to stress involves the total body. Which syndrome is this considered? a. General adaptation b. Local adaptation c. Negative feedback d. Total adaptation ANS: A General adaptation syndrome is the physiologic response of the whole body to stress. DIF: Cognitive Level: Knowledge REF: p. 43 OBJ: 4 TOP: Stress Response KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 6. What are the ability to solve problems and to maintain self-confidence and the willingness to accept criticism incorporated in according to Maslow? a. Safety and security b. Self-esteem c. Self-actualization d. Love and belonging ANS: C Self-actualization is characterized by the ability to solve problems, the willingness to accept suggestions and criticism from others, and the maintenance of broad interests and communication skills. DIF: Cognitive Level: Comprehension REF: p. 41 OBJ: 2 TOP: Maslow’s Basic Human Needs KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 7. A patient returning from surgery complains of incisional pain that is now rated 7 in intensity on the 1-to-10 pain scale. What should the nurse be aware that pain exemplifies? a. General adaptation syndrome b. Local adaptation syndrome c. Counter-current response d. Neuroendocrine response ANS: B Local adaptation syndrome is a short-term, local response to a specific stressor. Examples include pain, blood clotting, and wound healing. DIF: Cognitive Level: Comprehension REF: p. 43 OBJ: 5 | 6 TOP: Stress Response KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. A nurse clarifies that a neuroendocrine response involves both the autonomic nervous system and the endocrine system. Which syndrome is this considered? a. Local adaptation b. Total adaptation c. Acute adaptation d. General adaptation ANS: D The neuroendocrine response primarily involves the autonomic nervous and endocrine systems and is considered part of the general adaptation syndrome, which is physiologic and affects the entire body. DIF: Cognitive Level: Comprehension REF: p. 43 OBJ: 5 | 6 TOP: Stress Response KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. Which syndrome includes the alarm reaction stage, resistance stage, and exhaustion stage? a. Local adaptation syndrome b. General adaptation syndrome c. Total adaptation syndrome d. Absolute adaptation syndrome ANS: B After the initial alarm stage (of the general adaptation syndrome), the body stabilizes and physiologic processes return to normal levels. This is followed by the resistance stage. If the stressor lasts too long, the individual may enter the third stage of adaptation, which is exhaustion. DIF: Cognitive Level: Knowledge REF: p. 43 OBJ: 4 TOP: Stress Response KEY: Nursing Process Step: N/A MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. A nurse gives the example of when an individual becomes frightened and experiences an increased heart rate and mental activity along with increased blood flow to the skeletal muscles and dilated pupils. The person is experiencing an alarm reaction that helps the body defend against stressors. What type of response is the alarm reaction considered? a. Positive feedback response b. Negative feedback response c. Fight-or-flight response d. Homeostasis response ANS: C The alarm reaction causes the body to respond to stress physiologically. Hormone levels, heart rate, cardiac output, respiratory rate, oxygen intake, and mental energy are increased, and the pupils dilate. These reactions together are called the fight-or-flight response. DIF: Cognitive Level: Comprehension REF: p. 46 OBJ: 7 | 8 TOP: Stress Response KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. A patient is being discharged from same-day surgery after a tonsillectomy. The nurse is aware that the patient will be in the phase of general adaptation syndrome, in which the body begins to heal after injury. Which stage is this considered? a. Alarm stage b. Resistance stage c. Exhaustion stage d. Initial stage ANS: B The resistance stage is characterized by adapting to the stressor. If the stressor can be overcome or repaired, as in a short-term illness or injury, the body begins to heal. DIF: Cognitive Level: Comprehension REF: p. 43 OBJ: 4 TOP: Stress Response KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. An anxious co-worker who is to present a comprehensive report to the hospital board on innovative staffing patterns sits down at a table in the lunchroom and begins to tell you what will be presented in the report. Which coping strategy is this co-worker using? a. Event rehearsal b. Problem solving c. Event review d. Social support ANS: A Coping strategies include event rehearsal, confrontation, distancing or denial, self-control, social support, accepting responsibility, faith, problem solving, positive reappraisal, and event review. Event review is discussing situations. DIF: Cognitive Level: Comprehension REF: pp. 45-46 OBJ: 9 TOP: Coping KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Physiological Adaptation 13. What is the best example for a nurse to use when explaining chronic illness? a. Acne b. Appendicitis c. Heart attack d. Asthma ANS: D Chronic illness, such as asthma, usually involves lifetime impairment or disability and requires long-term rehabilitation and medical or nursing treatment. Examples of chronic illness include coronary artery disease, diabetes, and endocrine disorders. Acne, appendicitis, and a heart attack are conditions that are acute in nature, although they may indicate a serious illness. DIF: Cognitive Level: Comprehension REF: p. 42 OBJ: 1 TOP: Concept of Illness KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 14. A nurse assesses that smoking, drinking alcohol, and exercising compulsively may occur as responses to a stressful situation. What type of response should this be considered? a. External b. Withdrawal c. Denial d. Internal ANS: D Examples of internal resources are physiologic and psychologic responses such as smoking, drinking alcohol, eating, and crying. DIF: Cognitive Level: Comprehension REF: pp. 45-46 OBJ: 7 | 8 TOP: Adaptation to Stress KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 15. Which type of response is demonstrated when an individual seeks help from family, friends, or a community resource during a time of stress? a. Internal b. External c. Physiologic d. Psychologic ANS: B Patients who deal with stress may use external responses, including help from family, friends, and service agencies in the community. DIF: Cognitive Level: Comprehension REF: pp. 45-46 OBJ: 7 | 8 TOP: Coping and Adaptation KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 16. What is the term for activities directed toward maintaining or enhancing well-being against illness? a. Health promotion b. Health treatment c. Health evaluation d. Health assessment ANS: A Health promotion activities are directed toward maintaining or enhancing well-being as a protection against illness. DIF: Cognitive Level: Knowledge REF: pp. 48-49 OBJ: 5 TOP: Health Promotion KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 17. A home health nurse is assisting a patient who is chronically ill with congestive heart failure to reorder time. What is the best intervention to assist this patient? a. Encouraging the patient to get up earlier or to go to sleep later b. Developing a daily schedule that allows time for activities, as well as for medical regimens c. Giving up time-consuming activities such as watching television or answering e-mail messages d. Encouraging the patient to complete only one task a day ANS: B Reordering time is developing a schedule that includes not only a medical regimen, but it also includes social and interpersonal activities, as well as hobbies. DIF: Cognitive Level: Application REF: p. 49 OBJ: 14 TOP: Reordering Time KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 18. What type of illness are the common cold, appendicitis, and urinary tract infections considered? a. Chronic b. Disabling c. Emergency d. Acute ANS: D An acute illness or disease is one that has a relatively rapid onset and a short duration. DIF: Cognitive Level: Comprehension REF: p. 42 OBJ: 1 TOP: Concept of Illness KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 19. What is the first step in helping patients to increase adaptability? a. Assess past methods of coping with stress. b. Suggest using past coping strategies. c. Determine external coping strategies. d. Determine what the patient perceives as stressful. ANS: A Nurses can help patients deal with stress by identifying the patient’s usual methods of coping or adapting. DIF: Cognitive Level: Knowledge REF: p. 43 OBJ: 10 TOP: Adaptation KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 20. How should a nurse describe a patient who has a functional interaction of the cognitive, affective, behavioral, and social dimensions of his personality? a. Effectively organized b. Personally satisfied c. Well rounded d. Mentally healthy ANS: D Mental health depends on the functional integration of the four dimensions of the personality. DIF: Cognitive Level: Comprehension REF: p. 41 OBJ: 1 TOP: Definition of Mental Health KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 21. A nurse assesses that a 42-year-old patient lives with her parents and is dependent on them for decisions about her life. Which mental health characteristic is this patient lacking? a. Reality orientation b. Autonomous behavior c. Spontaneity d. Ethical decision making ANS: B Autonomy is a mark of mental health. DIF: Cognitive Level: Comprehension REF: p. 41 OBJ: 1 TOP: Definition of Mental Health KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 22. What is an example of a positive stressor? a. Test anxiety b. Loss of a job c. Paying income tax d. Single motherhood ANS: A Test anxiety can be beneficial to promote study and sharpen focus. DIF: Cognitive Level: Knowledge REF: p. 43 OBJ: 7 TOP: Stress KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 23. Which action is an example of a person attempting to maintain homeostasis as a newcomer in a community? a. Joins a local church. b. Buys a new car. c. Stays in his or her apartment watching television. d. Spends hours writing e-mail messages to old friends. ANS: A The newcomer who attempts to balance the newcomer status with belonging is an example of homeostasis. DIF: Cognitive Level: Comprehension REF: p. 43 OBJ: 5 TOP: Homeostasis KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 24. Which behavior best exemplifies developmental activities in a 13-year-old teenager? a. Going out with a group of friends b. Reading an exciting book c. Volunteering for the local hospital d. Choosing a career ANS: A Interacting in peer relationships is a major developmental task of this age group. DIF: Cognitive Level: Comprehension REF: p. 44 OBJ: 3 TOP: Growth and Development KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 25. In which stage is introspection a major characteristic? a. Middle-aged adult b. Middle childhood c. Early adulthood d. Older-age adult ANS: D Introspection is properly identified as an activity of older age. DIF: Cognitive Level: Knowledge REF: p. 44 OBJ: 3 TOP: Growth and Development KEY: Nursing Process Step: N/A MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 26. A nurse hears a 5-year-old patient who just started kindergarten uses rude vocabulary. What is the best response to this behavior? a. Ignore it. b. Speak to his teacher about it. c. Praise him when he speaks properly. d. Talk about it at the parent–teachers association. ANS: C Learned behaviors can be unlearned with rewards for the desired behavior. DIF: Cognitive Level: Application REF: p. 44 OBJ: 14 TOP: Behavioral Theory KEY: Nursing Process Step: N/A MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 27. Which patient is most likely to experience the greatest cultural impact on his coping with a chronic debilitating illness? a. A 26-year-old Latino man with a family b. A 30-year-old divorced white man with no dependents c. A 35-year-old Asian wife with a family d. A 65-year-old widowed black church pastor with married children ANS: A The Latino man will have to deal with the loss of his culturally expected role as the head of the household. DIF: Cognitive Level: Analysis REF: p. 44 OBJ: 9 TOP: Coping with Illness KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 28. A patient with low back pain confesses that he drinks heavily each night to help him sleep and control pain. What does this behavior exemplify? a. Alternate pain control methods b. Coping with a chronic condition c. Using a social coping mechanism d. Using a maladaptive coping method ANS: D This behavior is an example of maladaptive coping. Drinking is not an appropriate means of coping with chronic pain. DIF: Cognitive Level: Application REF: p. 46|p. 49 OBJ: 9 | 13 TOP: Coping with Illness KEY: Nursing Process Step: N/A MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 29. What information should a nurse provide to a Native American patient taking herbal remedies and nutritional supplements? a. Herbs and vitamins are not helpful. b. If herbs and vitamins are not harmful, then they will be integrated into the plan of care. c. Medical research has shown that such alternative remedies are a waste of money. d. In the hospital, no physician will prescribe anything other than accepted medical protocols. ANS: B Care planning for individuals with different cultural beliefs requires respect and individualization. DIF: Cognitive Level: Application REF: p. 44 OBJ: 10 TOP: Cultural Beliefs KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 30. When a patient is given a diagnosis of cancer, his first statement is, “What did I ever do to deserve God punishing me?” What does this exemplify? a. Maladaptive coping b. Behavioral emotionalism c. Spiritual distress d. Spiritual maladaptation ANS: C This is a response to spiritual distress. The patient is questioning the meaning of illness and suffering. DIF: Cognitive Level: Comprehension REF: p. 45 OBJ: 10 TOP: Spirituality KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 31. A star quarterback on the high school football team is injured in a motorcycle accident. He will be unable to play football again. Which patient problem is most appropriate when planning care specific to coping? a. Immobility b. Impaired self-concept c. Decreased socialization d. Inadequate comfort ANS: B Athletes who sustain injuries can have impaired self-concept related to their altered body image. DIF: Cognitive Level: Application REF: p. 45 OBJ: 11 TOP: Self-Concept KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 32. A wife of a critically injured husband has been at his bedside constantly for 2 days. As the nurse speaks to the wife, the wife sobs, “This is awful. I can’t take it anymore.” What is the wife experiencing? a. Fear b. Denial c. Compensation d. Stress ANS: D Long-term stress causes fatigue and an inability to solve problems. DIF: Cognitive Level: Application REF: p. 45 OBJ: 8 | 9 TOP: Emotions: Stress KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 33. How does fear differ from anxiety? a. Fear is a useless emotion. b. Fear is an ineffective coping strategy. c. Fear is an irrational feeling. d. Fear is a response to a specific threat. ANS: D Fear is a response to a specific threat (e.g., a rattlesnake in the garden); anxiety is a response to a nonspecific threat (e.g., first day on a new job). DIF: Cognitive Level: Comprehension REF: p. 45 OBJ: 10 TOP: Emotions: Anxiety and Fear KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 34. An older Italian woman has an egg yolk in a bowl under her bed that she believes is absorbing the evil of her illness and making her feel better. Which action should a nurse implement? a. Move the egg yolk out of the way to the bathroom. b. Replace the egg yolk with a hard-boiled egg. c. Remove the egg for sanitary purposes. d. Include maintenance of the egg in the nursing care plan. ANS: D A nursing approach should help with coping, not increase the stress. DIF: Cognitive Level: Application REF: p. 44 OBJ: 11 TOP: Cultural Concepts KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 35. When a 25-year-old woman who had a hysterectomy 1 day earlier tearfully tells the nurse that she is grieving for the children she will never have, the nurse assesses the grief as positive. What does grief allow this patient to achieve? a. Focus on her loss. b. Forget about her concern. c. Reappraise her values for the future. d. Depend on others for grief support. ANS: C Grief and mourning signify an end to something. After the mourning, the patient is free to reappraise values for the future. DIF: Cognitive Level: Comprehension REF: p. 46 OBJ: 10 TOP: Perceived Loss and Grief KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 36. A 5-year-old patient was in an accident in which his cousin was killed. The patient starts to wet the bed at night. What question should the nurse ask the mother when she confirms that it has been several years since the patient had any difficulty with bedwetting? a. “Do you think this is related to the accident?” b. “Do others in the family have this problem?” c. “Does your child drink lots of fluids late at night?” d. “Are there any stressful situations in your family?” ANS: A Anxiety is the root of such defense mechanisms as regression. This behavior is an example of regression, in which the 5-year-old child has gone back to behavior more suited to a younger developmental age. DIF: Cognitive Level: Application REF: p. 47 OBJ: 10 TOP: Defense Mechanisms KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 37. A 24-year-old man scheduled for brain surgery in the morning constantly listens to music with his headphones on. What should a nurse recognize this behavior as? a. Conversion reaction b. Conscious coping strategy c. Defense mechanism of undoing d. Reaction formation ANS: B The use of a conscious coping strategy can help decrease stress. DIF: Cognitive Level: Comprehension REF: pp. 47-48 OBJ: 11 TOP: Conscious Coping Strategies KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 38. When a patient is asked whether he wants his pain medication, he says to you, “I don’t know; whatever you think is best.” What should the nurse recognize this maladaptive coping mechanism as? a. Powerlessness b. Helplessness c. Denial d. Depression ANS: A The patient feels that he has lost control of his situation and has started to defer decisions about his care to others. DIF: Cognitive Level: Application REF: p. 49 OBJ: 13 TOP: Maladaptive Coping Mechanisms KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 39. Which patient diagnosis and behavior should lead a nurse to conclude the patient is using the defense mechanism of denial? a. A patient with emphysema continues to smoke. b. A patient with diabetes mellitus uses a sugar substitute. c. A patient with a drug problem blames his mother for his habit. d. A patient with osteoarthritis angrily kicks the steps that he cannot climb. ANS: A The patient with emphysema is an example of denial, the patient with diabetes is an example of an adaptive response, the patient with a drug problem is an example of projection, and the patient with osteoarthritis is an example of regression. DIF: Cognitive Level: Comprehension REF: p. 49 OBJ: 13 TOP: Maladaptive Coping KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 40. What is the goal of nursing care for the patient with a chronic illness? a. Find the cause of the illness. b. Tell the patient that he or she will learn to live with the illness. c. Help the patient manage the illness. d. Give the patient websites that have information about the illness. ANS: C The goal of caring for patients with a chronic illness is to help them manage the illness and to develop coping skills. DIF: Cognitive Level: Comprehension REF: p. 42|p. 49|p. 50 OBJ: 14 TOP: Nursing Goals KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 41. What nursing action should be implemented when dealing with a patient who is an alcoholic in denial and claims to only drink in social situations? a. Insist that he stop drinking entirely. b. Point out that the patient is using denial. c. Help the patient investigate ways to reduce drinking. d. Provide information on Alcoholics Anonymous. ANS: C In dealing with patients in denial, the nurse may have to accept the denial while still getting cooperation. DIF: Cognitive Level: Application REF: p. 49 OBJ: 13 TOP: Denial KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation MULTIPLE RESPONSE 1. How can a nurse assist when a caregiver is frustrated and is complaining of being overwhelmed? (Select all that apply.) a. Taking over the care b. Referring the caregiver to a support group c. Seeking assistance from a home health agency d. Listening to the caregiver’s concerns e. Assisting in making a daily schedule for the caregiver to follow ANS: B, C, D, E Taking over the care is not a permanent solution. Seeking a helpful support group, listening, seeking assistance from a home health agency, and making a daily schedule to help the caregiver identify duties that can be put aside are all helpful in coping with stress. DIF: Cognitive Level: Application REF: pp. 42-45 OBJ: 14 TOP: Coping with Stress KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 2. What should the nurse explain as reasons why a person who is ill should be allowed to adopt the “sick role.” (Select all that apply.) a. Exempt from usual roles b. Seeking attention c. Expected to get well d. Actively seeking remedy e. Using illness as excuse for failure ANS: A, C, D The sick role allows the patient the time to recover by exempting him or her from the usual obligations with the expectation that the patient will seek remedy and recover. DIF: Cognitive Level: Comprehension REF: p. 42 OBJ: 9 TOP: Sick Role KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 3. What factors are known to influence coping strategies? (Select all that apply.) a. Age b. Financial status c. Role expectations d. Personal values e. Cultural expectations ANS: A, C, D, E Financial status is not a basic part of building coping strategies. All the other options, however, play integral parts in the patient’s ability to cope or design new coping strategies or both. DIF: Cognitive Level: Knowledge REF: pp. 47-50 OBJ: 11 TOP: Coping Strategies KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 4. What should a nurse evaluate to assess the social dimension of a patient’s persona? (Select all that apply.) a. Interaction with family b. Formulation of thoughts c. Presentation of self to community d. Problem solving e. Processing of information ANS: A, C Interacting with family and presenting oneself to the community are elements of the social component. The other options belong to the element of the cognitive component. DIF: Cognitive Level: Application REF: p. 40 OBJ: 1 TOP: Aspects of Personality KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 5. What are characteristics of a healthy person according to Maslow? (Select all that apply.) a. Acceptance of self b. Reality orientation c. Spontaneity d. Effective problem-solving skills e. No need for privacy ANS: A, B, C, D Mentally healthy people require some element of privacy. All other options are characteristics of self-actualization. DIF: Cognitive Level: Knowledge REF: p. 41 OBJ: 1 TOP: Characteristics of Mental Health KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Growth and Development COMPLETION 1. A tendency of biologic systems to maintain stability of the internal environment while continually adjusting to changes is . ANS: homeostasis The term is derived from Greek and describes the tendency of the body to maintain stability. DIF: Cognitive Level: Knowledge REF: p. 43 OBJ: 5 TOP: Homeostasis KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. The term that a nurse uses to refer to persons who fail to maintain treatment protocols is . ANS: nonadherence Nonadherence is a term that describes the patient who fails to maintain treatment protocols. The term is less negative than the earlier term, noncompliant. DIF: Cognitive Level: Knowledge REF: p. 42 OBJ: 6 TOP: No Adherence KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 3. A student nurse who was terrified of giving an injection now gives many injections every shift. The change in the nurse is the result of . ANS: adaptation Adaptation refers to a person’s efforts to respond to stressors in such a way as to overcome the stress. DIF: Cognitive Level: Comprehension REF: p. 43 OBJ: 5 TOP: Adaptation KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 4. A nurse recognizes that mild stress can be a positive force that stimulates the patient to a problem. ANS: solve Mild stress can cause a person to focus and be able to solve a problem. DIF: Cognitive Level: Comprehension REF: p. 43 OBJ: 2 TOP: Mild Stress KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation Chapter 05: Immunity, Inflammation, and Infection Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient in early labor says to the nurse, “I will pass on protection from diseases, and the baby will not ever need any shots.” What is the best response by the nurse? a. “Babies are born with innate (natural) immunity at birth.” b. “Babies are born with immunoglobulin E (IgE), an antibody that crosses the placenta, but it only briefly protects the baby.” c. “Yes, immediate antibody immunity from the mother is the first line of defense against disease for babies.” d. “Yes, the mother passes on cell-mediated immunity.” ANS: B Infants acquire antibodies from the mother, but they only last a few months. DIF: Cognitive Level: Application REF: p. 58 OBJ: 4 TOP: Newborn Immunity KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A school nurse starts a clean-up campaign at a local elementary school in an effort to combat allergens. What is the most common allergic response disorder? a. Anaphylaxis b. Asthma c. Contact dermatitis d. Urticaria ANS: B Fungi are principle allergens that can trigger respiratory allergic responses such as asthma. DIF: Cognitive Level: Knowledge REF: p. 77 OBJ: 18 TOP: Reduction of Allergens KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A nurse is discussing the body’s first and second lines of defense against infection with a community group. What does the body’s first line of defense include? a. Teeth b. Sweat c. White blood cells d. T lymphocytes ANS: B The sweat glands excrete an antimicrobial enzyme. DIF: Cognitive Level: Knowledge REF: p. 56 OBJ: 1 TOP: Lines of Defense KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A nurse explains that a medication given to a patient with a severe inflammatory response mimics a hormone secreted by the adrenal cortex. To what hormone is the nurse referring? a. Aldosterone b. Testosterone c. Histamine d. Cortisol ANS: D Cortisol slows the release of antihistamine and stabilizes lysosomal membranes. DIF: Cognitive Level: Knowledge REF: p. 59 OBJ: 5 TOP: Anti-inflammatory Agents KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. With the exposure to an antigen, a nurse explains that the initiator of the inflammatory response is the presence of histamine. What is responsible for releasing histamine? a. Neutrophils b. Eosinophils c. Basophils d. Monocytes ANS: C Basophils release histamine. DIF: Cognitive Level: Knowledge REF: p. 57 OBJ: 5 TOP: Inflammatory Response KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A nurse is bathing a patient who is immunodeficient and has a Cryptococcus infestation. What is the classification of this organism? a. Bacterium b. Virus c. Fungus d. Protozoa ANS: C Cryptococcus fungal infections can be life threatening. DIF: Cognitive Level: Knowledge REF: p. 62 OBJ: 9 TOP: Fungi KEY: Nursing Process Step: Knowledge MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. A mosquito or a fly carries an organism that infects another living organism. What is this mode of transmission of infection? a. Common vehicle b. Direct excretion c. Ingestion d. Vector ANS: D Vector-borne diseases are carried from one host to another. Part of the life cycle of the pathogen occurs in the body of the fly, mosquito, or tick. DIF: Cognitive Level: Comprehension REF: p. 63 OBJ: 10 TOP: Vector Transmission KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 8. What is the most effective method to control the spread of communicable disease? a. Isolate the infected person from all contact with noninfected persons. b. Vigorously petition the community health department to increase spraying. c. Administer prophylactic antibiotics to the rest of the family. d. Demonstrate and monitor a return demonstration of a good hand washing technique by the family. ANS: D Good hand washing is the cornerstone of infection control. DIF: Cognitive Level: Comprehension REF: p. 69 OBJ: 13 TOP: Prevention of the Spread of Infection KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 9. An air conditioner duct cleaning is recommended by a home health nurse. What should this precaution prevent the spread of in the patient’s home? a. Bacteria b. Viruses c. Fungi d. Protozoa ANS: C Air blowing into a room may be the mode of transfer of fungi spores that have remained dormant in the duct during nonuse. DIF: Cognitive Level: Knowledge REF: p. 73 OBJ: 10 TOP: Infectious Disease Transmission in the Home KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. A school nurse cautions a group of parents about children playing barefoot on dirt. To what infectious agents can this action expose the children? a. Helminthes b. Protozoa c. Rickettsiae d. Mycoplasmas ANS: A Worms in the dirt seek entry through the foot skin and into the blood circulation, where they are carried to the lungs; coughed up into the mouth; and swallowed into the gastrointestinal tract, where they cause serious infections. Barefooted children who do not have proper hygiene are at risk for these worm infections. DIF: Cognitive Level: Comprehension REF: p. 62 OBJ: 10 TOP: Helminth Transmission KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. A large, heavy, and older adult patient has a stroke and develops an infected decubitus ulcer on the sacrum during the hospital stay. Approximately 2 weeks after the patient has gone home, the patient returns to the hospital with pneumonia. What is the distinction between these two infections? a. The decubitus ulcer infection was transmitted from other patients on the unit, but the pneumonia was transmitted from a neighbor visiting when the patient was at home. b. The decubitus ulcer and pneumonia are caused by the same host. c. The decubitus ulcer is termed a health care–associated infection, and pneumonia is termed a community-acquired infection. d. The decubitus ulcer is considered to be caused by protozoa, but the pneumonia is considered unpreventable because of the size of the patient. ANS: C Because the decubitus ulcer developed during the stay in a health care facility, it is classified as a health care–associated infection. Because the patient did not have pneumonia when he left the facility, it is classified as a community-acquired infection. DIF: Cognitive Level: Comprehension REF: p. 64|p. 66 OBJ: 12 TOP: Community-Acquired versus Health Care–Associated Infections KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 12. On a visit to administer the fifth in a series of 10 antibiotic doses, a home health nurse is told that the patient is now complaining about a bothersome vaginal discharge. The nurse communicates the problem and arranges for medication. What is the most likely cause of the vaginal discharge? a. Poor genital hygiene—not changing underwear often enough b. Allergy to the soap or soap products used in the genital area c. Superinfection response to the antibiotic medication d. Sexual contact with another infected person ANS: C Antibiotics frequently wipe out good bacteria and cause other bacteria to overgrow, causing vaginitis. DIF: Cognitive Level: Comprehension REF: p. 67 OBJ: 12 TOP: Superimposed Infections KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 13. Which patient diagnosis is most likely related to acquiring a health care–associated infection? a. Abdominal abscess after a ruptured appendix b. Lice and nits that have come from the emergency department c. Urinary infection after the insertion of a Foley catheter d. Two-day, postoperative foot fungus after a hip replacement ANS: C Iatrogenic or health care–associated infections are those acquired during the hospital stay. Urinary catheters are frequently the source of such infections. Abscesses frequently follow a ruptured appendix; lice and athlete’s foot are long-term conditions not caused by hospital interventions. DIF: Cognitive Level: Application REF: p. 67 OBJ: 12 TOP: Iatrogenic Infections KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 14. A community picnic is held. A number of the attendees become ill after the picnic. How was the pathogen acquired? a. Indirect contact b. Common vehicle c. Airborne transmission d. Vector transmission ANS: B Food at the picnic that was shared in common became the vehicle for transmission. DIF: Cognitive Level: Comprehension REF: p. 63 OBJ: 10 TOP: Common Vehicle Transmission KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 15. A nurse caring for a patient who is immunosuppressed is diligent about protecting the patient from infection. When visitors come in, in addition to having them put on isolation attire, what should the nurse also prohibit? a. Battery-operated DVD player b. Book c. Potted plant d. Box of candy ANS: C The soil in the flowerpot is a reservoir for bacteria and fungi. DIF: Cognitive Level: Application REF: p. 73|p. 77 OBJ: 16 | 18 TOP: Reverse Isolation for Immunosuppressed Patient KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 16. A nurse explains that although some drugs reduce inflammation, they also hinder the body’s immune response. What are examples of such drugs? a. Antihistamines and salicylates b. Bronchodilators and corticosteroids c. Cardiotonic and anticholinergics d. Diuretics and sedatives ANS: B The immune response is dampened by corticosteroids. DIF: Cognitive Level: Comprehension REF: p. 76 OBJ: 18 TOP: Pharmacologic Care for Allergies KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 17. A patient has had several increasingly severe allergic reactions during last year’s pollen season. This year, the patient comes regularly to the office to receive some antigen injections. What education will the nurse provide regarding these injections? a. They will combat infection brought on by the allergic response. b. They will act as a steroid to lessen the allergic response. c. They will increase tolerance to the antigen. d. They will decrease the production of the antibodies. ANS: C Injections of increasing amounts of minute doses of the antigen will desensitize the body against the antigen. DIF: Cognitive Level: Application REF: p. 76 OBJ: 18 TOP: Long-Term Pharmacologic Treatment of Allergies KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 18. A patient who is receiving daily steroids for the control of a condition calls the nurse to ask advice about whether a small child who has been exposed to influenza should come and visit because she has not had any symptoms. What is the most appropriate response by the office nurse? a. “Yes, let the child visit. There is no reason not to visit because this child is not sick.” b. “No, the child should not visit. Infectious diseases are often most communicable in the short period before the child actually becomes ill.” c. “It would be up to the patient. Plan not to get overtired with a small child running and bouncing around.” d. “Take the child who is not sick to her own physician and ask this question first.” ANS: B Children, especially those who have been exposed to a contagious disease but are not yet symptomatic, are still very contagious, especially to an immunocompromised patient. DIF: Cognitive Level: Application REF: pp. 63-64 OBJ: 10 TOP: Contagious Infections KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 19. A patient with the diagnosis of Clostridium difficile infection asks what has caused the diarrhea. What is the best response by the nurse? a. It is caused by a protozoal infection. b. It is caused by a fecal–oral contamination. c. It is caused by an inflammatory response. d. It is caused by a long-term antibiotic therapy. ANS: D Superinfections such as Clostridium difficile infections are caused by long-term antibiotic therapy, which kills all the natural flora of the bowel and causes diarrhea. DIF: Cognitive Level: Comprehension REF: p. 67 OBJ: 10 TOP: Superinfection KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 20. A patient receiving a large intramuscular dose of antibiotic was asked to please wait 20 to 30 minutes before checking out. What is the reason for this request? a. The office staff needs to make sure that the right medicine was administered before the patient leaves. b. The nurse always forgets to ask the patient about allergies before administering the antibiotic. c. Antibiotics are a common source of severe allergic reactions within the first few minutes after an injection. d. The staff wants to make sure that the patient has time to pay for the services delivered that day. ANS: C Antibiotic administration is a common cause of anaphylaxis. The patient is asked to wait to allow medical personnel to reverse the condition should it occur within minutes after an injection. DIF: Cognitive Level: Comprehension REF: pp. 77-78 OBJ: 18 TOP: Antibiotic Anaphylaxis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 21. After receiving an injection of penicillin, a patient undergoes an anaphylactic reaction. What should the nurse do first? a. Administer oxygen. b. Prepare fluids to combat shock. c. Notify the charge nurse. d. Cover with several blankets. ANS: A The first intervention should be to supply oxygen. Notification of the charge nurse and the administration of fluids to combat hypovolemia will come afterward. Covering with blankets would increase the vasodilation and increase the shock. DIF: Cognitive Level: Application REF: p. 78 OBJ: 18 TOP: Anaphylaxis Assessment and Intervention KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 22. The Centers for Disease Control and Prevention (CDC) has issued new guidelines for infection control. Nursing care plans for patients with infection should mainly address which protocol? a. Disease-specific precautions b. Manner in which clean gloves are worn c. Standard Precautions guidelines d. Placement of needles and sharps ANS: C The CDC has issued new guidelines for Standard Precautions for infection control. These cover disease-specific precautions, the manner in which clean gloves are worn, and the placement of needles and sharps. Only the Standard Precautions guidelines are all inclusive. DIF: Cognitive Level: Comprehension REF: p. 69 OBJ: 14 TOP: Centers for Disease Control and Prevention: Multiple Guidelines for Standard Precautions KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 23. Which vitamin can enhance wound healing? a. A b. B c. C d. D ANS: C The addition of vitamin C and zinc to the medication regimen can hasten wound healing. DIF: Cognitive Level: Knowledge REF: p. 75 OBJ: 7 TOP: Wound Healing KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 24. A patient is hospitalized with cryptococcal pneumonia and AIDS. What is the most important Standard Precaution for the health care team to implement? a. Hands are washed before and after gloving. b. After gloves are put on, they do not need to be changed until care is finished. c. Needles and sharps should be placed in puncture-resistant containers on the medicine cart out of the room. d. Mouth-to-mouth resuscitation must be performed immediately unless the patient is a designated as “do not resuscitate.” ANS: A Hand washing is necessary before and between care in areas of contamination. DIF: Cognitive Level: Application REF: p. 69 OBJ: 14 TOP: Standard Precautions KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 25. The organs involved in immunity include the tonsils, spleen, and lymph nodes. What other organ is involved in immunity? a. Liver b. Lungs c. Periosteum d. Pancreas ANS: A The liver filters the blood and plays a part in the immune response by the production of globulins and other chemicals involved in the immune response. DIF: Cognitive Level: Knowledge REF: p. 58 OBJ: 3 TOP: Organs Involved in Immune Response KEY: Nursing Process Step: N/A MSC: NCLEX: Physiological Integrity 26. What is required by medical asepsis that is not required by surgical asepsis? a. Good hand washing technique b. That no nonsterile product comes into contact with the patient c. Elimination of all microorganisms d. Hand washing with antimicrobial soap for 3 minutes ANS: A Surgical asepsis is sterile technique. Medical asepsis is considered a clean technique. DIF: Cognitive Level: Comprehension REF: pp. 67-69 OBJ: 14 TOP: Difference between Medical and Surgical Asepsis KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 27. The daughter of an 89-year-old resident in a long-term care facility asks if she may give her father an over-the-counter (OTC) antihistamine that she uses for seasonal allergy. What is the nurse’s most appropriate response? a. “Yes. OTCs are mild and very helpful.” b. “No. Many antihistamines cause confusion in the older adult.” c. “Yes. The drug might energize him so he won’t be so drowsy.” d. “No. Allergic symptoms should be allowed to run their course.” ANS: B Many antihistamines cause the older adult to become confused. These drugs also cause drowsiness, and many OTC drugs are not mild. DIF: Cognitive Level: Application REF: p. 77 OBJ: 18 TOP: Antihistamines KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies MULTIPLE RESPONSE 1. What occurrences of disease is the school nurse required to report to the health department? (Select all that apply.) a. Rubella b. Lyme disease c. Pediculosis d. Salmonella e. Clostridium difficile ANS: A, B, D Rubella, Lyme disease, and Salmonella must all be reported. Lice and Clostridium difficile do not need to be reported. DIF: Cognitive Level: Application REF: p. 65 OBJ: 12 TOP: Reportable Communicable Diseases KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control COMPLETION 1. A nurse assesses a high eosinophil count in a pediatric patient. The nurse recognizes that this elevation is an indicator of . ANS: allergy High eosinophil counts are indicators of an allergic response. DIF: Cognitive Level: Comprehension REF: p. 57 OBJ: 18 TOP: Allergy Indicators KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. Persons with human immunodeficiency virus (HIV) have acquired Pneumocystis jiroveci (PCP), a serious pulmonary infection caused by . ANS: protozoa Protozoa cause the opportunistic pulmonary infection of PCP. DIF: Cognitive Level: Knowledge REF: p. 62 OBJ: 9 TOP: Pneumocystis jiroveciKEY: Nursing Process Step: N/A MSC: NCLEX: N/A 3. A nurse reminds the patient who is to undergo hyperbaric oxygen therapy that the clothing worn into the chamber must be made of . ANS: cotton Cotton clothing is worn in the hyperbaric chamber to reduce the threat of fire. Synthetic materials can cause a spark of static electricity. DIF: Cognitive Level: Knowledge REF: p. 75 OBJ: 13 TOP: Clothing in Hyperbaric Chamber KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 4. Prioritize the events of an antibody-mediated immunity response. (Place the events in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Antibodies seek out and bind with specific antigen. b. Antigen binds to a B lymphocyte. c. Circulating antibody–antigen complexes are destroyed. d. Antibodies are produced. e. Antibodies are replenished. ANS: BDACE Antigen binds to a B lymphocyte, and antibodies are produced for that specific antigen. Antibodies seek out and bind with the specific antigen when it is reintroduced to the organism and bind with them. These circulating antigen–antibody complexes are targeted and destroyed by phagocytes. Antibodies are continually replenished in most cases. DIF: Cognitive Level: Analysis REF: pp. 58-59 OBJ: 2 TOP: Antibody-Mediated Immunity KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 06: Fluid, Electrolyte, and Acid–Base Imbalance Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse assesses that a patient’s urine has become much more concentrated. What is the most likely cause for the change? a. Adrenaline b. Aldosterone c. Antidiuretic hormone (ADH) d. Insulin ANS: B Aldosterone acts on the kidney tubules, affecting water retention and its attendant urine concentration. DIF: Cognitive Level: Comprehension REF: p. 85 OBJ: 6 TOP: Urine Concentration KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. When the water absorption in the renal tubules becomes greater than normal, what assessment finding should a nurse anticipate? a. More concentrated urine b. Less concentrated urine c. More alkaline urine d. Less alkaline urine ANS: A When more water is kept back in the body, the water left to form urine is less; therefore, the urine is more concentrated. DIF: Cognitive Level: Analysis REF: p. 85 OBJ: 6 TOP: Water Reabsorption by Kidney KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. What process occurs when oxygen is directed out of the arteries and into the capillaries? a. Active transport b. Diffusion c. Filtration d. Osmosis ANS: B Diffusion is the movement from areas of higher concentration to areas of lower concentration. DIF: Cognitive Level: Knowledge REF: p. 84 OBJ: 2 TOP: Fluid Movements between Portions of the Circulatory System KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A patient’s intravenous (IV) injection has been infusing at a very high rate. What assessment indicates fluid volume overload in this patient? a. Hypotension b. Tachycardia c. Pulmonary edema d. Kidney failure ANS: C An IV infusing at a high rate is used to increase intravascular fluid volume, but there is an equalization level, after which the patient goes into fluid overload; this results in pulmonary edema. DIF: Cognitive Level: Application REF: p. 87 OBJ: 4 TOP: Fluid Overload KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. A small child is hospitalized with severe metabolic acidosis after ingesting a whole bottle of baby aspirin approximately 8 hours earlier. In addition to providing reassurance to the patient, which nursing action is the most appropriate? a. Providing IV treatments as ordered but without sodium bicarbonate b. Frequently assessing the mental and neurologic status c. Taking daily weights and vital signs d. Inducing vomiting ANS: B The baby aspirin was ingested too long ago to have vomiting or stomach aspiration be of any use. The child requires frequent assessment of neurologic function because the child may need mechanical ventilation. DIF: Cognitive Level: Application REF: pp. 98-99 OBJ: 8 TOP: Metabolic Acidosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. What is primarily responsible for carrying fluids with nutrients and wastes on a random basis throughout the body? a. Filtrates b. Extracellular fluid c. Intracellular fluid d. Osmolytes ANS: B The blood and lymph are the main media for transporting nutrients and wastes in the body. DIF: Cognitive Level: Knowledge REF: p. 82 OBJ: 3 TOP: Fluid Transportation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A nurse clarifies that electrolytes, such as sodium and potassium (K+), break down into smaller particles when dissolved. What are these smaller particles? a. Cells b. Elements c. Ions d. Molecules ANS: C Electrolytes dissolved in water are called ions. DIF: Cognitive Level: Knowledge REF: p. 83 OBJ: 2 TOP: Ions KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. A nurse assists a patient with dyspnea to sit in a high Fowler position. What process allows gravity to help move oxygen from the pulmonary capillaries into the blood when the patient is in this position? a. Active transport b. Diffusion c. Filtration d. Osmosis ANS: B The Fowler position increases blood flow through the lungs and therefore facilitates better oxygen diffusion. DIF: Cognitive Level: Comprehension REF: p. 84 OBJ: 3 TOP: Movement of Oxygen in the Body KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. A nurse evaluates the laboratory reports on electrolyte values carefully to assess the balance between positive and negative ions. What is responsible for the regulation of this process? a. Adaptation b. Diffusion c. Homeostasis d. Osmosis ANS: B Diffusion allows the ions to support homeostatic balance. DIF: Cognitive Level: Knowledge REF: p. 84 OBJ: 3 TOP: Electrolyte Values KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. What is being administered when a nurse hangs an IV bag with Na+, K+, and Cl–? a. Nutrients b. Electrolytes c. Enzymes d. Vitamins ANS: B Sodium, K+, and chlorides are electrolytes. DIF: Cognitive Level: Knowledge REF: p. 83 OBJ: 2 TOP: Electrolyte Administration KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. Each compartment of the body has a water-fluid distribution movement of its own. What is the process allowing these fluids to move and distribute themselves among compartments? a. Active transport b. Diffusion c. Filtration d. Osmosis ANS: D The intracellular and extracellular compartments contain water and dissolved substances. The water filters back and forth as needed to maintain homeostasis via osmolarity. DIF: Cognitive Level: Knowledge REF: p. 84 OBJ: 3 TOP: Water Distribution and Movement KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 12. A licensed practical/vocational nurse (LPN/LVN) is preparing to add a new IV of 5% dextrose in water (D5W) with potassium (K+) to an existing line. The LPN/LVN notices that only 25 mL of urine has been collected over the past hour. What is the most appropriate nursing intervention? a. Avoid hanging the IV with K+ and inform the registered nurse (RN) of the urine output. b. Run the IV rapidly for 30 minutes to stimulate urine production. c. Call the physician who ordered the K+. d. Hang the IV as ordered and chart the output. ANS: A The low urine output will allow K+ to build up to a hazardous level. K+ administration is dependent on adequate urine output. LVN/LPNs are required to report problematic findings to an RN. DIF: Cognitive Level: Analysis REF: p. 96 OBJ: 8 TOP: K+ Administration KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 13. Both the intracellular and extracellular fluids are made up of many different electrolytes. What is the most abundant intracellular positively charged electrolyte? a. Calcium b. Chloride c. Potassium d. Sodium ANS: C K+ is the most abundant electrolyte in the cell. DIF: Cognitive Level: Knowledge REF: p. 83 OBJ: 5 TOP: Electrolytes KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 14. For what compensatory condition should the nurse carefully assess when the patient with metabolic acidosis is hyperventilating? a. Metabolic alkalosis b. Respiratory acidosis c. Respiratory alkalosis d. Thyroid imbalances ANS: C When in metabolic acidosis, the body attempts to compensate by increasing respirations and creating respiratory alkalosis. DIF: Cognitive Level: Application REF: p. 96 OBJ: 11 TOP: Acidosis and Compensatory Alkalosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 15. The K+ laboratory report shows a level of 5.2 mEq/L. What is the most important assessment for the nurse to make? a. Excessive thirst b. Irregular heartbeat c. Swelling of ankles d. Frightening hallucinations ANS: B Arrhythmias can be triggered by hyperkalemia. DIF: Cognitive Level: Comprehension REF: p. 96 OBJ: 8 TOP: Hyperkalemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 16. A patient has renal damage because of diabetes. What is the highest risk for this patient? a. Hypercalcemia b. Hypocalcemia c. Hyperkalemia d. Hypokalemia ANS: C When the renal system cannot rid the body of enough K+, this electrolyte builds up and a condition called hyperkalemia develops. DIF: Cognitive Level: Analysis REF: p. 96 OBJ: 6 TOP: Kidney Damage Limiting Excretion of Potassium KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 17. What is usually associated with hyperchloremia? a. Metabolic acidosis b. Metabolic alkalosis c. Respiratory acidosis d. Respiratory alkalosis ANS: A Chlorides bind with positively charged ions such as K+ in the patient with metabolic acidosis. DIF: Cognitive Level: Comprehension REF: p. 96 OBJ: 6 TOP: Hyperchloremia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 18. Older adults are at risk for dehydration because of reduced thirst and aging kidneys. What should the nurse assess as an early indicator of dehydration? a. Reduced skin turgor b. Constipation c. Concentrated urine d. Disorientation ANS: B Because older adults have poor skin turgor and urine concentration is difficult to assess, constipation is the earliest indicator of a fluid deficit. DIF: Cognitive Level: Application REF: p. 86 OBJ: 9 TOP: Fluid Loss in Older Adults KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 19. A nurse has two newly admitted patients with dehydration. One patient is dehydrated from heat exhaustion, and the other is dehydrated from an overdose of Lasix. What finding should be present in both patients? a. Increased skin turgor b. Decreased pulse and respirations c. Copious saliva and nasal secretions d. Increased laboratory values of hemoglobin and hematocrit ANS: D Water has been lost; therefore, the red blood cells will concentrate and show artificially high values of hemoglobin and hematocrit. DIF: Cognitive Level: Analysis REF: p. 92 OBJ: 4 TOP: Dehydration Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 20. A nurse understands that fluid balance is mainly monitored in the body by which two systems? a. Circulatory and renal b. Respiratory and circulatory c. Renal and gastrointestinal d. Hepatic and lymphatic ANS: A The monitoring of basic fluid balance in the body is performed by the renal and circulatory systems. DIF: Cognitive Level: Knowledge REF: p. 85 OBJ: 3 TOP: Fluid Balance KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 21. What primarily maintains extracellular fluid osmolarity? a. Chloride b. Magnesium c. Potassium d. Sodium ANS: D Sodium, as the primary extracellular electrolyte, controls the osmolarity (either too much or too little) of the extracellular fluid. DIF: Cognitive Level: Comprehension REF: p. 85 OBJ: 5 TOP: Extracellular Fluid Osmolarity KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 22. How does the healthy kidney adjust the volume and composition of filtrate that prevents excessive fluid loss? a. Active transport b. Filtration in the lymphatic system c. Secretion of adrenalin d. Tubular reabsorption ANS: D The kidney reabsorbs water and other electrolytes in response to chemical receptors. DIF: Cognitive Level: Comprehension REF: p. 85 OBJ: 3 TOP: Renal Physiology KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 23. What process involves blood being brought by the incoming capillaries into the kidney, which contains nitrogenous substances to be excreted as waste? a. Active transport b. Diffusion c. Filtration d. Osmosis ANS: C Capillary blood from the renal arteries filters into the kidney for processing as the first step. DIF: Cognitive Level: Knowledge REF: p. 84 OBJ: 3 TOP: Kidney Filtration KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 24. What should treatment focus on when a patient is hypovolemic? a. Extracellular fluid deficit and limiting drinking water b. Hypertonic intracellular deficit and limiting water intake c. Extracellular fluid deficit and encouraging fluid intake d. Circulatory system hormone deficit and limiting water intake ANS: C A fluid volume deficit occurs when the fluid volume in the body is inadequate; the nurse may encourage drinking fluids as a nursing action. DIF: Cognitive Level: Application REF: p. 91 OBJ: 8 TOP: Fluid Deficit KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 25. A patient is frequently thirsty. To what should the nurse attribute this symptom? a. Too much sodium and too much water in the body b. Too little sodium and too much water in the body c. Too much sodium and too little water in the body d. Too little sodium and too little water in the body ANS: C Normal thirst is the body’s way of calling for an increase in fluid volume, which could mean that the body is retaining too much sodium and too little water. DIF: Cognitive Level: Comprehension REF: p. 85 OBJ: 6 TOP: Thirst Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. What should a nurse instruct a patient with a K+ level of 6.2 to avoid? (Select all that apply.) a. Lima beans b. Bananas c. Carrots d. Tomatoes e. Celery ANS: B, C, D, E Banana, carrots, tomatoes, and celery are all high in K+ and should be avoided. Lima beans are low in K+. DIF: Cognitive Level: Application REF: p. 95 OBJ: 8 TOP: Foods High in K+ KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. A nurse assesses that a patient with congestive heart failure who is being treated with a diuretic has lost 4.4 lb in 1 day. This weight loss is equivalent to the loss of L of fluid. ANS: 2 1 L of fluid is equal to 2.2 lb. A weight loss of 4.4 lb is equal to 2 L. DIF: Cognitive Level: Analysis REF: pp. 87-88 OBJ: 4 TOP: Fluid Loss KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse assesses deep-rapid respirations in a patient with metabolic acidosis to be an indicator of the homeostatic system at work to reduce the level. (Do not abbreviate your answer.) ANS: carbon dioxide The lungs are primarily responsible for the regulation of CO2 by changing the rate and depth of respirations. DIF: Cognitive Level: Comprehension REF: p. 97 OBJ: 10 TOP: Metabolic Acidosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A nurse should anticipate in a patient with respiratory acidosis that the blood pH reading would be lower than . ANS: 7.3 The lowest normal value for blood pH is 7.35. Any value lower than 7.3 indicates acidosis. DIF: Cognitive Level: Application REF: p. 98 OBJ: 10 TOP: Respiratory Acidosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A nurse cautions a group of high school athletes about fluid loss in hot, dry weather, because the normal loss from respiration, which is 300 to mL/day, is doubled. ANS: 400 The normal fluid loss through evaporation is 300 to 400 mL a day. The fluid loss increases in hot, dry weather. DIF: Cognitive Level: Application REF: p. 86 OBJ: 3 TOP: Insensible Fluid Loss KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 07: The Patient with Cancer Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Which statement best defines concepts to be included in a teaching plan for a patient with cancer? a. Cancer is a group of diseases. The cancer cells are different from the cells in the tissue of its origin in both the growth and spreading of abnormal cells. b. Cancer is the third leading cause of death in the United States. Many hospitals have the highest number of patients with this diagnosis. c. Americans who have a diagnosis of cancer die within 1 year or less. d. When a person is genetically predisposed to a type of cancer, nothing can be done to prevent its occurrence. ANS: A Information about the disease and disease process is helpful to allay anxiety, as well as to instruct about its pathophysiologic changes. DIF: Cognitive Level: Comprehension REF: pp. 102-104 OBJ: 3 TOP: Morbidity and Mortality of Cancer KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse explains that the seven warning signs of cancer written by the American Cancer Society (ACS) can be recalled by the acronym CAUTION. What should the nurse change to point out that the A in the acronym represents? a. A sore that will not heal b. Alopecia c. Abscess d. Anorexia ANS: A The acronym is a change in bowel or bladder habits, a sore that will not heal, unusual bleeding or discharge, a thickening or lump in the breast or elsewhere, indigestion or difficulty swallowing, and a nagging cough or hoarseness. DIF: Cognitive Level: Knowledge REF: p. 106 OBJ: 4 TOP: Seven Danger Signs KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A home health nurse is compiling a patient profile on a 23-year-old obese woman who smokes one-half pack of cigarettes a day and drinks 1 beer a week. She works as a cook in a long-term care facility. She has two children and eats a diet high in fats. She exercises 30 minutes a day. Both parents are dead of heart disease. How many risk factors for cancer in this profile should the nurse identify? a. 2 b. 3 c. 5 d. 6 ANS: B Cancer risks identified are obesity, smoker, and high-fat diet. DIF: Cognitive Level: Comprehension REF: p. 103|p. 106 OBJ: 4 TOP: Cancer Risks KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. What phase is considered the latent period before the period of rapid growth of tumors? a. Initiation b. Promotion c. Progression d. Metastasis ANS: B The stage of promotion is the latest period in which a cell is quiet, just before the rapid growth and tumor production, which begins in the progression phase. DIF: Cognitive Level: Knowledge REF: p. 105 OBJ: 3 TOP: Transformation KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. Which is true about both malignant tumors and benign tumors? a. Both contain cells that closely resemble those in the tissue of origin. b. Both travel quickly to invade and destroy other tissues and organs. c. Both always grow and multiply very rapidly, competing for space and nutrients and causing severe pain. d. Both may press on nearby surrounding tissues, such as nerves and blood vessels, causing pain. ANS: D Both benign and malignant tumors may create pressure on or obstruct an organ. DIF: Cognitive Level: Comprehension REF: pp. 103-104 OBJ: 2 TOP: Characteristics of Benign and Malignant Cells KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A patient newly diagnosed with cancer says, “I feel like I’ve lost my future. I feel so much harm has been done to me that I’m overwhelmed.” To what type of coping strategies should the nurse recognize this attitude will most likely lead the patient? a. Avoidant b. Problem solving c. Approach oriented d. Confrontational ANS: A Persons who appraise their cancer diagnosis as harm or loss are more likely to use avoidant coping strategies. DIF: Cognitive Level: Comprehension REF: p. 121 OBJ: 6 TOP: Coping Styles KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 7. A patient has a cancer that has been TNM staged as T3 (1-4, size of primary tumor), N2 (0-3, degree of spread to regional lymph nodes), and M1 (0-1, presence of metastasis). He has an as needed order of 4 mg of morphine intramuscularly every 4 hours. He requests another pain injection approximately 3.5 hours after the last one. What is the most appropriate nursing action? a. Inform the patient that this narcotic may be given only every 4 hours to prevent addiction. b. Ignore the call bell for 20 minutes and then take at least 10 minutes to prepare and administer the injection. c. Give the morphine and evaluate the results of pain relief. Arrange for the physician to evaluate for breakthrough pain. d. Ask the family to assist in helping the patient accept waiting longer to receive an addicting medication such as morphine. ANS: C Terminal care does not include concerns about morphine addiction. Medication may be given slightly before the allotted time. The occurrence of breakthrough pain is a real concern for this patient. DIF: Cognitive Level: Application REF: p. 127 OBJ: 7 TOP: Nursing Care of the Terminal Patient in Pain KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. A patient is scheduled for a chemotherapy treatment in approximately 30 minutes. Breakfast trays have arrived and are being served on the unit. What is the nurse’s best intervention? a. Encourage the patient to eat all his breakfast to keep up his strength to fight the cancer. Remind the patient that breakfast is about one third of his daily intake. b. Listen attentively to any concerns that the patient expresses regarding the treatment. Offer to hold his tray until after the treatment. c. Offer to call the family to come and be present after the treatment. Encourage the patient to drink at least all of the orange juice and coffee. d. Suggest that the patient request a dose of strong analgesic instead of eating because this treatment is very painful. ANS: B Chemotherapy causes nausea and vomiting. Holding the tray until later provides for better intake and for holding the food in the stomach for digestion. DIF: Cognitive Level: Application REF: pp. 113-114 OBJ: 6 TOP: Care of the Patient Undergoing Chemotherapy Treatment KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. A nurse explains that drugs such as cannabinoids or Benadryl are frequently ordered for patients with cancer who are taking chemotherapy. What do these types of drugs accomplish? a. Promote amnesia to dampen the fear. b. Maintain fluid retention to prevent dehydration. c. Control nausea, vomiting, and taste disorders caused by the therapy. d. Control bouts of diarrhea or uncomfortable constipation. ANS: C Cannabinoids and antihistimines such as Benadryl are useful to help control nausea. DIF: Cognitive Level: Comprehension REF: p. 124 OBJ: 6 TOP: Drugs Commonly Ordered for Patients with Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 10. While bathing a patient with cancer, a nurse assessed several large new bruises on the patient’s upper arms and thighs. What is the best understanding of the possible causes and the correct nurse’s actions for these findings? a. The patient must have fallen last night walking to the bathroom. Teach the patient to use the call bell when assistance is needed. b. The patient may have disseminated intravascular coagulation. The size, shape, location, color, and tenderness must be reported and recorded fully. c. An intravascular fluid overload is occurring because of the chemotherapy. Place the patient on strict input/output (I/O) status and limit fluids. d. The patient must have had a drug-induced seizure, which caused arm and leg thrashing and the bruises. Report and record the findings, and pad the side rails. ANS: B These signs of hemorrhage may indicate the oncologic emergency of disseminated intravascular coagulation. Serious signs need to be reported in a timely manner and fully described. DIF: Cognitive Level: Comprehension | Cognitive Level: Application REF: p. 128 OBJ: 6 TOP: Oncologic Emergencies KEY: Nursing Process Step: Assessment| Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 11. What manifestations might be assessed by a nurse when a patient is diagnosed with the oncologic emergency hypercalcemia? a. Hypertension and bradycardia b. Fatigue, confusion, and weakness c. Laboratory test results of potassium 3.5 mEq/L, sodium 143 mEq/L d. Urine output less than 30 mL/hr ANS: B The indications for hypercalcemia are fatigue, confusion, weakness, and poor muscle tone. If left untreated, renal failure and death may occur. DIF: Cognitive Level: Comprehension REF: p. 128 OBJ: 6 TOP: Oncologic Emergencies KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. A female college student has had a melanoma of the forehead surgically removed and given a course of chemotherapy. Which comment demonstrates an understanding of the treatments and prognosis? a. “Why did you bring me this shampoo? You guys took all my hair, so I don’t have anything to wash or fix.” b. “Why don’t my friends from school come to visit? Did you tell them to stay away?” c. “My spring dance is only 3 weeks away. Do you think I could find a wig to cover my head where the hair fell out from the chemo?” d. “Well, this looks like the end of the problem for me, thank goodness! I won’t have to bother that doctor again until I graduate in a couple of years because all my shots must be up to date now.” ANS: C Acceptance of the diagnosis, treatments, side effects, and prognosis by the patient are reflected in her understanding that she will be bald. DIF: Cognitive Level: Comprehension REF: p. 116|p. 122 OBJ: 6 TOP: Understanding the Significance of the Treatments KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 13. A patient whose cancer has been staged at T4 N2 M1 has been assigned for care. What is the best interpretation of this staging information in planning care for this patient? a. The primary tumor has shrunk, although some lymph nodes remain involved. Teach the patient that this is good news. b. The primary tumor has now responded to a combination of chemotherapy and radiation. The patient should now receive much less analgesic medication. c. The primary tumor is quite large and has extended to lymph glands and distant areas. Gentle touch and therapeutic listening will be especially helpful. d. After the series of radiation treatments, the distant metastases are still present. Prepare the patient to accept only the cure of the primary tumor. ANS: C Correct interpretation and differentiating components of staging data are used to plan effective nursing care. DIF: Cognitive Level: Analysis REF: p. 106 OBJ: 7 TOP: Tumor Staging Used to Plan Care KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. Which symptom reported by a patient taking doxorubicin (Adriamycin) should be considered a priority for intervention? a. Nausea b. Visual disturbances c. Headache and dizziness d. Rapid heartbeat ANS: D Adriamycin is cardiotoxic medication and can cause heart failure. DIF: Cognitive Level: Application REF: p. 123 OBJ: 6 TOP: Complication of Doxorubicin (Adriamycin) KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 15. A diagnosis of breast cancer is first made at stage T1 N0 M0. Which patient problem would be appropriate? a. “Altered body image, related to threats of anticipated changes.” b. “Anxiety, related to outcome of treatments.” c. “Potential for infection, related to decreased white blood cell count.” d. “Inadequate coping, related to husband’s expectations regarding anticipated treatments.” ANS: B Early stages of cancer create anxiety about the outcome of treatments for the patient. DIF: Cognitive Level: Application REF: p. 119 OBJ: 3 | 6 TOP: Nursing Diagnosis KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 16. What is the most common site of cancer in adult women? a. Breast b. Lung c. Kidney d. Uterus ANS: A The gender of the person determines the risk for some cancers and the need for early detection. The incidence of breast cancer is 31% of the reported cases of cancer. DIF: Cognitive Level: Knowledge REF: p. 103 OBJ: 1 TOP: Common Sites of Cancer in Women KEY: Nursing Process Step: N/A MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. Which complaint should a nurse consider a warning sign for cancer? a. Intense pain in an area such as a hip or groin after carrying several gallons of paint up a ladder and painting the garage b. Persistent indigestion associated with difficulty swallowing c. Diarrhea that lasts 2 days after an all-day picnic at the beach d. A painful lump under the umbilicus that recedes when pushed but comes out again with a sneeze or hard cough ANS: B Persistent indigestion associated with dysphagia is an American Cancer Society–published risk for a cancerous sign. DIF: Cognitive Level: Comprehension REF: p. 106 OBJ: 4 TOP: Warning Signs of Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 18. What is the most common site of cancer in adult men? a. Colon b. Lung c. Pancreas d. Prostate ANS: D Gender defines some of the potential risks for cancer. Prostate cancer accounts for 33% of the reported cases of cancer in men. DIF: Cognitive Level: Knowledge REF: p. 103 OBJ: 1 TOP: Cancer Sites in Men KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 19. Which cytologic test, usually performed in outpatient settings, suggests the probability of a need for further testing for cancer cells? a. Chest radiography b. Koch test c. Papanicolaou (Pap) test d. Tine test ANS: C Preventive testing (Pap test) and screening reduce the risks for cancer and increase the chances of early treatment and is the most commonly performed screening test. DIF: Cognitive Level: Knowledge REF: p. 108 OBJ: 4 TOP: Knowledge of Diagnostic Tests KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 20. What is the cause of cell death when a patient receives radiation as a treatment for cancer? a. Separation of the cell from normal cells b. Damage of the cell membrane c. Alteration of the DNA of the cell d. Reduction of cell nutrition ANS: B The immediate effect of radiation is cell death as a result of damage to the cell membrane. The delayed effect is the alteration of the DNS so that it cannot replicate. DIF: Cognitive Level: Comprehension REF: p. 111 OBJ: 6 TOP: Radiation KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 21. What is the best menu choice for a patient with nausea who is undergoing radiation treatments every other day? a. Bowl of vegetable soup, chopped egg and pickle sandwich on wheat bread, one apple, and 8 oz of orange juice b. Broiled chicken with rice, vanilla yogurt, one-quarter cup of spinach, one-half ripe banana, and 8 oz of grape juice c. Spanish rice, one-half cup of mixed green salad, one-half cup of canned peaches, and 8 oz of Coke d. Spaghetti with tomato sauce, cheddar cheese toast strips, six celery sticks with peanut butter, and 8 oz of whole milk ANS: B Food choices for a nauseated patient should be mild and easily digested, with no spicy sauces or dark colas. DIF: Cognitive Level: Application REF: p. 125 OBJ: 6 TOP: Nutrition for Nauseated Patients KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 22. A patient is close to death with terminal liver cancer with widespread metastases and calls the nursing staff to his room every 5 minutes. Which interventions will be most supportive and in the best interest of the patient? a. Encourage and insist that the family request a transfer to hospice care because the general hospital does not have enough staff members to keep responding to the patient’s end-stage frequent calling and requests for minor help. b. Use fixed interval and cocktail medication administration. Frequently evaluate for breakthrough pain and anxieties. Answer the call bell quickly on the intercom or in person. c. Tell the family that as of this afternoon, all of the patient’s questions, comments, and expressed fears of dying and financial worries will be referred to the social worker, physician, or clergy. Otherwise, one of them can come in and sit beside the bed. d. Plan to limit strictly the time spent with the patient because the nurse cannot do much that could be beneficial at this point. ANS: B Therapeutic touch, the nurse’s presence, and sufficient pain medication to make the patient comfortable are appropriate nursing actions. DIF: Cognitive Level: Application REF: p. 127 OBJ: 7 TOP: Terminal Care Planning KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 23. Which statement by a patient should lead the nurse to conclude that the precolonoscopy instruction provided has been effective? a. “I know that the lighted tube he will use will help the doctor look at my tumor, and he might take a small piece of tissue to look at in the lab.” b. “I know that the light on the tube will help cure my cancer.” c. “I know the colonoscopy is very painful and embarrassing, and I hope no one sees me in that position.” d. “My daughter is coming in to see me today. I am glad to be looking forward to something pleasant.” ANS: A Colonoscopy diagnostic procedures are essentially painless but have no curative benefit. DIF: Cognitive Level: Application REF: p. 109 OBJ: 5 TOP: Colonoscopy KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. Which factors in middle-aged persons promote the formation of malignant cells? (Select all that apply.) a. Childbearing b. Increasing age c. Hormonal changes d. Heredity e. Diet ANS: B, C, D, E Increased age, hormonal changes, heredity, and a poor diet are possible sources of increased incidence of cancer in middle-aged persons. DIF: Cognitive Level: Knowledge REF: p. 103|p. 105 OBJ: 4 TOP: Conditions That Increase Incidence of Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What recommendations should a nurse make to a visitor of a patient who has an internal radiation implant? (Select all that apply.) a. Avoid visitation if you are pregnant. b. Take off all metals, such as your watch and belt. c. Limit your visitation time. d. Wear a protective lead apron. e. Stay at least 6 feet away from bedside. ANS: A, C, E Visitors are important to reduce the isolation of the patient who is undergoing radiation, but pregnant women should not visit. The visits of all persons should be limited to a few minutes, and they should be at least 6 feet from the bedside. Removing metal objects and wearing protective devices are not necessary. DIF: Cognitive Level: Comprehension REF: p. 112 OBJ: 6 TOP: Radiation Precautions KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 3. Why is adjuvant therapy given to patients with cancer who are free of signs of the disease? (Select all that apply.) a. Ensures eradication of undetected cells. b. Stabilizes normal cells. c. Diminishes recurrence of breast cancer. d. Reduces the extent of the tumor before surgery or radiation. e. Changes the pH of the system to inhibit cell growth. ANS: A, C Adjuvant therapy is given to symptom-free patients with cancer to eradicate undetected cells and to diminish the recurrence of breast cancer. Administration before surgery or radiation to reduce tumor bulk is called nonadjuvant therapy. The therapy does not stabilize normal cells or alter the pH. DIF: Cognitive Level: Comprehension REF: p. 110 OBJ: 4 TOP: Adjuvant Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 4. What action should a nurse implement if an intravenous vesicant cancer drug has extravasated? (Select all that apply.) a. Place a warm compress on the area. b. Chill the area with an ice pack. c. Raise the patient’s arm above the level of the heart. d. Stop the infusion. e. Notify the charge nurse. ANS: D, E The licensed practical nurse should stop the infusion and notify the charge nurse so that specially trained personnel can intervene. DIF: Cognitive Level: Application REF: p. 114 OBJ: 6 TOP: Extravasation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 5. When is surgical remedy for cancer most successful? (Select all that apply.) a. Cancer is detected early. b. The tumors are fast growing. c. Cancer cells have invaded only a nonvital structure. d. Lymph glands have not been involved. e. Cancer cells are confined to only two areas. ANS: A, D Surgical remedies have a high success rate if the cancer is detected early, the tumors are not fast growing, the cancer cells have not invaded any vital structure, the lymph glands have not been involved, and the cancer cells are isolated in one area. DIF: Cognitive Level: Knowledge REF: p. 108 OBJ: 6 TOP: Surgery for Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort COMPLETION 1. A nurse clarifies that cells that change from their tissues of origin and have multiple nuclei are categorized as _. ANS: undifferentiated Undifferentiated cells are those that change from normal cells of tissue origin. These cells may have a large nucleus or multiple nuclei. DIF: Cognitive Level: Knowledge REF: p. 103 OBJ: 2 TOP: Undifferentiated Cells KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Radiation is now measured in gray rather than rads. One gray is equal to rads. (Use numeric characters only.) ANS: 100 One gray is equal to 100 rads. DIF: Cognitive Level: Knowledge REF: p. 111 OBJ: 2 TOP: Gray KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 3. List the tumors in order based on the following tissue of origin: 1, fat; 2, fibrous; 3, smooth muscle; 4, glands; 5, bone. (Place the events in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Sarcoma b. Lipoma c. Leiomyoma d. Fibroma e. Carcinoma ANS: BDCEA Tumors are associated with the tissue from which they arise: fat tumors are lipomas, fibrous tissue tumors are fibromas, smooth muscle tumors are leiomyomas, and bone tumors are sarcomas. Carcinomas include glands. DIF: Cognitive Level: Comprehension REF: p. 105 OBJ: 3 TOP: Tumor Type KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 08: Pain Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. The length of time that a nurse should leave heat to an injured hip of a patient is no longer than a. 15 minutes. b. 20 minutes. c. 30 minutes. d. 1 hour. ANS: C If a heating device is left on more than 30 minutes, the effectiveness of the treatment is diminished, and injury to the tissues may occur. DIF: Cognitive Level: Comprehension REF: p. 142 OBJ: 8 TOP: Timing of Heat Application KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A patient with an extensive abdominal surgical procedure is assessed by the nurse as having predictable pain. How often should the nurse administer analgesics to this patient to be most effective? a. As needed (PRN) b. Once a day c. Twice a day d. Around the clock ANS: D Using a preventive approach for managing this patient’s pain management is the best plan for the nurse because the pain is predictable and major. DIF: Cognitive Level: Application REF: p. 143 OBJ: 8 TOP: Predictable Pain and Analgesic Administration KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. What sympathetic responses to pain might be assessed by the nurse? a. Increased blood pressure, increased pulse, and increased respiratory rate b. Decreased blood pressure, decreased pulse, and increased respiratory rate c. Increased blood pressure, decreased pulse, and increased respiratory rate d. Decreased blood pressure, decreased pulse, and decreased respiratory rate ANS: A The sympathetic nervous system controls blood pressure, pulse, and respiration; it is stimulated during pain. DIF: Cognitive Level: Comprehension REF: p. 134 OBJ: 7 TOP: Sympathetic Response to Pain KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A health care provider has prescribed both heat and cold treatments for an older adult patient with a leg injury. The nursing care plan reflects secondary diagnoses of peripheral vascular disease (PVD), diabetes, and an allergy to latex. Which of the prescribed treatments should the nurse administer and why? a. The nurse will use cold treatment because patients with diabetes and a latex allergy cannot tolerate heat. b. The nurse will use cold treatment for this patient with a fracture because cold will help set the cast. c. The nurse will use heat treatment because cold is contraindicated for patients with PVD. d. The nurse will use heat treatment because heat will increase circulation and increase the threat of infection in the injured part. ANS: C Patients with PVD have blood flow problems that physiologically slow circulation. This problem would be exacerbated by cold. Heat will increase the circulation, which would be a desired effect. DIF: Cognitive Level: Application REF: p. 141 OBJ: 6 | 8 TOP: Thermal Applications with Secondary Diagnosis KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Reduction of Risk 5. A nurse notices that a patient seems calm and peaceful despite an assessment that the patient’s injuries might be causing severe pain. The patient tells the nurse that using yoga and meditation lessens the perceptions of pain to tolerable levels. Which other alternative intervention should the nurse suggest to help relax this patient for pain relief? a. Indulging in a favorite food b. Music by a favorite artist c. Reading exciting science fiction d. Self-administration of drugs ANS: B Alternate methods of pain relief are effective for many patients. Activities such as yoga, meditation, and listening to music are helpful and relaxing. DIF: Cognitive Level: Application REF: p. 141 OBJ: 3 | 8 TOP: Alternate Methods of Pain Relief KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. What intervention of pain control exemplifies the gate control methods of pain relief? a. Assisting the patient to ambulate b. Giving a massage c. Providing an ice cold beverage d. Instructing the patient in stretching exercises ANS: B Massage, position change, hot or cold applications, and distraction all can close the gate. DIF: Cognitive Level: Comprehension REF: p. 132 OBJ: 2 TOP: Gate Theory KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. To perform a nursing assessment correctly, a nurse must remember that pain perception involves several central nervous system (CNS) processes. Which are examples of CNS processes? a. Afferent pathways carry messages to the spinal cord. b. Efferent pathways stimulate the spinal cord to recognize the location of pain. c. Nociceptors in the brain stimulate the spinal cord. d. Pain receptors in muscle, skin, and subcutaneous tissue stimulate efferent pathways. ANS: B Pain perception ascends to the brain and back down again to imprint the pain. These are functions of the CNS. Efferent pathways carry pain impulses to the body via the spinal cord. Afferent pathways carry messages to the brain for interpretation. DIF: Cognitive Level: Comprehension REF: p. 132 OBJ: 2 TOP: Pain Pathways KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. A nurse is teaching a patient how to use a transcutaneous electrical nerve stimulation (TENS) unit and how it works. What is the most appropriate information for the nurse to relay? a. “The stimulation of the skin seeks to localize the acute pain and will last for several minutes after the unit is applied.” b. “This unit stimulates both the skin and the underlying tissues to decrease the intensity of the pain.” c. “The mechanism for use of this unit is well known and can be read.” d. “During those days when using the TENS unit, no analgesic can be given.” ANS: B The exact mechanism for the pain relief is unknown. The effects last for the time that the unit is applied to the patient and a short time thereafter. DIF: Cognitive Level: Application REF: p. 141 OBJ: 8 TOP: TENS Units KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. What should greatly reduce postoperative pain for a patient about to undergo a hip replacement? a. Femoral nerve blocks b. Extremely deep general anesthesia c. Practicing leg lifting exercises before surgery d. Placing an analgesic patch directly over the incision ANS: A Preoperative femoral nerve blocks will significantly reduce the pain for 24 hours postoperatively. DIF: Cognitive Level: Comprehension REF: pp. 133-134 OBJ: 8 TOP: Femoral Blocks KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 10. A patient continues to report pain after the administration of the prescribed analgesic. Why should the nurse change the nursing care plan? a. Patient’s pain threshold has risen. b. Patient’s pain threshold has lowered. c. Patient has become addicted. d. Patient is seeking attention. ANS: B The sensation of pain is perceived as increased when the pain threshold is lowered. Insufficient data exists in this situation to assume addiction or the need for attention. DIF: Cognitive Level: Comprehension REF: p. 133 OBJ: 10 TOP: Lowered Pain Threshold KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. A nurse administers nalbuphine (Nubain), an opioid agonist–antagonist, to a 78-year-old patient. The family is worried about the patient and thinks that this drug is too strong and will cause harm. What should the nurse assure the family regarding this drug? a. Does not accumulate in the body b. Blocks the side effects observed in opioid agonists c. Does not affect the CNS d. Can only be given orally ANS: B A drug classified as an agonist–antagonist is able to relieve pain at the CNS level and is able to block some side effects of opioid agonists. The drug can be given intramuscularly or orally. DIF: Cognitive Level: Application REF: p. 145 OBJ: 9 TOP: Use of Opioids KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. A patient admitted with the diagnosis of possible myocardial infarction complains of pain and tingling in the left arm and says, “How in the world could I be having a heart attack when it’s just my arm that is giving me trouble?” What type of pain should the nurse explain that the patient is experiencing? a. Referred pain b. Psychogenic pain c. Neuromuscular pain d. Muscle spasms of shoulder ANS: A Pain is what the patient says it is and should be communicated as such. However, pain in specific areas may be referred pain, and left arm discomfort is typically referred from the heart. The nurse administers the analgesic as ordered and frequently checks to determine whether the pain is relieved. DIF: Cognitive Level: Comprehension REF: p. 137 OBJ: 4 TOP: Referred Pain KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. Every time the right arm is raised, a patient reports to the nurse that pain is triggered in the right shoulder. How should the nurse document this description? a. Referred pain b. Aggravating factor c. Alleviating factor d. Past experience with the pain ANS: B The aggravating factor that is causing pain is important information to gather by the nurse and to communicate specifically in the chart, as well as to the registered nurse. DIF: Cognitive Level: Comprehension REF: p. 137 OBJ: 2 TOP: Factors Defining the Pain Description KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Coordinated Care 14. A patient who had a myocardial infarction 2 days earlier has been eating well, is ambulating with assistance, and is receiving antibiotics and morphine by intravenous (IV) drip. The patient complains of constipation this morning. What should the nurse assess as the probable cause of the constipation? a. Inadequate fluid intake b. Lack of exercise c. Administration of antibiotics d. Administration of an analgesic medication ANS: D Opioid administration frequently causes constipation. This patient is eating, taking IV fluids, and walking. Antibiotics rarely cause constipation. DIF: Cognitive Level: Application REF: p. 147 OBJ: 9 TOP: Side Effects of Opioids KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 15. A patient who is obviously in pain refuses the morphine that has been prescribed for pain control because of a fear of addiction. What should the nurse explain is the estimated percentage of patients taking prescribed pain protocols who become addicted? a. Less than 1% b. 10% to 25% c. 30% to 50% d. 80% to 90% ANS: A When used for severe pain management relief, opioids rarely result in addiction. DIF: Cognitive Level: Knowledge REF: p. 151 OBJ: 9 TOP: Addiction Potential KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 16. Morphine sulfate (30 mg) IM PRN was prescribed for pain for an 80-year-old patient with emphysema who weighs 100 lb. What is the most appropriate action for the licensed practical/vocational nurse (LPN/LVN)? a. Transcribe the order and wait to see if the patient needs it. b. Transcribe the order for an oral dose instead of IM dose. c. Call the physician and clarify the order. d. Tell the RN about the order. ANS: D Morphine is usually given in a dose of 10 mg (one-sixth grain) IM. The usual oral dose is 0.5 gr (30 mg). The order should be called to the attention of the RN so that the intent can be clarified before transcribing the order for the older patient, who usually requires a smaller dose. DIF: Cognitive Level: Application REF: p. 145 OBJ: 6 TOP: Morphine Dosage KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 17. What assessment should a nurse make to evaluate the presence of pain in a patient who is cognitively impaired? a. Amount of time spent sleeping during the day b. Consistent stoic facial expression c. Increased social interaction d. Increasing confusion ANS: D Patients who are cognitively impaired may show pain by increased confusion, reduction in social contacts, grimacing, or squinting the eyes. DIF: Cognitive Level: Application REF: p. 140 OBJ: 7 TOP: Pain Assessment in Cognitively Impaired KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 18. Which steps should the LPN/LVN follow when performing a pain assessment? a. Assess vital signs, status of pain, and aggravating factors. b. Assess location, quality, and intensity on an identified scale. c. Assess the intensity on an identified scale and record findings. d. Assess vital signs and location, and report to the RN. ANS: B The assessment of pain requires the nurse assess location, quality, and intensity based on an identified scale. Vital signs are important in addition but are not part of the six steps. DIF: Cognitive Level: Application REF: pp. 137-138 OBJ: 7 TOP: Nurse’s Pain Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 19. Two patients are hospitalized with the same diagnosis, but one is 23 years old, with acute recent pain from an injury, and the other is 64 years old, with pain of long-standing duration of several years. What is the difference in the anticipated assessments? a. Acute pain for young patients is more intense at the same level, but these patients experience few changes in vital signs. b. Young patients with acute pain exhibit fewer changes in vital signs but still report true levels of pain at levels 8 to 10. c. Older adult patients with chronic pain exhibit increased changes in vital signs and report levels of pain lower than reality. d. Older adult patients with chronic pain usually report lower levels of pain much less severe than they really are. ANS: D Older adult patients with chronic pain do not report pain as severe at the same level as younger patients do for several reasons. For example, older adult patients believe that pain comes with old age, or they do not want to bother the staff. Frequently, chronic long-standing pain does not change normal values of the vital signs. DIF: Cognitive Level: Comprehension REF: p. 133 OBJ: 6 TOP: Age-Related Assessments of Pain KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. How does the International Association for the Study of Pain define the sensation of pain? a. Unpleasant sensory and emotional experience b. Whatever the person experiencing it says it is c. Psychogenic response to tissue injury d. Physical and psychogenic response to the need for drugs ANS: A The International Association for the Study of Pain defines pain as an unpleasant sensory and emotional experience. DIF: Cognitive Level: Knowledge REF: p. 131 OBJ: 1 TOP: Definition of Pain KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 21. A nurse is notified when a patient, newly admitted with liver and gallbladder disease, complains of pain in the right middle back and asks for some pain medication. What is the best interpretation of this reported assessment by the nurse? a. The patient is just complaining to see whether the staff will give out pain medications. b. The patient has referred pain sensations. The nurse should follow orders for administering pain medication. c. The patient has an injury on the back from an unknown cause that needs immediate assessment. d. The patient is a chronic complainer with anxieties about his condition. ANS: B Referred pain is a very real physical complaint, and the nurse should give the patient the pain medication as ordered. DIF: Cognitive Level: Application REF: pp. 137-138 OBJ: 2 | 5 TOP: Referred Pain KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 22. What is the most common result of prolonged and unrelieved pain? a. Release of endorphins b. Lowered pain threshold c. Stimulated gate control d. Lowered blood pressure ANS: B Pain that is unrelieved lowers the pain threshold because the patient becomes anxious that the pain may not ever be relieved. The blood pressure increases, and the effects of endorphins and gate control have been exhausted. DIF: Cognitive Level: Comprehension REF: p. 133 OBJ: 4 TOP: Pain Unrelieved KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 23. A nurse is administering morphine IM, which was prescribed for a patient reporting severe pain. What should be the nurse’s primary assessment focus on to evaluate the patient’s response to this drug? a. Cardiac rhythms for tachycardia b. Respiratory rate for tachypnea c. Increased bowel sounds in the gastrointestinal system d. Sedative effects in the neurologic system ANS: D Morphine initially produces sedation that allows the patient to sleep and rest from the pain. This result is considered a side effect. DIF: Cognitive Level: Application REF: p. 146 OBJ: 9 TOP: Morphine IM for Pain Relief KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 24. A nurse explains to a patient the gate control theory of pain. Where does the perception of pain originate in the gate control theory? a. Large arteries b. Vena cava c. Large nerve fibers d. Small nerve fibers ANS: D The perception of pain is made through small nerve fibers, which transmit impulses up to the brain, where they are interpreted as pain. Large nerve fiber receptors block the gate to decrease transmission to the interpretive brain area. DIF: Cognitive Level: Knowledge REF: p. 132 OBJ: 2 TOP: Pain Perception/Gate Control Theory KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 25. When a patient with sciatica seats himself in a chair, he gasps and complains of a burning and shooting pain in his hip. What type of pain does this represent? a. Referred b. Neuropathic c. Visceral d. Acute ANS: B Neuropathic pain is characterized by burning and shooting sensations without a stimulus. This situation is not an example of acute pain because neuropathic pain does not follow a nociceptor path as do both visceral and referred pain. DIF: Cognitive Level: Comprehension REF: p. 135 OBJ: 4 TOP: Neuropathic Pain Perception KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. What are the standards for pain management published by The Joint Commission (TJC)? (Select all that apply.) a. Perform organized pain assessment. b. Record results of analgesia. c. Give adequate discharge instruction about pain relief. d. Recognize the right of a nurse to manage pain. e. Teach patients about pain control methods. ANS: A, B, C, E Performing organized pain assessment, recording results of analgesia, giving adequate discharge information about pain, relief and teaching patients about pain control methods are all standards for pain management published by the Joint Commission. The standards include recognizing the right of the patient to assess and manage pain, not the nurse. DIF: Cognitive Level: Knowledge REF: p. 139 OBJ: 8 TOP: TJC Standards KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. What instruction should the nurse provide to a patient who has had radiofrequency lesioning for leg pain? (Select all that apply.) a. Relief may not be permanent. b. The leg may tingle occasionally. c. The foot may discolor and twitch at times. d. Snug shoes should be worn at all times. e. Caution should be taken to prevent injury to the leg. ANS: A, B, E The relief may not be permanent because of the regeneration of nerve tissue. Extra caution should be taken to prevent injury because pain perception is altered. Snug shoes would cause injury. The goal of radiofrequency lesioning is to provide prolonged pain relief and patients may report tingling or buzzing sensations instead of pain. DIF: Cognitive Level: Comprehension REF: p. 133 OBJ: 8 TOP: Radiofrequency lesioning KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. A nurse explains that afferent pathways are activated by pain receptors called . ANS: nociceptors Pain receptors that are called nociceptors activate the afferent pathways. DIF: Cognitive Level: Knowledge REF: p. 132 OBJ: 2 TOP: Nociceptors KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. and enkephalins are natural opioid-like substances that block pain perception. ANS: Endorphins Endorphins and enkephalins are natural opioid substances that help block the perception of pain. DIF: Cognitive Level: Knowledge REF: p. 132 OBJ: 2 TOP: Endorphins KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 09: Shock Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What are the four types of shock? a. Multiple organ, cardiogenic, renal, and anaphylactic b. Cardiogenic, renal, hypovolemic, and septic c. Renal, hypervolemic, obstructive shock, and neurogenic d. Hypovolemic, cardiogenic, obstructive shock, and vasogenic ANS: D The four large categories of shock are hypovolemic (low-circulating volume), cardiogenic (low-cardiac output), obstructive (occluded vascular pathway), and vasogenic (massive vasodilation). DIF: Cognitive Level: Knowledge REF: p. 153 OBJ: 1 TOP: Types of Shock KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Although several life-supporting systems of the body are involved in the pathophysiologic characteristics of shock, shock itself results from failure of which system? a. Circulatory b. Endocrine c. Neurologic d. Respiratory ANS: A When the heart fails as a pump, the lack of tissue perfusion follows and deprives all the body’s cells of oxygen and the removal of wastes. DIF: Cognitive Level: Knowledge REF: p. 153 OBJ: 2 TOP: Definition of Shock KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 3. A nurse is assessing a patient who is in shock. What should the nurse be aware that one common sign will be, regardless of the cause of the shock? a. The skin is cool and dry with cyanotic nail beds. b. The skin is cool and moist with cyanotic nail beds. c. The nail beds are reddened, and the skin is moist and warm. d. The nail beds are reddened, and the skin is dry and warm. ANS: B Venous blood pools in the extremities of the fingers as a result of the lack of adequate perfusion of tissues, which makes the skin cool and moist from a lack of oxygen and waste exchanges. DIF: Cognitive Level: Comprehension REF: p. 157 OBJ: 3 TOP: Common Signs of Shock KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. What should a nurse assessing a patient in the organ-dysfunction stage of shock expect to find? a. Bounding pulse, decreased respirations, and decreased blood pressure b. Bounding pulse, shallow respirations, and significantly increased blood pressure c. Thready pulse and deep respirations with decreased blood pressure d. Thready pulse and irregular respirations with increased blood pressure ANS: C When the cause of shock is not corrected, irreversible organ damage takes place. The pulse is weak; the respirations increase in an effort to decrease the carbon dioxide level; and, with less volume being pumped, the blood pressure falls. DIF: Cognitive Level: Comprehension REF: p. 156 OBJ: 3 TOP: Signs of Shock KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. A licensed practical/vocational nurse (LPN/LVN) is assisting in developing a nursing care plan for a patient in shock. Which patient problem should be included? a. Excess cardiac output, related to hypertension b. Excess cardiac output, related to hypotension c. Inadequate cardiac output, related to hypovolemia d. Inadequate cardiac output, related to hypertension ANS: C Decreased amount of blood is ejected from the heart because of a decreased volume of fluid in the intravascular compartment. DIF: Cognitive Level: Application REF: p. 153 OBJ: 7 TOP: Nursing Diagnosis for Patients in Shock KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. How does the intraaortic balloon pump (IABP) assist a patient who is in cardiogenic shock to increase cardiac output? a. Provides generalized vasoconstriction. b. Inflates during the diastole phase. c. Constricts the vena cava. d. Adds hypertonic fluid to the circulating volume. ANS: B The IABP inflates during diastole (relaxation) phase and deflates during the systole (constriction) phase, which improves cardiac output. DIF: Cognitive Level: Comprehension REF: p. 160 OBJ: 6 TOP: IABP KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A nurse is explaining to a family member the pathophysiologic characteristic of distributive shock. What information should the nurse include? a. The intravascular compartment fills beyond capacity, allowing fluid to leak out, compressing vital organs. b. The circulating volume causes excessive constriction of the vessels, causing blood pooling. c. Widely fluctuating blood pressures stimulate vascular collapse, causing severe alterations in peripheral perfusion. d. Although the circulating volume is intact, excessive vascular dilation causes drastic drops in the blood pressure. ANS: D In distributive shock, blood pooling from dilated vessels drops the blood pressure without loss of circulating volume. DIF: Cognitive Level: Knowledge REF: p. 154 OBJ: 2 TOP: Distributive Shock KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. A nurse is caring for a patient who has a cervical spine injury and assesses progressive hypotension. What does this signify? a. Anaphylaxis b. Respiratory alkalosis c. Multiple organ dysfunction syndrome (MODS) d. Neurogenic shock ANS: D Gradually decreasing blood pressure in a person with a spinal injury is an indicator of neurogenic shock related to the parasympathetic stimulation, which causes generalized vasodilation. DIF: Cognitive Level: Comprehension REF: p. 155 OBJ: 3 TOP: Implementation KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. While shopping in the mall, a nurse sees a lady suddenly fall to the floor. On immediate assessment, the nurse realizes she is not in cardiac arrest and has no need for cardiopulmonary resuscitation (CPR). What should be the immediate actions by the nurse? a. Check the pulse and respirations and call for a blood pressure cuff. b. Check the pulse, respirations, skin color, and temperature. c. Call for help and check the pulse, respiration, and mental status. d. Ask someone to help place large blankets or coats under her legs and trunk. ANS: C Shock treatment requires expert medical implementation. However, the nurse may provide first-line support until such help arrives. Circulatory collapse has to be monitored first; pulse, respiration, and mental status should be assessed to evaluate whether oxygen is reaching the brain. DIF: Cognitive Level: Application REF: p. 157 OBJ: 4 TOP: Emergency Aid for Shock Victim KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. A nurse is explaining the rationale behind the use of hypothermic devices to a patient’s family. When relaying information what explanation should the nurse provide when asked why this garment is used? a. To improve neurologic recovery. b. Decreases internal hemorrhage. c. Warms the patient to create less metabolic demand. d. Applies pressure during the systole phase and relax pressure during the diastole phase. ANS: A Hypothermic devices cool the body by circulating ice water while in direct contact with the patient’s skin. These devices may improve neurologic recovery after cardiac arrest of cardiac origin. DIF: Cognitive Level: Comprehension REF: p. 160 OBJ: 6 TOP: Hypothermic devices KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. In treating a person outside of a medical facility, a nurse knows that immediate circulatory support for the vital organs must begin as quickly as possible because, without oxygen, the brain cells will begin to die in how many minutes? a. 4 b. 6 c. 14 d. 24 ANS: A Brain cells must have oxygen to live; they are very sensitive to lack of oxygen and begin to die in 4 minutes. DIF: Cognitive Level: Knowledge REF: p. 165 OBJ: 2 TOP: Brain Death without Oxygen KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. The stages of shock proceed in a definite sequence. What is the correct order? a. Hypovolemic, obstructive, cardiogenic b. Cardiogenic, hypovolemic, obstructive c. Pre-shock, shock, end-organ dysfunction d. Pre-shock, end-organ dysfunction, shock ANS: C The sequence of the stages of shock are pre-shock, shock, and end-organ dysfunction. Understanding the sequence of the progression of shock allows the medical team to plan and implement the correct steps to reverse it. Hypovolemic, obstructive, and cardiogenic are types of shock. DIF: Cognitive Level: Knowledge REF: p. 155 OBJ: 1 TOP: Stages of Shock KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 13. Which position enhances cerebral blood flow to counteract the symptoms of neurogenic shock? a. Fowler b. Trendelenburg c. Gravity neutral d. Side lying ANS: B The Trendelenburg position, with the patient’s head down, allows gravity to pull blood to the cerebrum. All other positions are ineffective for improving cerebral perfusion. DIF: Cognitive Level: Knowledge REF: p. 164 OBJ: 5 TOP: Positions to Counteract Shock KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A nurse is administering heparin, subcutaneous twice daily, to a patient in cardiogenic shock. What is the expected action of this drug? a. Inotropic to improve cardiac contractibility b. Anticoagulant to prevent blood clots c. Antidysrhythmic to restore normal cardiac contractibility d. Vasopressor to increase blood pressure ANS: B Cardiogenic shock may produce clots because of blood stasis, and the heparin will delay clot formation. DIF: Cognitive Level: Knowledge REF: p. 163 OBJ: 5 | 6 TOP: Heparin for Anticoagulation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 15. One of the most important assessments that a nurse makes is to check urine output. Which value objectively validates minimal acceptable renal perfusion for the average-size person? a. 0.5 mL/kg/hr b. 0.5 mL/lb/hr c. 1 mL/lb/hr d. 0.2 mL/kg/hr ANS: A When the kidneys produce at least 0.5 mL/kg/hr of urine, the indication is that the vital organs are also being perfused. DIF: Cognitive Level: Knowledge REF: p. 161 OBJ: 5 TOP: Urine Output As Measure of Tissue Perfusion KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 16. A patient is receiving norepinephrine as a first line treatment for shock in order to increase vascular resistance. Which type of shock is the patient being treated for? a. Septic b. Cardiogenic c. Anaphylactic d. Neurogenic ANS: A Norepinephrine is used as a first line treatment for septic shock in order to increase vascular resistance. DIF: Cognitive Level: Comprehension REF: p. 159 OBJ: 6 TOP: Pharmacologic Therapy KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 17. A patient’s family voices concern regarding the purpose of some of the interventions for systemic inflammatory response syndrome (SIRS). What explanation by the nurse is most appropriate when explaining the rationale of treatment? a. “Applying a MAST garment is mandatory to promote and conserve body heat.” b. “Inserting an IABP is required to decrease fluid leaking into the extravascular space.” c. “Maintaining strict isolation is vital to prevent an overlying bacterial infection.” d. “Aggressive treatment is necessary to support the multiple failing organs.” ANS: D SIRS is the final and possibly fatal stage of shock. The body’s defenses are supported aggressively and rapidly. MAST and IABP are measures used to increase circulating volume. Isolation is not indicated. DIF: Cognitive Level: Comprehension REF: pp. 162-163 OBJ: 6 TOP: SIRS Treatment KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk COMPLETION 1. A nurse explains that pericardial tamponade and tension pneumothorax can place the patient at risk for shock. ANS: obstructive Obstructive shock can result from pericardial tamponade or tension pneumothorax. DIF: Cognitive Level: Knowledge REF: p. 154 OBJ: 1 | 2 TOP: Obstructive Shock KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse explains that when shock forces the body into anaerobic metabolism, organ damage is caused by a product of that metabolism, which is . ANS: lactic acid Lactic acid, a by-product of anaerobic metabolism, can cause organ damage in the patient who is in shock. DIF: Cognitive Level: Knowledge REF: p. 156 OBJ: 2 TOP: Lactic Acid KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A nurse explains that the minimal acceptable hourly urine output for a patient in shock who weighs 220 lb is mL. (Use numeric characters only.) ANS: 50 220 lb ÷ 2.2 lb = 100 kg; 0.5 mL/kg/hr x 100 kg = 50 mL. DIF: Cognitive Level: Analysis REF: p. 161 OBJ: 7 TOP: Minimum Urine Output KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A nurse is aware that immobility and insertion of urinary catheters, although therapeutic, also places the patient at risk for . ANS: infection The insertion of a Foley catheter and long-term immobility can cause infections. DIF: Cognitive Level: Comprehension REF: p. 162 OBJ: 6 TOP: Infection KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Reduction of Risk Chapter 10: The Older Adult Patient Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. How is the term old age or aged best defined? a. Person’s state of mind b. Person older than 65 years of age c. Process of growing older d. Person of advanced age ANS: D Aged or old age is defined as advanced in years. DIF: Cognitive Level: Comprehension REF: p. 167 OBJ: 2 TOP: Definitions of Old Age KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. How is aging recognized by gerontologists as a developmental process? a. Measured in chronologic years b. Directly related to heredity c. Related to behavioral characteristics d. Begins at the time of birth ANS: D Geriatrics is the science of old age and the application of knowledge related to the biologic, biomedical, behavioral, and social aspects of aging. DIF: Cognitive Level: Knowledge REF: p. 167 OBJ: 2 TOP: Definitions of Old Age KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 3. What understanding is a prerequisite for a nurse working with the geriatric patient? a. Specialized knowledge is needed. b. Geriatric patients are physically impaired. c. Most geriatric patients will develop dementia. d. Geriatric patients need to be closely supervised. ANS: A Knowledge, understanding, and caring are prerequisites for working effectively with older adults. Although specialized formal education programs at the graduate level are available for gerontological nurses, many nurses gain specials skills through on-the-job experiences. DIF: Cognitive Level: Comprehension REF: p. 168 OBJ: 1 TOP: Roles of the Gerontological Nurse KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 4. A 78-year-old resident of a long-term care facility insists on wearing high heels and miniskirts to the dining room for meals and will not leave her room without first applying glamorous makeup. What should the gerontological nurse assess as the reason for this behavior? a. Insecurity about her appearance b. Trying to cope with the changes of aging c. Denial concerning her advancing age d. Her fashion consciousness ANS: C Some older people confront aging, but others deny it by acting in a younger manner. DIF: Cognitive Level: Analysis REF: p. 175 OBJ: 2 TOP: Ageism: Myths and Stereotypes KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 5. What does Butler, a well-known gerontologist, relay regarding ageism? a. It dehumanizes older individuals. b. It is based on the biologic theory of aging. c. It is based on natural and purposeful occurrences. d. It continues to change as the population ages. ANS: A Ageism is the stereotyping of and discrimination against people because of their age. DIF: Cognitive Level: Comprehension REF: p. 168 OBJ: 2 TOP: Ageism: Myths and Stereotypes KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 6. What are the effects of aging on the nervous system? a. Accelerated loss of neurons in the brain b. Gradually declining loss of intellectual capability c. Decreased conduction speed of neurons d. Loss of long-term memory ANS: C Age-related effects on body systems are integral parts of the basis of nursing care for older adults. The aging nervous system is characterized by decreased conduction speed of neurons. DIF: Cognitive Level: Comprehension REF: p. 170 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A nurse is caring for older adult patients with mild cognitive impairment (MCI). What are these patients more likely to develop? a. Dementia, non-Alzheimer type b. Alzheimer dementia c. Parkinson disease d. Psychotic disorders ANS: B Approximately 40% of people with MCI develop Alzheimer dementia within 3 years. DIF: Cognitive Level: Comprehension REF: p. 171 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. What is the most appropriate nursing action when planning activities to improve short-term memory for an older adult patient experiencing memory deficits? a. Maintain the same daily schedule. b. Rehearse memory training. c. Provide a varied and stimulating daily schedule. d. Conduct deep-breathing exercises. ANS: B Using mnemonics and memory rehearsal may improve memory performance in some older individuals. DIF: Cognitive Level: Application REF: p. 171 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. What is the best example of normal memory change or lapse of memory? a. Relying on another person to remember names or important events b. Occasional forgetfulness or inability to recall names or facts c. Difficulty in recalling recent events d. Difficulty in recalling past events ANS: B Memory lapses such as forgetting a name or misplacing an item are common, normal memory changes. DIF: Cognitive Level: Comprehension REF: p. 170 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 10. Which facts are generally accepted for most older adults? a. Intellectual capabilities are impaired. b. Functional brain activities decrease. c. Functional intellectual capability is maintained. d. Creativity and judgment are severely impaired. ANS: C Functional ability may not be significantly affected because reserve cells are able to compensate. DIF: Cognitive Level: Comprehension REF: p. 170 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 11. What factor increases the risk of respiratory infection for older adults? a. Decreased ciliary action b. Decreased physical activity c. Inadequate hydration d. Poor personal hygiene ANS: A The ability to perform strenuous work decreases with age. The ciliary action responsible for movement of secretions from the lung is compromised because of epithelial atrophy. DIF: Cognitive Level: Comprehension REF: p. 171 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. A nurse is caring for an older person whose renal changes make it impossible to concentrate or dilute urine. For what is this patient at the greatest risk? a. Urinary infection b. Dehydration c. Incontinence d. Renal failure ANS: B The kidney’s ability to concentrate urine is a major defense against dehydration. DIF: Cognitive Level: Application REF: p. 172 OBJ: 3 TOP: Physiologic Renal Change KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. Which assessment is the greatest priority to report when considering the gastrointestinal (GI) changes that take place in the geriatric patient? a. 24-hour urinary output of 1450 mL b. 24-hour dietary intake of 75% of meals c. Last bowel movement 4 days ago d. Weight loss of 2 lb since admission 2 months ago ANS: C GI changes include bloating, diarrhea, pernicious anemia, and constipation. DIF: Cognitive Level: Application REF: p. 173 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 14. Which assessment made by the nurse is a major sign of renal changes related to age? a. Hematuria b. Nocturia c. Urgency incontinence d. Renal calculi ANS: C Urgency incontinence is related to several age-related changes in the urinary musculature. Renal calculi and hematuria are pathologic symptoms and are not age related. Nocturia is not specifically related to aging. DIF: Cognitive Level: Comprehension REF: p. 172 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 15. What should be the most significant assessment when gathering data concerning the musculoskeletal system? a. Slow gait b. Degree of motion of all joints c. Enlarged joints d. Crepitus in joints ANS: B Determine mobility by assessing the range of motion in all joints; in addition, look for signs of inflammation and pain associated with mobility. DIF: Cognitive Level: Application REF: p. 173 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 16. What is the most appropriate nursing intervention for a patient with presbycusis? a. Speak clearly and distinctly while facing the patient. b. Announce your presence when entering the patient’s room. c. Place needed articles within easy reach. d. Orient the patient to time and place as needed. ANS: A Presbycusis is hearing loss. Get the patient’s attention so that the patient can concentrate on what you are saying or read lips. DIF: Cognitive Level: Application REF: p. 173 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 17. What should the nurse suspect a patient is developing when he is observed holding his Bible 6 inches from his face and turns his head to read out of the corner of his eyes? a. Cataracts b. Glaucoma c. Presbyopia d. Macular degeneration ANS: D The leading cause of new blindness in old age is macular degeneration, which results in the loss of central vision. DIF: Cognitive Level: Comprehension REF: p. 174 OBJ: 3 TOP: Macular Degeneration KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 18. What is true regarding the chemosensory changes observed in older adults? a. They are directly related to the aging process. b. They are most often caused by disease. c. They begin in the fifth decade of life. d. They affect more women than men. ANS: B Major changes in the ability to taste are often caused by disease or a side effect of certain drugs. DIF: Cognitive Level: Comprehension REF: p. 174 OBJ: 3 TOP: Chemosensory Change KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 19. A nurse explains to family members that the final developmental stage is ego integrity. What should occur in the older adult, according to Erikson, if this stage is not mastered? a. Needs to repeat a previous stage. b. Experiences despair. c. Inability to advance past the present stage d. Experiences disappointment. ANS: B The final developmental task is ego versus despair. This negative resolution is often seen as depression and social withdrawal. DIF: Cognitive Level: Comprehension REF: p. 175 OBJ: 3 TOP: Psychosocial Factors KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 20. What is the best nursing action when assisting an older patient to relieve the discomfort of pruritus related to dry skin? a. Encourage the patient to talk to the primary care physician about the problem. b. Encourage the patient to take a tepid bath and use moisturizers. c. Teach the patient that pruritus is an expected consequence of aging. d. Establishing a medication regimen to control the discomfort. ANS: B Because pruritus is caused by loss of oils in the skin, the patient should be encouraged to take tepid baths; use moisturizers; and avoid overuse of antiperspirants, soaps, perfumes, and long hot baths. DIF: Cognitive Level: Application REF: p. 172 OBJ: 3 TOP: Physiologic Change KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 21. A newly admitted 72-year-old resident of a long-term care facility naps frequently during the day, stating that he is tired. What is the best action by the nurse? a. Obtain an order from the primary caregiver for a sedative. b. Ask the patient if he is sleeping well at night. c. Plan activities to keep the patient awake during the day. d. Tell the patient that he cannot take any more naps. ANS: B Determining if or the reason why the patient is not sleeping at night will help the nurse implement the appropriate nursing actions. Depression may be interfering with adapting to the long-term facility. DIF: Cognitive Level: Application REF: pp. 175-176 OBJ: 4 TOP: Psychosocial Factors KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance 22. What is the best reason that drug toxicity can occur as a result of an age-related change in the liver? a. Increased liver size b. Decreased liver enzyme activity c. Rapid blood flow through the liver d. Fluid accumulation in the portal vein ANS: B Decreased liver enzyme activity does not prepare the drug for excretion. The liver size is decreased in older persons; blood flow through the liver is also decreased. DIF: Cognitive Level: Comprehension REF: p. 177 OBJ: 3 TOP: Decreased Liver Function KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 23. A 77-year-old recently admitted to a long-term care facility refuses to join in activities or go to the dining room for meals. How should the nurse interpret this behavior? a. Stubbornness b. Depression c. Fear d. Exhaustion ANS: B Some older people respond to loss by losing their sense of personal identity and fulfillment. They have a deterioration in self-esteem and become depressed. DIF: Cognitive Level: Analysis REF: pp. 175-176 OBJ: 5 TOP: Psychosocial Factors KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. What are included in age-related cardiovascular changes? (Select all that apply.) a. Decreased resting cardiac output b. Increased blood pressure c. Increased risk for heart attack d. Increased coronary blood flow e. Decreased rigidity of the heart ANS: A, B, C Decreased resting cardiac output, increased blood pressure, and increased risk for heart attack are all age-related cardiovascular changes. Coronary blood flow in older adults may be reduced by as much as 35%. The heart becomes increasingly rigid with age. DIF: Cognitive Level: Knowledge REF: p. 171 OBJ: 3 TOP: Cardiovascular Changes KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 11: Falls Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What recommendation should a nurse make to the family of a patient diagnosed with ataxia when preparing discharge to home? a. Remove all scatter rugs from the home. b. Rearrange the bedroom furniture. c. Arrange for someone to stay with the patient 24 hours a day. d. Purchase oversized shoes so that they are easy to get on. ANS: A Scatter rugs can slip and cause a patient to fall. DIF: Cognitive Level: Application REF: p. 186 OBJ: 5 TOP: Fall Prevention KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 2. What should be the first intervention when a nurse finds that a patient has fallen? a. Ask the patient to stand up. b. Document the fall according to agency policy. c. Remove or correct the cause of the fall. d. Assess the circumstances of the fall and any injuries sustained. ANS: D The first implementation should be to assess what happened, determine whether any injuries have occurred, and then document and correct the cause. DIF: Cognitive Level: Application REF: p. 188 OBJ: 6 TOP: Implementations for a Fall KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 3. What should discharge planning for a patient who lives alone and is at high risk for falling include? a. Cannot go home unless someone is with him all the time. b. Must go to a long-term care facility. c. Can wear devices around the neck that can signal for help. d. Needs to be aware of the dangers of living alone. ANS: C A person who is at risk for falling would be wise to have a call system to obtain help from others. Devices worn around the neck that can send signals to a control center are effective and provide a feeling of well-being for the individual who has the potential for falling. DIF: Cognitive Level: Comprehension REF: p. 188 OBJ: 5 TOP: Implementations for a Fall KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 4. A nurse explains that older adults account for a large percentage of the total deaths resulting from falls. What is this percentage? a. 13% b. 27% c. 40% d. 72% ANS: D Older adults constitute only 12% to 13% of the total U.S. population, but they account for 72% of the total deaths resulting from falls. DIF: Cognitive Level: Knowledge REF: p. 181 OBJ: 2 TOP: Incidence of Falls KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 5. A nurse is caring for an older adult patient who has undergone a total hip replacement. What is the best action to reduce the risk of further injury? a. Leave all the lights on in the room at night. b. Leave the side rails down at all times to enable the patient to get to the bathroom quickly. c. Keep the call bell and other frequently used items in easy reach. d. Keep the bed in the high position to discourage the patient from getting out of bed without assistance. ANS: C Keeping the call bell and other frequently used items within easy reach will prevent the patient from having to reach, which increases the risk for falling. DIF: Cognitive Level: Application REF: p. 187 OBJ: 5 TOP: Fall Prevention KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 6. A nurse is talking to the family of a patient who has fallen several times. What is the most important intervention for preventing falls that the nurse to relay to this family? a. Prevention b. Hospitalization c. Continuous observation d. Restraint ANS: A The most important implementation for falls is prevention. The best prevention is education that is aimed toward minimizing intrinsic and extrinsic factors. DIF: Cognitive Level: Comprehension REF: p. 184 OBJ: 5 TOP: Fall Prevention KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 7. How often should a nurse remove and release restraints when caring for a patient who requires wrist restraints? a. Once every 8 hours for at least 30 minutes b. Once every 4 hours for at least 15 minutes c. Once every 2 hours for at least 10 minutes d. Once every 1 hour for at least 5 minutes ANS: C Physical restraints must be removed and released every 2 hours for 10 minutes. In addition, they should be frequently checked to ensure that the restraint is properly used and is providing adequate protection and comfort without impeding circulation or breathing. DIF: Cognitive Level: Knowledge REF: p. 183 OBJ: 4 TOP: Physical Restraints KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. An older adult patient in a long-term care facility is at risk for injury because of confusion. The patient’s gait is stable. What is the best method of restraint to prevent injury to the patient? a. Geriatric chair b. Ambularm bracelet c. Vest restraint d. Wrist or ankle restraint or both ANS: B If a physical restraint is used, the least restrictive device is best. This patient has a stable gait, so the alarm bracelet allows the patient to move about freely while preventing him from leaving the premises. DIF: Cognitive Level: Knowledge REF: pp. 183-184 OBJ: 4 TOP: Physical Restraints KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 9. A nurse is admitting a new patient to the nursing unit. When conducting the admission procedure, what is important for the nurse to ask in order to assess the patient’s risk for falling? a. “How many times have you fallen before?” b. “How many hours do you sleep at night?” c. “What are your eating habits?” d. “Do you smoke?” ANS: A People who are at the greatest risk for falls and injury are those who have fallen before. DIF: Cognitive Level: Application REF: p. 184 OBJ: 3 TOP: Fall Prevention KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 10. A patient has asked a nurse to assist him to ambulate to the bathroom. The nurse is aware that the patient is currently taking an antidepressant medication. What action should the nurse implement? a. Never leave the patient alone in his room. b. Ask the patient if he could use the bedside commode instead of going to the bathroom. c. Make suicidal precautions part of the care plan. d. Ask the patient to sit on the side of the bed for a minute or two before standing and then stand slowly. ANS: D Psychotropic drugs, such as antidepressants, commonly cause orthostatic hypotension. The patient should sit on the side of the bed and then stand slowly to prevent falling. DIF: Cognitive Level: Application REF: p. 184 OBJ: 3 TOP: Chemical Restraints KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 11. In reviewing a patient’s medication administration record, a nurse is aware that some medications are considered to be chemical restraints. Which medication is considered a chemical restraint? a. Warfarin (Coumadin) b. Alprazolam (Xanax) c. Isosorbide (Isordil) d. Ibuprofen (Motrin) ANS: B Alprazolam (Xanax) is a psychotropic drug used as a chemical restraint. DIF: Cognitive Level: Knowledge REF: p. 184|p. 186 OBJ: 4 TOP: Chemical Restraints KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. A nurse in a long-term care facility determines the need to place a vest restraint on a patient. The patient does not want the vest restraint applied. What nursing action should be implemented? a. Apply the restraint anyway. b. Call the physician and obtain an order for the restraint. c. Medicate the patient with a sedative and then apply the restraint. d. Compromise with the patient and use wrist restraints. ANS: B A physician’s order is required for restraint use, and the order must specify the duration and circumstances under which the restraint may be used. DIF: Cognitive Level: Application REF: p. 182 OBJ: 4 TOP: Physical Restraints KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 13. What is the most appropriate nursing intervention after a patient has fallen? a. Apply a vest restraint. b. Have the patient begin ambulating as soon as possible. c. Administer haloperidol (Haldol) as prescribed or as needed. d. Apply wrist restraints. ANS: B The patient should begin ambulating as soon after a fall as possible to prevent the hazards of bed rest and to restore confidence. Applying restraints after a fall is tempting, but avoiding their use, if possible, is best. DIF: Cognitive Level: Application REF: p. 188 OBJ: 6 TOP: Implementations for a Fall KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 14. Which unexpected circumstance best defines a fall? a. Falls to the ground, floor, or lower level b. Loses consciousness, resulting in injury c. Loses balance, resulting from a lack of equilibrium d. Injures self, resulting from a side effect of a medication ANS: A Definitions of falls vary, but a fall is an unintentional event that is unrelated to medication or loss of consciousness and that results in injury. DIF: Cognitive Level: Knowledge REF: p. 181 OBJ: 1 TOP: Falls KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 15. A nurse is assessing the potential risk factors a patient may have for falling. Which two major factors cause falls? a. Mental and emotional factors b. Aging and physical factors c. Genetic and environmental factors d. Intrinsic and extrinsic factors ANS: D Intrinsic factors are related to the functioning of the individual (e.g., aging process, physical illness). Extrinsic factors are related to the environment. DIF: Cognitive Level: Knowledge REF: p. 181 OBJ: 2 TOP: Incidence of Falls KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 16. The Omnibus Reconciliation Act (OBRA) was enacted to protect patients from unnecessary restraint in long-term care facilities. According to OBRA regulations, what is a permissible reason to restrain a patient? a. Staffing level is inadequate, and nurses are unable to check on the patient at regular intervals. b. The patient is verbally abusive to the nursing staff. c. The patient is at an extremely high risk for a fall that is life threatening. d. Medical procedures cannot be performed because the patient is not being cooperative. ANS: C The only people who are considered restrainable are those who (1) are at high risk for a fall that is life threatening; (2) need postural support for safety, comfort, or both; (3) may be a serious hazard to themselves, objects, or others; and (4) have life-threatening medical symptoms and for whom a restraint may be temporarily used to provide necessary treatment. DIF: Cognitive Level: Comprehension REF: pp. 182-183 OBJ: 4 TOP: Restraints KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 17. Which patient population is at greatest risk for injury from falls? a. Toddler b. Teenager c. Middle-aged adult d. Older adult ANS: D Older adults are at particular risk for accidents because of changes brought about by aging, a greater potential for injury, and poorer clinical outcomes. DIF: Cognitive Level: Comprehension REF: p. 181 OBJ: 3 TOP: Risk of Falls KEY: Nursing Process Step: Analysis MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 18. Where should a patient with a visual impairment of the left eye place items that are frequently used to prevent the risk of injury? a. On the patient’s left side b. In the patient’s bathroom c. In the patient’s closet d. On the patient’s right side ANS: D The unaffected side and within reach. This placement reduces the risk of falling. DIF: Cognitive Level: Application REF: p. 185 OBJ: 5 TOP: Fall Prevention KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 19. An older adult patient with osteoporosis is at risk for falls. What should a nurse advise the patient to do in order to maintain safety in the home? a. Take the rubber mat out of the shower. b. Install a grab rail in the bath and shower and by the toilet. c. Avoid rubber-soled shoes. d. Avoid exercise. ANS: B The patient who is at risk for falls must have rails to hold to prevent falling. A rubber mat in the shower and rubber-soled shoes are important to prevent slipping. Moderate exercise is beneficial. DIF: Cognitive Level: Comprehension REF: p. 187 OBJ: 5 TOP: Fall Prevention KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 20. A nurse assesses a resident in a long-term care facility with the “get up and go” technique. What should this involve observing the resident do? a. Walk carefully through a cluttered area without incident. b. Rise from the bed, and go to the bathroom. c. Sit and rise from an armless chair. d. Ambulate in a straight line for 1 foot. ANS: C The “get up and go” technique of evaluation requires that the resident be able to sit and rise from an armless chair. DIF: Cognitive Level: Comprehension REF: p. 186 OBJ: 5 TOP: Fall Prevention KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 21. A nurse is discussing the risk of falling with the family of a 75-year-old patient. The family asks, “Why are you so worried about her falling? She falls all the time and doesn’t get hurt much.” To which fact should the nurse’s response relate? a. Falls are the most frequent cause of accidental injury and death among older adults. b. Worrying is probably unnecessary because she hasn’t been hurt in the past. c. Falls usually occur in institutional settings. d. Falls by older adults are not preventable. ANS: A The risk of injury from falls is highest in people older than 65 years, and falls are the most frequent cause of accidental injury and death among older adults. Older adults account for 72% of total deaths resulting from falls. DIF: Cognitive Level: Comprehension REF: p. 181 OBJ: 2 TOP: Incidence of Falls KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 22. A nurse visiting a patient in the patient’s home assesses the environment for extrinsic risk factors for falling. Which factors should the nurse have the patient or family correct? a. No door thresholds are present. b. The kitchen floor is clean, shiny, and slick. c. Lamps have 60-watt bulbs. d. The telephone is placed on the bedside table. ANS: B Slick floors can cause the patient to slip and fall. The other choices are implementations that will help reduce the risk of falls. DIF: Cognitive Level: Comprehension REF: p. 186 OBJ: 3 TOP: Fall Prevention KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 23. A nurse is teaching a patient methods for getting up after a fall. The nurse instructs the patient to pull up to a sitting position on the floor, shuffle the buttocks to a nearby piece of furniture, and pull up on the knees in front of the furniture. What should the nurse instruct the patient to do next? a. Stand up. b. Place hands on the floor for leverage. c. Pivot so that the furniture is behind the body. d. Sit back down. ANS: A The last step of the shuffle method is to stand up. DIF: Cognitive Level: Application REF: p. 188 OBJ: 6 TOP: Getting Up after a Fall KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control 24. A nurse is aware that many residents in a long-term care facility refuse to wear the hip protector garment. What reason do residents state makes them resistive to wear this protective garment? a. It is uncomfortable. b. It is too expensive. c. It is degrading. d. It is too easily soiled. ANS: A Residents resist wearing the hip protector garment because it is uncomfortable. DIF: Cognitive Level: Knowledge REF: p. 188 OBJ: 3 TOP: Hip Protector Garment KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 25. What should the home health nurse recommend to a patient if a fall occurs at home? a. Assume a crawling position and push up from the floor. b. Pull self up using sturdy furniture. c. Roll to a doorway and pull up using the door knob. d. Place the right foot flat on floor and push up on the right knee. ANS: B All techniques for rising after a fall rely on pulling up on sturdy furniture. DIF: Cognitive Level: Comprehension REF: p. 188 OBJ: 6 TOP: Rising after a Fall KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 26. A nurse is trying to keep a confused resident from removing a feeding tube by following the “rule of least restriction.” What should replace the wrist restraint? a. Mittens b. Vest restraint c. Administration of a mild sedative d. Tightly tucked sheet ANS: A Mittens are the lesser of restraints that will hinder the patient from removing the feeding tube. DIF: Cognitive Level: Knowledge REF: p. 183 OBJ: 7 TOP: Restraints KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. In what ways might people who have a fear of falling alter their lifestyle? (Select all that apply.) a. Restrict physical activities. b. Restrict social activities. c. Become more dependent. d. Have increased need for residency in a long-term care facility. e. Become depressed. ANS: A, B, C, D Restricting physical and social activities, becoming more dependent, and having an increased need for residency in a long-term-care facility all have to do with an altered lifestyle. The development of depression is not a lifestyle alteration but may be a result of the lifestyle change. DIF: Cognitive Level: Comprehension REF: p. 181 OBJ: 3 TOP: Fear of Falls KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 2. A home health nurse cautions the family of a frail 82-year-old woman about the intrinsic factors that may be a potential cause of injury. Which intrinsic factors should be included? (Select all that apply.) a. Diminished vision b. Pet cats c. Cluttered bedroom d. Wearing loose house slippers e. Generalized weakness ANS: A, E Diminished vision and generalized weakness are the only options related to the individual that cannot be changed (intrinsic). The other options are related to the environment and can be changed (extrinsic). DIF: Cognitive Level: Comprehension REF: pp. 181-182 OBJ: 5 TOP: Intrinsic Factors KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Safety and Infection Control COMPLETION 1. A nurse is aware that of all the reported falls in the United States, only 1% to 5% result in a . ANS: fracture According to reported falls, only 1% to 5% result in a fracture. DIF: Cognitive Level: Knowledge REF: p. 182 OBJ: 2 TOP: Incidence KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. A nurse helps the physical therapist teach residents in a long-term care facility how to diminish the risk of injury from a fall by teaching them rotation maneuvers to help them avoid falling . ANS: sideways Rotation maneuvers can be taught to patients to help them avoid falling sideways. DIF: Cognitive Level: Knowledge REF: p. 188 OBJ: 5 TOP: Fall Prevention KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Coordinated Care 3. A nurse suggests that a resident who is at risk for falling come to the class to improve balance. ANS: Tai Chi The slow rhythmic movements of Tai Chi are helpful in improving balance. DIF: Cognitive Level: Knowledge REF: p. 184 OBJ: 9 TOP: Tai Chi KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 12: Immobility Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What negative effects does immobilization have on the musculoskeletal system? a. Demineralization of bone b. Increase in aerobic capacity c. Increased muscle oxidation d. Lengthening of muscle fibers ANS: A Immobilization has negative effects on the musculoskeletal system such as demineralization of bone, a decrease in aerobic capacity, a decrease in muscle oxidation, and shortening of muscle fibers. DIF: Cognitive Level: Comprehension REF: p. 192 OBJ: 1 TOP: Effects of Immobility KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. What should the nurse be aware is the best prevention of immobility-related disorders? a. Dietary supplements b. Fluids c. Adequate fiber d. Exercise ANS: D Exercise will help reduce the patient’s risk of immobility-related disorders. DIF: Cognitive Level: Knowledge REF: pp. 193-194 OBJ: 2 TOP: Preventing Complications of Immobility KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A nurse’s assessment reveals an area of erythema on an immobilized patient’s sacrum. What is the initial nursing action? a. Apply a wet-to-dry dressing. b. Massage the reddened area. c. Reposition the patient. d. Rub the area with alcohol. ANS: C The first intervention is to reposition the patient with follow-up to ensure that the patient is repositioned often. DIF: Cognitive Level: Application REF: p. 198 OBJ: 5 TOP: Treatment of Pressure Ulcers KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. A nurse is providing discharge instructions to the family of an older adult patient who is unable to get out of bed. What should the nurse instruct the family regarding the most effective way to prevent urinary incontinence associated with immobility? a. Use absorbent underpads. b. Set up a toileting program. c. Restrict fluid intake to 500 mL per 24 hours. d. Restrict fluids after dinner and throughout the night. ANS: B Patients should have scheduled toileting times with adjustments in the schedule based on the patient’s voiding patterns. Studies have been inconclusive regarding the effectiveness of limiting fluids. DIF: Cognitive Level: Application REF: p. 201 OBJ: 6 TOP: Urinary Incontinence KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. The care plan of an older adult patient states that the patient should be monitored while in the bathroom because of a history of vasovagal reflex. What should the nurse assess with this patient? a. Extremely elevated blood pressure after ambulation b. Nausea and vomiting after a meal c. Lightheadedness and fainting during defecation d. Inability to urinate ANS: C Constipated individuals may strain to defecate, causing an increase in intra-abdominal pressure. This is called the Valsalva maneuver or vasovagal reflex, and it can lead to cardiovascular alterations. DIF: Cognitive Level: Comprehension REF: p. 200 OBJ: 6 TOP: Vasovagal Reflex KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. What is the most effective intervention to prevent constipation in a patient who recently sustained a fractured femur and is currently in traction? a. Get the patient up and to the bathroom at least twice each day. b. Administer enemas each day until the patient has a bowel movement. c. Administer pain medication to prevent pain during defecation. d. Encourage a high-fiber diet and increased amounts of fluids. ANS: D Inactivity, decreased fluid intake, and a lack of adequate fiber in the diet can combine to cause constipation. Activity is not an option for this patient, but encouraging a high-fiber diet and increased fluids can help prevent or relieve constipation. DIF: Cognitive Level: Application REF: p. 200 OBJ: 6 TOP: Constipation KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A nurse caring for a patient who has been prescribed bed rest for 1 week notices a reddened area on the patient’s left hip. The skin is intact, but when the nurse presses on the area, the redness does not fade. How should this area of pressure be classified? a. Stage I b. Stage II c. Stage III d. Stage IV ANS: A The major characteristic of a stage I pressure ulcer is erythema (redness) that does not blanch when pressed. DIF: Cognitive Level: Analysis REF: p. 198 OBJ: 4 TOP: Stages of Pressure Areas KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. What action should the nurse implement when positioning an immobile patient? a. Ensure that the patient’s knees and hips are flexed. b. Visualize how a person looks while standing and try to have the patient achieve that position while lying down. c. Reposition the patient no more often than every 4 hours. d. Always position the patient on his or her back with the head raised to prevent aspiration. ANS: B Positioning should be done to maintain joints in their functional positions so they are not abnormally flexed or extended. DIF: Cognitive Level: Application REF: p. 195 OBJ: 2 TOP: Positioning KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. What intervention is most appropriate to prevent respiratory complications resulting from immobility? a. Suction every 4 to 6 hours. b. Administer pain medications as frequently as possible. c. Teach the patient the technique of pursed lip breathing. d. Reposition the patient, and encourage him or her to cough and deep breathe at least every 2 hours. ANS: D When a person remains immobile or does not take deep breaths, thick secretions can accumulate and pool in the lower respiratory structures. DIF: Cognitive Level: Application REF: p. 199 OBJ: 6 TOP: Respiratory Complications KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 10. A nurse transcribes a discharge order for the patient with left-sided weakness after having a stroke indicating to teach the patient to perform range-of-motion exercises on affected extremities. The patient asks why she needs to do range-of-motion exercises. What is the nurse’s best response? a. “Because the physician has ordered it.” b. “You will regain full use of your arm and leg if you will do the exercises correctly.” c. “They prevent the muscles and tendons from shortening and becoming unmoveable.” d. “It will give you something to do because you can’t work anymore.” ANS: C Muscular activity maintains range of motion by allowing the joint to remain flexible and functional. When little or no movement of a joint occurs, the muscles shorten and lose their elasticity. DIF: Cognitive Level: Application REF: p. 194 OBJ: 2 TOP: Exercises KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. A nurse assesses a patient’s risk for developing a pressure ulcer using the Norton scale. The patient’s score is 18. What nursing action should be implemented? a. Call the physician immediately. b. Implement a pressure ulcer prevention program. c. Document the score. d. Order an alternating air mattress. ANS: C If the total score on the Norton scale is greater than 14, then little risk exists for the development of pressure ulcers. If the total score is less than 14, then significant risk exists. DIF: Cognitive Level: Application REF: p. 195 OBJ: 3 TOP: Norton Scale KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. A patient in traction with a fractured hip is diagnosed with a stage I pressure ulcer. She asks the nurse how a pressure ulcer could occur after only 2 days of immobility. On what knowledge should the nurse base a response? a. “Erythema can occur in 1 to 2 hours even in a person with healthy skin and adequate circulation.” b. “It takes several days for a pressure ulcer to form.” c. “The pressure ulcer probably occurred when you fell.” d. “The cause of pressure ulcers isn’t really known.” ANS: A Because of impaired blood flow, capillaries in the area of pressure can become congested, and erythema can occur in 1 to 2 hours. DIF: Cognitive Level: Comprehension REF: p. 195 OBJ: 3 TOP: Pressure Ulcers KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. A patient is complaining to the nurse that he feels the need to have a bowel movement but has not been able to defecate. He has had cramping and even a small amount of brown watery stool. What should the nurse recognize these symptoms as? a. Diarrhea b. Fecal incontinence c. Fecal impaction d. Flatulence ANS: C Symptoms of a fecal impaction include painful defecation, a feeling of fullness in the rectum, abdominal distention, and sometimes cramps and a watery stool. DIF: Cognitive Level: Comprehension REF: p. 200 OBJ: 6 TOP: Fecal Impaction KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. During the shift report, a nurse is told that a patient she will be caring for has a stage II pressure ulcer. What should the nurse expect to visualize during the dressing change? a. Ulcer that appears black with possible signs of infection b. Shallow ulcer that appears blistered, cracked, or abraded c. Craterlike sore with a distinct outer margin formed as the epidermis thickens and rolls over the edge toward the ulcer base d. Redness of skin with no ulceration ANS: B In a stage II pressure ulcer, some skin loss in the epidermis and dermis has occurred. DIF: Cognitive Level: Comprehension REF: p. 198 OBJ: 4 TOP: Stages of Pressure Ulcers KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 15. When preparing a plan care for an older adult patient, a nurse should consider the common problems associated with immobility. What should these problems be classified as? a. Environmental and intellectual b. Internal and external c. Mental and medical d. Physical and psychosocial ANS: D Immobility can have a profound impact on both the mind and the body. Psychosocial problems include depression, fear, anxiety, social withdrawal, and apathy. Physically, immobility can have an adverse effect on every body system. DIF: Cognitive Level: Comprehension REF: p. 191 OBJ: 1 TOP: Problems Associated with Immobility KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 16. How does the National Pressure Ulcer Advisory Panel prefer to refer to skin breakdown? a. Bed sores b. Pressure ulcers c. Decubitus ulcers d. Decubiti ANS: B Decubitus means lying down; therefore, decubitus ulcers and bed sores are associated with lying in a bed. Skin breakdown can also develop from sitting. DIF: Cognitive Level: Knowledge REF: p. 198 OBJ: 1 TOP: Pressure Ulcers KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 17. A patient complains that his “bottom” is sore. The nurse assesses the area and finds an open area on the sacrum that appears blistered. What action should the nurse implement? a. Document the cause of the burn. b. Clean with alcohol, apply moisturizer, and cover with a set dressing. c. Massage the area to promote circulation. d. Clean with mild soap, dry, and apply a light dressing. ANS: D If pressure ulcers develop despite all preventive measures, proper and early treatment improves the chance for reversal. A stage II ulcer should be cleaned with mild soap and water or with sterile normal saline, patted dry, and covered with a dressing that allows airflow. DIF: Cognitive Level: Application REF: p. 196 OBJ: 5 TOP: Pressure Ulcers KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 18. A nursing assistant is bathing a patient who has a stage I pressure ulcer on the right shoulder. What action by the health care team could cause that the tissue to become more damaged? a. Positioning the patient on the left side b. Massaging the reddened area c. Cleaning the area with mild soap and water d. Positioning the patient in a prone position ANS: B Any type of massage around or on a reddened area of skin can damage fragile capillaries. DIF: Cognitive Level: Comprehension REF: p. 197 OBJ: 5 TOP: Treatment of Pressure Ulcers KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 19. A nurse is planning the care of a patient who is immobile. Why should the nurse consider this patient to be at risk for urinary tract infection? a. Urine will pool in the bladder when the patient remains in a supine position. b. The patient is likely to have urinary incontinence. c. The patient’s appetite may be decreased. d. The patient may not be able to move quickly enough to get to the bathroom. ANS: A If the body remains in a supine position for even a few days, the flow becomes sluggish, and the urine pools in the bladder, which will increase the risk of a urinary tract infection. DIF: Cognitive Level: Comprehension REF: p. 201 OBJ: 6 TOP: Urinary Tract Infection KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 20. What should the nurse instruct a patient in a wheelchair to do to decrease risk for pressure ulcers? a. Use a ring pillow on the seat of the chair. b. Lift the weight of the body using the arms of the wheelchair every 15 minutes. c. Scoot forward and back in the seat to stimulate circulation. d. Wear underwear that holds moisture close to skin. ANS: B Using the arms of the wheelchair to lift the weight off the buttocks and coccyx is beneficial to reduce the risk of pressure ulcers in patients using wheelchairs. DIF: Cognitive Level: Comprehension REF: p. 193 OBJ: 5 TOP: Pressure Ulcer in a Wheelchair KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 21. A nurse is instructing a patient on performing isometric exercises. What instruction should the nurse include? a. Contract the muscle for several seconds, then relax the muscle for a few seconds, and contract it again. b. Perform full range-of-motion exercises of each joint. c. Have a family member perform full range-of-motion exercises on each of the patient’s joints. d. Stand in front of a wall and push with the arms without bending the elbow. ANS: A Isometric exercises maintain muscle tone without moving the joint. This type of exercise is helpful in maintaining muscle strength after a fracture. DIF: Cognitive Level: Comprehension REF: p. 194 OBJ: 2 TOP: Isometric Exercises KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 22. A nurse is talking with a patient who recently became paraplegic as a result of a cervical spinal cord injury. When some home equipment is discussed, the patient becomes angry and says, “I don’t need to worry about any kind of home equipment.” What is the best response by the nurse? a. “I know you will be walking soon, but you may need some equipment until then.” b. “There is very little chance that you will ever walk.” c. “Tell me what it is about this equipment that bothers you.” d. “Let me call the physician to come explain your injuries to you.” ANS: C The nurse should use therapeutic communication techniques to explore the patient’s feelings. DIF: Cognitive Level: Application REF: p. 191 OBJ: 1 TOP: Therapeutic Communication KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 23. During a skin integrity assessment, a nurse notices an area on the right heel that is black and draining purulent, foul-smelling exudate. How should the nurse document this as a pressure ulcer? a. Stage I b. Stage II c. Stage III d. Stage IV ANS: D In a stage IV pressure ulcer, full-thickness skin loss has occurred with extensive destruction of the deeper underlying muscle and, possibly, the bone tissue. DIF: Cognitive Level: Analysis REF: p. 198 OBJ: 4 TOP: Stages of Pressure Ulcers KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 24. What is the classification of incontinence in older adults related to the inability to get to the bathroom in time? a. Stress incontinence b. Urge incontinence c. Functional incontinence d. Sporadic incontinence ANS: C Functional incontinence occurs when the older adult patient cannot move quickly enough to reach the toilet in time. DIF: Cognitive Level: Knowledge REF: p. 201 OBJ: 6 TOP: Functional Incontinence KEY: Nursing Process Step: N/A MSC: NCLEX: N/A MULTIPLE RESPONSE 1. Which are characteristics of a stage I pressure ulcer? (Select all that apply.) a. The area is regular and well defined. b. Tissue hardening is present. c. Swelling has occurred at the site. d. The condition is reversible. e. Nonblanching erythema is observed. ANS: B, C, D, E A stage I ulcer has irregular and poorly defined margins, with swelling and hardening at the site of the nonblanching erythema. At this stage, the ulcer is reversible. DIF: Cognitive Level: Knowledge REF: p. 197 OBJ: 4 TOP: Characteristics of Stage I Pressure Ulcer KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. What should a nurse document when assessing a new pressure ulcer? (Select all that apply.) a. Precise measurement of the ulcer b. Location of the wound and its description c. Color of the ulcer d. Amount and characteristics of the drainage e. Probable cause of the ulcer ANS: A, B, C, D Documentation should include the precise location, color, size, shape, and drainage, as well as treatment applications. DIF: Cognitive Level: Comprehension REF: p. 197 OBJ: 5 TOP: Documentation of Pressure Ulcers KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 3. What therapeutic reasons exist that explain why a patient might become immobile? (Select all that apply.) a. Reduction of the workload of the heart b. Fear of falling c. Reversal of the effects of gravity d. Bereavement e. Healing of a fracture ANS: A, C, E A reduction of the heart’s workload, a reversal of the effects of gravity (as in the treatment of a hernia or prolapse), and the healing of a fracture are all therapeutic reasons for immobilization. The fear of falling and bereavement are not therapeutic reasons. DIF: Cognitive Level: Comprehension REF: p. 191 OBJ: 1 TOP: Therapeutic Rationale for Immobilization KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. A home health nurse instructs a family about boosting the patient in bed so that a(n) type of skin injury will not occur. ANS: shearing force Shearing force injuries occur when a patient is dragged up in bed, causing the skin to be abraded against the bed linens. DIF: Cognitive Level: Knowledge REF: p. 195 OBJ: 3 TOP: Shear Force KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance 2. A nurse evaluates the effectiveness of the treatment for a stage III pressure ulcer as satisfactory when the bed of the ulcer is pink, indicating the presence of , which is an indicator of tissue perfusion. ANS: granulation tissue The appearance of healthy pink granulation tissue in the bed of a pressure ulcer is a positive sign for improved perfusion and the beginning of closure. DIF: Cognitive Level: Knowledge REF: p. 199 OBJ: 5 TOP: Presence of Granulation Tissue KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A nurse takes into consideration that such emotions as worry, anxiety, and depression can contribute to the common nutritional problem of . ANS: anorexia Anorexia can be caused by emotional factors such as worry, anxiety, and depression. DIF: Cognitive Level: Knowledge REF: p. 200 OBJ: 6 TOP: Anorexia KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. When bacteria are localized at the site of a stage III pressure ulcer, it is said to be . ANS: colonized Colonized bacteria are those who are in one location, such as an ulcer, and not systemic. DIF: Cognitive Level: Knowledge REF: p. 199 OBJ: 4 TOP: Colonization of bacteria KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 5. The negative impact of immobilization on a patient depends on the duration, degree, and type of . ANS: mobility limitation Duration, degree, and type of mobility limitation have the greatest impact. The other choices may affect the impact of immobilization when the mobility limitation becomes an issue. DIF: Cognitive Level: Knowledge REF: p. 192 OBJ: 2 TOP: Impact of Immobility KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 13: Delirium and Dementia Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. The family of a patient with Alzheimer disease asks the nurse, “When will my mother quit being so confused?” On what information regarding dementia should the nurse base a response? a. It is a short-term confusional state that is typically reversible. b. It is a state of confusion caused primarily by medications. c. It is a state of confusion that usually begins abruptly and lasts a short period. d. It is a syndrome that is chronic and irreversible. ANS: D Alzheimer disease is a type of dementia that is chronic and irreversible. Delirium is a short-term confusional state that has a sudden onset and is typically reversible. DIF: Cognitive Level: Knowledge REF: p. 205 OBJ: 2 TOP: Dementia KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Basic Care and Comfort 2. A nurse is admitting a patient who has been diagnosed as having confusion. What is the most important observation that the nurse should make regarding this patient? a. Eating, drinking, and sleeping patterns b. Behavior, orientation, memory, and sleeping habits c. Urinary and bowel elimination habits d. Talking, walking, and sleeping patterns ANS: B The first step in assessing a confusional state is to observe the patient’s behavior, orientation, memory, and sleeping habits. DIF: Cognitive Level: Comprehension REF: p. 206 OBJ: 6 TOP: Confusion Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 3. While a nurse is dressing a patient who has dementia as a result of Huntington disease, the patient states, “I don’t want to wear clothes today” and begins to resist help putting on her clothes. What is the nurse’s most appropriate action? a. Tell the patient that she must wear clothes or she cannot see her family later. b. Get another nurse to help her force the patient to get dressed. c. Talk to the patient about her family coming this afternoon and continue to assist the patient gently with dressing. d. Let the patient go without clothes but make her stay in her room. ANS: C When patients with dementia resist activities such as bathing or dressing, avoiding confrontations and diverting their attention elsewhere are best. DIF: Cognitive Level: Application REF: p. 211 OBJ: 6 TOP: Resisting Care KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 4. What are the adaptations to interventions that the Cognitive Developmental Approach (CDA) to caring for patients with dementia designed to achieve? a. Increase cognitive abilities. b. Adapt environment to patient. c. Offer a wide variety of choices. d. Abolish irrational fears. ANS: B The CDA adapts implementations based on the patient’s cognitive abilities as they are, modifies the environment, and offers limited choices. DIF: Cognitive Level: Knowledge REF: p. 211 OBJ: 6 TOP: Cognitive Developmental Approach KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 5. A nurse is gathering information from the family of a patient who is experiencing confusion. What important question should the nurse ask the family? a. “Are you sure she is confused? Maybe she just didn’t hear what you were saying.” b. “When did you first think she might be confused? Tell me exactly what happened.” c. “Did something bad happen to her during her childhood?” d. “How can you say she is confused? She knows who she is.” ANS: B Family members may be able to provide helpful information when the patient cannot. The nurse should ask when the symptoms of confusion started and whether the confusion is constant or intermittent. DIF: Cognitive Level: Application REF: p. 206 OBJ: 6 TOP: Assessing Confusion KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity 6. The family of a patient with dementia expresses concern to the nurse about the patient wandering at night. They are afraid that the patient might get up while they are sleeping and go outside. What is the best advice for the nurse to provide? a. Apply a vest restraint at night. b. Perform constant reality orientation. c. Learn some behavior modification techniques. d. Put new locks on the outside doors in new places. ANS: D Take advantage of the fact that patients with dementia are usually unable to learn new things. They will probably not be able to figure out how to work a new lock. DIF: Cognitive Level: Application REF: p. 211 OBJ: 6 TOP: Dementia Safety KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 7. A nurse is planning for the nutritional needs of a patient with Alzheimer disease. What is the best plan to have the dietary department provide? a. Pureed diet to be fed with a syringe b. Foods that the patient can cut up to keep busy and not lose interest in eating c. Finger foods several times a day d. High-protein liquid diet ANS: C Small, frequent meals are less confusing to patients. Finger foods high in protein and carbohydrates allow patients to feed themselves more easily. DIF: Cognitive Level: Comprehension REF: p. 209 OBJ: 6 TOP: Nutritional Needs KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. What initial nursing action should be implemented when assisting a patient with dementia to dress? a. Hand the patient her clothes and ask her to put them on. b. Hand the patient each article of clothing separately and ask her to put it on. c. Assist her with each article, giving specific instructions such as, “Put your arm in this hole.” d. Put the patient’s clothes on without assistance from the patient. ANS: C The goal should be to maintain the highest level of functioning possible, but tasks must be broken down into individual steps to be performed one at a time. DIF: Cognitive Level: Application REF: p. 209 OBJ: 6 TOP: Self-Care Needs KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 9. Reality orientation is helpful for some patients with confusion. What patient diagnosis is most appropriate for the nurse to implement this technique? a. Organic brain syndrome b. Senile dementia c. Senility d. Acute confusional state (delirium) ANS: D Acute confusional state is another name for delirium. The other choices are other names for dementia. Reality orientation may be helpful for patients with delirium but tends to agitate patients with dementia. DIF: Cognitive Level: Comprehension REF: p. 208 OBJ: 6 TOP: Reality Orientation KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 10. A nurse is assessing a patient for the possibility of confusion. What two major types of confusion should the nurse be aware of to appropriately assess this patient? a. Acute and chronic senility b. Temporary and permanent confusion c. Delirium and dementia d. Senility and senile dementia ANS: C The two major types of confusion are acute confusional states, or delirium, and chronic confusion dementia. DIF: Cognitive Level: Knowledge REF: p. 203 OBJ: 1 TOP: Types of Confusion KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 11. A patient with delirium repeatedly cries out for her husband. What is the most appropriate initial nursing intervention? a. Administer Haldol as ordered. b. Apply restraints so that the patient will not harm herself. c. Calmly tell the patient that she is in the hospital and that her husband is not there. d. Call the husband and tell him that he needs to come and stay with his wife. ANS: C Anyone dealing with a delirious patient should be calm, warm, and reassuring. Frequent orientation to the surroundings and situation is important as well. DIF: Cognitive Level: Application REF: p. 208 OBJ: 6 TOP: Delirium KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 12. When admitting a patient who has recently become confused, the nurse asks the family for a list of all the medications that the patient is currently taking. Which medication identified by the family should the nurse be aware could be causing confusion? a. Amoxicillin b. Acetaminophen c. Furosemide d. Digoxin ANS: D Drugs that most commonly cause confusion include anticholinergics, digoxin, histamine-2 receptor blockers, benzodiazepines, nonsteroidal anti-inflammatory drugs, and many antiarrhythmic and antihypertensive medications. DIF: Cognitive Level: Comprehension REF: p. 206 OBJ: 3 TOP: Confusion Due to Medications KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 13. A patient has been admitted with a diagnosis of confusion. The physician’s admission note states that he wants to assess for delirium versus dementia. What should the nurse be aware that the main differences include? a. Whereas delirium usually lasts several years, dementia lasts only a few days. b. Whereas delirium usually has sudden onset and is reversible, dementia is chronic and irreversible. c. Whereas dementia is usually caused by medications, delirium is not. d. Whereas dementia is easily treated with reality orientation, delirium is not. ANS: B Delirium is a short-term, confusional state that has a sudden onset and is typically reversible. Dementia is a syndrome that is often chronic and irreversible. DIF: Cognitive Level: Knowledge REF: pp. 203-206 OBJ: 4 TOP: Delirium versus Dementia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Psychosocial Adaptation 14. A nurse has found a patient with delirium in other patients’ rooms several times. What is the best action by the nurse? a. Firmly tell the patient that he must stay out of other patients’ rooms and tell him to return to his room. b. Take him back to his room and put him in bed with the side rails up. c. Take him to the nurses’ station and let him visit for a while. d. Administer a dose of lorazepam (Ativan) as ordered. ANS: C Avoid using physical restraints, which tend to increase anxiety and agitation. Sitting at the nurses’ station will allow the nurses to monitor his activity and frequently orient him to his surroundings. DIF: Cognitive Level: Application REF: p. 208 OBJ: 6 TOP: Delirium KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 15. A nurse in a long-term care facility is taking patients to the dining room for lunch. She asks the patient who has been diagnosed with delirium if she is ready to go eat lunch. The patient does not respond. What should be the nurse’s next action? a. Take the patient by the arm and lead her to the dining room. b. Assist the patient to bed and bring her lunch to her. c. Tell the patient that she can go to the dining room whenever she gets hungry. d. Ask the patient again if she is ready to go eat lunch. ANS: D A patient with delirium may have difficulty focusing or paying attention, and questions must often be repeated several times. DIF: Cognitive Level: Application REF: p. 203 OBJ: 6 TOP: Communication KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 16. A patient asks a nurse what causes dementia. What two most prevalent types of dementia should the nurse consider before responding? a. Pick disease and Huntington disease b. Alzheimer disease and vascular dementia c. Creutzfeldt-Jakob disease and Pick disease d. Vascular dementia and Huntington disease ANS: B Alzheimer disease and vascular dementia are the two most prevalent types of dementia. DIF: Cognitive Level: Knowledge REF: p. 205 OBJ: 2 TOP: Types of Dementia KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Psychosocial Adaptation 17. A nurse is assessing a patient for delirium versus dementia. What should the nurse expect the patient with dementia to display? a. Intermittent fear affect b. Perplexity affect c. Bewilderment affect d. Flat affect ANS: D The patient with dementia will have a flat or indifferent affect. The other three choices would be presented by a patient with delirium. DIF: Cognitive Level: Comprehension REF: p. 207 OBJ: 4 TOP: Dementia Affect KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 18. A nurse is taking a patient who has Alzheimer disease to the bathing room for a tub bath. The patient states, “Please don’t make me take a bath today. I am so afraid that I will be washed down the drain.” What is the nurse’s best response? a. “Don’t be silly; there’s no way you would fit in the drain.” b. “I am your nurse, and I will stay with you, so you shouldn’t be afraid of your bath.” c. “Let’s go back to your room, and I will bathe you there.” d. “Today is your day for a bath.” ANS: C The nurse should recognize irrational fears and arrange alternative ways to give personal care. DIF: Cognitive Level: Application REF: p. 208 OBJ: 6 TOP: Alzheimer Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 19. Which characteristics are most likely to be present in the patient with dementia? a. Forgets things relatively quickly and is usually unable to learn new things b. Can remember new tasks but will forget any previously taught tasks c. Cannot learn new information but will probably remember anything you ask about the past d. Responds well to reality orientation and needs to have a flexible schedule ANS: A Keeping in mind the following two important concepts when taking care of patients with dementia is helpful: (1) they usually forget things relatively quickly, and (2) they are usually unable to learn new things. DIF: Cognitive Level: Comprehension REF: p. 211 OBJ: 1 | 4 TOP: Dementia KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 20. A patient is displaying confusion, which began very suddenly and lasted less than 1 week. What should the nurse suspect is present? a. Dementia b. Delirium c. Symptoms of Huntington disease d. Senile dementia ANS: B Delirium begins abruptly and generally lasts a short period. It usually lasts 1 week and rarely lasts longer than 1 month. DIF: Cognitive Level: Comprehension REF: p. 203 OBJ: 4 TOP: Acute Confusion KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 21. A nurse is preparing a room for a patient being transferred from the emergency department with a diagnosis of delirium. What should the nurse ensure in regard to the room? a. Brightly lit b. Shared by another patient c. Visible from the nurses’ station d. Dark and quiet ANS: C The patient should be in a private room with continual supervision. The room should be quiet and uncluttered, and lighting should be soft and diffuse to avoid shadows. DIF: Cognitive Level: Comprehension REF: p. 211 OBJ: 6 TOP: Environmental Consideration KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 22. A nurse caring for a patient with dementia notices that the patient stays awake most of the night. What is the nurse’s most appropriate action? a. Give a prescribed sleeping medication. b. Tell the patient that it is nighttime and that she must go to sleep. c. Check the patient’s record to see whether she is sleeping during the day. d. Put the patient to bed and put the side rails up. ANS: C Sleep and awakening are often reversed in patients with dementia. Trying to keep the patient awake during the day is helpful. DIF: Cognitive Level: Application REF: p. 210 OBJ: 6 TOP: Sleep Patterns KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 23. A nurse is discussing home care of a patient with dementia with the patient’s family. What should the nurse advise the family do to prevent the patient from wandering? a. Apply a vest restraint to keep the patient in bed or in a chair. b. Put locks on any doors that it would be dangerous for the patient to open (e.g., outside doors, medicine cabinet). c. Have someone remind the patient at least every 2 hours that he or she must not go outside by him or herself. d. Set up a reward system for the times the patient stays where the family has requested. ANS: B Patients with dementia must have the environment adapted to them rather than trying to adapt the patient to the environment. They usually forget things relatively quickly and will probably not remember what you have told them. DIF: Cognitive Level: Application REF: p. 211 OBJ: 6 TOP: Wandering KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 24. A patient asks a nurse, “My doctor says I get confused sometimes because I have vascular dementia. What caused me to have that?” What is the most appropriate response by the nurse? a. “It is usually caused from damage to brain cells because of inadequate blood supply, like a small stroke.” b. “It is probably just some abnormal electrical activity in your brain.” c. “You probably have a brain tumor.” d. “I’m sure he will explain it to you later.” ANS: A Patients with vascular dementia often have had a series of small strokes that cause progressive damage. DIF: Cognitive Level: Knowledge REF: p. 205 OBJ: 1 TOP: Vascular Dementia KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 25. What should nursing care focus on to best support a patient with mild cognitive impairment (MCI)? a. Reorienting the patient to the physical environment b. Developing strategies to improve memory c. Assisting with dressing and eating d. Establishing toileting schedules ANS: B Persons with MCI need strategies for improving their memory. These persons have memory impairment but have otherwise normal cognition. DIF: Cognitive Level: Comprehension REF: pp. 204-205 OBJ: 1 | 6 TOP: MCI KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 26. An 80-year-old patient with delirium related to high fever is hallucinating about large animals being in the room. What is the most reassuring nursing response to this patient? a. “Yes, the animals are in here, but they are sound asleep.” b. “I’m going to turn out the lights so you won’t have to look at the animals.” c. “You are in the hospital. There are no animals in this room.” d. “The hospital does not allow animals in the room.” ANS: C Reorientation and presentation of reality are helpful with patients who have delirium. DIF: Cognitive Level: Application REF: p. 208 OBJ: 6 TOP: Hallucinations KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. What are believed to be causes of Alzheimer disease? (Select all that apply.) a. Amyloid deposits in the brain b. Excess of acetylcholine c. Neurofibrillary tangles d. Infiltration of Lewy bodies e. Series of small strokes ANS: A, C The cause of Alzheimer disease is still unclear, but protein deposits of amyloid have been found during autopsies of the brains of patients with Alzheimer disease, as well as tangled neurofibers. In addition, a deficiency of acetylcholine exists. Lewy bodies are associated with another type of dementia, and small strokes are thought to be the cause of vascular dementia. DIF: Cognitive Level: Knowledge REF: p. 205 OBJ: 2 TOP: Etiology of Alzheimer Disease KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. When a normally oriented 87-year-old resident in a long-term care facility exhibits acute confusion, the nurse should first assess for a(n) . ANS: infection Infections, especially those that cause fever, can result in an older patient becoming confused or delirious. DIF: Cognitive Level: Application REF: pp. 203-204 OBJ: 3 TOP: Infections as Cause of Acute Confusion KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. An 80-year-old woman who has Alzheimer disease is restless, wanders during mealtimes, and will not sit down to eat. The nurse assisting with writing the care plan prioritizes the following interventions for the goal: The patient will eat at least 25% of each meal. (Prioritize the options in sequence, from the most therapeutic to the least therapeutic. Do not separate answers with a space or punctuation. Example: ABCD.) a. Place her in a chair with a vest restraint. b. Assign a nursing assistant (NA) to feed her. c. Give her a high-protein drink in a small cup to carry with her. d. Offer peanut butter crackers as she passes by. e. Leave her alone. She will eat when she is hungry. ANS: CDBAE Offering a high-energy drink in a small cup partially meets the goal without further agitating the patient. Offering a cracker accomplishes the same thing, but accurate evaluation of whether the crackers are eaten or just dropped might be difficult. Assigning an NA to feed her may agitate her further and reduce her intake even more; in addition, it may not be the best use of available personnel. Placing her in a chair with a vest restraint is not a very desirable intervention and may not encourage her to eat. Leaving her alone does not meet the goal nor does it reduce the nutrition deficit. DIF: Cognitive Level: Analysis REF: pp. 209-210 OBJ: 6 TOP: Nutrition Deficit KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 14: Incontinence Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What instruction should a nurse provide to a patient scheduled for a postvoid residual (PVR) test? a. Call the nurse immediately after voiding. b. After voiding, wait 10 minutes and void again. c. Void into a flowmeter. d. Avoid fluid intake for 8 hours before the test. ANS: A The nurse must catheterize the patient immediately after voiding and measure the amount of urine. DIF: Cognitive Level: Application REF: p. 217 OBJ: 5 TOP: Postvoid Residual Test KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. Bladder training instructions are being given to a patient who has a history of urinary incontinence. What initial instructions should the nurse give to the patient? a. “Wait until you feel the urge to void.” b. “Don’t void any more often than every 4 to 6 hours.” c. “Void every 2 to 3 hours while awake.” d. “Void any time you feel the urge.” ANS: C Bladder training uses scheduled voiding; the patient is encouraged to delay voiding and void only every 2 to 3 hours while awake. DIF: Cognitive Level: Application REF: p. 217 OBJ: 5 TOP: Bladder Training KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A male patient with urinary incontinence has been using an external (condom) catheter. A nurse is assessing the patient’s technique of applying the device. What techniques demonstrated by the patient would indicate the need for further instruction? a. Washes the penis with warm soapy water and dries the area well before applying the device. b. Encircles the penis with tape to secure the device. c. Uses elastic tape and wraps in a spiral pattern to secure the device. d. Carefully assesses the penis for any signs of irritation before applying the device. ANS: B Encircling the penis with tape can restrict circulation and cause damage to the tissue. DIF: Cognitive Level: Application REF: p. 220 OBJ: 6 TOP: External Urine Collection Device KEY: Nursing Process Step: Evaluation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 4. A patient being assessed by the physician states, “I wet my pants every time I cough.” The nurse recognizes this as which type of incontinence? a. Reflex b. Overflow c. Urge d. Stress ANS: D Stress incontinence is the involuntary loss of small amounts of urine during physical activity that increases abdominal pressure, such as coughing, laughing, sneezing, and lifting. DIF: Cognitive Level: Knowledge REF: p. 222 OBJ: 3 TOP: Stress Incontinence KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. What instruction should a nurse provide to a patient who has been diagnosed with stress incontinence? a. “Restrict fluid intake to less than 1000 mL/day.” b. “Avoid fluids such as tea, coffee, and cola.” c. “Delay voiding until you feel the urge to void.” d. “Void no more often than every 4 hours.” ANS: B Fluids such as tea, coffee, and cola have a diuretic effect and should be avoided. DIF: Cognitive Level: Application REF: p. 223 OBJ: 6 TOP: Stress Incontinence KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A home health nurse is performing an evaluation of the home of an older adult patient to assess for any safety issues. What should the nurse recognize as an environmental factor that could lead to functional incontinence? a. Night-light in the bathroom b. Patient’s room located on the opposite end of the house from the bathroom c. Handrails located around the toilet and bathtub d. Caregiver’s room located close to the patient’s room ANS: B Functional incontinence is the term used when a person voids inappropriately because of an inability to get to the toilet or manage the mechanics of toileting. The patient’s room should be located close to the bathroom. DIF: Cognitive Level: Comprehension REF: p. 225 OBJ: 3 TOP: Functional Incontinence KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. What condition should a nurse specifically ask a patient about when taking the medical history to reveal clues to the potential cause of urinary incontinence? a. Diabetes mellitus b. Impetigo c. Hypotension d. Trigeminal neuralgia ANS: A Patients who have diabetes may develop neurologic problems that affect the bladder and are uncontrolled; they may produce large volumes of urine. DIF: Cognitive Level: Comprehension REF: p. 226 OBJ: 5 TOP: Medical History KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. A patient, talking to a home health nurse about urinary incontinence, gives the nurse a list of the current medications she is taking. What medication should the nurse recognize as possibly contributing to the patient’s urinary incontinence? a. Methylcellulose (Citrucel) b. Diazepam (Valium) c. Simvastatin (Zocor) d. Digoxin (Lanoxin) ANS: B Valium is a sedative that can increase the incidence of incontinency of urine. DIF: Cognitive Level: Comprehension REF: p. 224 OBJ: 5 TOP: Urinary Incontinence KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 9. A nurse is instructing a patient on the procedure for a clean-catch urine specimen. The patient has tried several times but is having difficulty understanding the instructions. What is the best action for the nurse to implement? a. Take whatever specimen the patient can obtain. b. Provide the patient with a clean bedpan to obtain the specimen. c. Ask the laboratory personnel to come and obtain a urine specimen. d. Call the physician for a catheterization order. ANS: D If the patient cannot cooperate with the clean-catch procedure, catheterization may be necessary. DIF: Cognitive Level: Application REF: p. 217 OBJ: 5 TOP: Clean-Catch Urine Specimen KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. A patient who is scheduled for an urodynamic test asks the nurse why he is having this test. What is the nurse’s best response? a. “To test the capacity of the bladder.” b. “To see how much urine is left in the bladder after you have voided.” c. “To test the function of the nerves and muscles of the bladder.” d. “To detect involuntary passage of urine.” ANS: C Urodynamic procedures assess the neuromuscular function of the lower urinary tract. DIF: Cognitive Level: Comprehension REF: p. 215 OBJ: 5 TOP: Urodynamic Test KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. A nurse is asked to instruct a patient on performing Kegel exercises to improve muscle endurance. The patient should be instructed to contract the muscles normally used to stop the flow of urine. Which proper technique should the nurse explain? a. Contract for 3 to 4 seconds and relax for 10 seconds. b. Contract for 10 seconds and relax for 10 seconds. c. Contract for 10 seconds and relax for 3 to 4 seconds. d. Contract for 3 to 4 seconds and relax for 3 to 4 seconds. ANS: B Long (6-12 seconds) contractions, followed by relaxation for 6-12 seconds, improves endurance. This patient should hold the contraction for 10 seconds and then relax for 10 seconds. The goal is to work up to 10 repetitions three or four times each day. DIF: Cognitive Level: Application REF: p. 218 OBJ: 6 TOP: Kegel Exercises KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. A patient who uses a pessary to help control incontinence is given instruction for its care. What should these instructions include? a. Remove periodically for cleaning. b. Douche daily with a cleansing solution. c. Check for proper placement once a month. d. Periodically deflate the cuff. ANS: A A pessary is a device that is inserted into the vagina to hold the pelvic organs in place. The device must be removed periodically for cleaning and replaced as needed. DIF: Cognitive Level: Comprehension REF: p. 221 OBJ: 6 TOP: Pessary KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. A patient who has urinary incontinence is at risk for urinary tract infection and urinary calculi. What should the nurse teach the patient and family regarding the best way to prevent these complications? a. Restrict the patient’s fluid intake and frequency of incontinence. b. Be sure the patient’s voiding schedule is no more often than every 4 hours. c. Use an indwelling catheter. d. Encourage the patient to void at least every 2 hours and to take at least 2000 mL of fluid daily. ANS: D The risk of urinary tract infection and calculi can be reduced by having the patient empty the bladder as scheduled and providing adequate fluids. DIF: Cognitive Level: Application REF: p. 228 OBJ: 6 TOP: Urinary Tract Infection and Calculi KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A patient is having problems with fecal incontinence. What should the nurse encourage the patient to include in the diet to help with this problem? a. Beans and broccoli b. Potatoes and bread c. Coffee and tea d. Prune and grape juice ANS: B Foods that thicken the stool, such as potatoes, bread, bananas, rice, cheese, yogurt, oatmeal, oat bran, boiled milk, and pasta, should be encouraged. DIF: Cognitive Level: Application REF: p. 230 OBJ: 6 TOP: Dietary Changes KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 15. What should a nurse include as an essential factor when providing patient education about managing fecal overflow incontinence? a. Daily use of mineral oil b. Regular evacuation c. Daily administration of enemas d. Long-term use of mineral oil ANS: B Initially, the colon needs to be cleansed, and then regular evacuation is essential. DIF: Cognitive Level: Application REF: p. 230 OBJ: 6 TOP: Fecal Overflow Incontinence KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 16. A patient tells a nurse that his bowel movements normally occur every morning after breakfast. What should the nurse understand as the rationale for this occurrence? a. Fecal overflow b. Gastrocolic reflex c. Autonomic dysreflexia d. Lack of sphincter control ANS: B When food enters the stomach, it stimulates activity throughout the digestive tract and causes the movement of fecal mass into the rectum. DIF: Cognitive Level: Comprehension REF: p. 230 OBJ: 4 TOP: Gastrocolic Reflex KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 17. A physician’s admission report states that a patient has a history of tarry stools. What should the nurse anticipate when assessing characteristics of this patient’s stool? a. Brown and formed b. Bright red and liquid c. Black and sticky d. Clay colored and pasty ANS: C Tarry is used to describe stools that are shiny, sticky, and black, which is usually an indication of blood in the stool. DIF: Cognitive Level: Knowledge REF: p. 231 OBJ: 5 TOP: Characteristics of Stool KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 18. What education should a nurse provide to a patient diagnosed with anorectal incontinence? a. Take a daily laxative. b. Increase fiber in the diet. c. Perform pelvic muscle exercises. d. Administer daily enemas. ANS: C Anorectal incontinence is associated with nerve damage that causes the muscles of the pelvic floor to be weak. Pelvic muscle exercises can help strengthen these muscles. The other choices would cause the incontinence to worsen. DIF: Cognitive Level: Application REF: p. 231 OBJ: 5 TOP: Anorectal Incontinence KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 19. Which result of postvoid catheterization would indicate adequate bladder emptying? a. Less than 125 mL b. Less than 100 mL c. Less than 75 mL d. Less than 50 mL ANS: D If the catheterization immediately after voiding is less than 50 mL, the voiding can be viewed as adequate or normal. DIF: Cognitive Level: Knowledge REF: p. 217 OBJ: 5 TOP: Postvoid Catheterization Evaluation KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 20. A nurse is cleaning a patient with fecal incontinence when the patient says, “This is so embarrassing, and it makes me really angry.” What is the nurse’s best response? a. “Don’t worry about it; it’s my job to clean you up.” b. “If you would have called me sooner, this wouldn’t have happened.” c. “Do you feel angry and embarrassed?” d. “Would you rather let your family clean you up?” ANS: C The nurse should use therapeutic communications of reflection to validate the patient’s feelings. DIF: Cognitive Level: Application REF: p. 233 OBJ: 1 TOP: Fecal Incontinence KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 21. What foods should a nurse explain to a patient can cause diarrhea? a. Cheese b. Cabbage c. Rice d. Yogurt ANS: B Foods such as cabbage, raw vegetables, and spicy foods can cause diarrhea. Cheese, rice, and yogurt thicken stool. DIF: Cognitive Level: Knowledge REF: p. 230 OBJ: 5 TOP: Dietary Changes to Reduce Diarrhea KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 22. A patient with fecal incontinence should be taught the importance of maintaining good skin integrity. What should be the focus of a nurse’s teaching? a. Cleanse the perianal area thoroughly after each stool. b. Use a fecal pouch. c. Change incontinence undergarments once a day. d. Take an over-the-counter laxative daily. ANS: A Skin integrity can be best maintained by keeping the perianal area clean and dry. The other choices may cause an impairment of skin integrity. DIF: Cognitive Level: Application REF: p. 233 OBJ: 5 TOP: Skin Integrity KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 23. What is the cause of symptomatic incontinence? a. Colorectal disease b. Gastrocolic reflex c. Constipation d. Nerve damage ANS: A Symptomatic incontinence is the result of colorectal disease. Medical care should be sought to identify and treat the cause. DIF: Cognitive Level: Knowledge REF: p. 231 OBJ: 3 TOP: Symptomatic Incontinence KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 24. A patient asks a home health nurse if the periurethral bulking procedure will be a permanent remedy to urinary incontinence. On what knowledge regarding the effects of this procedure should the nurse base a response? a. Are permanent. b. Are only helpful to men. c. Usually last for approximately 6 months. d. Remain for 2 or 3 years. ANS: D The periurethral bulking procedure that injects a bulking product around the urinary meatus usually has to be repeated every 2 to 3 years. DIF: Cognitive Level: Comprehension REF: p. 218 OBJ: 4 TOP: Periurethral Bulking KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 25. What does the uroflowmetry diagnostic tool measure? a. Voiding duration b. Specific gravity of urine c. Effectiveness of the detrusor muscle d. General bladder tone ANS: A The uroflowmetry is a diagnostic tool designed to measure voiding duration, rate, and amount. DIF: Cognitive Level: Knowledge REF: p. 215|p. 217 OBJ: 1 TOP: Uroflowmetry KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. What should a nurse include when providing instructions to a patient as to what to do when feeling the urge to void? (Select all that apply.) a. Breathe deeply and try to relax. b. Perform several Kegel maneuvers without resting in between. c. Walk to the bathroom at a normal pace while performing Kegel maneuvers. d. Distract herself with a book or a television program. e. Stop what she is doing and sit down or stand quietly. ANS: A, B, C, E Breathing deeply, trying to relax, and performing Kegel maneuvers are all helpful in urge suppression. Distraction is seldom effective. DIF: Cognitive Level: Comprehension REF: p. 218 OBJ: 2 TOP: Urge Suppression KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. What should the nurse include in the plan of care to protect the skin integrity of an incontinent patient? (Select all that apply.) a. Immediately remove wet garments and linens. b. Wash skin with an antiseptic and towel dry. c. Inspect for areas of redness and breakdown every morning. d. Apply cornstarch to the perineum to absorb moisture. e. Apply protective creams per agency policy. ANS: A, E Any wet clothing or linens should be removed, and protective creams should be applied according to agency policy. Applying an antiseptic or cornstarch is not recommended because antiseptics are drying and cornstarch gives rise to yeast infections. The skin should be inspected every time the brief is changed. DIF: Cognitive Level: Application REF: p. 228 OBJ: 4 TOP: Skin Integrity KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 3. Which is true regarding the habit training technique prompted voiding? (Select all that apply.) a. Is useful with cognitively impaired persons. b. Helps the patient to recognize incontinence. c. Is based on giving praise for staying dry. d. Strengthens the pelvic floor. e. Uses the Valsalva maneuver to force urine from bladder ANS: A, B, C Prompted voiding technique is used with cognitively impaired persons. This technique helps the patient recognize incontinence and the praise for staying dry. DIF: Cognitive Level: Comprehension REF: p. 217 OBJ: 4 TOP: Prompted Voiding KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. A patient complains, “My allergies make me sneeze and urinate in my pants. I take my allergy drug and I urinate in my pants even more.” The nurse assesses that the drug the patient is referring to is an . ANS: antihistamine Many antihistamine preparations increase the incidence of incontinence. DIF: Cognitive Level: Application REF: p. 224 OBJ: 5 TOP: Drugs That Increase Incontinence KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity 2. A nurse explains that the normal bladder will empty when it reaches the capacity of 200 to mL. (Use numeric characters only.) ANS: 250 The urge to void will occur when the bladder is holding 200 to 250 mL of urine. DIF: Cognitive Level: Comprehension REF: p. 215 OBJ: 6 TOP: Bladder Capacity KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. The method by which a nurse manually expresses urine from the bladder by pressing gently on the lower abdomen is the method. ANS: Credé The Credé method calls for the manual expressing of urine from the bladder be gently pressing down on the lower abdomen and pressing the bladder. DIF: Cognitive Level: Knowledge REF: p. 225 OBJ: 2 TOP: Credé Method KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 15: Nutrition Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Which carrier protein is responsible for absorption of vitamin B12? a. Pepsin b. Intrinsic factor c. Hydrochloric acid d. Gastrin ANS: B Active transport requires the input of energy for the movement of particles across a membrane against an energy gradient. This movement requires a carrier protein. The best-known carrier protein is the intrinsic factor, which is responsible for the absorption of vitamin B12. DIF: Cognitive Level: Knowledge REF: p. 247 OBJ: 2 TOP: Mechanisms of Absorption KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. An adolescent patient reports she is following a severe fad diet that only allows 80 g of carbohydrate a day. What should the nurse warn that continuing this diet can result in when providing education? a. Alkalosis b. Hyperglycemia c. Ketosis d. Hypernatremia ANS: C Diets with only 50 to 100 g of carbohydrates per day are likely to lead to ketosis. DIF: Cognitive Level: Knowledge REF: p. 235 OBJ: 7 TOP: Recommended Dietary Allowance KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. Which foods have the least amount of fat? a. Vegetables, cottonseed oil, and safflower oil b. Fruits, vegetables, and cereal grains c. Milk, cheese, and ice cream d. Bagels, cream cheese, and ham ANS: B Fruits, vegetables, and cereal grains are relatively low in fat. DIF: Cognitive Level: Comprehension REF: p. 238 OBJ: 3 TOP: Food Sources of Fat KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 4. Energy balance is measured by weight gain or weight loss. How is protein balance measured? a. Nitrogen b. Weight c. Muscle development d. Carbon ANS: A The body cannot store protein, so it needs to be eaten in the diet each day. Nitrogen in the urine is a good indicator of protein levels in the body. If protein intake is inadequate, nitrogen will be conserved by the kidneys, causing the urine nitrogen level to be low. DIF: Cognitive Level: Comprehension REF: p. 242 OBJ: 1 TOP: Protein Deficiency KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 5. What is the function of protein in the body? a. Provides the main source of energy. b. Serves as a catalyst for fat catabolism. c. Slows the rate of digestion and absorption of nutrients. d. Furnishes amino acids to build and repair tissue. ANS: D Functions of proteins include serving as building blocks (amino acids) to build and repair body tissue. Carbohydrates and fats are the major sources of energy. DIF: Cognitive Level: Knowledge REF: p. 236 OBJ: 1 TOP: Function of Protein KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 6. What is the minimum amount of protein needed for a well-balanced diet? a. 10% b. 20% c. 30% d. 40% ANS: A Protein should make up a minimum of 10% in the adult diet. DIF: Cognitive Level: Comprehension REF: p. 236 OBJ: 7 TOP: Protein in Diet KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. Which cereal would be most effective to increase the fiber in a patient’s diet? a. Rice Krispies b. Corn Flakes c. Wheaties d. Bran Flakes ANS: D Bran products offer more fiber content than rice, corn, or wheat. DIF: Cognitive Level: Application REF: p. 247 OBJ: 7 TOP: Dietary Fiber KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. An older man weighs 125 lb. How much should his daily fluid intake be for adequate hydration? a. 1684 to 1700 mL/day b. 1704 to 1988 mL/day c. 2005 to 2200 mL/day d. 2368 to 2490 mL/day ANS: B Water is the largest component of the body and body tissues and is essential to all life processes. To prevent dehydration in an older adult, 30 to 35 mL/kg are recommended daily. 125 lb = 56.8 kg 56.8 kg 30 mL = 1704 mL 56.8 kg 35 mL = 1988 mL DIF: Cognitive Level: Analysis REF: p. 250 OBJ: 1 TOP: Age-Related Changes KEY: Nursing Process Step: Application MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. A 13-year-old patient is 5 feet, 6 inches tall, weighs 102 lb, and is constantly worried about getting “too fat” and is refusing to eat. What condition should the nurse suspect? a. Bulimia b. Anorexia nervosa c. Malabsorption d. Peptic ulcer ANS: B Anorexia nervosa is an eating disorder characterized by self-imposed starvation. Persons with this disorder believe that they are fat even though they appear quite thin. DIF: Cognitive Level: Analysis REF: p. 244 OBJ: 5 TOP: Eating Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. A nurse observes a young patient who accepts her food tray and appears to eat it enthusiastically, but the patient goes into the bathroom immediately after eating. The nurse suspects that the patient is causing herself to vomit. What do these assessments suggest? a. Bulimia b. Anorexia nervosa c. Hyperemesis d. Diabetes mellitus ANS: A Bulimia is an eating disorder characterized by periods of binge eating followed by purging. DIF: Cognitive Level: Analysis REF: p. 244 OBJ: 5 TOP: Eating Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. For what complication should a nurse monitor in a patient on total parenteral nutrition (TPN)? a. Respiratory congestion b. Hypoglycemia c. Vomiting d. Hypotension ANS: A Central parenteral nutrition can cause pulmonary congestion if the fluid is not absorbed quickly enough. TPN may also cause hyperglycemia and hypertension but not vomiting. DIF: Cognitive Level: Analysis REF: p. 246 OBJ: 6 TOP: Nutritional Support KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. What is usually infused with standard peripheral parenteral nutrition intravenous (IV) therapy? a. 50% glucose b. 5% glucose c. 0.9% sodium chloride d. Sterile water ANS: B Peripheral parenteral nutrition, the standard IV therapy, may be made up of dextrose (5% to 10%). DIF: Cognitive Level: Comprehension REF: p. 246 OBJ: 6 TOP: Nutritional Support KEY: Nursing Process Step: N/A MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 13. A patient on an enteral feeding suddenly complains of feeling faint and is sweating. The diastolic blood pressure has dropped 20 points. The nurse recognizes this as signs of the dumping syndrome. What is the cause of dumping syndrome? a. Hypertonic fluid entering the jejunum and pulling large amounts of water from the circulating volume b. Rich enteral feeding causing bowel irritation with severe cramping c. Hypertonic solution rapidly entering the stomach causing pyloric spasm d. Rapid drop in blood glucose as a result of the hypertonic solution pooling in the jejunum ANS: A Enteral tube feedings can cause dumping syndrome by pooling feeding in the jejunum, which pulls fluid from the circulating volume and causes hypotension. DIF: Cognitive Level: Comprehension REF: p. 245 OBJ: 6 TOP: Nutritional Support KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies COMPLETION 1. Cysteine, proline, isoleucine, valine, tryptophan, phenylalanine, methionine, and histidine are all classified as _. ANS: essential amino acids The essential amino acids are cysteine, proline, isoleucine, valine, tryptophan, phenylalanine, methionine, and histidine. DIF: Cognitive Level: Knowledge REF: p. 236 OBJ: 1 TOP: Essential Amino Acids KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. A nurse calculates the needed kilocalories (kcal) for a 150-lb moderately active person to be kcal. (Use only numeric characters.) ANS: 2043 150 pounds ÷ 2.2 pounds = 68.1 kg 30 kcal = 2043 kcal. DIF: Cognitive Level: Analysis REF: p. 246 OBJ: 2 TOP: Kilocalorie Calculation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 16: Intravenous Therapy Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. In an assessment of a patient who has been receiving intravenous (IV) fluids for the past 6 hours, a nurse finds that the pulse is now bounding, the blood pressure is more than 15 mm Hg higher than the last reading, and pedal edema has developed. What should the nurse suspect? a. Infiltration of the IV site b. Vascular fluid volume excess c. Pulmonary air embolism d. Phlebitis of the leg veins ANS: B Fluid volume excess accounts for the changes in the vital signs. DIF: Cognitive Level: Comprehension REF: p. 262 OBJ: 5 TOP: Increased Vascular Fluid Volume KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. As part of a written standard protocol for the unit, a nurse adds that irrigation of an occluded cannula is not recommended. What is the rationale against performing this procedure? a. It may damage a venous valve. b. It may introduce an air embolus into the line. c. It may cause the patient pain. d. It may force blood clots into the main bloodstream. ANS: D A cannula may be occluded because a clot has formed against the end of the shaft. By irrigating it, the clot is forced into the bloodstream. DIF: Cognitive Level: Comprehension REF: p. 264 OBJ: 5 TOP: Occluded Cannula KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. What is a major advantage when medication is administered intravenously? a. Better maintained at a therapeutic blood level b. Less expensive than oral route c. Safer than administering by oral or intramuscular route d. Lower incidence of allergy than other routes ANS: A Patients who receive intravenous medications can be better ensured of a more constant therapeutic blood level. DIF: Cognitive Level: Comprehension REF: p. 253 OBJ: 1 TOP: IV Care Plan KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 4. How often should intravenous (IV) rounds be performed during a nursing shift? a. Every 15 minutes b. Every 30 minutes c. Every 60 minutes d. Twice per shift ANS: C IV checks every hour, made by a nurse, ensure maintenance of a proper rate, infusion condition, and complication detection. DIF: Cognitive Level: Application REF: p. 258 OBJ: 6 TOP: Time Checks for IV Infusions KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 5. Using an intravenous (IV) infusion system that delivers 60 drops/L, a nurse hangs a 1000-mL bag of 5% dextrose in water (D5W), which the physician has ordered to infuse at 80 mL/hr. It is now 1000. What time should the nurse anticipate the IV will need to be changed? a. 1800 b. 2000 c. 2030 d. 2230 ANS: D 1000 mL (whole volume) ÷ 80 mL (volume infused per hour) = 12.5 hours. 1000 + 12.5 hours = 2230. Military times should be used. DIF: Cognitive Level: Analysis REF: pp. 259-260 OBJ: 4 TOP: IV Rate and Times KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 6. Using an IV infusion system that delivers 60 drops/mL, a nurse hangs a 500-mL bag of normal saline (NS) at 0800. The physician has ordered a rate of 20 mL/hr. What should the nurse set the roller clamp to deliver? a. 10 gtt/min b. 20 gtt/min c. 25 gtt/min d. 30 gtt/min ANS: B 20 mL (amount to be infused in 1 hr) 60 gtt = 1200 gtt/hr. 1200 gtt ÷ 60 min in 1 hr = 20 gtt/min. This roller clamp is an old method to determine rates, but in the case of a nonavailability of electronic delivery devices, it is a good thing to know. DIF: Cognitive Level: Analysis REF: pp. 259-260 OBJ: 4 TOP: IV Calculations KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 7. A physician prescribes a hypertonic intravenous line for an extremely edematous patient. What solution should the nurse anticipate to be prescribed? a. D5W in NS b. Lactated Ringer solution c. D5W in 0.25 NS d. 10% glucose in water ANS: D D5W in 0.25 NS is hypotonic. D5W in NS and lactated Ringer solution are isotonic. 10% glucose is hypertonic. DIF: Cognitive Level: Comprehension REF: p. 263 OBJ: 2 TOP: IV Tonicity KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 8. What is the source of calories in IV solutions? a. Electrolytes b. Dextrose c. Vitamins d. Water ANS: B Dextrose is sugar and the source of calories. DIF: Cognitive Level: Comprehension REF: p. 254 OBJ: 2 TOP: Calories in IVs KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. What signs of infiltration should be assessed by a nurse? a. Burning sensation, pain, and puffy b. Pain, heat, and puffy c. Burning sensation and no feeling at the site d. Red streak up the arm ANS: A Intravenous fluid in the immediate tissues causes pain and swelling of the adjacent tissues. DIF: Cognitive Level: Knowledge REF: pp. 252-263 OBJ: 5 TOP: IV Infiltration KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Reduction of Risk 10. A physician orders an infusion of 1000 mL of 5% dextrose in 0.45% NS to be completed in 8 hours. The IV delivery system’s drop factor is 20 gtt. How many mL/hr should the nurse set the electronic infusion pump to deliver the infusion? a. 125 mL/hr b. 100 mL/hr c. 85 mL/hr d. 42 mL/hr ANS: A Whole volume (1000 mL) divided by number of hours (8) = 125 mL/hr. Volume per hour (125 mL) 8 hr = 1000 mL. DIF: Cognitive Level: Analysis REF: pp. 259-260 OBJ: 4 TOP: IV Calculations KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. A nurse assesses an area where an intravenous (IV) line had been recently removed. The area has redness, swelling, and warmth. What should the nurse suspect as the cause? a. Infiltration and air embolus b. Inflammation and possible phlebitis c. Blood loss and hemorrhage d. Embolus from the former catheter ANS: B IV sites may show signs of inflammation or infection or both after an IV line has been removed. DIF: Cognitive Level: Comprehension REF: p. 263 OBJ: 5 TOP: Infection and Inflammation in Previous IV Site KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. A nurse has a patient with a central line. The insertion site is covered by an occlusive dressing with yesterday’s date. The nurse is to give an intravenous drug through the central line. What should be the initial action of the nurse? a. Use any of the three ports for delivery. b. Change the occlusive dressing. c. Affirm catheter placement by withdrawing 10 mL of blood. d. Check dilution of the drug. ANS: D Checking the drug for the proper dilution is essential. The dressing is not due to be changed. Drawing 10 mL of blood for site placement is excessive. Only two of the ports, which are color coded, are to be used for drug, fluid, or blood administration. DIF: Cognitive Level: Application REF: pp. 253-265 OBJ: 3 TOP: IV Medication through Central Line KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. A nurse is choosing an intravenous cannula for an older adult patient and will choose the smallest size that will deliver the appropriate fluid. What size cannula is the most appropriate choice? a. 12 gauge b. 14 gauge c. 18 gauge d. 22 gauge ANS: D The inside diameter, called the gauge, is expressed in reverse numerical order. DIF: Cognitive Level: Comprehension REF: p. 254 OBJ: 3 TOP: IV Needle Sizes KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 14. A nurse assesses for signs of infected phlebitis. How should the nurse most accurately describe this complication when documenting? a. Rupture of the cannula with a lump under the skin b. Pale, cool skin with swelling at the puncture site c. Firm, cool, raised, painful area at the puncture site; oozing and purulent drainage d. Puncture site red, warm, with an oozing drainage ANS: D Infection causes redness, warmth, and drainage from the intravenous site. Red streaks following the path of the vein may be visible. DIF: Cognitive Level: Comprehension REF: p. 263 OBJ: 5 TOP: Phlebitis Signs KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 15. What instruction should a nurse provide to a patient when removing a central catheter? a. Lean forward and cough. b. Take a deep breath and bear down. c. Breathe deeply through the mouth. d. Lie on the right side. ANS: B The patient is instructed to take a breath and bear down to prevent air from entering the bloodstream as the catheter is removed. DIF: Cognitive Level: Comprehension REF: p. 264 OBJ: 6 TOP: Removal of Central Line KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 16. Where is the best place to begin to select a vein for an initial intravenous (IV) site in a left-handed patient? a. Antecubital vein of the right arm b. Antecubital vein of the left arm c. Right forearm d. Left forearm ANS: C Unless other reasons are identified, IV sites should be started in the most distal portion of the nondominant arm or hand. DIF: Cognitive Level: Knowledge REF: p. 257 OBJ: 6 TOP: Beginning an IV KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 17. Where should a nurse inject medication when administering an intravenous (IV) push medication to a patient who is receiving a continuous infusion? a. Into the hanging IV bag b. Directly into the insertion cannula after temporarily disconnecting the IV bag c. Into the port nearest to the insertion site to ensure quick delivery d. Into the port nearest to the IV bag for less painful administration ANS: C An IV push is to be administered through the port closest to the patient. DIF: Cognitive Level: Knowledge REF: p. 256 OBJ: 6 TOP: IV Push KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 18. An intravenous (IV) administration of doxycycline (Vibramycin) has extravasated. What nursing action should be implemented after stopping the IV line? a. Notify the physician, and restart the IV line in another site. b. Restart the IV line at another site and document the extravasation. c. Flush NS through cannula at the insertion site. d. Discard the IV tubing and the IV bag. ANS: A Because doxycycline is a vesicant, the physician should be notified. The IV line should be restarted to maintain the drug at a therapeutic level. DIF: Cognitive Level: Application REF: p. 263 OBJ: 7 TOP: Extravasation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 19. A patient is to receive ampicillin (Unasyn) IV piggyback in 100 mL of fluid every 8 hours. The main intravenous (IV) line of D5W is running at 80 mL/hr and is on time. A nurse’s responsibility is to calculate the total 24-hour intake. At the end of the 24-hour shift, how much IV intake should the nurse document that the patient has received? a. 300 mL b. 800 mL c. 1920 mL d. 2220 mL ANS: D 80 mL/hr 24 hr = 1920 mL; 100 mL 3 = 300 mL. Therefore, 1920 mL + 300 mL = 2220 mL in 24 hours. DIF: Cognitive Level: Analysis REF: pp. 259-260 OBJ: 4 | 6 TOP: IV Calculation for 24 Hours KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. A patient with a subclavian line complains of shortness of breath after an infusion. The patient is diaphoretic, and the blood pressure is 168/100 mm Hg, higher than a previous reading of 140/86 mm Hg. What should the nurse assess these symptoms as indicating? a. Fluid overload from too rapid an infusion b. Incorrect dilution of the infused drug c. Infection from faulty aseptic technique d. Embolus from introduced air or blood clot ANS: D Air can be introduced into the subclavian line from any of the ports that are left unclamped. The symptoms have occurred too quickly for an overload or infection. DIF: Cognitive Level: Analysis REF: pp. 253-265 OBJ: 6 TOP: Embolus KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 21. A patient has had an air embolus. What should be the immediate action of the quick-thinking nurse? a. Turns the patient to the left side and lowers the head of the bed b. Calls the “code team” c. Gives oxygen at 100% in a non-rebreathing mask d. Notifies the charge nurse ANS: A Lowering the head of the bed and turning the patient to the left side traps the air in the left atrium, where it can be more readily reabsorbed. DIF: Cognitive Level: Application REF: p. 264 OBJ: 6 TOP: Air Embolus KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 22. An older adult patient is quite ill and confused and begins to cry pitifully when a nurse approaches the bed to start an intravenous (IV) line. What is the best action for the nurse at this time? a. Keep the infusion equipment out of sight as much as possible, talk slowly, and divert the attention of the patient. b. Inform the patient that the physician has ordered the IV and calmly continue to prepare the site and start the IV. c. Give an analgesic as ordered, wait a few minutes, and then proceed. d. Restrain the patient’s arm to a padded arm board and proceed as directed. ANS: A Confusion during a bout of illness in older adults is common. Distraction and reassurance usually gain compliance. Medication and restraints are not indicated. DIF: Cognitive Level: Application REF: pp. 253-265 OBJ: 6 TOP: IVs and Older Adult Patients KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 23. What action should the nurse implement when discontinuing an intravenous (IV) line? a. Remove the dressing, remove the catheter, dispose of the used equipment in the sharps container, and chart observations and actions. b. Observe the site for redness, swelling, and pain, and put on sterile gloves. Remove the dressing catheter and chart the findings and action. c. Observe the site for redness, swelling, and pain, and put on clean gloves. Remove the dressing and catheter, place a 2 2 dressing over the site, and chart the findings and action. d. Observe the site for redness, swelling, and pain and put on clean gloves. Remove the dressing and catheter; chart the findings and action. ANS: C This procedure is not sterile. Clean gloves protect the nurse from the body fluids. Placement of a small 2 2 dressing keeps the area clean until the insertion site closes. DIF: Cognitive Level: Application REF: p. 260 OBJ: 6 TOP: Discontinuing an IV KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 24. Which order should be clarified by a nurse when transcribing orders? a. Potassium chloride, 80 mEq in 1000 mL D5W in 24 hours b. Potassium chloride, 40 mEq IV in 10 mL D5W IV push c. Potassium chloride, 50 mEq in 500 mL D5W in 4 hours d. Potassium chloride, 80 mEq in 1000 mL D5W in 12 hours ANS: B Potassium chloride is never given by intravenous push in such a small amount of diluent. Potassium chloride is always dissolved in D5W and should be infused at no more than 10 mEq/hr. DIF: Cognitive Level: Analysis REF: p. 262 OBJ: 7 TOP: IV Potassium KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies MULTIPLE RESPONSE 1. A nurse explains to a patient that, in the event of an accidental needlestick, the nurse should adhere to hospital policy. What directives should the nurse follow? (Select all that apply.) a. Antibiotics are taken if infection is present. b. Blood is drawn from both the nurse and the patient. c. Repeat blood draws are performed 4 weeks after the stick. d. Obtain the physician’s permission to return to work. e. An incident report is initiated. ANS: A, B, E Most policies follow the general guidelines of making an incident report in case of time lost from the injury, drawing blood from both the nurse and the patient to determine whether an infection might be present and what type it is, and giving the antibiotic protocol to the nurse in the event of an infection in the patient. As a rule, permission from a physician to return to duty or a blood draw in 4 weeks is not necessary. DIF: Cognitive Level: Comprehension REF: p. 260 OBJ: 6 TOP: Needlestick KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control COMPLETION 1. A nurse explains to a patient that the peripheral intravenous (IV) tubing administration set and dressing should be changed per . ANS: facility protocol To prevent infection, the IV tubing administration set and dressing should be changed according to individual facility protocol. DIF: Cognitive Level: Knowledge REF: p. 258 OBJ: 6 TOP: IV Administration Sets Change KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 2. What steps should a nurse take when administering an intravenous (IV) push drug through a peripheral intermittent device? (Place the events in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Clear the device with NS. b. Flush the device with NS only or a combination of NS and heparin. c. Check placement of the device. d. Slowly administer the drug through the device. e. Check the concentration of the drug. ANS: ECADB IV push medication requires careful checking of the appropriate dilution, checking the placement of the device, flushing the device with NS to clear it, slowly injecting the drug, and flushing the device with NS or a combination of NS and heparin. DIF: Cognitive Level: Application REF: pp. 256-257 OBJ: 3 | 6 TOP: Peripheral Intermittent Device KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. What actions should a nurse implement when assessing a peripheral intravenous (IV) line for an infiltration? _ (Place the events in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Elevate the arm. b. Apply warm compresses to the area. c. Restart the infusion at a different site. d. Stop the infusion. e. Notify the charge nurse. ANS: DCABE The infusion must be stopped to reduce the risk of further infiltration and then restarted to ensure that the adequate dose is received. The affected arm is elevated, warm compresses are applied, and the charge nurse is notified. DIF: Cognitive Level: Application REF: p. 263 OBJ: 5 | 6 TOP: Infiltration KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 17: Surgery Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A postoperative patient is complaining of incisional pain. An order has been given for morphine every 4 to 6 hours as needed (PRN). What should the nurse assess first? a. Assess for the presence of bowel sounds. b. Assess pupillary reaction. c. Ask the patient’s family if she is having pain. d. Determine when the patient last received pain medication. ANS: D Verifying the time of the last dose decreases the risk of a dose of medication being given too soon. DIF: Cognitive Level: Application REF: p. 289 OBJ: 8 TOP: Acute Pain KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A nurse is caring for a postoperative patient. What should the nurse ask when assessing for the complication of malignant hyperthermia? a. “Do you think you might have a fever?” b. “Do you currently have an infection?” c. “Has anyone in your family ever had problems with general anesthesia?” d. “Have you ever had any type of malignancy?” ANS: C Malignant hyperthermia is a life-threatening complication that occurs in response to certain drugs. Susceptibility to this response is inherited. DIF: Cognitive Level: Application REF: p. 279 OBJ: 8 TOP: General Anesthesia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Reduction of Risk 3. A patient who had a hysterectomy yesterday has not been allowed food or drink by mouth (NPO). The physician has now ordered the patient’s diet to be clear liquids. What should the nurse assess prior to providing this patient with clear liquids? a. Feelings of hunger b. Bowel sounds c. Positive Homans sign d. Gag reflex ANS: B The absence of bowel sounds would contraindicate a diet of clear liquids. DIF: Cognitive Level: Application REF: p. 281 OBJ: 7 | 8 TOP: Postoperative Nursing Implementations KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. Which technique should a nurse implement when changing a postoperative dressing? a. Enteric isolation b. Aseptic technique c. Clean technique d. Respiratory isolation ANS: B The aseptic technique is important to reduce the risk of infection. DIF: Cognitive Level: Comprehension REF: p. 286 OBJ: 7 TOP: Postoperative Risk for Infection KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 5. A nurse is caring for a postoperative patient who has had spinal anesthesia. Which assessment is a priority for this patient? a. Complaints of a headache b. Pulse rate of 78 beats/min c. Voided 300 mL d. Blood pressure of 126/78 mm Hg ANS: A One complication of spinal anesthesia is postspinal headache, which is caused by the leaking of cerebrospinal fluid at the puncture site. DIF: Cognitive Level: Application REF: p. 278 OBJ: 7 TOP: Regional Anesthesia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. During a nurse’s preoperative assessment, the nurse notices that a patient is extremely anxious. The patient’s blood pressure is 142/92 mm Hg, the heart rate is 104 beats/min, and respirations are 32 breaths/min. What nursing action should be implemented? a. Give the preoperative medicine early to help calm the patient. b. Call the surgical department and cancel the surgery. c. Notify the anesthesiologist or surgeon. d. Instruct the patient on possible postoperative complications. ANS: C When significant fear is associated with surgical complications, sometimes surgery is postponed until the anxiety level is reduced. DIF: Cognitive Level: Analysis REF: p. 270 OBJ: 3 TOP: Preoperative Anxiety KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 7. A nurse is performing a postoperative assessment on a patient who has just returned from a hernia repair. The patient’s blood pressure is 90/60 mm Hg, and the apical pulse is 108 beats/min. What should be the nurse’s first action? a. Check the dressing for bleeding. b. Notify the registered nurse (RN). c. Document the vital signs. d. Increase the rate of infusion of intravenous fluids. ANS: A A decrease in blood pressure and tachycardia could indicate postoperative bleeding. The first action of the nurse should be to check the dressing and then report to the RN. DIF: Cognitive Level: Application REF: p. 283 OBJ: 9 TOP: Postoperative Complications KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. A postoperative patient who has no previous medical conditions is difficult to arouse when transferred to the surgical unit from the postanesthesia care unit. A nurse monitors the pulse oximeter and gets a reading of 85%. What should be the nurse’s next action? a. Assess the pulse oximeter reading again in 1 hour. b. Arouse the patient, have him cough, and encourage deep breathing. c. Administer a dose of pain medication. d. Suction fluid from the oral cavity. ANS: B If the pulse oximeter reading is less than 90%, the patient should be aroused and encouraged to take deep breaths. The patient’s respirations may not be adequate as a result of the effects of anesthesia. DIF: Cognitive Level: Application REF: p. 281 OBJ: 9 TOP: Hypoxia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. A nurse has completed giving discharge instructions to a patient after a hernia repair. What verbalization by the patient should lead the nurse to determine that the patient understands the instructions? a. Go back to work tomorrow. b. Do not change the dressing until he sees his physician in 2 weeks. c. Ignore changes in the size of his abdomen. d. Report fever, redness, swelling, or increased pain at the incision site. ANS: D The patient should report any signs and symptoms of infection (e.g., fever, redness, swelling, pain). DIF: Cognitive Level: Comprehension REF: pp. 292-293 OBJ: 10 TOP: Discharge Planning KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. A nurse should include the proper use of an incentive spirometer in teaching a preoperative patient. What postoperative assessment of this patient would reveal that the incentive spirometry teaching has been effective? a. Adventitious breath sounds b. Expiratory wheezing c. Thick, green respiratory secretions d. Clear breath sounds ANS: D An incentive spirometer is used to promote lung expansion, which opens airways, reduces atelectasis, and stimulates coughing to clear secretions. DIF: Cognitive Level: Comprehension REF: p. 286 OBJ: 9 TOP: Impaired Gas Exchange KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. The suprapubic area of a postoperative patient is distended. The patient states that he has not voided since surgery approximately 9 hours ago. What should be the nurse’s first action? a. Notify the head nurse or physician. b. Insert a catheter and document insertion. c. Seat the patient on the side of the bed to try to void. d. Prepare the patient to return to surgery. ANS: C The patient should be encouraged to try to void in a natural position before other measures are taken. Seated on the bedside or on a bedside commode may make urination easier. DIF: Cognitive Level: Application REF: p. 280 OBJ: 9 TOP: Postoperative Urinary Retention KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 12. Which modification should the nurse implement when caring for a postoperative patient after cataract surgery? a. Early ambulation is not necessary. b. Remove the dressing immediately. c. Omit instructions relative to coughing. d. Omit use of an incentive spirometer for deep breathing. ANS: C There are only a few instances in which coughing is contraindicated. They include surgeries for hernias, cataracts, and brain surgery. DIF: Cognitive Level: Application REF: pp. 293-294 OBJ: 7 TOP: Postoperative Complications KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. When obtaining a patient’s signature on the surgical consent form, the patient seems confused about the procedure to be performed. What is the most appropriate response by the nurse? a. Tell the patient to talk to the physician after he or she gets to the surgical department. b. Ask the patient to go ahead and sign the consent. c. Ask the patient what the physician told him and then call the physician if necessary. d. Encourage the patient to ask his family what the physician told them. ANS: C The patient may not understand some of the medical terms used by the physician, and the nurse may be able to explain them. If the patient needs further information, notify the physician. The physician is responsible for explaining the procedure and the risks to the patient. DIF: Cognitive Level: Application REF: p. 272 OBJ: 3 TOP: Consent Form KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 14. A nurse is doing an assessment of a patient who has returned from a cardiac catheterization and had conscious sedation. Which finding should the nurse report? a. Difficulty arousing the patient b. Blood pressure of 124/72 mm Hg c. Oxygen saturation of 96% d. Patient complaints of the need to void ANS: A Conscious sedation uses intravenous drugs to reduce pain intensity or awareness without a loss of reflexes. A complication may be excessive sedation approaching that of general anesthesia. The patient should be easily aroused. DIF: Cognitive Level: Application REF: p. 279 OBJ: 6 TOP: Anesthesia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 15. What is the goal of palliative surgery? a. Remove and study tissue to make a diagnosis. b. Relieve symptoms or improve function without correcting the basic problem. c. Remove diseased tissue or correct defects. d. Correct serious defects that only affect appearance. ANS: B Palliative surgery is performed only to relieve symptoms or to improve function. It is not curative. DIF: Cognitive Level: Comprehension REF: p. 267 OBJ: 1 TOP: Types of Surgery KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. What information should a nurse ask a patient during the preoperative assessment? a. Current address and telephone number b. Food preferences c. Allergies, medications, and past medical conditions d. Bathing and sleep patterns ANS: C If an emergency should arise, any allergies can be promptly managed. Knowledge of the patient’s medications can enable the nurse to anticipate possible drug interactions. Past medical conditions may increase surgical risks or require special attention during the perioperative period. DIF: Cognitive Level: Comprehension REF: p. 269 OBJ: 2 TOP: Preoperative Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 17. Which member of the surgical team administers anesthetics and monitors the patient’s status throughout the procedure? a. Surgeon b. Circulating nurse c. Perfusionist d. Anesthesiologist ANS: D The anesthesiologist and nurse anesthetist have special training and are the members of the surgical team that administer anesthesia and are responsible for closely monitoring the patient during surgery. DIF: Cognitive Level: Knowledge REF: p. 277 OBJ: 5 TOP: Surgical Team KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 18. A nurse is assisting in the transfer of a postoperative patient from the postanesthesia care unit to the surgical nursing unit. What action should the nurse implement to ensure the safety of the patient? a. Put the side rails up after moving the patient from the stretcher to the bed. b. Ask the patient to move from the stretcher to the bed. c. Move the patient rapidly from the stretcher to the bed. d. Uncover the patient before transferring from the stretcher to the bed. ANS: A The patient will probably still be experiencing residual effects of anesthesia; the side rails should be up to prevent the patient from falling out of bed. DIF: Cognitive Level: Application REF: p. 285 OBJ: 9 TOP: Postoperative Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 19. A patient who has just undergone a colon resection complains to a nurse that he felt something pop under his dressing while trying to get out of bed. The nurse removes the dressing and finds that dehiscence of the wound has occurred. What nursing action should be implemented first? a. Replace the dressing; dehiscence is normal. b. Call the physician. c. Pull the wound edges together and replace the dressing. d. Cover the wound with sterile dressings saturated with normal saline. ANS: D The first action of the nurse should be to cover the wound with saline-saturated dressings to prevent damage of the exposed organs from drying and then to call the physician. DIF: Cognitive Level: Application REF: pp. 290-292 OBJ: 9 TOP: Wound Dehiscence KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 20. A patient has just returned to the surgical unit after varicose vein stripping and ligation. What is the best technique for a nurse to evaluate pain relief? a. Check the patient’s record for the last dose of pain medication administered. b. Ask the patient to rate the severity of the pain on a scale of 1 to 10. c. Ask the family if they think that the patient is having pain. d. Tell the patient to ask for pain medicine when it is needed. ANS: B Having the patient rate the pain provides a system for evaluating response to the pain medication. Pain is controlled better if treated before it becomes severe, and the patient may not ask for pain medicine soon enough. DIF: Cognitive Level: Application REF: p. 289 OBJ: 8 TOP: Postoperative Pain Relief KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 21. A patient scheduled for a liver biopsy has given a nurse a list of medications routinely taken at home. Which medication should the nurse question? a. Aspirin b. Multivitamin c. Furosemide d. Acetaminophen ANS: A Aspirin is an anticoagulant, which can increase the risk of postoperative bleeding. Drugs that have been taken for a long time may require dose adjustments because of the effects of surgery or the effect of additional drugs, which may be held or modified. DIF: Cognitive Level: Application REF: p. 268 OBJ: 2 TOP: Preoperative Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 22. What should a nurse suggest to a patient to prevent the effects of postoperative immobility on the gastrointestinal system? a. Avoid taking antibiotics. b. Increase her fluid intake. c. Avoid high-fiber foods. d. Limit her activity for the first 3 to 4 days. ANS: B The intake of oral fluids and ingestion of a normal diet help stimulate peristalsis. DIF: Cognitive Level: Application REF: p. 293 OBJ: 9 TOP: Postoperative Complications KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Infection Control 23. A postanesthesia care nurse is evaluating a patient for possible transfer to the surgical unit. Which assessment should prevent the patient’s transfer? a. Blood pressure of 126/78 mm Hg b. Pulse rate of 82 beats/min c. Pulse oximeter reading of 85% d. Respirations of 22 breaths/min ANS: C The pulse oximeter reading should be 95% to 100%. The patient should not be transferred from the recovery room until the vital signs are stable, respiratory and circulatory functions are adequate, pain is minimal, the patient is easily awakened, no complications have been experienced, and the gag reflex is present. DIF: Cognitive Level: Analysis REF: p. 284 OBJ: 8 TOP: Postoperative Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 24. Why should a nurse assess a patient’s limbs and position the limbs frequently after a regional anesthesia? a. Pain is not perceived, although motion is possible. b. Rashes and skin eruptions would indicate an allergy. c. Permanent paralysis is a concern. d. Contracture deformities may occur. ANS: A After a regional anesthesia, movement is possible, but pain is not perceived immediately after surgery, which leaves the patient susceptible to injury. DIF: Cognitive Level: Comprehension REF: p. 278 OBJ: 6 TOP: Regional Anesthesia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 25. A patient who received Penthrane as an inhaled anesthesia complains of a sore throat and a raspy voice. What should the nurse explain as the probable cause of these discomforts? a. Drying effect of the anesthesia b. Insertion of an endotracheal tube c. Postsurgical dehydration d. Possible upper respiratory infection ANS: B Inhalant anesthesia is administered via an endotracheal tube that is inserted after the patient is unconscious. DIF: Cognitive Level: Comprehension REF: p. 279 OBJ: 6 TOP: Inhalant Anesthesia KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. Patients with preoperative disorders put them at risk during recovery. What disorders should a nurse be aware may pose this hazard? (Select all that apply.) a. Diabetes b. Warfarin therapy c. Fungal skin infection d. Hepatitis C e. Chronic obstructive pulmonary disease (COPD) ANS: A, D, E Diabetes, hepatitis C, and COPD all complicate recovery related to blood-clotting deficiencies, respiratory problems, or disturbance in the healing process. Warfarin therapy is not a disorder and should have been discontinued well before surgery, and fungal skin infections do not pose a threat. DIF: Cognitive Level: Comprehension REF: p. 268 OBJ: 2 TOP: Conditions That Complicate Recovery KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A patient has an extensive bowel preparation of oral laxatives and enemas for a colon resection. What rationales should the nurse list when asked about the rigorous preparation? (Select all that apply.) a. Reduces possibility of fecal contamination of the operative site. b. Flattens the colon. c. Decreases postoperative distention. d. Avoids postoperative constipation. e. Decreases straining at stool. ANS: A, C, D, E Preoperative bowel preparation reduces the risk for infection from bowel contents and decreases postoperative distention, constipation, and straining at stool. DIF: Cognitive Level: Comprehension REF: pp. 272-273 OBJ: 3 TOP: Rationale for Bowel Preparation KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A nurse carefully monitors an obese patient after a hysterectomy for the peculiar postoperative complications. Which postoperative complications are associated with obesity? (Select all that apply.) a. Nausea b. Wound infection c. Hypertension d. Hemorrhage e. Respiratory difficulties ANS: B, E Obese patients are especially prone to postoperative respiratory complications of pneumonia and atelectasis. Obese patients are at increased risk for infection because of the amount of adipose tissue. DIF: Cognitive Level: Comprehension REF: p. 267 OBJ: 8 TOP: Postoperative Complications in the Obese Patient KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Reduction of Risk 4. What are the responsibilities of a circulating nurse? (Select all that apply.) a. Assisting the surgeon with the procedure b. Setting up the surgical room c. Scrubbing in to handle instruments d. Maintaining patient safety e. Documenting nursing care ANS: B, D, E The circulating nurse is in charge of the operating room, monitors asepsis, provides supplies, and documents patient care. The first assistant helps the surgeon with the procedure and the scrub nurse handles the instruments. DIF: Cognitive Level: Knowledge REF: p. 277 OBJ: 5 TOP: Circulating Nurse KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. A nurse discovers on the preoperative assessment that a patient has a condition that would require increased amounts of general anesthesia. The condition is . ANS: alcoholism Individuals who use alcohol excessively usually require greater amounts of anesthesia. DIF: Cognitive Level: Comprehension REF: p. 268 OBJ: 6 TOP: Conditions That Affect Anesthesia KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 18: The Patient with an Ostomy Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Which term appropriately defines an artificial opening into a body cavity? a. Gastrostomy b. Ostomy c. Colonoscopy d. Ureterostomy ANS: B An ostomy is an artificial opening into a body cavity. DIF: Cognitive Level: Knowledge REF: p. 298 OBJ: 3 TOP: Terminology KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. Why is a patient who has undergone a colostomy instructed to measure the width of the stomas for the first 6 weeks postoperatively before applying each new pouch? a. The stoma will shrink during this time. b. A poor-fitting pouch will cause infection of the stoma. c. The paste will not adhere. d. Prolapse will result. ANS: A During the first 6 weeks, the stoma normally shrinks. The pouch needs to fit as closely to the stoma as is comfortable and safe to prevent skin irritation. DIF: Cognitive Level: Comprehension REF: p. 303 OBJ: 4 | 7 TOP: Pouch Fit KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A 47-year-old patient with a permanent colostomy reports some abdominal discomfort and rigidity 3 days after surgery. Which assessment should the nurse report and record? a. Vital signs are temperature, 100 F; pulse, 92 beats/min; and blood pressure, 160/98 mm Hg. b. Stoma is swollen and red; small amount of blood is observed at the base. c. Pouch has drained 110 mL of green-brown liquid, oozing from the pouch edges. d. Stoma is protruding. ANS: A Vital signs, in conjunction with the complaint of abdominal discomfort, should be reported and recorded as possible signs of impending peritonitis. DIF: Cognitive Level: Application REF: p. 308 OBJ: 4 TOP: Signs of Peritonitis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A nurse is aware that many patients with ostomies have an altered self-image. What might this cause? a. Inadequate self-care b. Altered sexual function c. Nonadherence to diet d. Irrational anger ANS: B A damaged self-image or body image may cause patients with ostomies to feel unattractive and embarrassed about possible sexual activity. Open-ended questions assist the patient to talk about their feelings. DIF: Cognitive Level: Comprehension REF: p. 304 OBJ: 4 | 7 TOP: Self-Concept Issues in an Ostomate KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 5. What should a nurse instruct the patient to do to ensure a good fit of the appliance to avoid leakage? a. Place the pouch only when lying down. b. Check pouch placement to ensure a firm seal. c. Confirm that the pouch fits tightly to the edges of the stoma. d. Confirm that the pouch covers the entire abdomen. ANS: B Placement of the pouch should provide a good fit and be comfortable in all positions but not too snug on the stoma to risk laceration. The pouch needs to only cover enough of the abdomen to allow for a firm fit. DIF: Cognitive Level: Application REF: p. 299 OBJ: 4 | 7 TOP: Placement of the Stoma KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 6. What should a nurse suggest to a patient with a colostomy choose when selecting an appropriate diet to reduce excess gas or diarrhea? a. Roast beef, mashed potatoes, and peeled stewed tomatoes b. Broiled pork chop, boiled potato, and corn on the cob c. Broiled trout, mashed potatoes, and spinach d. Barbeque pork on a white bun, coleslaw, and French fries ANS: A Gas-forming or spicy foods and roughage, such as corn, fish, and cabbage, usually cause gas and diarrhea. DIF: Cognitive Level: Application REF: p. 305 OBJ: 7 TOP: Ostomy Nutrition Teaching KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. A patient who has had a temporary colostomy to rest his ulcerated bowel says, “I don’t know how I will continue to work at my job with this thing stuck to my stomach.” Which response by the nurse is most likely to stimulate communication? a. “This is only a temporary adjustment for you, and the colostomy will be reanastomosed in less than 6 months.” b. “A nurse with special training will be in to help you.” c. “What is there about your job that you feel you cannot do?” d. “Many people feel as you do, but they learn to dress and act and work just like they did before the surgery.” ANS: C Open-ended questions without prejudgment or belittling encourage the patient to identify sources of anxiety and help the patient cope with, adapt to, or problem solve stressful events. DIF: Cognitive Level: Application REF: p. 299 OBJ: 2 TOP: Interpersonal Communication Skills KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 8. What is the primary advantage of a J-pouch anal anastomosis procedure? a. No odor b. Easier to irrigate c. Near-normal bowel elimination d. Less problem with diarrhea ANS: C Preoperative teaching includes the expectation of near-normal bowel elimination. As with any bowel elimination, odor and possibly occasional diarrhea will occur. An irrigation is not necessary. DIF: Cognitive Level: Comprehension REF: p. 301 OBJ: 3 TOP: Preoperative Teaching for J-pouch KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. A patient with an ostomy asks the nurse what limitations should be observed in the immediate postoperative period when at home. What is the most informative information that the nurse should share? a. Avoid heavy lifting for at least 3 months. b. Limit fluid intake to no more than 1000 mL/day. c. Wear loose clothing without belts or elastic. d. Cover your appliance with plastic sheeting while showering. ANS: A Avoiding heavy lifting for 3 months is advised. People with ostomies should take in at least 2000 mL of fluid every day. They may wear ordinary clothes that do not bind the stoma. Showering is allowed because the appliance is waterproof. DIF: Cognitive Level: Comprehension REF: p. 306 OBJ: 7 TOP: Postoperative Limitations for Ostomates KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. A patient with a colostomy continues to worry about odor. What instruction should a nurse provide to allay this concern? a. Pierce the top of the appliance bag with a pin to allow gas to escape. b. Rinse the pouch in a vinegar solution. c. Wear tight-fitting underwear. d. Improve personal hygiene. ANS: B The problem of odor is a frequent cause of anxiety to patients with colostomies. Rinsing the bag with a vinegar solution or putting a small amount of vinegar in the bag is helpful in odor control. Piercing the bag allows gas to escape more easily, and wearing tight-fitting clothing does nothing to alleviate odor. Personal hygiene is not a consideration in controlling the odor of feces. DIF: Cognitive Level: Application REF: p. 305 OBJ: 7 TOP: Controlling Odor from a Colostomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 11. A 20-year-old patient with a permanent colostomy asks whether she will be able to become pregnant. What is the most informative response by the nurse? a. “No. The colostomy weakened the pelvic floor to the point that it will not support a pregnancy.” b. “Yes. Pregnancy may be accomplished with artificial insemination because the fallopian tubes are usually damaged by a colostomy.” c. “No. The abdominal pressure exerted by a pregnancy will cause the prolapse of the stoma.” d. “Yes. The colostomy will not interfere with pregnancy or delivery.” ANS: D Colostomies do not interfere with pregnancy or delivery. DIF: Cognitive Level: Comprehension REF: p. 306 OBJ: 7 TOP: Pregnancy KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. A baby born without a urinary bladder has a surgically created cutaneous ureterostomy. One stoma exists. What should be discussed with the child’s family regarding the care? a. “This urinary diversion is permanent, and urine will drain from it continually.” b. “In the future, a second surgery will offer an exit for the urine from the other kidney.” c. “This pouch needs to be changed only once a week.” d. “You should notify the surgeon if the stoma becomes paler in color.” ANS: A The baby’s ureterostomy and drainage of urine are constant. This is a permanent solution because of the lack of a bladder. Both ureters are joined for the release of urine through the stoma. The pouch will be on continually and needs to be changed as needed several times a day. DIF: Cognitive Level: Application REF: p. 312 OBJ: 5 | 7 TOP: Cutaneous Ureterostomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. What should the initial assessment of a patient that just returned from surgery for the creation of an Indiana pouch include? a. Drainage of urine from the Penrose drain at the operative site b. Condition and color of the stoma c. Appearance of mucus in the urine d. Copious and odorous urine drainage from the incision ANS: A Indiana pouches initially have a Penrose drain to drain the small amount of urine; it will have mucus in it but no odor. No stoma exists to observe. Irrigations may be necessary to remove clots and mucus. DIF: Cognitive Level: Application REF: pp. 316-317 OBJ: 3 | 6 TOP: Assessment of New Postoperative Patient KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 14. A patient says, “I hate this yucky paste under my appliance. I think I will just tape it on.” What is the best response by the nurse? a. “Taping will not work!” b. “Taping will not seal the wafer tight enough to prevent leakage or fill increases.” c. “Taping with waterproof tape is just as effective as the paste.” d. “Taping is far more irritating to the skin than the paste would be.” ANS: B Reminding the patient that the paste both bonds and waterproofs is the best information. DIF: Cognitive Level: Application REF: p. 304 OBJ: 6 | 7 TOP: Function of Paste on Ostomy Appliance KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 15. A patient comes to the industrial nurse and is frantic because the stoma to the colostomy has prolapsed 1 year after surgery. What is the best response by the nurse? a. “If there are still feces coming from the stoma, then it is not blocked. Contact your surgeon for an evaluation.” b. “You must come in immediately because the stoma may completely retract into your abdomen.” c. “This is an emergency situation because it has stenosed.” d. “Don’t worry about that. Coughing or sneezing might have caused the prolapse. It will come back out in a few hours.” ANS: A The prolapse of a stoma is very disturbing to a patient. The condition should be evaluated by the surgeon. However, if the stoma is still patent, emergency implementation is not necessary. Prolapse can be caused by coughing or sneezing, but the stoma will still need evaluation. DIF: Cognitive Level: Application REF: p. 312 OBJ: 7 TOP: Stomal Prolapse KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. A patient is receiving discharge instructions and shares with the nurse that he intends to do a lot of traveling. What instruction should the nurse include? a. “Pack plenty of extra colostomy supplies in your checked airline luggage. Some places you might visit do not always carry the supplies you will need.” b. “Exercise caution with new foods, especially local fruits and vegetables because they may cause diarrhea or gas.” c. “If visiting somewhere where drinking local water is not advised, irrigating the colostomy with the local water is still okay.” d. “Repeat back to me what we just talked about so that you will remember everything you have been taught.” ANS: B Warning about foods in a different country is appropriate. Supplies should be placed in a carry-on bag for quick access or in the case of lost luggage. Water that is not safe to drink is not appropriate as irrigation fluid. DIF: Cognitive Level: Application REF: p. 306 OBJ: 7 TOP: Discharge Instructions KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 17. Which assessment by a nurse caring for an immediate postoperative patient with an ileal conduit should be reported or receive attention immediately? a. Lack of bowel sounds b. Distended abdomen c. Mucus present in the urine d. Small amount of blood in the drainage ANS: B The distended abdomen suggests that the gastrointestinal suction is not effective to prevent bowel distention. The nurse must check the efficiency of the suction. Lack of bowel sounds, mucus in the urine, and a small amount of blood in the drainage are to be expected as normal postoperative assessments. DIF: Cognitive Level: Application REF: p. 309 OBJ: 4 TOP: Postoperative Care of Ileal Conduit KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 18. A patient asks if rectal suppositories can be used to assist with constipation problems with his colostomy. What should the nurse clarify regarding suppositories? a. They can be used in double-barreled colostomies. b. They can be used in a stoma. c. They should not ever be used in a colostomy. d. They will not penetrate well enough to relieve constipation. ANS: B Suppositories can be used effectively in double-barreled colostomies and in stomas of a single colostomy. DIF: Cognitive Level: Application REF: p. 312 OBJ: 7 TOP: Use of Rectal Suppositories KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 19. What might the continual loss of liquid stool result in with an ileostomy patient? a. Acidosis b. Alkalosis c. Erosion of stoma d. Colitis ANS: A Metabolic acidosis can result from a loss of bicarbonates in the stool. DIF: Cognitive Level: Comprehension REF: p. 304 OBJ: 4 TOP: Signs of Electrolyte Imbalance KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 20. Which is the best nursing strategy for encouraging an ostomy patient to perform self-care? a. Plan to change the pouch when family members will be present, and have the patient watch and listen to the procedure. b. Frequently tell the patient that if he or she does not learn stoma self-care, no one is going to do it for him or her. c. Encourage the patient to watch the stoma care procedure, gradually encouraging participation. d. Shield the patient from sight of the stoma until the patient actually asks to see it. ANS: C The goal for teaching patients with ostomies is to assist them to care for themselves without pressure or forcing. DIF: Cognitive Level: Application REF: p. 306 OBJ: 7 TOP: Encourage Self-Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 21. A patient asks a nurse if karaya products can be used to seal the urostomy appliance. On what knowledge should the nurse base a response? a. Any adhesive is effective on a urostomy appliance. b. Urine breaks down karaya products. c. Karaya products can cause urinary infections. d. Formation of urine crystals is increased with the use of karaya products. ANS: B Urine breaks down karaya products and should not be used as a paste with urinary diversion appliances. DIF: Cognitive Level: Comprehension REF: p. 314 OBJ: 4 TOP: Karaya Products KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 22. What is caused by some adhesive pouch material used to hold the appliance in place? a. Melting of the pouch b. Excoriation of the stoma c. Allergic reaction d. Unpleasant odor ANS: C Pouch adhesives can cause allergic reactions, but they do not melt the pouch or cause odor. Because the paste is not in contact with the stoma, it does not affect it. DIF: Cognitive Level: Comprehension REF: p. 304 OBJ: 7 TOP: Pouch Materials KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 23. What is the most effective way for a nurse to help provide support to the patient with an ostomy who has ineffective regimen management? a. Ask a volunteer from the American Cancer Society or United Ostomy Association to visit. b. Ask a volunteer from the Reach for Recovery Society to visit. c. Send a close family member for psychiatric counseling. d. Obtain humor books pertaining to illness, such as Anatomy of an Illness, or watch several episodes of The Three Stooges on television. ANS: A Contact with persons who have coped with all the aspects of ostomies are excellent resources for individuals with new ostomies. Every effort is made to send a volunteer of the same age and gender. DIF: Cognitive Level: Comprehension REF: p. 299 OBJ: 4 | 6 TOP: Support for Ostomy Patients KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation MULTIPLE RESPONSE 1. A postoperative patient with an ostomy has the potential for loss of fluid volume and electrolyte imbalance. Which assessments indicate such loss? (Select all that apply.) a. Changing mental status b. Twitching c. Poor skin turgor d. Moist mucous membranes e. Weakness ANS: A, B, C, E The loss of base products from the bowel that allow for metabolic acidosis can be a very serious postoperative complication. Signs and symptoms include changing mental status, muscular twitching, poor skin turgor, dry mucous membranes, and weakness. DIF: Cognitive Level: Comprehension REF: p. 304 OBJ: 4 TOP: Assessments for Fluid and Electrolyte Loss KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What can be caused by lack of thorough cleansing of fecal matter from around a stoma? (Select all that apply.) a. Fungal infection b. Bacterial infection c. Yeast infection d. Deterioration of the stoma e. Odor ANS: A, B, C, E Fecal matter left on the skin and trapped under the pouch can cause fungal, bacterial, and yeast infections, as well as odor. DIF: Cognitive Level: Comprehension REF: p. 304 OBJ: 4 TOP: Cleaning Stoma of Fecal Matter KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. What are complications that may occur with continent pouches (Kock and Indiana)? (Select all that apply.) a. Incontinence b. Difficult catheterization c. Pyelonephritis d. Rupture of the pouch e. Peritonitis ANS: A, B, C The most frequent complications are incontinence, difficult catheterization, and reflux pyelonephritis. Rupture and peritonitis are not threats to the patient from this surgery. DIF: Cognitive Level: Knowledge REF: p. 317 OBJ: 3 TOP: Complication of Kock and Indiana Continent Pouches KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. What should be considered when deciding placement of a stoma? (Select all that apply.) a. Good seal b. Stabilization from the abdominal rectus c. Ease of self-care d. Inoffensive appearance e. Proximity to the umbilicus ANS: A, C The two major considerations for the placement of the stoma are that the placement allows for a good seal and ease in self-care. Stabilization is nice but not necessary. The placement should not be near the umbilicus. DIF: Cognitive Level: Comprehension REF: p. 299 OBJ: 3 TOP: Stoma Placement KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. When a patient complains of urine crystals forming on the urostomy stoma, the home health nurse recommends dissolving them with a pad saturated with . ANS: vinegar A pad soaked in vinegar with dissolve urine crystals that may form on the stoma of a urostomy. DIF: Cognitive Level: Comprehension REF: p. 314 OBJ: 7 TOP: Urine Crystals KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 19: Palliative and Hospice Care Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. How should a nurse position the body after the death of a patient? a. Prone b. Supine c. On the side d. In Fowler position ANS: B The body should be placed in the supine position, with the arms at the sides or with the hands across the abdomen. DIF: Cognitive Level: Knowledge REF: p. 333 OBJ: 1 TOP: Positioning after Death KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. According to Strauss and Glaser, three states of awareness of terminal illness have been identified. What do these states include? a. Denial, anger, and depression b. Shock, yearning, and anguish c. Avoidance, confrontation, and accommodation d. Closed awareness, mutual pretense, and open awareness ANS: D Strauss and Glaser have identified three states of awareness: closed awareness, mutual pretense, and open awareness. DIF: Cognitive Level: Knowledge REF: p. 323 OBJ: 2 TOP: Awareness of Terminal Illness KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 3. When planning the care of a patient who is terminally ill, a nurse should include the prevention of pain and relief from discomfort. What should the nurse implement when administering pain medication? a. Narcotics have the potential for addiction. b. Pain medication must be given before the pain becomes unbearable. c. Pain medication should be given no more often than every 6 hours. d. Narcotics must be given as needed only. ANS: B Pain control must be consistent to provide constant relief rather than waiting until the pain is unbearable and then trying to relieve it. Addiction to narcotics is of little concern. DIF: Cognitive Level: Application REF: p. 331 OBJ: 5 TOP: Pain Control KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 4. What is one of the most important interventions for a nurse to implement when caring for a patient who is terminally ill? a. Touching and listening to the patient b. Encouraging the patient to express any regrets c. Assessing for signs and symptoms of impending death d. Talking to the patient about how other patients have handled the dying process ANS: A The simple presence of someone provides support and comfort. Neither words nor actions are necessary unless the patient requires something. Holding hands, touching, and listening are quality nursing responses. DIF: Cognitive Level: Application REF: p. 332 OBJ: 5 TOP: Fear of Loneliness KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 5. A nurse is assessing a patient who is terminally ill for clinical signs of impending death. What should the nurse expect when assessing the patient’s respirations? a. Deep, clear breath sounds b. Noisy, wet-sounding respirations c. Even, unlabored respirations d. Shallow, clear breath sounds ANS: B Breathing may sound wet and noisy. Noisy, wet-sounding respirations, termed the death rattle, are a response based on mouth breathing and accumulation of mucus in the upper airways. DIF: Cognitive Level: Comprehension REF: p. 325 OBJ: 2 TOP: Respiratory Changes KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. What is believed to be the last sense to remain intact during the death process? a. Touch b. Sight c. Smell d. Hearing ANS: D Hearing is commonly believed to be the last sense to remain intact during the death process. DIF: Cognitive Level: Knowledge REF: p. 327 OBJ: 2 TOP: Sensory Changes KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A patient’s family asks a nurse what to expect when the patient dies. What is the most accurate response by the nurse? a. His heart will stop, and then later he will quit breathing. b. His respirations will cease first, and then the heart stops beating within a few minutes. c. His heartbeat and breathing will just stop suddenly without warning. d. He will quit breathing first, and then it could be several hours before his heart stops. ANS: B The body gradually relaxes until all functions end. The respirations cease first, and then the heart stops beating within a few minutes. DIF: Cognitive Level: Comprehension REF: p. 327 OBJ: 2 TOP: Death Process KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. While a nurse bathes a patient, he says, “Why are you giving me a bath? I’m going to die no matter what.” What should be the nurse’s most appropriate response? a. “A bath will make you feel better.” b. “Would you like to talk about how you are feeling?” c. “Don’t you want your bath today?” d. “I can give you some medicine to make you feel better.” ANS: B Anger is a common and normal response to grief. Therapeutic communication should focus on the patient’s feelings. DIF: Cognitive Level: Comprehension REF: p. 322 OBJ: 5 TOP: Anger KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 9. A patient recently diagnosed with inoperable lung cancer tells a nurse, “I am looking forward to seeing my daughter graduate from college in 2 years.” What stage of grief should the nurse recognize this as according to Elizabeth Kübler-Ross? a. Denial b. Anger c. Bargaining d. Depression ANS: A Kübler-Ross identifies denial as the person refusing to acknowledge the impending loss. DIF: Cognitive Level: Knowledge REF: p. 322 OBJ: 2 TOP: Kübler-Ross Stages of Grief KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 10. The family of a patient who is showing signs of impending death tells a nurse that they would like for any organs that can be used to be donated. What action should the nurse implement? a. Wait until the patient has died before discussing organ donation with the family. b. Tell the family that the patient has not signed a consent, so the organs cannot be donated. c. Check the patient’s record to see whether the physician has written an order for the patient to have organs donated. d. Notify the physician of the family’s wishes. ANS: D The physician should be notified immediately because some tissues must be harvested within hours after death. The decision to donate organs may be made by the patient or immediate family. DIF: Cognitive Level: Application REF: p. 324 OBJ: 7 TOP: Organ Donation KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 11. A patient who is terminally ill has asked a nurse if he can request that cardiopulmonary resuscitation (CPR) not be used in the event he has respiratory or cardiac arrest. What is the best response by the nurse? a. “The physician is the only one that can make that decision.” b. “I will be glad to get you some information on advance directives, which are written statements of a person’s wishes regarding medical care.” c. “Yes, you can make that decision; I will tell all the nurses.” d. “Your family will have to make the decision.” ANS: B Written information concerning a patient’s rights to accept or refuse treatment must be provided to the patient. Advance directives are written statements of a person’s wishes regarding medical care. DIF: Cognitive Level: Application REF: p. 324 OBJ: 7 TOP: Cardiopulmonary Resuscitation KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 12. A nurse is caring for a patient who is terminally ill whose religion is Orthodox Jew. This patient’s physician’s orders specify “do not resuscitate” (DNR). The patient is alone and is having signs of impending death. What action should the nurse implement? a. Notify the family. b. Wait until the patient dies and then notify the family. c. Transfer the body to the mortuary or the morgue immediately after death. d. Stay with the patient until death occurs, prepare the body, and then call the family. ANS: A Only designated Orthodox Jewish persons or a Jewish burial service may care for the body. The dying person is not left alone. The body is not left alone between death and burial, which must occur within 24 hours. The body is not to be touched for up to 30 minutes after death. DIF: Cognitive Level: Comprehension REF: p. 325 OBJ: 5 TOP: Cultural Considerations KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 13. In caring for a dying patient who is grieving, a nurse bases patient care on the theory that grief is helpful and assists the person in accepting the reality of death. What is this type of grief is called? a. Dysfunctional b. Unresolved c. Uncomplicated d. Maladaptive ANS: C Uncomplicated grief assists the person in accepting the reality of death. DIF: Cognitive Level: Knowledge REF: p. 321 OBJ: 2 TOP: Grief KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 14. A nurse is on duty in the emergency department when a patient is brought in who has died almost immediately after admission. The family states that the patient has had no history of medical problems and that no apparent reason for death is known. What should occur in this situation? a. The police must be notified. b. The family may choose to have an autopsy performed. c. An autopsy is required by law, and the coroner or medical examiner must be notified. d. The body must be held at the hospital for 24 hours. ANS: C Under law, in most states, an autopsy is required if a person expires by suicide, homicide, within 24 hours of admission to a health care facility, or from unknown causes. DIF: Cognitive Level: Comprehension REF: p. 332 OBJ: 7 TOP: Autopsy KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 15. A nurse is preparing a patient’s body after death and discovers that the patient’s dentures were not in his mouth before death. What action should the nurse implement? a. Insert them gently into the mouth. b. Give them to the family. c. Throw them away. d. Send them to waste management to be disposed of properly. ANS: A Dentures may be inserted gently to maintain the normal facial appearance. If the dentures cannot be inserted easily, do not force them. DIF: Cognitive Level: Application REF: p. 332 OBJ: 7 TOP: Body Preparation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. A patient who is terminally ill asks a nurse what is meant by a medical power of attorney. What is the nurse’s best explanation of this written document? a. “It allows another person to manage your financial affairs.” b. “It allows the physician to make any medical decisions that need to be made for you.” c. “It says you have given up all rights to make medical decisions for yourself.” d. “It allows you to select someone to make health care decisions for you only if you are unable to do so for yourself.” ANS: D A medical power of attorney allows someone other than the patient to make medical decisions for the patient only if the person is incapable of making decisions as certified by the physician. DIF: Cognitive Level: Knowledge REF: p. 325 OBJ: 7 TOP: Medical Power of Attorney KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 17. What right does the Omnibus Reconciliation Act of 1990 require institutions to provide written information to patients concerning? a. Donation of organs b. Accepting or refusing treatment c. Autopsy d. Physician-assisted suicide ANS: B The Omnibus Reconciliation Act requires that all institutions that participate with Medicare must provide written information to patients concerning their rights to accept or refuse treatment. DIF: Cognitive Level: Knowledge REF: p. 325 OBJ: 7 TOP: Omnibus Reconciliation Act KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 18. What important need should a nurse caring for a dying patient understand? a. Frequent, thorough physical assessments b. Not imposing repeated and unnecessary assessments c. Current, updated health history from the patient d. Limiting the amount of visitors allowed ANS: B Being sensitive and not imposing repeated and unnecessary assessments on the dying patient are important. DIF: Cognitive Level: Comprehension REF: p. 331 OBJ: 5 TOP: Assessment of the Dying Patient KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 19. Nurses who have been caring for patients who are terminally ill frequently begin to feel helpless and frustrated. What is best for the nurse to implement when caring for the terminally ill patient? a. Find another job. b. Express feelings to a friend or co-worker. c. Ignore these feelings because they will soon be gone. d. Ask to care for different patients. ANS: B The basic recognition of the nurse’s feelings allows openness with the patient and the family. DIF: Cognitive Level: Application REF: p. 333 OBJ: 6 TOP: Caregiver Response KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 20. What should be the primary nursing goal when caring for a patient who is experiencing dysfunctional grieving? a. Enhancement of self-esteem b. Resolution of grief c. Provision of safety measures d. Prevention of complications ANS: B Dysfunctional grief is disruptive to a person’s typical lifestyle and must be resolved. DIF: Cognitive Level: Comprehension REF: p. 330 OBJ: 4 TOP: Dysfunctional Grief KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 21. A patient who has been diagnosed with a terminal illness is crying when a nurse enters the room. The patient states, “I promised God that I would be a better person if He will just let me get over this disease.” What stage of grieving according to Kübler-Ross should the nurse recognize this as? a. Denial b. Anger c. Bargaining d. Depression ANS: C In the bargaining stage, the person wishes for more time to avoid the loss. The patient may express feelings that the loss is occurring as a punishment for past actions and may try to bargain with a higher power to gain time. DIF: Cognitive Level: Knowledge REF: p. 322 OBJ: 2 TOP: Kübler-Ross Stages of Grief KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 22. A dying 10-year-old boy tells a nurse, “I am going to leave and live with my grandpa in heaven.” How should the nurse interpret this child is feeling? a. Fearful of death b. Accepting his own death based on adult attitudes c. Experiencing death anxiety d. Expressing anger ANS: B A 10- to 12-year-old child accepts death based on adult attitudes. DIF: Cognitive Level: Analysis REF: p. 322 OBJ: 2 TOP: Child’s View of Death KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 23. A 16-year-old boy who is positive for the human immunodeficiency virus (HIV) confesses to the school nurse that he sneaks out of his home at night and rides his motorcycle at high rates of speed. How should the nurse interpret this behavior? a. An attempt at manipulation b. Striving for identity c. Defiance of impending death d. A normal teenage prank ANS: C Teenagers between the ages of 13 and 18 years may act out with dangerous or risky behavior in defiance of death. DIF: Cognitive Level: Analysis REF: p. 322 OBJ: 2 TOP: Defiant Behavior KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation MULTIPLE RESPONSE 1. What is the focus of the provision of palliative care? (Select all that apply.) a. Care and not cure b. Service only in the hospital c. Environment for a pain-free death d. Psychologic support to the patient e. Psychologic support to the family ANS: A, C, D, E The concept of palliative care is to provide a painless death and psychologic support to the patient and family. Care outside of the hospital is provided by nurses from a hospice service that come into the home. DIF: Cognitive Level: Comprehension REF: p. 323 OBJ: 4 TOP: Palliative Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 2. A nurse counsels the family of a 6-year-old child experiencing the death of his grandfather not to shield the child from the grandfather’s death. What feelings might this child develop if protected from the pain of bereavement? (Select all that apply.) a. Fear b. Anger c. Abandonment d. Blame e. Inability to express feelings ANS: A, C, E Small children who are protected from the grief of the death of a loved one frequently develop feelings of fear and abandonment. They frequently regress to a younger level of developmental behavior and feel an inability to express their feelings. DIF: Cognitive Level: Knowledge REF: p. 322 OBJ: 2 TOP: Child’s Bereavement KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Growth and Development 3. How is death frequently viewed in American society? (Select all that apply.) a. Integral part of life b. Natural c. Negative d. Spiritually positive e. Unacceptable ANS: C, E Americans essentially view death and impending death as an event that is negative and unacceptable to their values of preservation of health and prolonging life. DIF: Cognitive Level: Knowledge REF: p. 321 OBJ: 1 TOP: American Concept of Death KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 4. What preferences does the document “Five Wishes” help a dying person communicate to the family? (Select all that apply.) a. Who should make decisions b. What medical treatment will be acceptable c. How to distribute assets such as real estate d. Degree of comfort desired e. How they wish to be treated ANS: A, B, D, E The document “Five Wishes” does not act in the place of a will, but it is recognized as a patient’s advance directives. DIF: Cognitive Level: Knowledge REF: p. 325 OBJ: 2 TOP: Five Wishes KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. When the family of a dying person does not discuss the issue of death openly and avoids the subject of dying altogether, the nurse recognizes this behavior representative of the stage described by Straus and Glaser. ANS: mutual pretense The process of mutual pretense occurs with the family and the dying patient denying the approaching death and avoids any discussion about it. DIF: Cognitive Level: Comprehension REF: p. 323 OBJ: 2 TOP: Strauss and Glaser’s Phases KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation Chapter 20: Complementary and Alternative Therapies Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What concept is believed to be the cause of illness with nontraditional therapies? a. Evil spirits b. Lack of harmony with the environment c. Deliberate abuse of the body d. Inappropriate diet ANS: B Alternate therapies are designed to recreate harmony and balance with the environment. DIF: Cognitive Level: Knowledge REF: p. 340 OBJ: 1 TOP: Alternate Therapies KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. The nurse is preparing a patient for surgery. Which statement by the patient would cause the greatest concern? a. “I take black cohosh to ease menopausal symptoms.” b. “I take garlic supplements daily to lower my cholesterol.” c. “I find St. John’s Wort helps my depression.” d. “When I feel nauseous I take ginger to settle my stomach.” ANS: B Garlic supplements taken daily can cause bleeding and must be discontinued before any surgical procedure. DIF: Cognitive Level: Comprehension REF: p. 339 OBJ: 4 TOP: Herbal Supplements KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A patient reports occasional constipation. Which herbal dietary supplement would the nurse recommend? a. Garlic b. Flaxseed c. Coenzyme 10 d. Feverfew ANS: B Flaxseed can be used to treat occasional constipation due to its laxative effect. DIF: Cognitive Level: Comprehension REF: p. 339 OBJ: 3 TOP: Herbal Supplements KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. Which complementary/alternative is built on complete systems of theory and practice that have evolved in different cultures apart from conventional medicine? a. Movement therapy b. Manipulative practice c. Energy therapy d. Whole medicine systems ANS: D Whole medicine systems are built on complete systems of theory and practice that have evolved in different cultures apart from conventional medicine. DIF: Cognitive Level: Comprehension REF: p. 338 OBJ: 3 TOP: Alternative and Complementary Therapies KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. A 50-year-old woman reports to the nurse she has been experiencing hot flashes due to menopause. Which herbal supplement is most likely to help with this symptom? a. Green tea b. Ginkgo biloba c. St. John’s Wort d. Black cohosh ANS: D Black cohosh can be used to treat menopausal symptoms. DIF: Cognitive Level: Comprehension REF: p. 339 OBJ: 3 TOP: Herbal Supplements KEY: Nursing Process Step: Intervention MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. Why are nontraditional remedies becoming popular? (Select all that apply.) a. Many remedies are available without a prescription. b. Remedies do not interfere with traditional medications. c. Treatment modalities can be self-taught. d. Practitioners charge lower fees than medical physicians. e. Remedies are noninvasive. ANS: A, C, D, E Alternative remedies are frequently available without a prescription and can be self-taught. The fees of the practitioners are much less than physicians, and the remedies are not invasive. The remedies may conflict with regular medications, however. DIF: Cognitive Level: Comprehension REF: p. 343 OBJ: 5 TOP: Alternative Remedies KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Which of the following herbal supplements have anticoagulant effects? (Select all that apply.) a. Cranberry juice b. Feverfew c. Garlic d. Ginger root e. Probiotics ANS: A, B, C, D Cranberry juice, feverfew, garlic, and ginger root can all have anticoagulant effects. DIF: Cognitive Level: Knowledge REF: p. 339 OBJ: 4 TOP: Herbal Supplements KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. A nurse explains that a patient who is taking Valium for a nervous disorder but is also taking passion flower tablets to combat symptoms is using a combination of traditional and alternative therapy that is called . ANS: complementary Complementary therapy is the use of traditional medication with the addition of nonprescription herbs. DIF: Cognitive Level: Knowledge REF: p. 337 OBJ: 1 TOP: Complementary Therapies KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. A nurse describes yoga as an alternative therapy that creates a mind– _ intervention. ANS: body Yoga is an alternative therapy that creates a mind–body intervention. Some individuals can attain a trancelike status. DIF: Cognitive Level: Knowledge REF: p. 340 OBJ: 3 TOP: Yoga KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. The most commonly used natural product in America is . ANS: fish oil A large NIH survey assessed the use of nonmainstream products and practices among Americans. The most commonly used natural product was fish oil. DIF: Cognitive Level: Knowledge REF: p. 343 OBJ: 3 TOP: Natural Products KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 21: Neurologic System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. To what does the neural synapse refer? a. Length of time it takes for afferent neurons to carry impulses to the central nervous system (CNS) b. Length of time it takes for efferent neurons to carry impulses to the motor neurons c. Space between the axons and the dendrites of a neuron d. Space between the axons of one neuron and the dendrites of the next ANS: D Smooth, coordinated transmission must travel from one neuron to another across the neural synapse. DIF: Cognitive Level: Knowledge REF: p. 350 OBJ: 1 TOP: Anatomy and Physiology of the Central Nervous System (CNS) KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. An older adult patient is experiencing extreme stress related to an admission to the hospital. What should the nurse expect the patient to demonstrate? a. Decreased heart rate b. Decreased blood pressure (BP) c. Irregular respiration d. Dilation of the pupils ANS: D Stress stimulates the fight-or-flight reaction with the release of epinephrine and norepinephrine, which causes increased heart rate and BP, reduced peristalsis, and pupil dilation. DIF: Cognitive Level: Comprehension REF: p. 351 OBJ: 4 TOP: Effects of Sympathetic Nervous System KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. Which neurologic finding would be considered abnormal in an 88-year-old patient? a. Slow papillary response to light b. Jerky eye movements c. Dizziness and problems with balance d. Absence of the Achilles tendon jerk ANS: C Dizziness and vertigo, although common, are considered abnormal. DIF: Cognitive Level: Comprehension REF: p. 350 OBJ: 2 TOP: Age-Related Neurologic Changes KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. What is the most reliable indicator of neurologic status? a. Blood pressure b. Pulse rate c. Temperature d. Level of consciousness ANS: D The ability to respond readily and correctly to person, place, and time is good evidence of intact sensorium. DIF: Cognitive Level: Knowledge REF: p. 354 OBJ: 3 TOP: Neurologic Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. A patient is stuporous but reacts by withdrawing from painful stimuli. What term is most appropriate for this patient? a. Comatose b. Lethargic c. Semicomatose d. Somnolent ANS: C A stuporous patient who reacts to pain is semicomatose. The patient with no reaction to pain is comatose. DIF: Cognitive Level: Knowledge REF: p. 355 OBJ: 3 TOP: Neurologic Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. Which describes the Babinski reflex? a. Downward curl of the toes b. Big toe bending upward c. Spreading out of the toes d. Pain in the big toe ANS: A Normal cortical function causes the toes to curl downward. Abnormal findings would be the toes turning up and spreading. DIF: Cognitive Level: Knowledge REF: p. 359 OBJ: 3 TOP: Neurologic Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. What should the nurse assess when a patient is scheduled for an angiogram? a. Dizziness b. Allergy to shrimp c. Increased BP d. Irregular heartbeat ANS: B Allergy to shrimp and other shellfish also indicates a probable allergy to contrast medium. DIF: Cognitive Level: Application REF: p. 361 OBJ: 4 TOP: Angiogram Preassessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 8. What diagnostic test might be contraindicated for a patient who has a pacemaker? a. Computed tomography (CT) b. Electromyography (EMG) c. Magnetic resonance imaging (MRI) d. Electroencephalography (EEG) ANS: C Metal appliances may be affected by the magnetic field during MRI. DIF: Cognitive Level: Knowledge REF: p. 362 OBJ: 4 TOP: Neurologic Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 9. A patient with a severe head injury begins to assume a posture of flexed upper extremities, with plantarflexed lower extremities. What do these assessments indicate? a. Increasing intracranial pressure (ICP) with decorticate posturing b. Decreasing ICP with decerebrate posturing c. Decreasing ICP with decorticate posturing d. Increasing ICP with decerebrate posturing ANS: A Increasing pressure on the tissue above the midbrain results in abnormal flexion (decorticate posturing). DIF: Cognitive Level: Analysis REF: p. 366 OBJ: 4 TOP: Symptoms of Intracranial Pressure KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. What should be immediately reported by the nurse caring for a 90-year-old patient with a closed head injury? a. Blood pressure change from 147/72 to 176/70-mm Hg b. Respiration rate increase from 14 to 18 breaths/min c. Slow pupillary reaction bilaterally d. Temperature decrease from 100.2 F to 97.6 F ANS: A The widening pulse pressure is an indicator of increased ICP. Respirations and temperature are returning to more normal levels. Older adults have a slowed pupillary response as they age. DIF: Cognitive Level: Analysis REF: p. 366 OBJ: 3 TOP: Nursing Care of Patient with Closed Head Injury KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. Which assessment on a patient on mannitol therapy for cerebral edema indicates the medication is effective in decreasing ICP? a. Increased BP b. Increased urinary output c. Decreased pulse d. Widening pulse pressure ANS: B Mannitol is a hyperosmolar diuretic that draws fluid from brain tissue into the bloodstream, which is then excreted by the kidneys. Decreasing pulse and widening pulse pressure indicate increased ICP. DIF: Cognitive Level: Comprehension REF: p. 367 OBJ: 5 TOP: Mannitol Therapy in Increased Intracranial Pressure (ICP) KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. What should a nurse instruct a patient after a lumbar puncture to prevent a headache? a. Lie flat. b. Lie on left side. c. Stay in semi-Fowler position. d. Ambulate in the room with assistance. ANS: A Lying flat for a prescribed period will allow the loss of cerebrospinal fluid during the procedure to replenish. DIF: Cognitive Level: Application REF: p. 361 OBJ: 4 TOP: Lumbar Puncture Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. Which three symptoms are characteristic of Cushing triad associated with increased ICP? a. Hypotension, tachycardia, and narrowing pulse pressure b. Hypertension, tachycardia, and headache c. Widening pulse pressure, headache, and seizure d. Bradycardia, hypertension, and widening pulse pressure ANS: D Bradycardia, increasing BP, and widening pulse pressure are all signs of increased ICP. DIF: Cognitive Level: Knowledge REF: p. 366 OBJ: 3 TOP: Increased ICP: Cushing Triad KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 14. How can the nurse help reduce ICP in caring for the patient after a craniotomy? a. Keeping the patient flat in bed b. Elevating the head of the bed 30 degrees c. Closely monitoring the IV rate d. Turning the patient to the right side ANS: B Elevating the head of the bed at least 30 degrees helps reduce ICP. DIF: Cognitive Level: Application REF: p. 365 OBJ: 4 TOP: Intervening for Increased ICP KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. Which neurotransmitters support smooth neural transmission? (Select all that apply.) a. Acetylcholine b. CSF c. Dopamine d. Dendrite e. Epinephrine ANS: A, C, E Acetylcholine, dopamine, and epinephrine are neurotransmitters. CSF bathes the brain and spinal cord but has no transmission activity; the dendrite is the locus of the synapse. DIF: Cognitive Level: Knowledge REF: p. 350 OBJ: 1 TOP: Neurotransmitters KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Which are normal brain alterations associated with age? (Select all that apply.) a. Decrease in brain weight b. Pigmentation of brain with lipofuscin c. Present of amyloid d. Tiny clot formation e. Tangled nerve fibers ANS: A, B, C, E All brain alterations listed are expected changes that affect the older adult’s neurologic function except for tiny clot formations, which are a pathologic change. DIF: Cognitive Level: Knowledge REF: p. 350 OBJ: 1 TOP: Age-Related Cerebral Changes KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. The nurse assessing the level of consciousness in a patient will perform the following: (Arrange in order from the simplest to the most complex. Do not separate answers with a space or punctuation. Example: ABCD.) a. Apply pressure to the nail bed. b. Shake the patient. c. Touch the patient. d. Call the patient’s name. e. Approach the patient. ANS: EDCBA The assessment begins with simply approaching the patient and progresses to imposing painful stimuli. DIF: Cognitive Level: Application REF: p. 355 OBJ: 3 TOP: Assessing Level of Consciousness KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. The nurse conducting a Romberg test will ask the patient to do what? (Arrange in the correct sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Touch his or her nose with the index finger with the eyes open. b. Stand with eyes closed. c. Touch his or her nose with the index finger with the eyes closed. d. Touch his or her fingertip to nurse’s fingertip. e. Pat the knees with the palms and then the back of the hands rapidly. ANS: BEDAC These simple exercises used to assess balance and perception should be performed in order from least to most difficult. DIF: Cognitive Level: Application REF: p. 355|p. 357 OBJ: 3 TOP: Romberg Test for Balance KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 22: Neurologic Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient with generalized convulsive disorder is unaware about the side effects of phenytoin (Dilantin). Which instruction would be most appropriate? a. Take medication with food. b. Brush teeth vigorously to encourage gingival growth. c. Limit fluids and eats foods that reduce diarrhea. d. Reduce stimuli and take warm baths to induce drowsiness. ANS: A Dilantin is irritating to GI tissues. Dilantin causes gingival hyperplasia, constipation, and drowsiness. DIF: Cognitive Level: Application REF: p. 372 OBJ: 2 TOP: Dilantin KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. A nurse is caring for a patient with meningitis who has a positive Brudzinski sign. Which assessment led to this conclusion? a. Flexed hips when the neck is flexed by the nurse b. Inability to extend the flexed leg fully because of hamstring pain c. Resisting efforts of the nurse to flex his or her neck d. Flexing the big toe upward and fan out the other toes ANS: A Inflamed meninges will stimulate hip flexion to reduce meningeal discomfort. DIF: Cognitive Level: Comprehension REF: p. 379 OBJ: 1 TOP: Symptoms of Meningitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A nurse is evaluating the effectiveness of teaching for a patient with multiple sclerosis (MS). Which statement by the patient indicates that accurate patient learning has taken place? a. “Now that I am taking steroids, I will be able to work like I used to.” b. “I’m making a list of things that are important and things I will simply have to let go.” c. “I will make a plan to allow for long rest periods at least four times a day.” d. “I am working on balancing time among rest, work, and family time.” ANS: D Balancing time between various activities indicates that the patient with MS understands the need to conserve energy, not just to give up things or attempt to perform at a preillness level. DIF: Cognitive Level: Application REF: p. 388 OBJ: 2 TOP: Altered Energy in Patients with Multiple Sclerosis (MS) KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A patient in the emergency department states that she fell and hit her head and blacked out for a while but became alert again. The nurse suspects an epidural hematoma. For what should the nurse be diligent to assess? a. Headache b. Drowsiness c. Increasing respiration rate d. Vomiting ANS: B Increasing BP, drowsiness, and a widening pulse pressure are indicators of increased ICP. DIF: Cognitive Level: Application REF: p. 376 OBJ: 2 TOP: Epidural Hematoma Assessment KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 5. Which intervention supports nutritional intake in a patient with Parkinson disease? a. Offer large meals with a variety of finger foods. b. Thicken liquids to make them easier to swallow. c. Puree all foods and drink through a straw. d. Offer a diet high in carbohydrates and fat and low in protein. ANS: B Thickened feedings are easier to swallow. Several small, protein-rich meals are preferable to large ones. A pureed diet is unappealing. DIF: Cognitive Level: Application REF: p. 385 OBJ: 2 TOP: Nutrition in Parkinson Disease KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A patient with Parkinson disease is depressed because his drug protocol of L-dopa and Sinemet is no longer controlling his symptoms. What is the best response by the nurse? a. Other drugs can be combined with L-dopa to increase its effectiveness. b. The effect of these drugs has an uneven course; symptoms will begin to subside again soon. c. The two drugs can be given in higher doses to control the symptoms. d. Surgical interventions have been very effective in the control of parkinsonian symptoms. ANS: A The addition of other drugs to L-dopa may improve the conversion of L-dopa to dopamine. Palliative surgical implementations all have had little effect on controlling the symptoms. DIF: Cognitive Level: Comprehension REF: p. 384 OBJ: 1 TOP: Treatment of Parkinson Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 7. A patient with Parkinson disease is considering taking St. John’s wort, an herbal remedy for depression, in addition to Sinemet and L-dopa. What is the most appropriate nursing response? a. Depression is reduced by the use of herbal remedies such as St. John’s wort. b. Doses of St. John’s wort and parkinsonian drugs should be taken on alternate days. c. St. John’s wort must be taken in large doses to reduce depression. d. Herbal remedies can interfere with the effectiveness of the parkinsonian drugs. ANS: D Herbal remedies interfere with effectiveness of prescribed parkinsonian drugs. DIF: Cognitive Level: Application REF: p. 385 OBJ: 1 TOP: Treatment of Parkinson Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 8. Which nursing assessment would indicate a need for suctioning a patient with Guillain-Barré who is experiencing impaired breathing patterns because of neuromuscular failure? a. Decreased pulse rate and respiration of 20 breaths/min b. Increased pulse rate and adventitious breath sounds c. Increased pulse rate and respiration of 16 breaths/min d. Decreased pulse and abdominal breathing ANS: B Increased pulse rate, adventitious breath sounds, and abdominal breathing indicate an impaired breathing pattern. DIF: Cognitive Level: Application REF: p. 382 OBJ: 2 TOP: Nursing Care of the Patient with Guillain-Barré Syndrome KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. A family member asks the nurse what would be an appropriate gift for a patient with Parkinson disease. What is the most useful suggestion? a. Soft-soled house shoes b. Jigsaw puzzle c. Set of card games d. Satin sheets ANS: D Satin sheets make moving in bed easier. Card games and jigsaw puzzles are frustrating because of the palsy. Hard-soled shoes provide better support than soft-soled shoes. DIF: Cognitive Level: Comprehension REF: p. 385 OBJ: 2 TOP: Care of the Patient with Parkinson Disease KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. What action should the nurse implement when a patient falls to the floor in a generalized seizure? a. Cradle the head to prevent injury. b. Insert an object between the teeth to prevent the patient from biting the tongue. c. Manually restrain the limbs. d. Keep the patient on his or her back to prevent aspiration. ANS: A Cradling the head and turning it to the side prevents injury and aspiration; restraint of limbs and insertion of an object into a patient’s mouth often result in injury. DIF: Cognitive Level: Application REF: p. 374 OBJ: 2 TOP: Seizure Implementations KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. Why is a patient with amyotrophic lateral sclerosis (ALS) uniquely prone to depression? a. Nutritional intake is poor. b. Intellectual capacity is not affected. c. Mobility is limited. d. Communication is altered. ANS: B Because of their unimpaired intellect, patients with ALS are able to assess their deterioration, which increases their risk for depression. Altered mobility, nutrition, and communication are common to many disorders. DIF: Cognitive Level: Comprehension REF: p. 389 OBJ: 1 TOP: Symptoms of Amyotrophic Lateral Sclerosis (ALS) KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 12. A nurse is careful about limb position in caring for an unconscious patient who sustained a head injury 10 days ago. What is the nurse trying to prevent? a. Flexion deformities b. Atrophy c. Paralysis d. Pathologic fracture ANS: A An unconscious patient should be positioned in anatomic alignment to prevent flexion deformities. Passive range of motion and frequent position changes are essential to maintain the limbs in a functional position. DIF: Cognitive Level: Comprehension REF: pp. 376-377 OBJ: 2 TOP: Flexion Deformities KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. What should the nurse implement before giving an enteral feeding to a patient? a. Palpate the abdomen to check for residual feeding. b. Warm the feeding. c. Elevate the head of the bed 30 degrees. d. Ask the patient to tip his head forward. ANS: C The head of the bed should be elevated 30 degrees to prevent aspiration. DIF: Cognitive Level: Application REF: p. 382 OBJ: 2 TOP: Enteral Feedings KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. A nurse caring for an immobilized patient with a brain tumor stimulates the patient several times a day with range-of-motion exercises and changes his position every 2 hours to try to prevent a disuse syndrome. What signs and symptoms does disuse syndrome include? (Select all that apply.) a. Pooling of pulmonary secretions b. Paralysis c. Muscle tremor d. Pressure ulcers e. Altered visual perceptions ANS: A, D A disuse syndrome includes pooling of pulmonary secretions, pressure ulcers, weakness, and stiff joints. DIF: Cognitive Level: Knowledge REF: p. 382 OBJ: 2 TOP: Disuse Syndrome KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. The nurse is caring for a patient with symptoms of a migraine headache. What assessment information supports this diagnosis? (Select all that apply.) a. Bilateral pain in temples b. Nausea c. Photosensitivity d. Elevated WBC count e. Tearing ANS: B, C, E Migraine pain is usually unilateral, often begins in the temple or eye area, and is often very intense. Tearing and nausea and vomiting may occur. The patient is hypersensitive to light and sound and prefers a dark, quiet environment. WBC count is not expected to be elevated. DIF: Cognitive Level: Comprehension REF: p. 369 OBJ: 1 TOP: Migraine Headaches KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort COMPLETION 1. The of the seizure is characterized by stiffening of the muscles or extremities with loss of consciousness. ANS: tonic phase The tonic phase of the seizure is characterized by stiffening of the muscles or extremities with loss of consciousness. DIF: Cognitive Level: Knowledge REF: p. 370 OBJ: 1 TOP: Seizures KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A(n) hematoma forms in the space between the inner surface of the skull and the outermost meningeal covering of the brain. ANS: epidural An epidural hematoma forms in the space between the inner surface of the skull and the outermost meningeal covering of the brain. DIF: Cognitive Level: Knowledge REF: p. 376 OBJ: 1 TOP: Hematoma KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 23: Cerebrovascular Accident Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient has weakness on the right side and impaired reasoning after having a cerebrovascular accident (CVA). What part of the brain is affected? a. Left hemisphere of the cerebrum b. Right hemisphere of the cerebrum c. Left cerebellum d. Right cerebellum ANS: A Impaired motor strength on the right side in conjunction with impaired reasoning indicates a lesion in the left hemisphere of the cerebrum. The cerebellum controls balance and is not contralateral. DIF: Cognitive Level: Comprehension REF: p. 404 OBJ: 3 TOP: Symptoms of a CVA KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Which patient is at the greatest risk for a CVA? a. A 20-year-old obese Latin woman who is taking birth control pills b. A 40-year-old athletic white man with a family history of CVA c. A 60-year-old Asian woman who smokes occasionally d. A 65-year-old African-American man with hypertension ANS: D Older African Americans have a higher incidence of CVA than occasional smokers, young persons, or athletes. Hypertension increases the risk. DIF: Cognitive Level: Analysis REF: p. 398 OBJ: 1 TOP: CVA Risk Factors KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A patient experienced a period of momentary confusion, dizziness, and slurred speech but recovered in 2 hours. Which assessment in the diagnosis of this episode would be most helpful? a. Patient’s complaint of nausea b. Blood pressure (BP) of 140/90 mm Hg c. Patient’s complaint of headache d. Results of MRI ANS: D TIA is generally suspected based on the health history and physical examination findings. Confirmation requires brain imaging studies, preferably with magnetic resonance imaging (MRI). BP of 140/90 mm Hg, although at the high end, is considered within normal limits. Headache and nausea alone are too common to be definitive. DIF: Cognitive Level: Application REF: p. 399 OBJ: 2 TOP: TIA Diagnosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A nurse is updating a teaching plan for a patient who sustained a TIA. What should the nurse be sure to include? a. Daily aspirin dose b. Long rest periods daily c. Reduction of fluid intake to 800 mL/day d. High-carbohydrate diet ANS: A Daily aspirin reduces platelet aggregation and may prevent another attack. Reductions of fluid and long rest periods encourage clot formation. DIF: Cognitive Level: Application REF: p. 399 OBJ: 3 TOP: Post-TIA Teaching KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 5. A patient recovering from a CVA asks the purpose of the warfarin (Coumadin). What is the best response by the nurse regarding the purpose of Coumadin? a. Dissolves the clot b. Prevents the formation of new clots c. Dilates the vessels to improve blood flow d. Suppresses the formation of platelets ANS: B Coumadin and heparin prevent more clots rather than dissolving them. Coumadin has no effect on vasodilation or blood cell production. DIF: Cognitive Level: Comprehension REF: p. 399 OBJ: 3 TOP: Coumadin Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 6. A patient has had a complete stroke as a result of a ruptured vessel in the left hemisphere. How should this patient’s CVA be classified? a. Ischemic, embolic b. Hemorrhagic, subarachnoid c. Hemorrhagic, intracerebral d. Ischemic, thrombotic ANS: C A ruptured vessel in a hemisphere is an intracerebral hemorrhagic CVA. It did not occur in the subarachnoid space. Ischemic CVAs are the result of occluded vessels. DIF: Cognitive Level: Analysis REF: p. 402 OBJ: 2 TOP: CVA Classification KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. What should a nurse ensure as a priority for a patient immediately after a CVA? a. Preservation of motor function b. Airway maintenance c. Adequate hydration d. Control of elimination ANS: B Adequate oxygenation prevents hypoxemia, which can extend and worsen effects of the CVA. DIF: Cognitive Level: Application REF: p. 412 OBJ: 7 TOP: Nursing Care of Acute CVA KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. When should a nurse recognize that the acute phase of a CVA has ended? a. Forty-eight hours has passed from its onset. b. The patient begins to respond verbally. c. BP drops. d. Vital signs and neurologic signs stabilize. ANS: D When the vital and neurologic signs stabilize, the acute phase has ended. Verbal response, lower BP, and the passage of time without other signs are not adequate evidence that the acute phase has ended. DIF: Cognitive Level: Comprehension REF: p. 406 OBJ: 7 TOP: Acute Phase of CVA KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. A patient in the acute phase of a CVA who has been speaking distinctly begins to speak indistinctly and only with great effort but still coherent. What should this nurse determine when assessing this patient? a. Stroke in evolution with dysarthria b. Lacunar stroke with fluent aphasia c. Complete stroke with global aphasia d. Stroke in evolution with dyspraxia ANS: A As symptoms worsen, the CVA is still evolving. Speech that is coherent but difficult is dysarthria rather than any type of aphasia. Dyspraxia is a motor impairment, not a speech impairment. DIF: Cognitive Level: Analysis REF: p. 403 OBJ: 4 TOP: CVA Deficits KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. Several days after a CVA, a patient’s family asks a nurse if tissue plasminogen activator (tPA) is a drug therapy option now. The nurse’s response is based on the knowledge that this drug must be used within how many hours after the onset of symptoms? a. 3 b. 5 c. 10 d. 24 ANS: A tPA is to be given within 3 hours of the onset of symptoms per the U.S. Food and Drug Administration’s guidelines. In some special treatment centers, this drug is given intravenously up to 6 hours after the stroke. DIF: Cognitive Level: Knowledge REF: p. 405 OBJ: 6 TOP: CVA Medication Implementation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 11. A nurse explains that a lumbar puncture is most helpful as a diagnostic tool for a new patient who has had a CVA. What would this diagnostic test help determine regarding the stroke? a. It is lacunar. b. It is hemorrhagic or embolic. c. It is complete or in evolution. d. It will result in paralysis. ANS: B Blood in the spinal fluid indicates a hemorrhagic stroke and will help direct medical protocol in the subsequent treatment. DIF: Cognitive Level: Comprehension REF: p. 405 OBJ: 5 TOP: CVA Diagnostic Tests KEY: Nursing Process Step: N/A MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. A patient who has sustained a hemorrhagic stroke is placed on a protocol of 60 mg of calcium channel blocker (nimodipine) every 4 hours. The patient’s pulse is 82 beats/min before the administration of the prescribed dose. Which action should the nurse implement? a. Give the full dose as prescribed without further assessment. b. Omit the dose, recording the pulse rate as the rationale. c. Delay the dose until the pulse is below 60 beats/min. d. Give half of the prescribed dose (30 mg). ANS: A The dose should be given; it would be held only if the pulse is below 60 beats/min. Assessments should be made regarding BP, urine output, and edema. DIF: Cognitive Level: Application REF: p. 401 OBJ: 3 TOP: CVA Medical Protocol KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 13. During the acute CVA phase, a risk for falls related to paralysis is present. Which intervention best protects the patient from injury? a. Keep the bed in a high position for ease of nursing care. b. Keep the side rails up, according to agency policy. c. Assess vision deficit related to ptosis. d. Monitor the condition every 2 hours. ANS: B Rails keep patients in bed. The bed should be low, monitoring the patient should be more frequent than every 2 hours, and visual assessment is not directly related to fall prevention. DIF: Cognitive Level: Application REF: p. 409 OBJ: 8 TOP: Acute Care: Fall Prevention KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 14. Pneumonia is the most frequent cause of death after a stroke. Which intervention would be contraindicated in the acute care of a patient with a hemorrhagic CVA? a. Thicken liquids to ease swallowing and prevent aspiration. b. Change position every 30 to 60 minutes. c. Maintain adequate fluid intake, orally or IV. d. Encourage forceful coughing to stimulate deep breathing. ANS: D Forceful coughing is contraindicated for the patient with a hemorrhagic CVA because it may cause increased intracranial pressure. DIF: Cognitive Level: Comprehension REF: p. 412 OBJ: 8 TOP: Prevention of Pneumonia KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 15. Which assessment indicates a fluid volume excess in a patient in the acute phase of a CVA? a. Decreased BP b. Weak pulse c. Adventitious breath sounds d. High urine-specific gravity ANS: C Crackles in the lung fields are a major indicator of fluid excess. The pulse and BP are elevated in fluid excess. Urine-specific gravity is low in fluid excess. DIF: Cognitive Level: Application REF: p. 413 OBJ: 8 TOP: Fluid Excess KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. Which intervention should the nurse include in a patient’s plan of care to help preserve joint mobility in the acute phase of a CVA? a. Pull the limbs on the affected side into a functional position. b. Perform aggressive full range-of-motion exercises for all extremities. c. Support affected points in good functional alignment. d. Exercise the limbs every 8 hours. ANS: C Limbs maintained in a functional anatomic position and gently exercised (never pulled) into an acceptable range of motion several times during a shift will maintain optimal mobility. DIF: Cognitive Level: Application REF: p. 409 OBJ: 8 TOP: Preserving Joint Mobility KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 17. A patient in the acute phase of an embolic CVA has an order for 400 units of heparin per hour IV. The heparin is in a solution of 5000 units/100 mL normal saline (NS). The nurse should set the electronic IV monitor at how many milliliters per hour? a. 6 b. 8 c. 10 d. 16 ANS: B Regardless of the method of calculation, 50 units of heparin are in each milliliter of the solution; 8 mL/hr delivers 400 units (5000 units ÷ 100 mL NS = 50 units/mL. 400 units ÷ 50 units/mL = 8 mL). DIF: Cognitive Level: Analysis REF: p. 400 OBJ: 8 TOP: Heparin Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 18. Which assessment indicates that a patient with a CVA is in transition to the rehabilitation phase? a. BP has been within normal limits for 24 hours. b. Patient makes positive statements about his condition. c. No further neurologic deficits are observed. d. Successful attempts are made at independent function. ANS: C When no further deficits are noted and all vital signs have stabilized, the patient is considered to be in the rehabilitation phase. Positive statements and attempts at independence are not sufficient. DIF: Cognitive Level: Application REF: p. 416 OBJ: 8 TOP: Rehabilitation Phase KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 19. A patient with homonymous hemianopsia is in the rehabilitation phase of a CVA. When arranging this patient’s environment where should the nurse assure persons approaching and important items are visible and available? a. Unaffected side b. Affected side c. Direct front d. Either side ANS: B Making the patient scan the affected side helps stimulate the return of normal function in the rehabilitation phase. DIF: Cognitive Level: Application REF: p. 417 OBJ: 8 TOP: Hemianopsia KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. Which outcome criterion is the most appropriate for a patient with “Inadequate nutrition, related to dysphagia, with the goal of adequate intake of nutrients”? a. Offers a variety of food groups b. Eats half of all meals offered c. Maintains body weight of 150 to 155 lb d. Eats all meals independently ANS: C The maintenance of a desired weight is indicative of adequate nutrition. Eating a portion of a meal or eating independently does not adequately measure the extent to which the goal was met. Offering a variety of foods is a nursing or dietary function, not an outcome. DIF: Cognitive Level: Application REF: p. 410 OBJ: 9 TOP: Rehabilitation: Nutrition KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 21. Which is the most effective intervention for best support of regular bowel elimination and the prevention of constipation? a. Limit fluid intake from 32 to 50 oz daily to compact the stool. b. Administer small soapsuds enema every other day to cleanse the bowel. c. Give stool softeners daily, establishing a consistent time to attempt elimination. d. Administer a strong laxative on a daily basis to encourage evacuation. ANS: C Daily stool softeners, rather than daily laxatives or frequent enemas, help restore regularity and bowel tone. DIF: Cognitive Level: Application REF: p. 409 OBJ: 8 TOP: Bowel Elimination KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 22. A patient in the rehabilitation phase after a CVA accidentally knocks the adapted plate from the table and bursts into tears after failing to feed himself. What is the best response by the nurse? a. “Don’t cry. You’ll be mastering eating in no time.” b. “I don’t believe crying will help. Let’s try drinking from a special cup.” c. “Bless your heart! Let me get a new meal and feed you.” d. “Learning new skills is hard. Let’s see what may have caused the trouble.” ANS: D Recognizing effort and showing support are the best approaches to depression and frustration. Babying the patient and admonitions against crying add to the problem. Redirection to the task at hand is therapeutic. DIF: Cognitive Level: Application REF: p. 417 OBJ: 8 TOP: Rehabilitation: Coping KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 23. Which instruction is most helpful in teaching the family and patient who is in the rehabilitation phase after a CVA about altered sensation? a. Make frequent assessments for signs of pressure or injury. b. Use the affected side in supporting the patient in ambulation and transfer to stimulate better sensation. c. Apply ice packs to the affected limbs to encourage a return of sensation. d. Apply a heating pad to the affected limbs to increase circulation. ANS: A Frequent assessment using the National Institutes of Health Stroke Scale will allow early detection. The use of hot or cold applications and using the affected limbs in transfer or ambulation may cause injury. DIF: Cognitive Level: Application REF: p. 409 OBJ: 8 TOP: Altered Sensation KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 24. Which posthospital option should the nurse encourage a patient to do when recovering from a CVA to provide the most comprehensive assistance? a. Transfer to a rehabilitation center. b. Discharge to home with scheduled visits from home health care nurses. c. Discharge to home with scheduled visits from a physical therapist. d. Discharge to home with scheduled visits from an occupational therapist. ANS: A A rehabilitation center with all modalities of support (e.g., physical therapy, occupational therapy, speech therapy, simulated home environments) is obviously the best option. DIF: Cognitive Level: Comprehension REF: p. 417 OBJ: 10 TOP: Postdischarge Planning KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 25. The wife of a husband who has had a CVA asks why he is being treated with insulin since he has no history of diabetes. What is the best response by the nurse as to why hyperglycemia occurs after a stroke? a. Brain swelling b. Hypertension c. Immobility d. Stress ANS: D Hyperglycemia occurs after a CVA as the body’s response to stress. If left untreated, the hyperglycemia will cause increased brain damage and worsen the outcome of the stroke. DIF: Cognitive Level: Comprehension REF: p. 406 OBJ: 3 TOP: Hyperglycemia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 26. What purposes exist for a stent in the carotid artery of a person with a TIA? a. Capture circulating clots. b. Help with subsequent angioplasties. c. Keep the artery open. d. Prevent hemorrhage. e. Measure the pressure in the artery. ANS: C The only purpose of a stent is to keep an artery open. DIF: Cognitive Level: Knowledge REF: p. 401 OBJ: 3 TOP: Use of Stent KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 27. What signs and symptoms characterize expressive aphasia? a. Speech that sounds normal but makes no sense b. Total inability to communicate c. Difficulty understanding the written and spoken word d. Stuttering and spitting e. Difficulty initiating speech ANS: E Expressive aphasia makes it difficult for the patient to initiate speech. DIF: Cognitive Level: Knowledge REF: p. 404 OBJ: 3 TOP: Expressive Aphasia KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation MULTIPLE RESPONSE 1. Which transitory symptoms might occur when a patient is diagnosed with a TIA? (Select all that apply.) a. Incontinence b. Dysphagia c. Ptosis d. Tinnitus e. Dysarthria ANS: B, C, D, E All, except transitory incontinence, are classic symptoms of a TIA. These deficits usually disappear without permanent disability in approximately 24 hours. DIF: Cognitive Level: Comprehension REF: p. 399 OBJ: 3 TOP: Symptoms of TIA KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. How does a lacunar stroke differ from an ischemic CVA? (Select all that apply.) a. Causes a great deal of pain b. Alters the personality c. Affects small arteries d. Nearly always results in blindness e. Produces a small amount of neurologic damage ANS: C, E The lacunar CVA only affects small arteries and produces a small amount of neurologic damage. DIF: Cognitive Level: Comprehension REF: p. 403 OBJ: 2 TOP: Lacunar CVA KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. Which patients with CVAs are considered candidates for treatment with tPA? (Select all that apply.) a. A 62-year-old construction worker who had a subdural hematoma 6 months earlier b. A 58-year-old executive with a bleeding ulcer c. A 44-year-old individual who had a seizure at the onset of a stroke d. A 40-year-old individual who is taking warfarin (Coumadin) and has an INR of 2.5 e. A 19-year-old young adult with leukemia with a platelet count of 200,000 ANS: A, E The criteria for exclusion are a head injury within the last 3 months, a platelet count less than 100,000, active gastrointestinal bleeding, current treatment with an anticoagulant, and a seizure noted at the time of the CVA. DIF: Cognitive Level: Application REF: p. 407 OBJ: 6 TOP: Drugs to Treat CVA KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 4. Which home modifications will support rehabilitation for a patient who had a stroke? (Select all that apply.) a. Raised commode seat b. Provision of a seat in the shower c. Availability of soft, low chairs d. Bathtub handrails e. Bright-colored scatter rugs ANS: A, B, D A raised commode seat, a seat in the shower, and bathtub rails assist the patient who is recovering from a stroke with self-care. Low chairs are difficult to manage, and scatter rugs pose a hazard for falls. DIF: Cognitive Level: Comprehension REF: p. 417 OBJ: 8 TOP: Home Modification KEY: Nursing Process Step: Planning MSC: NCLEX Physiological Integrity: Reduction of Risk 5. What causes the 5% of strokes known to occur in persons younger than 45 years of age? (Select all that apply.) a. Drug abuse b. Alcohol abuse c. Birth control pills d. Sickle cell anemia e. Hemophilia ANS: A, C, D Strokes in younger people are caused by drug abuse, birth control pills, sickle cell anemia, leukemia, atrial fibrillation, and rheumatic fever. Alcohol abuse and hemophilia do not have a causative role in stroke. DIF: Cognitive Level: Knowledge REF: p. 398 OBJ: 3 TOP: Stroke in Young Persons KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. Approximately 30% of individuals who experience a TIA have a stroke within years. (Use numeric characters only.) ANS: 5 Approximately 30% of individuals who experience a TIA have a stroke within 5 years. DIF: Cognitive Level: Knowledge REF: p. 399 OBJ: 1 TOP: TIA/CVA KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 24: Spinal Cord Injury Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse explains that the spinal cord extends from the brainstem to the level of which vertebra? a. Last thoracic b. Second lumbar c. First sacral d. Coccygeal ANS: B The cord starts at the brainstem and extends to the second lumbar vertebra. DIF: Cognitive Level: Knowledge REF: p. 424 OBJ: 1 TOP: Anatomy and Physiology of the Central Nervous System (CNS) KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. On admission to the emergency department, a patient with a C5 compression fracture can move only his head and has flaccid paralysis of all extremities. The distraught family asks if the paralysis is permanent. What is the best response by the nurse? a. “Yes. In all likelihood, the paralysis is probably permanent.” b. “No. Significant recovery of function should occur in a few days.” c. “It is too early to tell. When the spinal shock subsides, we will know more.” d. “You should talk to your physician about things of that nature.” ANS: C Spinal shock caused by swelling may last from a few days to months, clouding the issue of the true extent of the injury. DIF: Cognitive Level: Application REF: p. 427 OBJ: 3 TOP: Spinal Shock KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. Which assessment would indicate the resolution of spinal shock? a. Extension and rigidity in affected limbs b. Spastic involuntary movements in affected limbs c. Tingling and burning in affected limbs d. Voluntary purposeful movements of affected limbs ANS: B Spastic involuntary movements after a period of flaccid paralysis announce the end of spinal shock. DIF: Cognitive Level: Comprehension REF: p. 429 OBJ: 3 TOP: Resolution of Spinal Shock KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. Which assessment leads the emergency department nurse to suspect that a patient’s spinal cord injury (SCI) is below C4? a. Voluntary eye movement b. Ability to blink the eyelids c. Unlabored respiration d. Ability to make a facial grimace ANS: C The phrenic nerve, which is at C1 to C4, controls the diaphragm and intercostal function for ventilation. DIF: Cognitive Level: Comprehension REF: p. 427 OBJ: 3 TOP: Level of SCIs KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. During a neurologic assessment, a nurse asks a patient to dorsiflex the foot against the resistance of the nurse’s hand. The patient is unable to perform this action. Where does this assessment confirm that cord damage has occurred? a. C4 to C5 b. L2 to L4 c. L5 d. S1 ANS: C The muscle group that controls the feet is at L5. DIF: Cognitive Level: Comprehension REF: p. 427 OBJ: 2 TOP: Neurologic Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 6. What technique should the nurse implement to move the impaired legs of a patient with an SCI to avoid stimulation muscle spasm? a. Firmly grasping the calf muscle and the thigh muscle b. Manipulating the limb by supporting the knee and ankle joints c. Holding the foot upright and slowly dragging the limb into position d. Requesting assistance to support the calf and thigh ANS: B Undue muscle stimulation can cause spasticity. Using the joint locations to support limbs when repositioning them reduces likelihood of spasticity. DIF: Cognitive Level: Application REF: p. 429 OBJ: 3 TOP: Spasticity KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. Which technique of opening the airway in the newly admitted patient with an SCI is the most appropriate? a. Chin lift b. Head tilt c. Jaw thrust d. Neck flexion ANS: C The jaw thrust does not require spinal movement. DIF: Cognitive Level: Comprehension REF: p. 430 OBJ: 6 TOP: Opening Airway KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 8. Brown-Séquard syndrome results in which neurologic deficit? a. Bilateral loss of pain sensation below the level of injury b. Bilateral loss of temperature and motor function below the level of injury c. Motor and sensory loss in the upper extremities only d. Ipsilateral loss of motor function and contralateral loss of pain sensation and temperature ANS: D Brown-Séquard syndrome is a hemisection of the cord resulting in ipsilateral motor loss and contralateral loss of pain and temperature. DIF: Cognitive Level: Knowledge REF: p. 427 OBJ: 3 TOP: Brown-Séquard Syndrome KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. Which level of independence is an appropriate nursing care plan goal for a patient with a C8 transection? a. Manage a mechanical wheelchair with a joystick. b. Manage a mechanical wheelchair with hand control. c. Manage a specially equipped wheelchair. d. Manage an ordinary wheelchair. ANS: D Upper extremity mobility and enhanced hand grip allow the use of an ordinary wheelchair by an individual with a C8 level SCI. DIF: Cognitive Level: Application REF: p. 428 OBJ: 6 TOP: Goal for Rehabilitation KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. A paraplegic patient excitedly reports seeing his foot move when he was being turned. How is this phenomenon best explained? a. Reflexive movement b. Return of motor function c. Early symptom of autonomic dysreflexia d. Result of hypertonicity of the muscle ANS: A Reflexive action is a movement that does not require communication to the brain via the spinal cord. DIF: Cognitive Level: Comprehension REF: p. 424 OBJ: 5 TOP: Reflexive Motion KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. After spinal shock has been resolved, an indwelling catheter is removed. What way should the nurse expect this patient to empty the bladder? a. Manual expression (Credé method) b. Spontaneous reflexive action c. Normal voluntary control d. Self-catheterization ANS: B After spinal shock resolves, spasticity of the bladder causes spontaneous emptying. DIF: Cognitive Level: Comprehension REF: p. 429 OBJ: 6 TOP: Bladder Control KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. A distressed family member asks about the purpose of the Gardner-Wells tongs. Which is the most helpful explanation by the nurse regarding the action of Gardner-Wells tongs? a. Compress the cervical vertebrae. b. Immobilize the head. c. Allow the patient to be moved out of bed. d. Align the cervical vertebrae. ANS: D The Gardner-Wells tongs are secured to the skull to separate and align the cervical vertebrae, but they do not immobilize the head. When the tongs are in place, the patient is bedridden. DIF: Cognitive Level: Comprehension REF: p. 430 OBJ: 4 TOP: Gardner-Wells Tongs KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. What is the major advantage of the halo device over the Gardner-Wells tongs? a. Separates the cervical vertebrae b. Allows the patient out of bed c. Aligns the cervical spine d. Relieves pain ANS: B The halo device and the Gardner-Wells tongs do exactly the same thing in terms of separation and alignment. The only advantage of the halo device is the mobility it allows. Neither traction modality specifically relieves pain. DIF: Cognitive Level: Comprehension REF: p. 518 OBJ: 4 TOP: Halo Device KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A patient is receiving methylprednisolone. What purpose should the nurse explain this drug has in treating a patient with an SCI? a. Reduces spinal cord cellular damage b. Counteracts spinal shock c. Increases blood supply to the injured cord d. Enhances sexual function ANS: A Methylprednisolone, if given within the first 8 hours of the injury, can significantly reduce cellular damage to the cord. DIF: Cognitive Level: Knowledge REF: p. 431 OBJ: 4 TOP: Methylprednisolone KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 15. A patient with an SCI begins to have seizures, and the blood pressure (BP) rises rapidly to 210/160 mm Hg. Which is the third indicator of the syndrome of autonomic dysreflexia? a. Profuse vomiting b. Hives on face and neck c. Excessive urine output d. Bradycardia ANS: D Bradycardia, hypertension, and seizure are the three signs of autonomic dysreflexia. DIF: Cognitive Level: Knowledge REF: p. 433 OBJ: 3 TOP: Autonomic Dysreflexia KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 16. What should be the immediate intervention when a nurse recognizes autonomic dysreflexia in the patient with an SCI? a. Flex the patient’s legs using the knee gatch of the bed. b. Cool the patient with alcohol solution. c. Raise the head of the bed to at least 45 degrees. d. Administer oxygen per mask. ANS: C Raising the head of the bed reduces the BP. Flexed legs, cooling, and oxygen will not alleviate the syndrome. DIF: Cognitive Level: Application REF: p. 433 OBJ: 6 TOP: Autonomic Dysreflexia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. Which intervention by a nurse is effective in the prevention of autonomic dysreflexia in the patient with an SCI? a. Ensure patency of the urinary catheter. b. Give warm baths to the patient to stimulate vasodilation. c. Keep lighting at a minimum to reduce stimulation. d. Offer the patient four or five small meals daily. ANS: A A distended bladder, constipation, and sudden jarring can all set off autonomic dysreflexia. Vagal stimulation retards vasodilation. The number and size of meals have no effect on preventing this syndrome. DIF: Cognitive Level: Application REF: p. 428 OBJ: 6 TOP: Autonomic Dysreflexia KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 18. The family members of a patient with an SCI, who is in the rehabilitation phase, want to take the patient outdoors for a visit. It is 90 F outside and very humid. What should the nurse suggest? a. Do not go outside at all but remain in the hospital. b. Take a spray bottle to spray water to cool the patient by evaporation. c. Take a light sweater to insulate the patient. d. Have the patient drink at least 32 oz of water during the outing. ANS: B Water will evaporate and cool the patient, similar to perspiration. DIF: Cognitive Level: Application REF: p. 435 OBJ: 3 TOP: Impaired Thermal Regulation KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 19. A nurse notes that no urinary output has occurred in a patient who underwent a laminectomy 2 hours earlier. What action should the nurse implement? a. Continue to monitor. b. Inform the charge nurse. c. Perform intermittent catheterizations. d. Turn the patient to the right side. ANS: A The nurse should continue to monitor the patient for urine output. Two hours is too soon to expect a continent patient to void. Informing the charge nurse and catheterization are not necessary. Turning this patient to the side is contraindicated. DIF: Cognitive Level: Application REF: p. 437 OBJ: 8 TOP: Postoperative Care for Laminectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. Which statement made by a male patient with an SCI could be assessed as a positive adaptation to sexual dysfunction? a. “I know I will never have a sexual relationship again.” b. “I need some suggestions as to how to direct my sexual energy into gardening or painting. or just anything.” c. “Can you arrange an appointment with a sex counselor so I can begin to examine alternative methods of sexual activity?” d. “I think that after a while I will be able to have sexual relationships just like I had before my accident.” ANS: C Seeking help from a counselor indicates an acceptance of learning alternative techniques. Remarks eliminating all possibilities of a sexual relationship are defeatist remarks and are not positive. However, a patient should realize that his or her sexual relationships will alter as a result of the SCI. DIF: Cognitive Level: Analysis REF: p. 435 OBJ: 7 TOP: Sexual Dysfunction KEY: Nursing Process Step: Evaluation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 21. What should a nurse emphasize regarding the rehabilitation of the patient with an SCI? a. Rehabilitation is usually achieved within a few months after stabilization. b. Rehabilitation will return the patient with an SCI to the preaccident functional level. c. Rehabilitation focuses on adjustments necessary to reenter society and the workplace. d. Rehabilitation completely targets self-care. ANS: C The goals of rehabilitation are modification of lifestyle, as well as expectations and adjustments, necessary to attain the highest level of independence possible. DIF: Cognitive Level: Comprehension REF: p. 436 OBJ: 7 TOP: Rehabilitation KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 22. What should a nurse include in a patient’s plan of care when considering interventions for the outcome of prevention of contractures in a patient with an SCI? a. Apply cold wraps to the limbs twice a day. b. Perform full ROM exercises every 2 hours. c. Use significant tactile stimuli each shift. d. Apply splints to the limbs. ANS: D Applying splints will reduce contractures. Cold application, agitation of the limb with ROM exercises too frequently, and tactile stimuli increase spasticity. DIF: Cognitive Level: Application REF: p. 434 OBJ: 7 TOP: Rehabilitation KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 23. The family of a patient with an SCI is concerned with the lack of bowel function 2 days after the injury. What is the best response by the nurse? a. “Because of his injury, he will always need to have enemas for bowel evacuation.” b. “Medical management is delaying bowel action because it places pressure on the injury.” c. “Bowel function should return in approximately 3 days after the accident.” d. “We’ll just have to wait and see if bowel action returns this week.” ANS: C Bowel action usually returns with peristalsis on the third day after the accident. The bowel responds to dilation from the content in the bowel and moves without voluntary action from the patient. DIF: Cognitive Level: Application REF: p. 434 OBJ: 1 TOP: Impaired Bowel Function KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 24. A home health nurse encourages the family of a patient with an SCI to use the assisted cough technique. What does this technique require the caregiver to do? a. Assist the patient to inhale a bronchodilator spray and then cough. b. Forcefully press on patient’s back below the rib cage while the patient is in the prone position. c. Assist the patient to lean forward, breathe deep, and then cough. d. Apply pressure to diaphragm as the patient coughs. e. Slap the patient on upper back while the patient is in the prone position. ANS: D To assist the patient with an SCI to cough, the caregiver applies pressure on the diaphragm as the patient attempts to cough after having taken a deep breath. DIF: Cognitive Level: Comprehension REF: p. 433 OBJ: 6 TOP: Assisted Cough KEY: Nursing Process Step: Intervention MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. What has occurred in the past 10 years to enhance rehabilitation of individuals with SCIs? (Select all that apply.) a. Technologically advanced assistive aids b. Rehabilitation personnel c. Development of trauma centers d. Health insurance e. Rapid transport of victims ANS: A, C, E New assistive aids, the development of decentralized trauma centers, and the rapid transport of victims have all increased the potential for rehabilitation. Rehabilitation personnel and health insurance are not new. DIF: Cognitive Level: Knowledge REF: p. 422 OBJ: 7 TOP: Enhanced Rehabilitation Potential KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. What changes occur with the intervertebral disks in older adults that increase the risk of injury? (Select all that apply.) a. Fill with calcium deposits b. Are less shock absorbent c. Are herniated d. Enlarge and swell e. Lose water ANS: B, E Age affects the water content in intervertebral disks, which makes them less able to absorb shock. Herniation and swelling can occur at any age. Disks do not fill with calcium. DIF: Cognitive Level: Knowledge REF: p. 424 OBJ: 2 TOP: Age-Related Changes to Intervertebral Disks KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A nurse is caring for a despondent young female patient with an SCI at C5. The patient verbalizes concern regarding sexual dysfunction. What should the nurse assure this patient she can still experience? (Select all that apply.) a. Vaginal sensation b. Vaginal orgasm c. Normal menses d. Intercourse e. Children ANS: C, D, E Intercourse, normal menses, and childbirth are all possible for a woman with a C5 lesion, but no vaginal sensation occurs. Orgasm is possible but not vaginally stimulated. DIF: Cognitive Level: Comprehension REF: p. 429 OBJ: 3 TOP: Risk for Sexual Dysfunction KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 25: Respiratory System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What portion of the internal nose traps particles and kills bacteria? a. Turbinates b. Mucous membrane c. Vestibular formations d. Cilia ANS: B The mucous membrane traps particles and bacteria that are inhaled; then an enzyme in the mucus destroys them. The cilia then sweep the particles into the throat to be swallowed. DIF: Cognitive Level: Knowledge REF: p. 440 OBJ: 1 TOP: Anatomy and Physiology of the Nose KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A patient comes into the clinic complaining of a runny nose and facial pain. What should the nurse’s initial assessment include? a. Assessment for nasal drainage and sinus tenderness b. Transillumination and nasal speculum examination c. Palpation of the frontal and maxillary sinuses and tonsillar inspection d. Turbinate assessment and assessment for patency of the nares ANS: A The assessment of the characteristics of the nasal drainage and location of the facial pain would be the first evaluation for sinusitis. DIF: Cognitive Level: Application REF: pp. 443-444 OBJ: 2 TOP: Physical Examination of the Nose KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A 68-year-old patient tells the nurse that her sense of smell is not as acute as before, her nose is drier, and she occasionally gets a nosebleed. What should the nurse suspect? a. An infection b. Normal age-related changes c. A nasal defect d. Allergies that are causing her symptoms ANS: B These options describe normal age-related changes. A suggestion that would make the patient more comfortable would be to use a humidifier to keep the mucous membranes moist. DIF: Cognitive Level: Application REF: p. 443 OBJ: 2 TOP: Age-Related Changes in the Nose and Sinuses KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. What does age-related relaxation of the esophageal sphincter in a 70-year-old patient cause? a. Excessive belching b. Dumping syndrome c. Tickling sensation, requiring frequent coughing d. Burning in the throat when lying down ANS: D A common age-related change in the throat is a weakened esophageal sphincter. This allows gastric contents to flow back up into the throat and irritate the larynx. Elevating the head of the bed is a common treatment. DIF: Cognitive Level: Comprehension REF: p. 442 OBJ: 4 TOP: Age-Related Changes KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. When a patient with sleep apnea says, “I’m not wearing that silly mask. I look like something out of Star Wars,” what should the nurse remind the patient about the function of the mask? a. Increases oxygen intake b. Stimulates regular respirations c. Sounds an alarm when the oxygen concentration drops d. Uses positive pressure to keep the airway open ANS: D The sleep apnea mask, through positive pressure, keeps the airway open during sleep. DIF: Cognitive Level: Comprehension REF: p. 463 OBJ: 4 TOP: Sleep Apnea Mask KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. What should patient education for a patient being given nose drops for the first time include? a. Asking the patient to sit down and tip her head to the side to allow for a better angle for the instillation of the drops b. Holding the dropper against the side of the nose so that all the medication flows into the nares c. Asking the patient to return any unused medication to the bottle d. Tipping the head back and holding the dropper over the nostril and then telling the patient to keep her head back for a few minutes ANS: D Appropriate instillation of nose drops requires that the head be tipped back and the bottle not touch the nose. DIF: Cognitive Level: Comprehension REF: p. 453 OBJ: 3 TOP: Nose Drops KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. A patient comes into the clinic complaining of waking up with a dry mouth and nose and asks if the dryness has caused the colds she has had in the past few months. What is the most appropriate suggestion for the nurse to suggest? a. Use a humidifier at home. b. Get a throat culture. c. Get a nose culture. d. Request an antibiotic. ANS: A A humidifier would be helpful in keeping the nasal mucous membranes moist, which can decrease nasal infections. DIF: Cognitive Level: Analysis REF: p. 459 OBJ: 3 TOP: Humidification KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. Which assessment should indicate the necessity for a nurse to suction a patient with a tracheostomy? a. Becomes restless and has increases in vital signs b. Has decreased peak airway pressure c. Shows diaphoresis d. Is coughing frothy mucus ANS: A The patient signals the need for suctioning by increased restlessness and an increase in vital signs. Peak airway pressures increase when suctioning is necessary. Frothy mucus is an expectation. DIF: Cognitive Level: Application REF: p. 459 OBJ: 3 TOP: Suctioning KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Reduction of Risk 9. Which position is the most appropriate for a patient returning from surgery with a nasal pack and mustache dressing? a. Side-lying position to prevent aspiration of drainage b. Semi-Fowler position and apply a warm compress to reduce pain c. High Fowler position and apply a cold dressing to reduce swelling d. Sims position and apply a cold dressing to facilitate drainage and reduce swelling ANS: C Patients who have a nasal pack should be placed in semi- or high Fowler position with a cold dressing. The position and cold dressing will reduce swelling. Any side-lying position makes it more difficult for the patient to breathe with a nasal pack in place. DIF: Cognitive Level: Application REF: p. 466 OBJ: 4 TOP: Nasal Pack KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. What intervention should a nurse implement when providing tracheostomy care? a. Wash and rinse the inner cannula in tap water and then dry it. b. Use a sterile solution of normal saline or other solution to wash the inner cannula and then rinse with sterile water. c. Clean the area around the stoma with tap water and a gentle soap. d. Remove the inner cannula, wash both hands with a bactericidal soap, and then don sterile gloves to clean the inner cannula. ANS: B The recommendation is to use a sterile technique for tracheotomy care. DIF: Cognitive Level: Application REF: p. 465 OBJ: 5 TOP: Tracheostomy Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 11. A nurse assesses wheezes in a patient with asthma. What should the nurse know is the cause of wheezes? a. Increased thickness of respiratory secretions b. Use of accessory muscles of respiration c. Tachypnea and tachycardia d. Movement of air through narrowed airways ANS: D Wheezes are adventitious sounds made by air passing through narrowed passages. DIF: Cognitive Level: Comprehension REF: p. 445 OBJ: 1 TOP: Asthma: Wheeze KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. The patient has had anterior nasal packing placed for severe epistaxis. The nurse notes that he is swallowing frequently. What should a nurse suspect? a. The patient’s throat is dry. b. Posterior packing is uncomfortable. c. The patient is bleeding. d. The patient’s saliva production is excessive. ANS: C Frequent swallowing after nasal surgery is a sign of bleeding. DIF: Cognitive Level: Analysis REF: p. 466 OBJ: 3 TOP: Epistaxis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 13. A patient asks the nurse how air goes from the nose to the lung. The nurse draws the route according to which sequence? a. Trachea, larynx, bronchi b. Pharynx, trachea, bronchi, alveoli c. Bronchi, trachea, bronchioles d. Larynx, trachea, alveoli, bronchi ANS: B The route of inspired air is pharynx, trachea, bronchi, and alveoli. DIF: Cognitive Level: Knowledge REF: p. 440 OBJ: 1 TOP: Physiology of Ventilation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A nurse charts that a patient has had periods of tachypnea during the night. What does this means in regard to the respiration rate? a. Below 12 breaths/min b. Uneven, with periods of apnea c. Gradually deepening, then shallow, and then periods of apnea d. Above 20 breaths/min ANS: D Tachypnea is a respiration rate above 20 breaths/min. Option a describes bradypnea, option b describes Biot respirations, and option c describes Cheyne-Stokes respirations. DIF: Cognitive Level: Comprehension REF: p. 443 OBJ: 1 TOP: Respiration Rate KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 15. A 90-year-old patient complains to the nurse of shortness of breath after walking up a flight of stairs. What age-related change should the nurse explain results in this problem? a. Flexible rib cage b. High-arched diaphragm c. Increased chest movement d. Enlarged bronchioles ANS: D Enlarged bronchioles require the inspiration of greater amounts of air. Other age-related changes make increased inspiration difficult. DIF: Cognitive Level: Comprehension REF: p. 443 OBJ: 2 TOP: Age-Related Changes KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 16. What should the nurse exclude when documenting the findings in the functional assessment portion of the nursing assessment for a patient with a respiratory disorder? a. Occupation b. Usual diet c. Smoking history d. Previous respiratory disorders ANS: D Previous respiratory disorders are assessed in the medical history portion of the assessment. DIF: Cognitive Level: Comprehension REF: p. 444 OBJ: 1 TOP: Respiratory Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. To auscultate breath sounds in the right middle lobe from the anterior aspect, the nurse should place the diaphragm of the stethoscope at which intercostal space? a. Second b. Third c. Fourth d. Fifth ANS: D The fifth intercostal space is the optimal position for auscultating the right middle lobe. DIF: Cognitive Level: Application REF: p. 445 OBJ: 3 TOP: Breath Sounds KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 18. What should the nurse suspect regarding the bronchus when auscultating coarse crackles in the lower right lobe? a. Partially filled with fluid b. Narrowed by spasm c. Partially filled with thick mucus d. Completely obstructed ANS: A Coarse crackles are indicative of fluid in the bronchi. Many times these sounds can be cleared by coughing. DIF: Cognitive Level: Application REF: p. 445 OBJ: 1 TOP: Breath Sounds KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity 19. A worried patient asks the nurse to explain the advantage of a fluoroscopy. What is the nurse’s best response regarding fluoroscopy? a. Shows respiratory function in motion b. Helps the physician evaluate ventilation-perfusion ratio c. Allows the physician to take tissue samples d. Facilitates the removal of fluid from the bronchi ANS: A A fluoroscopy allows the visualization of both lungs while the patient is in the process of ventilation. DIF: Cognitive Level: Comprehension REF: p. 450 OBJ: 3 TOP: Diagnostic Tests KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 20. Which nursing intervention is inappropriate in the immediate post-procedure care of a patient who has had a fiberoptic bronchoscopy? a. Place the patient in a semi-Fowler position. b. Offer fluids to assess swallowing ability. c. Assess for diminished breath sounds. d. Assess for stridor. ANS: B Patients are placed on nothing by mouth diet until the gag reflex returns. DIF: Cognitive Level: Application REF: p. 449 OBJ: 3 TOP: Diagnostic Tests KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 21. What is the importance of the nurse closely monitoring bilateral breath sounds and chest movement after a thoracentesis? a. Fluid may quickly accumulate as a result of inflammation. b. The lung may have been punctured during the procedure. c. Severe bronchospasm may cause atelectasis. d. Asthma may result after the procedure. ANS: B A possibility exists that the lung could have been punctured during the procedure. Bronchospasm, fluid collection, and asthma are not concerns related to a thoracentesis. DIF: Cognitive Level: Comprehension REF: p. 457 OBJ: 3 TOP: Diagnostic Tests KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 22. Which nursing assessment indicates a positive reading of a tuberculin (TB) skin test? a. 1 day after injection with a 10-mm area of redness and swelling b. 2 days after injection with a 5-mm area of redness and swelling c. 4 days after injection with a 3-mm area of redness and swelling d. 5 days after injection with a 2-mm area of redness and swelling ANS: B A positive reading of a TB skin test is an area of redness and swelling of 5 mm or larger 24 to 48 hours after injection. DIF: Cognitive Level: Comprehension REF: p. 458 OBJ: 3 TOP: Diagnostic Tests KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 23. A nurse performs an Allen test before performing the arterial stick for an arterial blood gas. What does this test assess? a. Respiratory function b. Tidal volume c. Concentration of oxygen d. Perfusion of the hand ANS: D The perfusion of the hand by the radial and ulnar arteries is assessed because the puncture of the radial artery might cause it to occlude. DIF: Cognitive Level: Comprehension REF: p. 451 OBJ: 3 TOP: Diagnostic Tests KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 24. A patient who is severely dyspneic and cyanotic enters the emergency department. What rate should a nurse administer oxygen to the patient? a. 2 L to preserve the hypoxic drive b. 6 L to relieve the dyspnea c. 8 L, humidified, to liquefy secretions d. 10 L, humidified aerosol, to dilate the bronchi ANS: A Low-dose oxygen is a safe initial dose to ensure that the hypoxic drive be preserved, especially for a patient whose history is unknown. DIF: Cognitive Level: Application REF: pp. 460-461 OBJ: 4 TOP: Oxygen Administration KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 25. Which assessment indicates to the nurse that the chest tube in a water seal drainage device is working correctly? a. Constant bubbling in the suction control chamber b. Decrease of accumulation in the drainage chamber c. Fluctuation of the column of water in the water seal d. Constant bubbling in the water seal chamber ANS: C The fluctuation of the level in the water seal indicates patency of the tubes with the reinflating lung. Constant bubbling in the wet suction control is normal. Constant bubbling in the water seal indicates an air leak. Decreasing drainage is normal. DIF: Cognitive Level: Comprehension REF: p. 463 OBJ: 4 TOP: Water Seal Drainage KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 26. Which assessment by the nurse at the bedside of a patient with a chest tube attached to a water seal drainage device should require intervention? a. Dependent loops in the chest tube b. Patient in a semi-Fowler position c. Changing level of water in the water seal chamber d. Increased level of drainage to 20 mL in 8 hours ANS: A Dependent loops in the chest tube can collect drainage and occlude the system. DIF: Cognitive Level: Application REF: p. 463 OBJ: 4 TOP: Water Seal Drainage KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 27. A home health nurse who is caring for an 88-year-old patient with severe hypertension in addition to a respiratory problem notices several drugs on the bedside table. Which medication should the nurse suggest the patient avoid? a. Aspirin b. Colace c. Expectorant d. Decongestant ANS: D Decongestants increase the blood pressure. DIF: Cognitive Level: Application REF: p. 453 OBJ: 5 TOP: Respiratory Drugs KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 28. How should a nurse position a patient who had a left pneumonectomy in the morning in an effort to enhance gas exchange? a. On the right side b. On the left side c. In a semi-Fowler position d. In a flat position with a small pillow ANS: C Elevation of the head helps gas exchange in the patient with a new pneumonectomy. A complete side-lying position on the unaffected side may cause mediastinal shift. DIF: Cognitive Level: Application REF: p. 467 OBJ: 5 TOP: Postpneumonectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 29. How should a nurse position a patient during a thoracentesis? a. Side-lying with bed in a Trendelenburg position b. High Fowler position with feet elevated c. Sitting on the side of the bed bent over bedside table d. Prone with the bed elevated ANS: C The patient sits on the side of the bed and leans the upper torso over the bedside table with the head resting on folded arms or pillows. If the patient is unable to sit up, then a side-lying position with the head of the bed elevated 30 degrees may be used. DIF: Cognitive Level: Application REF: p. 457 OBJ: 3 TOP: Thoracentesis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 30. How does the ventilator function of positive end-expiratory pressure assist the patient? a. Keeps pressure in the lungs after expiration b. Delivers 100% oxygen on inspiration c. Allows the patient to control expiratory pressure d. Delivers an inhalant medication under positive pressure ANS: A The positive end-expiratory pressure setting keeps the pressure in the lungs above the atmospheric pressure, which prevents atelectasis. DIF: Cognitive Level: Knowledge REF: p. 462 OBJ: 3 TOP: Mechanical Ventilators KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 31. The patient has had anterior nasal packing placed for severe epistaxis. The nurse notes that he is swallowing frequently. What should a nurse suspect? a. The patient’s throat is dry. b. Posterior packing is uncomfortable. c. The patient is bleeding. d. The patient’s saliva production is excessive. ANS: C Frequent swallowing after nasal surgery is a sign of bleeding. DIF: Cognitive Level: Analysis REF: p. 466 OBJ: 3 TOP: Epistaxis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. What should the postoperative care of a patient who has had nasal surgery include? (Select all that apply.) a. Changing the nasal packing when saturated b. Placing the patient in a semi-Fowler position without a pillow c. Giving frequent oral hygiene d. Providing humidification for dry mucous membranes e. Assessing the back of the throat for bleeding ANS: B, C, D, E Only the physician removes the nasal packing. The nurse may change the mustache dressing, however. DIF: Cognitive Level: Knowledge REF: p. 466 OBJ: 4 TOP: Postnasal Surgery Care KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. How should a nurse explain that the breathing pattern has been altered when a patient complains of tachypnea? (Select all that apply.) a. Increased pH levels stimulate chemoreceptors in the aorta and carotid arteries, which stimulates the phrenic nerve. b. Decreased oxygen level signals the phrenic nerve to alter the respiration rate. c. Muscles of respiration respond to the stimulus. d. The brain has become hypoxic and causes an alteration in the respiration rate. e. Deflated lung tissue results in an altered respiration rate. ANS: B, C A decreased oxygen level stimulates the phrenic nerve to signal the muscles of respiration to do the work of breathing. A decreasing pH level is the stimulus to the chemoreceptors. Neither the brain nor the lungs signal for tachypnea. DIF: Cognitive Level: Comprehension REF: p. 443 OBJ: 1 TOP: Respiration Center KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. What assessment findings would indicate respiratory dysfunction when examining a patient with respiratory difficulty? (Select all that apply.) a. Flushed facial skin b. Cyanotic nail beds c. Abdominal distention d. Curved spine e. Clubbed fingers ANS: B, C, E Clues to respiratory dysfunction are a distended abdomen, cyanotic nail beds, and clubbed fingers from inadequate oxygenation. DIF: Cognitive Level: Comprehension REF: p. 445 OBJ: 1 TOP: Clues to Respiratory Dysfunction KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. Which instructions should a nurse provide to a patient just before a scheduled spirometry test? (Select all that apply.) a. Avoid smoking 4 to 6 hours before test. b. Do not use bronchodilator medications for at least 4 hours. c. Exercise for a few minutes. d. Drink 2 glasses of fluid. e. Avoid eating. ANS: A, B Patients should not smoke, use bronchodilators, or exercise just before the test. Normal-sized meals and drinking fluids do not adversely affect the test. DIF: Cognitive Level: Comprehension REF: p. 451 OBJ: 3 TOP: Spirometry KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. A nurse computes the number of “pack-years” of a 24-year-old man who has smoked packs of cigarettes every day since he was 15 years old. This patient has pack-years. (Use only numeric characters. If the answer is not a whole number, use decimals instead of fractions.) ANS: 13.5 Pack-years are calculated by multiplying the number of years of smoking by the number of packs smoked each day. A 24-year-old patient who has smoked since he was 15 years of age = 9 years multiplied by 1.5 = 13.5. DIF: Cognitive Level: Application REF: p. 444 OBJ: 1 TOP: Pack Years KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What should a nurse do when taking a specimen for a throat culture? _ (Place the appropriate actions in the correct sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Depress the tongue with a tongue blade. b. Place the applicator in a culture tube. c. Ask the patient to tilt the head back. d. Swab the back of the throat and tonsils. ANS: CADB When collecting a specimen for throat culture the patient is asked to tilt the head back, the tongue is depressed with tongue blade, the back of the throat and tonsils are swabbed, and an applicator is placed in a culture tube. DIF: Cognitive Level: Comprehension REF: p. 446 OBJ: 2 TOP: Throat Culture Specimen KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance 3. What instructions should a nurse give to a patient when teaching deep breathing and coughing techniques? (Place the options in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Place the hand on the abdomen to check the rise and fall. b. Inhale through the nose, pause 1 to 3 seconds, and then exhale through the mouth. c. Assume a semi-Fowler position. d. Take 4 to 6 deep breaths. e. Cough deeply. ANS: CABDE The exercise is performed in a sequence to ensure open bronchioles and a good deep cough. DIF: Cognitive Level: Application REF: p. 457 OBJ: 3 TOP: Deep Breathing and Coughing KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 26: Upper Respiratory Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient complains of morning headaches, a feeling of fullness in her head, and a pain similar to that of a toothache under her eye. What should the nurse recognize that these symptoms indicate? a. Nasal polyps b. Impacted wisdom teeth c. Allergic rhinitis d. Sinusitis ANS: D Sinusitis has the classic signs of headache, sense of fullness in the head, and a sensitive area over the sinuses. DIF: Cognitive Level: Comprehension REF: p. 470 OBJ: 1 TOP: Sinusitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A patient complains that he wants an antibiotic medication for his cold. What is the best response by the nurse? a. “Antibiotics are not effective with viral infections.” b. “You will get better faster without the antibiotics.” c. “You might try echinacea or vitamin C.” d. “A cold is not that serious. Try forcing fluids.” ANS: A Antibiotics are not appropriate with colds because colds are caused by viruses. Overuse of antibiotics can promote resistant strains of bacteria to develop. DIF: Cognitive Level: Comprehension REF: p. 472 OBJ: 1 TOP: Acute Viral Coryza KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. What should the initial action of a nurse be when providing first aid to a person with spontaneous epistaxis? a. Apply direct pressure for 3 to 5 minutes. b. Have the person sit down and lean forward. c. Have the person lie down and apply an ice pack. d. Have the person clear the nasal passages by blowing the nose. ANS: B The first action is to sit down and lean forward. Applying pressure just below the nose will also help. DIF: Cognitive Level: Application REF: p. 473 OBJ: 1 TOP: Epistaxis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Reduction of Risk 4. What is true regarding bacterial pharyngitis that is untrue for viral pharyngitis? a. Has an abrupt onset b. Presents a normal complete blood count (CBC) c. Presents a negative culture d. Has no serious complications ANS: A Bacterial pharyngitis has an abrupt onset, an elevated white count on the CBC, and a positive culture and can lead to glomerulonephritis, rheumatic fever, and mastoiditis. DIF: Cognitive Level: Comprehension REF: p. 474 OBJ: 1 TOP: Bacterial Pharyngitis KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 5. Which is the best candidate for a tonsillectomy? a. A 52-year-old patient with a hearing deficit related to otitis media from tonsillitis b. A 23-year-old patient with a peritonsillar abscess c. A 34-year-old patient with enlarged tonsils and adenoids d. A 15-year-old patient with one bout of tonsillitis in the previous 12 months ANS: B The patient with the peritonsillar abscess is the most likely candidate. The hearing deficit in a middle-aged person would need more investigation before surgery. Enlarged tonsils and adenoids without a respiratory obstruction does not qualify as a need for surgery; only one episode of tonsillitis in a year does not qualify. DIF: Cognitive Level: Analysis REF: p. 476 OBJ: 1 TOP: Tonsillitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. What is best for a nurse to offer when encouraging a new patient after a tonsillectomy to increase fluids? a. Chilled citrus juices b. Tap water sipped through a straw c. Flavored popsicles to suck d. Ice cubes ANS: C Flavored popsicles provide fluid and cold applications to the surgical area. Citrus juices, the use of a straw, and ice cubes have the potential to injure the operative site. DIF: Cognitive Level: Application REF: p. 476 OBJ: 1 TOP: Posttonsillectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. What are the most common causes of laryngitis? a. Smoking and highly seasoned foods b. Alcohol and voice strain c. Nasal congestion and frequent coughing d. Respiratory infections and voice strain ANS: D Upper respiratory infections and voice strain are the most common causes of laryngitis. DIF: Cognitive Level: Knowledge REF: p. 478 OBJ: 1 TOP: Disorders of the Larynx KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. What is the most significant topic for a nurse to include in a teaching plan for a patient with frequent episodes of laryngitis? a. Observing voice rest b. Reducing smoking c. Eating warm foods d. Maintaining a consistent environmental temperature ANS: A Patients with laryngitis are advised to rest their voices. DIF: Cognitive Level: Comprehension REF: p. 478 OBJ: 2 TOP: Implementations for Laryngitis KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. A patient who has cancer of the larynx has been told that he needs a total laryngectomy. What action should this nurse consider to help the patient cope with the loss of his voice? a. Offer to have a volunteer from a local laryngectomy organization visit the patient. b. Explain in detail the available vocalization aids and techniques. c. Explain to the patient what will happen directly after the surgery. d. Notify the hospital chaplain of the patient’s needs. ANS: A Offering to request a volunteer from the laryngectomy organization is a recommended implementation to reduce the stress of losing the ability to speak. You should consult the patient before making the referral. DIF: Cognitive Level: Application REF: p. 480 OBJ: 1 TOP: Cancer of the Larynx KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 10. Which nursing concern takes priority in the care of a patient after a laryngectomy? a. Encouraging nutrition b. Avoiding infection c. Establishing a communication system d. Ensuring adequate fluid intake ANS: C Establishing a communication system with the patient who has undergone a laryngectomy is a primary concern. DIF: Cognitive Level: Application REF: p. 481 OBJ: 1 TOP: Postoperative Laryngectomy KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 11. A patient who had a laryngectomy 3 months earlier returns to the physician’s office with the complaint of increasing dyspnea. Which common postlaryngectomy complication should the nurse recognize this complaint as indicating? a. Hypertrophied stoma b. Salivary fistula c. Carotid blowout d. Tracheal stenosis ANS: D Tracheal stenosis causes the otherwise healthy recovering patient who has undergone a laryngectomy to experience increased dyspnea. DIF: Cognitive Level: Comprehension REF: p. 481 OBJ: 1 TOP: Postoperative Complications of Laryngectomy KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. What is one major postoperative difficulty for a patient having a supraglottic laryngectomy? a. Teaching the patient to use an assistive device to speak b. Coughing without letting food escape through the tracheostomy c. Taking care of the tracheostomy, because the patient will always have to have one d. Teaching the patient to swallow without aspiration ANS: D The patient who has had a supraglottic laryngectomy may never be able to swallow correctly, which could easily lead to aspiration pneumonia. DIF: Cognitive Level: Comprehension REF: p. 482 OBJ: 1 TOP: Supraglottic Laryngectomy KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. Which actions should the nurse include in a care plan to effectively assist the patient with a total laryngectomy to maintain airway clearance? (Select all that apply.) a. Turning, coughing, and deep breathing b. Placing the patient in a semi-Fowler position c. Maintaining hydration d. Attaching a tracheostomy collar e. Providing a method to communicate ANS: A, B, C, D Providing a communication method has high priority, but it is not related to airway clearance. DIF: Cognitive Level: Comprehension REF: p. 482 OBJ: 1 TOP: Maintaining Airway Clearance KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity COMPLETION 1. A nurse reminds a patient, who is to have a partial laryngectomy, that the temporary tracheostomy that he will have after the original surgery will be closed within days. (Use numeric characters only.) ANS: 5 The temporary tracheostomy, which is done as part of the partial laryngectomy surgery, is usually closed 5 days after the original surgery. DIF: Cognitive Level: Comprehension REF: p. 485 OBJ: 1 TOP: Tracheostomy in Partial Laryngectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 27: Acute Lower Respiratory Tract Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient with acute bronchitis is being discharged with a prescription for an antimicrobial medication to be taken for the next 14 days. What should the nurse stress when providing discharge teaching? a. Take the drug on an empty stomach before meals. b. Complete the entire course as prescribed. c. Maintain a thorough oral hygiene regimen. d. Maintain a daily fluid intake of 500 mL. ANS: B The entire course of the prescription should be taken to destroy the pathogen completely; otherwise, the pathogen may become resistant to the drug. DIF: Cognitive Level: Comprehension REF: p. 487 OBJ: 2 TOP: Acute Bronchitis KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. Which group of patients should a nurse advise to have a vaccination with conjugated pneumococcal? a. Adults with diabetes b. Persons 65 years and older c. Parents of children younger than 24 months d. Persons with cardiovascular disorders ANS: C The conjugated product is especially designed for young children. Unconjugated vaccine is recommended for older adults and those with cardiovascular disorders. DIF: Cognitive Level: Comprehension REF: p. 489 OBJ: 1 TOP: Pneumonia Vaccine KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. What action should a nurse implement to reduce the risk of aspiration in a patient receiving continuous enteral feedings at a rate of 70 mL/hr? a. Check the position of the tube during every shift. b. Notify the charge nurse or physician about a residual volume of 20 mL. c. Elevate the patient’s head during and for 10 minutes after feeding. d. Position the patient on the left side after the feeding. ANS: B A residual of more than 20% of the hourly rate should be reported so that the rate can be reduced (70 mL multiplied by 0.20 = 14). DIF: Cognitive Level: Application REF: p. 492 OBJ: 1 TOP: Aspiration Pneumonia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. What symptoms should a nurse expect to see in a patient with hypoxemia? a. Restlessness, tachycardia, and tachypnea b. Bradycardia, cyanosis, and restlessness c. Dyspnea, flushed face, and tachycardia d. Cyanosis, nausea, and bradycardia ANS: A The universal symptoms of hypoxemia, regardless of cause, are restlessness, tachycardia, and tachypnea. DIF: Cognitive Level: Comprehension REF: p. 490 OBJ: 2 TOP: Hypoxemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. A patient comes to the emergency department with a sucking chest wound. Which type of dressing should the nurse apply to begin the process of lung reinflation? a. Petroleum dressing covered with an airtight bandage b. No dressing at all c. Pillow weighted down with a sandbag d. Air-occlusive dressing taped on three sides (vented dressing) ANS: D The vented dressing occludes air from entering but allows air to escape, avoiding a tension pneumothorax and mediastinal shift. DIF: Cognitive Level: Application REF: p. 493 OBJ: 1 TOP: Pneumothorax Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. What should a nurse prepare when assessing paradoxical movement in a patient with a flail chest who has significant dyspnea? a. Thoracotomy b. Intubation c. Thoracentesis d. Body cast ANS: B A patient with an unstable chest usually requires intubation and mechanical ventilation. DIF: Cognitive Level: Application REF: p. 496 OBJ: 1 TOP: Flail Chest KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. Which intervention would be inappropriate for decreasing the risk of further emboli in a patient with a pulmonary embolism? a. Carefully applying compression stockings b. Performing passive range-of-motion exercises, especially of the lower limbs c. Placing pillows under the knees to elevate the legs d. Ambulating frequently ANS: C Nothing should be placed under the knees; doing so might impair circulation. DIF: Cognitive Level: Application REF: p. 498 OBJ: 2 TOP: Pulmonary Embolism KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort COMPLETION 1. Assessment of 24-year-old driver after an automobile accident, who is complaining of right-sided chest pain and is dyspneic, reveals the following: • Respirations: 26 breaths/min • Significant pain on inspiration • Hand is pressed to the rib area; large bruise is forming on the right chest • Blood pressure: 182/98 mm Hg Based on these assessments, the nurse suspects ribs. ANS: fractured The placement of the bruise and the pain on inspiration are the main clues to the rib fracture. DIF: Cognitive Level: Analysis REF: p. 496 OBJ: 1 TOP: Rib Fracture KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 28: Chronic Lower Respiratory Tract Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is caring for a patient with asthma and assesses signs and symptoms of inadequate oxygenation. Which intervention is the most appropriate? a. Provide postural drainage. b. Administer oxygen (O2) at 8 L/min. c. Position the patient flat in bed with small pillow. d. Increase fluid intake. ANS: D Increasing fluid intake thins the mucus in the lungs, making it easier to cough up, which helps clear the bronchioles and decrease ventilation-perfusion mismatch. Increasing O2 is not helpful if no air pathway exists to the alveoli. Increasing O2 to 8 L is excessive. DIF: Cognitive Level: Application REF: p. 508 OBJ: 3 TOP: Asthma KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. What is a characteristic of chronic obstructive pulmonary disease that places a patient at risk for poor nutrition? a. Increased metabolism b. Anxiety c. Chronic constipation d. Excessive respiratory effort ANS: D Respiratory effort interferes with swallowing, depletes energy, and increases caloric needs. DIF: Cognitive Level: Comprehension REF: p. 512 OBJ: 3 TOP: COPD: Nutrition KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. Which nursing intervention enhances the nutritional status of a patient with COPD? a. Offer small, frequent meals. b. Encourage extra liquids with meals. c. Assist the patient to exercise before meals. d. Supply information about nutrition. ANS: A Small meals are not as tiring for the patient and are more appealing. DIF: Cognitive Level: Application REF: p. 517 OBJ: 3 TOP: COPD: Nutrition KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. Which walking program would be the most effective for the nurse to recommend as part of a progressive walking program for an obese patient with COPD? a. 10 to 15 minutes a day b. 20 to 30 minutes a day c. 45 to 60 minutes a day d. Up to 2 hours a day ANS: A Walking for as little as 10 to 15 minutes a day and progressing up to 45 minutes a day has proven beneficial for persons with COPD because it improves oxygenation and helps with weight loss. DIF: Cognitive Level: Application REF: p. 512 OBJ: 3 TOP: Exercise for the Patient with COPD KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. What is the result of status asthmaticus that is not corrected? a. Pneumothorax, severe hypoxemia, and respiratory arrest b. Hypertension, cerebrovascular accident (CVA), and cardiac arrest c. Respiratory alkalosis, pneumonia, and death d. Lung abscess, cor pulmonale, and respiratory failure ANS: A Status asthmaticus, because of severe bronchospasms, can result in hypoxemia, which could lead to pneumothorax and arrest. DIF: Cognitive Level: Comprehension REF: p. 503 OBJ: 2 TOP: Status Asthmaticus KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. What should a nurse focus on when assessing for major sources of infection in a patient with COPD? a. Stasis of respiratory secretions b. Low body weight c. Episodes of postural hypotension d. Delayed antigen-antibody response ANS: A Retained static secretions in the lungs are major sources of bacterial infiltration and infection. DIF: Cognitive Level: Application REF: p. 514 OBJ: 2 TOP: COPD: Infection KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. A young patient with acquired immunodeficiency syndrome (AIDS) reports debilitating night sweats. Why should the home health nurse suggest that the patient visit the clinic? a. To get a prescription for antibiotics b. Tuberculosis (TB) screening c. Complete blood count (CBC) d. Treatment with an aerosol inhalant ANS: B The symptoms of TB are low-grade fever, night sweats, and cough. Patients with AIDS and anyone who is immunosuppressed are extremely prone to TB and should be carefully monitored for the development of the disease. DIF: Cognitive Level: Application REF: p. 519 OBJ: 2 TOP: Tuberculosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. A nurse is caring for an 80-year-old patient with COPD and suspects right-sided heart failure after assessing and recording the data. What should decrease with right-sided heart failure? a. Blood pressure b. Urine output c. Respirations d. Heart rate ANS: B The decreasing urine output is one of the signs. The fluid, instead of being excreted as urine, is trapped in the tissues as edema. Blood pressure, respirations, and heart rate will increase with right-sided heart failure. DIF: Cognitive Level: Comprehension REF: p. 517 OBJ: 2 TOP: Dyspnea KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. A patient with TB asks the nurse how long he will have to take his TB medications. What is the nurse’s best response? a. “Generally about 2 weeks.” b. “Depending on the drug, it may be as long as 2 years.” c. “TB drugs are usually taken throughout the life span.” d. “People frequently ask that question. It depends on many things.” ANS: B Some TB drugs are continued over the course of several years. DIF: Cognitive Level: Knowledge REF: p. 524 OBJ: 2 TOP: TB Drug Protocol KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Pharmacological Therapies 10. A patient with TB asks how to protect family members from the disease. Which discharge instruction given by the nurse is most informative? a. “Your family will need to take treatments to prevent infection.” b. “You will need to wear a mask at home to protect your family members.” c. “You should always cover your mouth and nose if coughing or sneezing.” d. “You should avoid intimate contact with everyone.” ANS: C Covering the mouth and nose to prevent droplet spread and carefully disposing of tissues are two significant ways to control the spread of infection. Masks or isolation is not necessary because before discharge, the patient will have been stabilized on an anti-TB medication. DIF: Cognitive Level: Application REF: p. 521 OBJ: 2 TOP: TB Infection Control KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 11. A nurse is providing education to a patient taking rifampin as a result of an exposure to TB. What side effect of this drug should the nurse include? a. Extreme drowsiness b. Illness if aged cheese or smoked meats are consumed c. Body fluids to become red-orange d. Oral contraceptive pills to become ineffective ANS: C Rifampin will color body fluids red-orange and will result in stained clothing and soft contact lenses. DIF: Cognitive Level: Comprehension REF: p. 521 OBJ: 2 TOP: Rifampin KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. A patient with asthma asks the purpose of learning how to use a peak expiratory flow rate (PEFR) device. What is the nurse’s best response regarding PEFR? a. Dilates the bronchi to relieve dyspnea b. Measures expired air to evaluate ventilation c. Soothes inflamed bronchi, reducing spasm d. Liquefies sputum for easier expectoration ANS: B The PEFR measures expired air. When the PEFR rate decreases 20% below the baseline, adjustments are usually made in the medications. DIF: Cognitive Level: Comprehension REF: p. 506 OBJ: 3 TOP: Peak Expiratory Flow Rate (PEFR) KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. A nurse is assigned to care for a patient with the diagnosis of centriacinar (centrilobar) emphysema. What is a characteristic of this type of emphysema? a. No significant smoking history in the patient b. Enlarged and broken down bronchioles with intact alveoli c. Hypoelastic bronchi and bronchioles d. Deficiency of the enzyme inhibitor alpha1-antitrypsin. ANS: B This type of emphysema is characterized by a long smoking history, enlarged and broken down bronchioles, and hypoelastic bronchi. DIF: Cognitive Level: Knowledge REF: p. 509 OBJ: 2 TOP: Emphysema KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A 25-year-old patient with cystic fibrosis (CF) tells the home health nurse that he wants to take a nice vacation. What is the best suggestion for the nurse to make? a. Greece in July b. Colorado in May c. New York in November d. The Mexican coast in August ANS: C New York is the best choice because individuals with CF sweat profusely and lose many salts, leading to significant electrolyte imbalance. Those with CF also have impaired respiration and should avoid heat (Greece in July, Mexico in August) and higher altitudes (Colorado at any time). DIF: Cognitive Level: Application REF: p. 518 OBJ: 2 TOP: Cystic Fibrosis: Avoiding Heat KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 15. Which assessment made by a nurse indicates that respiratory arrest is imminent in a patient with asthma? a. Agitation b. Tachycardia c. Absence of wheezing d. Flaring nares ANS: C An absence of wheezing indicates a diminished ventilation effort. DIF: Cognitive Level: Comprehension REF: p. 503 OBJ: 2 TOP: Asthma: Respiratory Arrest KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 16. A patient with COPD is observed to have extreme shortness of breath when ambulating. Which nursing intervention is most inappropriate? a. Bunch all nursing activities and treatments close together. b. Schedule rest periods during the day. c. Assist the patient only when needed to encourage independence. d. Provide daily ambulation to build tolerance. ANS: A Bunching nursing activities is tiring to the patient with COPD. Assisting only when needed saves patient energy, as well as enhancing independence. Activities should be spread out to allow for uninterrupted rest periods. Progressive ambulation is an acceptable way to build tolerance. DIF: Cognitive Level: Application REF: p. 517 OBJ: 3 TOP: Activity Intolerance in COPD KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 17. A nurse recognizes that a patient diagnosed with COPD has a rising level of partial pressure of carbon dioxide (CO2) in arterial blood (PaCO2). How should the nurse interpret this assessment? a. More arterial O2 is available than is needed. b. The ventilation-perfusion ratio is becoming balanced. c. Respiratory acidosis has begun. d. The anticholinergic medications are effective. ANS: C A rising PaCO2 level is acidic in nature and causes respiratory acidosis. DIF: Cognitive Level: Analysis REF: p. 507 OBJ: 2 TOP: PaCO2 KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 18. A patient with COPD asks a nurse if nicotine patches are very effective for smoking cessation. What is the best response by the nurse? a. “No. Only about 25% are successful.” b. “Yes. The success rate is between 50% and 60%.” c. “No. Prescriptions such as Wellbutrin are 90% effective.” d. “Yes. Individual success has been obtained with combination of patches and gum.” ANS: A The patches have a lower than 25% success rate. Smoking addiction is too strong to be overcome by medication or gum without a very unusual commitment from the patient. Successful smoking cessation is measured by 1 year of no smoking. DIF: Cognitive Level: Comprehension REF: p. 515 OBJ: 3 | 4 TOP: COPD: Smoking Cessation KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 19. A patient with cystic fibrosis (CF) furiously refuses any more manual chest physiotherapeutic treatment. Which alternative is appropriate for the nurse to suggest? a. Flutter mucus device b. Increase ambulation to 1 to 2 hours a day c. Steam inhalator several times a day d. Drink 3 quarts of fluid per day ANS: A A flutter mucus clearance device is a handheld vibrating tool that helps loosen and evacuate secretions in the lung. DIF: Cognitive Level: Application REF: p. 518 OBJ: 3 TOP: Cystic Fibrosis KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. What should a nurse expect when assessing the CBC results of a patient with chronic bronchitis? a. Decreased platelets b. Decreased white blood cells (WBCs) c. Increased eosinophils d. Increased red blood cells (RBCs) ANS: D Patients with chronic bronchitis show a large increase of RBCs with an attendant higher hemoglobin level because they must produce more RBCs for the transport of O2. Frequently, the WBCs are elevated because of the chronic inflammation. Decreased levels of platelets and increased eosinophils are indicative of pathologic characteristics other than bronchitis. DIF: Cognitive Level: Comprehension REF: p. 511 OBJ: 2 TOP: Chronic Bronchitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 21. A patient with COPD delightedly tells the nurse that he has quit smoking and is using chewing tobacco. What is the most appropriate nursing intervention? a. Congratulate him on his quitting smoking. b. Warn him of the dangers of oral cancer. c. Suggest that he add nicotine patches in addition to the chewing tobacco. d. Point out that he is still addicted and is using tobacco. ANS: B Smokeless tobacco has adverse effects, including oral cancer. DIF: Cognitive Level: Application REF: p. 516 OBJ: 2 TOP: COPD: Quit Smoking KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 22. A newly diagnosed patient with non–small cell lung carcinoma (NSCLC) is anxious about upcoming surgery. Which intervention by the nurse would be most helpful? a. Support the patient in preparation for surgery. b. Educate the patient regarding the high survival rate with this type of carcinoma. c. Assure the patient that chemotherapy and radiation can be used in this sort of cancer. d. Refer the patient to the American Cancer Society for postdischarge follow-up. ANS: A Surgery is the treatment of choice of NSCLC carcinomas. The survival rate is only approximately 14%. Although referral may be in the long-range plan, the patient’s need is immediate for information that is within the scope of nursing. DIF: Cognitive Level: Comprehension REF: p. 524 OBJ: 3 TOP: NSCLC KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 23. A nurse documents and reports the presence of foul, bulky stool in a patient with cystic fibrosis (CF). What does this finding indicate about the patient? a. Is being adequately maintained on the present dose of pancreatic enzyme b. Is not adequately digesting food c. Has diarrhea related to excess mucus in the bowel d. Has inadequate hydration ANS: B Foul, bulky stools are the result of inadequately digested food if oral pancreatic enzymes are inadequate. DIF: Cognitive Level: Application REF: p. 518 OBJ: 3 TOP: Foul Stools with Cystic Fibrosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 24. What should a patient who had the BCG (Bacillus Calmette-Guérin) vaccine 2 years ago anticipate? a. False-positive result from TB skin tests b. Being at risk for contracting TB c. 3-week prophylactic protocol of rifampin or isoniazid (isonicotinic acid hydrazide [INH]) d. Needing a booster every 2 years ANS: A Inoculation with BCG causes a false-positive result on TB skin tests that may be administered afterward. BCG is not used very much in the United States, but it is administered in most other countries. DIF: Cognitive Level: Comprehension REF: p. 519 OBJ: 3 TOP: Bacillus Calmette-Guérin (BCG) Vaccine KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 25. What nursing action should be implemented to help combat anorexia in a patient with COPD? a. Recommend a large meal in the middle of the day. b. Suggest taking only cold liquid nutritional drinks. c. Perform oral hygiene before meals. d. Gently exercise for 10 minutes before a meal. ANS: C Oral hygiene freshens the mouth and removes unpleasant tastes from medications or coughed-up secretions. DIF: Cognitive Level: Application REF: p. 514 OBJ: 3 TOP: Imbalanced Nutrition KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. A nurse uses a picture to demonstrate the bullae and blebs associated with emphysema. How do blebs differ from bullae? (Select all that apply.) a. They are between the alveolar spaces in the lungs. b. They are in the lung parenchyma. c. They can rupture, causing the lungs to collapse. d. They are responsible for diaphragm flattening. e. They are precancerous. ANS: B, C Blebs are growths inside the organ of the lung that enlarge and rupture, causing lung collapse. Bullae are the lesions between the alveolar spaces. Neither are the cause of diaphragm flattening nor are they precancerous. DIF: Cognitive Level: Comprehension REF: p. 510 OBJ: 2 TOP: Blebs and Bullae of Emphysema KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. A nurse cautions a group of individuals with COPD that using O2 at levels greater than 1 to 3 L/min can cause the loss of their . ANS: hypoxic drive The hypoxic drive is the stimulus of CO2 in the system that drives respiration. If the CO2 level is reduced by excessive administration of O2, then the patient will cease to breathe. DIF: Cognitive Level: Comprehension REF: p. 512 OBJ: 2 TOP: Hypoxic Drive KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse explains to a family how the asthma attack progresses by using a progressive list of pathologic events. (Place the options in the correct sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Bronchoconstriction b. Ventilation-perfusion mismatch c. Production of mucous plugs d. Hypoxemia with compensatory hyperventilation e. Triggering of inflammatory process ANS: EACBD After the allergen has triggered the inflammatory response, bronchoconstriction occurs, which leads to the formation of mucous plugs in the bronchioles that block O2 from entering the alveoli, causing a ventilation-perfusion mismatch and resulting in hypoxemia and hyperventilation. DIF: Cognitive Level: Analysis REF: p. 503 OBJ: 2 TOP: Progression of Asthma Attack KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 29: Hematologic System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Which is considered an approximate normal hematocrit value? a. Three times the hemoglobin value b. The same as the hemoglobin value c. Four times lower than the red blood cell count d. Same as the red blood cell count ANS: A Hematocrit is approximately three times the hemoglobin value. DIF: Cognitive Level: Knowledge REF: p. 533|p. 535 OBJ: 3 TOP: Normal Laboratory Values KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse is caring for a patient receiving a transfusion and assesses that the patient is wheezing and is complaining of back pain. What nursing action should take place after stopping the transfusion? a. Discontinue the intravenous (IV) transfusion. b. Notify the charge nurse. c. Administer heparin. d. Raise the patient’s head. ANS: B The charge nurse should be notified immediately after the transfusion is stopped. The charge nurse will notify the physician and the laboratory or blood bank. The head of the bed should be raised to aid in respiration, and oxygen should be administered in high doses. The blood tubing and bag should not be discarded because the blood bank will want it to check the accuracy of the typing. DIF: Cognitive Level: Application REF: p. 539 OBJ: 4 TOP: Blood Transfusion Reactions KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. A nurse is taking the history of a patient who has come in for evaluation of large areas of purpura on her limbs. The patient reports using alternative therapy for her menopausal symptoms. What alternative therapy is most likely responsible for the patient’s symptoms? a. Black cohosh b. Valerian c. Lavender d. Rosemary ANS: A Black cohosh interferes with blood clotting. DIF: Cognitive Level: Comprehension REF: p. 533 OBJ: 2 TOP: Alternative Remedies KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. To what level should the platelet count rise when the patient with a platelet count of 20,000/mm3 receives 1 unit of platelets? a. 25,000 to 30,000/mm3 b. 35,000 to 40,000/mm3 c. 45,000 to 50,000/mm3 d. 55,000 to 100,000/mm3 ANS: A Platelet transfusions are given when the platelet count falls below 20,000/mm3. One unit is expected to raise the count by 5000 to 10,000/mm3. DIF: Cognitive Level: Knowledge REF: p. 538 OBJ: 4 TOP: Platelet Transfusion KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 5. When a nurse is preparing to give ferrous sulfate (Feosol) to a home health care patient, what is the most appropriate nursing action to implement? a. Mix the drug with a high-protein milkshake. b. Give it undiluted with a small snack. c. Mix it with coffee or cola to disguise the bitter taste. d. Dilute it and offer through a straw and a few crackers. ANS: D Patients should avoid taking iron with milk or caffeine because both inhibit drug absorption. The liquid form of the drug is offered with food in a diluted form through a straw to prevent staining the teeth. DIF: Cognitive Level: Application REF: p. 541 OBJ: 4 TOP: Administration of Feosol KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 6. A nurse is completing an initial assessment on a new patient being seen in the hospital clinic. The presentation of this female patient includes vague symptoms of tiredness and large areas of ecchymosis. Which question is most important for the nurse to ask? a. “Are you allergic to anything?” b. “Do your gums easily bleed?” c. “How many hours do you sleep?” d. “How frequent are your periods?” ANS: B Bleeding gums are indicative of general bleeding tendencies. Sleep and frequency of menstrual periods are not significant, but the heaviness of the period is significant. History can reveal information pertinent to assisting the physician in making a diagnosis. DIF: Cognitive Level: Application REF: p. 531 OBJ: 2 TOP: Assessment of Patients with Hematologic Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. A nurse is assessing a patient 20 minutes after a bone marrow biopsy. Which statement by the patient is cause for the most concern? a. “There is fresh blood on my dressing.” b. “I am thirsty.” c. “My hip feels bruised where they stuck the needle.” d. “I had a sharp pain in my leg when they pulled the needle out.” ANS: A Fresh blood on the pressure dressing 20 minutes after the aspiration needs to be addressed. Usually, redressing with a pressure dressing and an ice pack is sufficient. Feelings of bruising and pain on extraction are to be expected. Thirst is of no clinical significance. DIF: Cognitive Level: Application REF: p. 535 OBJ: 3 TOP: Diagnostic Tests KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. At 1000 a nurse receives 2 units of blood for a patient to be transfused. What is the most appropriate nursing action? a. Set up 1 unit for the infusion to start by 1030 and send the other unit back until the first one has infused. b. Set up both units to infuse at the same time and to start at 1100. c. Set up one unit for infusion and place the other in the refrigerator for the later infusion. d. Send both units back and ask for a reissue of 1 unit only. ANS: A Blood must be started within 30 minutes of its receipt after it has been checked by two licensed staff members. In many settings, licensed practical nurses do not start the blood but can set up the infusion. The best option is to send the second unit back immediately, with an explanation that it will be called for later. One unit of blood usually takes about 2 to 4 hours to infuse. DIF: Cognitive Level: Application REF: p. 538 OBJ: 4 TOP: Transfusion Protocol KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Coordinated Care 9. A nurse is giving iron dextran intramuscularly (IM). Why should the nurse implement the Z-track method? a. Makes the injection less painful b. Prevents staining of the skin c. Prevents postinjection pain d. Allows another injection to be given at the same location ANS: B The Z-track method only ensures that no iron will be staining the skin after injection. The amount of pain is the same and, after all IM injections, the needle is cleaned on withdrawal. Injections are never given at recent injection sites. DIF: Cognitive Level: Comprehension REF: p. 541 OBJ: 4 TOP: Z-Track Method KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 10. What is the major difference between fresh-frozen plasma (FFP) and cryoprecipitate (CPP)? a. FFP contains more albumin. b. FFP has a longer infusion time. c. FFP contains no platelets. d. FFP has a very high probability of causing an allergic reaction. ANS: C FFP contains no platelets. DIF: Cognitive Level: Knowledge REF: p. 537 OBJ: 3 TOP: FFP versus CPP KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies MULTIPLE RESPONSE 1. What medical history information is significant to potential bleeding problems? (Select all that apply.) a. Drinks two glasses of wine a day b. Eats red meat three times a week c. Takes nonsteroidal anti-inflammatory drugs (NSAIDs) for the relief of arthritic pain four times a day d. Has hepatitis B e. Had a cardiac valve replaced 6 months earlier ANS: C, D, E NSAIDs and liver disorders enhance the probability of bleeding. The valve replacement of a few months earlier suggests that the patient is using anticoagulant drugs. DIF: Cognitive Level: Comprehension REF: p. 531 OBJ: 2 TOP: Factors Predisposing to Bleeding Tendency KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. A nurse plans the interventions to prepare a patient for a bone marrow aspiration. (Place the options in the correct sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Assist the patient to lie on his or her abdomen and drape the hip and lower limbs. b. Confirm the presence of laboratory personnel to stain the specimen. c. Apply a pressure dressing and help the patient lie on his or her back. d. Ensure that a signed permission form is obtained. e. Explain that the procedure will take about 30 minutes. ANS: EDABC The appropriate sequence is the following: (1) explain the procedure; (2) when the patient indicates an understanding, obtain a signed permission form; (3) assist the patient to lie on his or her abdomen and drape the hip and lower extremities; (4) confirm the presence of laboratory personnel to stain the specimen; and (5) apply a pressure dressing and help the patient lie on his or her back. DIF: Cognitive Level: Application REF: p. 535 OBJ: 3 TOP: Bone Marrow Aspiration Preparation KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control Chapter 30: Hematologic Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What should be a major focus in a teaching plan for a teenager with sickle cell anemia? a. Limit tobacco use to no more than two cigarettes a day. b. Eat foods high in iron and vitamin B. c. Maintain environmental temperature at 65 F to 68 F. d. Maintain adequate hydration. ANS: D The maintenance of adequate fluid intake (4 to 6 L/day) prevents hemoconcentration. The use of alcohol and tobacco is contraindicated for the patient with sickle cell anemia as the cause vasoconstriction. Warm environments are more therapeutic as warm environments do not cause vasoconstriction. DIF: Cognitive Level: Application REF: p. 548 OBJ: 2 TOP: Sickle Cell Anemia KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse is caring for a patient who is having radiation treatment for cancer. How many days after the start of radiation should the nurse know that the threat of thrombocytopenia exists? a. 2 b. 5 c. 9 d. 12 ANS: D Thrombocytopenia becomes a nursing concern 10 to 14 days after therapy has begun. This concern is true for radiation and chemotherapy. DIF: Cognitive Level: Knowledge REF: p. 549 OBJ: 1 TOP: Thrombocytopenia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. What happens to the sickle-shaped red blood cells during a sickle cell crisis? a. Rupture b. Production of hemoglobin S c. Interference with blood production d. Obstruction of major arteries ANS: D Circulatory obstruction causes severe pain in patients with sickle cell anemia, which is the major symptom in sickle cell crisis. The hemoglobin S does not, in itself, cause the crises until the cells obstruct a vessel. DIF: Cognitive Level: Comprehension REF: p. 546 OBJ: 1 TOP: Sickle Cell Anemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. What information should a nurse be sure to include when preparing discharge plans for a patient recently diagnosed with pernicious anemia? a. Adding daily high-fat, low-fiber supplements b. Adding a rigorous daily workout c. Avoiding prolonged exposure to direct sunlight d. Providing sufficient rest periods throughout the day ANS: D Fatigue and weakness are seen in all anemias. DIF: Cognitive Level: Application REF: p. 545 OBJ: 2 TOP: Pernicious Anemia KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. What is the rationale for administering injections of vitamin B12 to patients with pernicious anemia? a. The patient’s body does not normally manufacture enough vitamin B12. b. The patient may lack the intrinsic factor necessary for vitamin B12 absorption. c. Vitamin B12 is found in very small quantities in the patient’s body. d. Vitamin B12 is a mineral necessary to aid in the formation of strong bones. ANS: B The patient with pernicious anemia lacks the intrinsic factor, found in the stomach, which is essential for vitamin B12 absorption. DIF: Cognitive Level: Comprehension REF: p. 545 OBJ: 1 TOP: Pernicious Anemia KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 6. Which foods should a nurse include in a nutrition teaching plan for a patient with iron deficiency anemia? a. Beans and dried fruit b. Apples and white rice c. Yogurt and cooked carrots d. Yellow squash and tortillas ANS: A Iron-rich foods include beans, dried fruit, liver, red meat, fish, and whole-grain breads. DIF: Cognitive Level: Comprehension REF: p. 545 OBJ: 2 TOP: Iron-Deficiency Anemia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. A child with sickle cell anemia is prescribed the drug hydroxyurea. What effect from the drug should the patient expect to have? a. Increase energy b. Decrease cardiomegaly c. Clean out obstructed vessels d. Produce a hemoglobin that resists sickling ANS: D Hydroxyurea produces a hemoglobin that resists sickling. DIF: Cognitive Level: Comprehension REF: p. 546 OBJ: 1 TOP: Hydroxyurea KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 8. A newborn infant has developed significant jaundice and has a positive Coombs test result resulting from high levels of bilirubin. What should a nurse be aware that these symptoms may indicate? a. Aplastic anemia b. Hemophilia c. Hemolytic anemia d. Sickle cell anemia ANS: C Newborns can develop hemolytic anemias resulting from blood incompatibility to their mother. These are typical signs of hemolytic anemia in the newborn. DIF: Cognitive Level: Comprehension REF: p. 545 OBJ: 1 TOP: Hemolytic Anemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. A 3-year-old African-American child is diagnosed with sickle cell anemia. The parents know that sickle cell anemia is hereditary but do not understand why their child has the disease because neither of them has it. What is the most accurate information to provide? a. At least one of the parents has to have the disease. b. Only one parent has to have the disease or the trait. c. Someone in previous generations had the disease. d. Both parents were carriers of the sickle cell trait. ANS: D Sickle cell anemia is a genetic disease carried by the recessive genes of both parents, who will not exhibit any symptoms of the disease. DIF: Cognitive Level: Comprehension REF: pp. 545-546 OBJ: 1 TOP: Anemia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. A 35-year-old man is examined in an urgent care clinic. His presenting symptoms suggest polycythemia vera. Which extreme laboratory value would confirm this possible diagnosis? a. High hemoglobin level b. Low white cell count c. Low platelet count d. High iron level ANS: A The symptoms of polycythemia vera are extremely high hemoglobin and hematocrit values because of the excessive production of red blood cells. Patients with polycythemia vera have 1 pint of blood taken from them until the blood values become more normal. The blood is collected as it would be for a blood donation, but it cannot be used for transfusion purposes. DIF: Cognitive Level: Comprehension REF: p. 544 OBJ: 1 TOP: Polycythemia Vera KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. A 52-year-old man has a diagnosis of aplastic anemia. What information in the patient history is pertinent to this diagnosis? a. Long family history of cancer b. Regular blood donor c. 25-year employee in a chemical plant d. Gain of 5 lb in the last 2 years ANS: C Exposure to toxic chemicals can cause aplastic anemia. DIF: Cognitive Level: Analysis REF: p. 544 OBJ: 1 TOP: Aplastic Anemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. At the end of a shift, a nurse documents the effectiveness of parent teaching concerning the transmission of hemophilia. Which statement by the mother would best indicate an accurate parental perception? a. “Hemophilia is a genetic disorder, and I am a carrier, although I do not have the disease.” b. “My son developed hemophilia because I had measles while I was pregnant.” c. “Because my husband isn’t affected by the disease, our daughter will not be a carrier.” d. “I know it is not necessary to have my two daughters tested for the disease.” ANS: A Women carry the trait and pass it on to their sons. DIF: Cognitive Level: Comprehension REF: p. 549 OBJ: 1 TOP: Hemophilia KEY: Nursing Process Step: Evaluation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 13. What should a nurse be careful to observe for when assessing a patient with thrombocytopenia? a. Distended neck veins and skin discoloration b. Discoloration of the nails and sclera c. Petechiae on the skin and bleeding gums d. Enlarged thyroid gland and excitability ANS: C Symptoms of thrombocytopenia include petechiae, purpura, bleeding gums, and epistaxis. DIF: Cognitive Level: Analysis REF: p. 549 OBJ: 1 TOP: Thrombocytopenia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A nurse caring for a patient with crushing injuries from an automobile accident notes that the patient is bleeding profusely from the nose, mouth, and rectum, as well as from the injuries. What should the nurse suspect as the cause of this patient’s bleeding? a. Hemophilia b. Disseminated intravascular coagulation (DIC) c. Leukemia d. Thrombocytopenia ANS: B DIC occurs in massive crushing injuries, burns, and allergic responses. The body’s clotting ability is exhausted because of its attempt to repair so many areas with coagulation. When the platelet supply is gone, the clotting ability is lost, and massive hemorrhaging occurs. DIF: Cognitive Level: Analysis REF: p. 549 OBJ: 1 | 2 TOP: DIC KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. The nurse is caring for a patient with hemophilia who is experiencing a bleeding episode. Which intervention(s) should the nurse anticipate implementing? (Select all that apply.) a. Providing intravenous morphine for pain relief b. Administering rectal suppositories c. Activities ad lib d. Administering aspirin e. Prepare for transfusion ANS: A, E Medical treatment for patients experiencing a bleeding episode is symptomatic. The physician usually prescribes transfusions of FFP or cryoprecipitate, or both. The pain can be very severe. The patient needs adequate pain relief during these episodes, even if they last several days. Intravenous morphine is commonly prescribed for pain relief. Rectal suppositories would be avoided due to high risk for mucous membrane bleeding if inserted. Bed rest would be anticipated during a bleeding episode. Aspirin would enhance bleeding due to anticoagulant effects. DIF: Cognitive Level: Application REF: p. 550 OBJ: 1 | 2 TOP: Hemophilia KEY: Nursing Process Step: Interventions MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. is a condition in which too many RBCs are produced. ANS: Polycythemia vera Polycythemia vera is a condition in which too many red blood cells are produced. DIF: Cognitive Level: Knowledge REF: p. 544 OBJ: 1 TOP: Red Blood Cell Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 31: Immunologic System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What is responsible for initiating the inflammatory response in addition to immunoglobulin E (IgE)? a. Eosinophils b. Lymphocytes c. Basophils d. Neutrophils ANS: C Basophils initiate a massive inflammatory response with histamine that quickly brings other white blood cells (WBCs) to the site of an infection. DIF: Cognitive Level: Knowledge REF: p. 554 OBJ: 1 TOP: Components of the Immune System KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Where are histamine-releasing mast cells located? a. Circulating in the blood b. Circulating in the lymph c. Attached to organ tissue d. Embedded in the bone marrow ANS: C Mast cells are located in organ tissue when they release their histamine. The organ to which they are attached is the host of the inflammatory response. If the organ is the lung, the response may be asthma; if the organ is the colon, the response may be diarrhea. DIF: Cognitive Level: Knowledge REF: p. 554 OBJ: 1 TOP: Mast Cells KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. What is true concerning passive-acquired immunity? a. Antibodies are acquired from outside the host and instilled in the host. b. Antibodies are manufactured in response to a disease in the host. c. Antibodies are innately acquired because of being born a human being. d. Antibodies are cell mediated inside the host. ANS: A Gamma globulin injections provide passive-acquired immunity. The antibodies that are injected have been produced by another host, collected, fused in the mixture, and injected into a separate host. This gives the host a passive-acquired immunity that lasts for only 2 to 3 months. DIF: Cognitive Level: Knowledge REF: p. 557 OBJ: 1 TOP: Functions of the Immune System KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A patient taking dexamethasone (Decadron) reports insomnia. What is the best information to provide this patient regarding administration of this medication? a. Take with milk. b. Take at breakfast. c. Dissolve in fruit juice. d. Take at bedtime. ANS: B Patients taking steroids should take them early in the day to avoid sleep disturbances. DIF: Cognitive Level: Knowledge REF: p. 566 OBJ: 5 TOP: Insomnia with Steroids KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 5. A nurse is preparing a patient for a liver and spleen scan. Which intervention is most important to implement before the procedure? a. Prepare the biopsy site with a clean field. b. Check for any allergies to contrast media. c. Explain the procedure to the patient’s family. d. Have the patient eat a complete regular diet. ANS: B Allergies should always be checked before any diagnostic test. DIF: Cognitive Level: Application REF: p. 561 OBJ: 3 TOP: Preparation for Diagnostic Tests KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 6. After a bone marrow transplant, a patient is placed on a protocol of chemotherapy and radiation and has the potential for injury. Which nursing assessment should cause the nurse concern? a. Increased urine output b. Decreasing bilirubin levels c. Increasing blood pressure d. Increasing abdominal girth ANS: D High doses of chemotherapy and radiation can damage the liver, which would lead to increasing abdominal girth with ascites and increasing bilirubin levels. DIF: Cognitive Level: Application REF: p. 567 OBJ: 4 TOP: Bone Marrow Transplantation Risk KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A patient diagnosed with leukemia has had a bone marrow transplant and has completed chemotherapy. What is the greatest risk for this patient while healthy bone marrow is growing back? a. Infection and bleeding b. Hypertension and headache c. Oliguria and urinary retention d. Dyspnea and wheezing ANS: A Patients are at greater risk for infection and bleeding while their healthy bone marrow is growing back. DIF: Cognitive Level: Comprehension REF: p. 567 OBJ: 4 TOP: Bone Marrow Complications KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 8. What is the primary function in the immune process of the spleen? a. Filter microorganisms from the blood. b. Store lymphocytes used to fight infections. c. Produce additional RBCs (red blood cells). d. Stimulate WBC production. ANS: A The spleen filters microorganisms from the blood. DIF: Cognitive Level: Knowledge REF: p. 555 OBJ: 1 TOP: Functions of the Spleen KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. Which laboratory result for a patient with acute leukemia should alert the nurse to the fact that the drug protocols are not effective? a. Decreased prothrombin time b. Platelet count lower than 50,000/mm3 c. Negative Western blot result d. Neutrophils 50% to 62% ANS: B A low platelet count predisposes a patient to bleeding. A count less than 50,000/mm3 is a cause for concern. DIF: Cognitive Level: Comprehension REF: p. 562 OBJ: 3 TOP: Platelet Count KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. What type of bone marrow transplant uses the patient’s own bone marrow? a. Allergenic b. Allogeneic c. Peripheral blood stem cell d. Autologous ANS: D An autologous bone marrow transplant uses the patient’s own bone marrow. DIF: Cognitive Level: Knowledge REF: p. 566 OBJ: 3 TOP: Bone Marrow Transplantation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 11. Which human immunity is an example of innate immunity? a. Hoof-and-mouth disease b. Measles c. Rabies d. Mange ANS: A Humans, by nature of their innate properties at birth, have an innate immunity to hoof-and-mouth disease. Cows also have an innate immunity to measles. DIF: Cognitive Level: Comprehension REF: p. 555 OBJ: 1 TOP: Innate Immunity KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. Which nursing action should be implemented when performing skin testing? a. Select an 18-gauge needle. b. Inject 1 mL intradermally. c. Check the site in 2 to 3 days for swelling. d. Wrap the site with a pressure dressing. ANS: C A cell-mediated response will show swelling in 2 to 3 days, indicating antibodies working at the site of the exposure to an antigen. DIF: Cognitive Level: Application REF: p. 561 OBJ: 3 TOP: Skin Testing Procedure KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. What are the four distinct stages of the inflammatory process? (Select all that apply.) a. Dolor b. Rubor c. Tumor d. Calor e. Rumor ANS: A, B, C, D The four processes are rubor (red), tumor (swelling), calor (heat), and dolor (pain). DIF: Cognitive Level: Knowledge REF: p. 556 OBJ: 1 TOP: Stages of Inflammatory Process KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. A nurse explains that early in life, lymphocytes migrate from the marrow of the bones to the , in which they mature into T cells. ANS: thymus The lymphocytes migrate and mature to T cells in the thymus. DIF: Cognitive Level: Comprehension REF: p. 555 OBJ: 1 TOP: Thymus KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Cells in the bone marrow that are capable of developing into RBCs, WBCs, or platelets are the cells. ANS: stem Adult stem (progenitor) cells can evolve into WBCs, RBCs, or platelets. Stem cells from an embryo can mature into any specialized cell. Adult stem cells are limited to cells of their origin. DIF: Cognitive Level: Comprehension REF: p. 553 OBJ: 1 TOP: Adult Stem Cells KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 32: Immunologic Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Which population, according to statistics from the Centers for Disease Control and Prevention (CDC), has the greatest incidence of human immunodeficiency viral (HIV) infection in the United States? a. Asian Americans b. African Americans c. Latinos d. Whites ANS: B Of those with HIV infection in the United States, African Americans make up 49%, whites 27%, and Latinos 12%. Asian Americans were not reported. DIF: Cognitive Level: Knowledge REF: p. 577 OBJ: 2 TOP: Human Immunodeficiency Virus (HIV) Incidence in the United States KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What does enzyme reverse transcriptase transcribe? a. DNA to mimic CD4 cells b. T4-helper cells to RNA c. HIV RNA to HIV DNA d. T4 cells to HIV virions ANS: C Reverse transcriptase reverses the normal process and allows the RNA to be transcribed to the DNA rather than the DNA to be transcribed to the RNA. DIF: Cognitive Level: Knowledge REF: p. 578 OBJ: 1 TOP: Pathophysiology KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. What is the most common form of transmission of the HIV virus? a. Injection drug use b. Heterosexual contact c. Exposure to contaminated blood products d. Male to male ANS: D Male-to-male transmission is still the most common mode. DIF: Cognitive Level: Knowledge REF: p. 578 OBJ: 2 TOP: Transmission of HIV KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A nurse is assessing a patient with AIDS for risk factors. What is recognized as the most risky behavior in the patient history? a. Oral sex without contact with the glans penis b. Oral sex with a condom c. Use of sex toys d. Anal sex with a condom ANS: D Anal sex, even with a condom, is a higher risk behavior than the other three options. DIF: Cognitive Level: Comprehension REF: p. 578 OBJ: 2 TOP: Risk Factors KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. When is a patient with HIV considered to have progressed to AIDS? a. Two or more opportunistic infections are diagnosed. b. Kaposi sarcoma appears. c. CD4 cell level drops to 200. d. Patient tested positive for enzyme-linked immunosorbent assay (ELISA). ANS: C A person with an HIV infection is not diagnosed with AIDS until the CD4 count falls to 200. Other AIDS markers exist as well. DIF: Cognitive Level: Knowledge REF: p. 578 OBJ: 3 TOP: AIDS KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A very anxious young man comes to the clinic believing that he may have HIV infection because of his persistent influenza-like symptoms and his risky sexual behavior. What should the nurse anticipate that a positive blood analysis would show? a. High levels of CD8 cells b. High levels of HIV-infected cells c. Low levels of T cells d. Low levels of antibodies ANS: B In the initial phase of HIV infection, high levels of HIV-infected cells, high levels of T cells, and high levels of antibodies are present as the body attempts to rid the body of the virus through the immune response. DIF: Cognitive Level: Comprehension REF: p. 578 OBJ: 1 TOP: Diagnosis of AIDS KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. How long does the initial stage of an HIV infection usually last? a. 2 to 4 weeks b. 4 to 8 weeks c. 8 to 12 weeks d. 12 to 16 weeks ANS: B The initial phase of an HIV infection lasts from 4 to 8 weeks. DIF: Cognitive Level: Knowledge REF: p. 578 OBJ: 1 TOP: Initial Phase of HIV Infection KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. A young man at the HIV clinic tells the nurse how relieved he is that he does not have HIV because he now has no symptoms at all when just a few weeks ago he felt awful. What is the most appropriate nursing response? a. “Flulike symptoms frequently are misdiagnosed as HIV.” b. “In the latent stage, the physical symptoms are reduced, but the HIV is still present in the lymph nodes.” c. “A high antibody count can overwhelm HIV infection in the early stage.” d. “Antiretroviral drugs are very effective in the first stage in reducing symptoms.” ANS: B In the latent stage, the symptoms are reduced as the virus enters the lymph nodes. DIF: Cognitive Level: Application REF: p. 578 OBJ: 1 TOP: Stages of HIV Infection KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. A nurse is educating patients about the progression of HIV infections. Which statement by the patient in the latent stage indicates that teaching has been effective? a. “I had better get my affairs in order. I don’t have a lot of time left.” b. “Whew! I thought when I got AIDS that I was a ‘goner.’” c. “Now I won’t have to take all those expensive drugs that I have been using.” d. “I can still enjoy life and live pretty much as I want for the next several years.” ANS: D The latent stage may last as long as 12 years without developing into AIDS. Medications will be continued. DIF: Cognitive Level: Application REF: p. 585 OBJ: 1 TOP: Latent Stage of HIV Infection KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. A nurse is caring for a patient with HIV infection taking Retrovir, a nucleoside antiviral that is a reverse transcriptase inhibitor. For what should the nurse be especially observant? a. Decreased urine output b. Hypertensive episodes c. Jaundice d. Edema of the face ANS: C Retrovir has the potential of causing a fatal hepatotoxic reaction. Jaundice is a possible sign of hepatic impairment. DIF: Cognitive Level: Comprehension REF: p. 578 OBJ: 1 TOP: Drug Side Effects KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 11. What indicates that a patient has entered the third stage of HIV infection? a. T-helper CD4 cell count of 500 b. Rise in antibody count c. Drop in viral load d. Increase in T4 helper cells ANS: A In the third stage of HIV infection, T-helper CD4 cells drop to approximately 500. Antibodies are always high throughout the infection but are ineffective. The viral count is high. DIF: Cognitive Level: Comprehension REF: p. 580 OBJ: 1 TOP: Third Stage of HIV Infection KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. A nurse is preparing a teaching plan for a patient with HIV who has been diagnosed with microsporidiosis. Which implementation should be included? a. Drink 3 quarts of fluid a day to combat dehydration. b. Include milk products with every meal. c. Consume liberal amounts of fat for increased energy. d. Limit protein intake to reduce serum ammonia levels. ANS: A The patients need plenty of fluids to combat the diarrhea and proteins for calories. They should avoid milk products and fat. DIF: Cognitive Level: Application REF: p. 587 OBJ: 1 TOP: Microsporidiosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Basic Care and Comfort 13. What should a patient be encouraged to do before the initiation of any anti-HIV drug protocol? a. Give up sexual activity for several months. b. Follow the strict dietary guidelines. c. Comply with the drug protocol. d. Involve the partner in a support program. ANS: C Patients with HIV are assessed for their willingness to comply with the drug protocol because nonadherence causes the HIV organisms to become resistant to the drug. DIF: Cognitive Level: Application REF: p. 587 OBJ: 1 TOP: Compliance KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 14. A patient with HIV complains to the home health nurse that he has been having watery diarrhea for the past 10 days. The nurse suspects toxoplasmosis. What is the most significant question for the nurse to ask? a. “Have you stopped taking your antiviral medication?” b. “Have you been drinking alcohol?” c. “Have you been eating aged cheese or organ meats?” d. “Do you have a cat?” ANS: D Cat litter boxes and undercooked meats are the major sources of toxoplasmosis, which causes a persistent watery diarrhea. DIF: Cognitive Level: Comprehension REF: p. 581 OBJ: 1 TOP: Toxoplasmosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 15. A patient with HIV is diagnosed with progressive multifocal leukoencephalopathy (PML). What should a nurse encourage the patient to do? a. Take daily exercise for 30 minutes. b. Avoid excessive fats in the diet. c. Remove all potted plants from inside the home. d. Prepare advanced directives. ANS: D The completion of advanced directives is essential as this disease is rapidly progressing, and death usually occurs 4 to 6 weeks after diagnosis. DIF: Cognitive Level: Application REF: p. 580 OBJ: 1 TOP: PML KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 16. Which should take priority in the care of an outpatient with AIDS? a. Therapeutic regimen management b. Physical mobility c. Skin integrity d. Social isolation ANS: A Failure to take anti-HIV drugs as scheduled can encourage resistant strains of HIV. DIF: Cognitive Level: Analysis REF: p. 587 OBJ: 1 TOP: Nursing Diagnosis: AIDS KEY: Nursing Process Step: Nursing Diagnosis MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 17. A nurse removes a potted plant from the room of a patient with HIV. What is the nurse trying to prevent? a. Aspergillosis b. Candidiasis c. Coccidioidomycosis d. Cytomegalovirus (CMV) ANS: A Aspergillosis can be contracted from the potting soil in and around the plant in the pot. DIF: Cognitive Level: Comprehension REF: p. 581 OBJ: 1 TOP: Aspergillosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 18. What childhood exposure causes painful shingles experienced by the patient with HIV? a. Measles b. Mumps c. Impetigo d. Chickenpox ANS: D Chickenpox can be reactivated as shingles. DIF: Cognitive Level: Knowledge REF: p. 582 OBJ: 1 TOP: Shingles KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 19. Which nursing action should be implemented to increase the comfort of a patient with oral hair leukoplakia? a. Allow aspirin to melt in the mouth and then wash out with warm water. b. Encourage mouth rinses with warm salt water several times a day. c. Limit intake of ice cream and other cold foods. d. Offer fluids through a straw. ANS: D Using a straw keeps fluids from flooding the entire oral cavity. Warm or acidic items are to be discouraged because they add to the discomfort. Ice cream and popsicles can numb the area. DIF: Cognitive Level: Application REF: p. 582 OBJ: 1 TOP: Oral Hair Leukoplakia KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. What should a patient with HIV avoid to prevent bacillary angiomatosis (BA)? a. Cats b. Large crowds of people c. Consuming unwashed fruits d. Exposure to mosquito bites ANS: A Cats and their fleas are thought to transmit BA. DIF: Cognitive Level: Comprehension REF: p. 583 OBJ: 1 TOP: Prevention KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 21. What sign should a nurse report when caring for the patient with AIDS who has cutaneous Kaposi sarcoma? a. Nausea b. Fatigue c. Abdominal pain d. Weight loss ANS: C Abdominal pain may be an indication of organ involvement from Kaposi sarcoma. DIF: Cognitive Level: Comprehension REF: p. 583 OBJ: 1 TOP: Kaposi Sarcoma KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 22. Which statement by a patient diagnosed with AIDS should lead a nurse to suspect an infection by CMV? a. “I need to get glasses; I can’t see as well as I did a few months ago.” b. “I need to drink more water. This diarrhea has really dehydrated me.” c. “I need to get smaller clothes. I have lost 10 lb in the past 6 weeks.” d. “I need to take some pep pills. I don’t have any energy.” ANS: A Visual changes indicate the presence of CMV retinitis, which will eventually lead to blindness. Diarrhea is indicative of a fungal infection, and decreases in weight and energy are expected manifestations of AIDS. DIF: Cognitive Level: Comprehension REF: p. 582 OBJ: 1 TOP: Assessing CMV KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 23. A nurse is caring for a patient with HIV infection who has been prescribed highly active antiretroviral therapy (HAART). What should the nurse warn the patient that inconsistent administration of the drug can result in? a. HIV strain becoming resistant to the drug b. Decrease in antibodies in the circulating volume c. Addition of another antiretroviral agent to the protocol d. Rapid increase in the symptoms of AIDS ANS: A Inconsistent administration of HAART drugs can cause the HIV strain to become resistant to the drug. DIF: Cognitive Level: Knowledge REF: p. 591 OBJ: 4 TOP: HAART KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 24. Which symptom should a nurse recognize as being pertinent to a possible diagnosis of systemic lupus erythematosus (SLE)? a. Butterfly rash of the face b. Protruding abdomen c. Thinning hair d. Bloody diarrhea ANS: A The classic butterfly rash of the face is one of the most recognizable signs. Because the symptoms come and go, SLE is extremely hard to diagnose quickly. DIF: Cognitive Level: Comprehension REF: p. 575 OBJ: 5 TOP: Systemic Lupus Erythematosus KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 25. What should a nurse include when developing a plan of care for a patient with human immunodeficiency virus (HIV)? a. Careful aseptic technique to prevent infection b. Instruction to limit fluids to prevent congestive heart failure c. Oral alcohol rinses to control mouth infections d. Selections of high-fat foods in the daily diet ANS: A A major complication of HIV is opportunistic infections. DIF: Cognitive Level: Application REF: p. 578 OBJ: 1 TOP: Prevention of Infection in Patients with Human Immunodeficiency Virus (HIV) KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 26. An 11-year-old girl is diagnosed with idiopathic thrombocytopenic purpura (ITP). Which parental statement helps the nurse evaluate that teaching is successful? a. “Our daughter can still be involved in gymnastics.” b. “When our daughter’s hemoglobin falls below 3.5, she’ll need blood.” c. “Our daughter will need genetic counseling before she marries.” d. “Our daughter should avoid drugs containing sulfonamides.” ANS: D Drugs known to induce ITP include sulfonamides. DIF: Cognitive Level: Application REF: p. 574 OBJ: 5 TOP: Idiopathic Thrombocytopenic Purpura Care Plan KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 27. What is most appropriate for a nurse to include when preparing discharge plans for a patient with SLE? a. Need to consume 2 L of fluid daily b. Close monitoring of daily blood glucose level c. Use of daily sunscreens with a sun protection factor (SPF) higher than 15 d. Careful concern for certain food allergies ANS: C Patients with SLE are photosensitive to sunlight. DIF: Cognitive Level: Application REF: p. 576 OBJ: 5 TOP: Systemic Lupus Erythematosus KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 28. A nurse is caring for a patient with thrombotic thrombocytopenic purpura who is having plasmapheresis every day. Which assessment alerts the nurse of a complication? a. Hypotension b. Seizure activity c. Diarrhea d. Intense headache ANS: A During the period of treatment by plasmapheresis, the patient can become hemodynamically unstable and have a reduced cardiac output with the attendant hypotension. This is a serious complication and can lead to renal failure. DIF: Cognitive Level: Application REF: p. 575 OBJ: 6 TOP: Thrombotic Thrombocytopenic Purpura KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 29. A nurse assesses a neutrophil count of 900/mm3 in a patient with acute leukemia. What should the nurse anticipate initiating? a. A high-protein diet b. Increased doses of steroids c. Compromised host precautions d. Injections of blood-building medication ANS: C Patients with neutrophil counts of approximately 1000 cells/mm3 are placed on compromised host precautions. DIF: Cognitive Level: Application REF: p. 573 OBJ: 6 TOP: Compromised Host Precautions KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 30. A nurse is caring for a patient in the last stages of leukemia and is aware that the patient is at risk from the bacteria of his own body. Which is an example of internal bacteria? a. Beta-hemolytic streptococci b. Streptococcus pneumoniae c. Streptococcus viridans d. Pseudomonas aeruginosa ANS: D Internal bacteria such as P. aeruginosa and Escherichia coli are capable of attacking the compromised immune system from inside the body. DIF: Cognitive Level: Comprehension REF: p. 573 OBJ: 5 TOP: Risk for Infection in Leukemia KEY: Nursing Process Step: Nursing Diagnosis MSC: NCLEX: Physiological Integrity: Physiological Adaptation 31. The nursing staff of an oncology unit cautions visitors to be free of infections before visiting patients. What can chemotherapy and decreased bone marrow production cause in these patients? a. Hemorrhage b. Neutropenia c. Edema d. Hypovolemia ANS: B Neutropenia occurs when the total number of neutrophils is abnormally low, placing the patient at increased risk for infection. DIF: Cognitive Level: Comprehension REF: p. 571 OBJ: 5 TOP: Neutropenia KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 32. A 24-year-old woman is admitted to the hospital for a complete medical examination. Her current complaints are indicative of SLE. Which symptom would indicate this diagnosis? a. Recent weight gain of 10 lb b. Difficulty breathing in the morning c. Frequent episodes of diarrhea d. Musculoskeletal pain in the hands ANS: D Musculoskeletal symptoms are experienced by 95% of patients with SLE at some time during the course of their disease. DIF: Cognitive Level: Comprehension REF: p. 575 OBJ: 5 TOP: Systemic Lupus Erythematosus KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. Which populations are at the highest risks of contracting HIV? (Select all that apply.) a. Health care workers who mishandle infected sharps b. Breastfed infants of HIV-infected mothers c. Persons sharing living quarters with an HIV-infected person d. Heterosexual partners of an HIV-infected person e. Newborns of an HIV-infected mother ANS: A, B, D, E Sharing living quarters without intimate contact does not expose a person to HIV infection. DIF: Cognitive Level: Comprehension REF: p. 577 OBJ: 2 TOP: Prevalence of HIV KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse is designing a teaching plan for a patient with AIDS. What should be included relative to food preparation precautions? (Select all that apply.) a. Check expiration dates on frozen foods. b. Leave produce unwashed to preserve protective spray. c. Drink a small glass of red wine before each meal to stimulate the appetite. d. Eat three large, well-balanced meals daily. e. Avoid leftovers. ANS: A, E Using food before the expiration date and avoiding leftovers reduce the risk of food contamination. Individuals with AIDS should wash all fresh produce to get rid of contaminants, eat several small meals daily, and avoid alcohol and caffeine. DIF: Cognitive Level: Application REF: p. 590 OBJ: 1 TOP: Nutritional Precautions KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. Which factors explain the increase in HIV infections in persons over the age of 50 years? (Select all that apply.) a. Older persons are usually not questioned by health professionals about sex or drug abuse. b. Older persons are more promiscuous in earlier years. c. Older persons are less likely to seek HIV screening. d. Older persons mistake HIV symptoms as part of the discomforts of increased age. e. Older persons tend to use hormonal forms of contraception. ANS: A, C, D Individuals older than 50 years of age are less likely to be questioned by health care professionals relative to sex activities or illicit drug use. Older adults are less likely to seek HIV screening and frequently accept the symptoms of HIV as part of increasing age. DIF: Cognitive Level: Comprehension REF: p. 584 OBJ: 2 TOP: Older Persons with HIV KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 4. Which opportunistic fungal diseases threaten patients with HIV? (Select all that apply.) a. Aspergillosis b. Pneumocystis jiroveci c. Herpes simplex d. Oral hairy leukoplakia e. Tuberculosis ANS: A, B Aspergillosis and P. jiroveci are caused by fungi. Herpes simplex and leukoplakia are caused by viruses. Tuberculosis is caused by bacteria. DIF: Cognitive Level: Knowledge REF: p. 579 OBJ: 1 TOP: Fungal Infections KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A nurse explains that in autoimmune diseases, the body identifies its own proteins as foreign matter and sets out to destroy itself. Which are examples of autoimmune diseases? (Select all that apply.) a. SLE b. Type 1 diabetes mellitus (DM) c. Rheumatoid arthritis (RA) d. Osteoarthritis e. Pancreatitis ANS: A, B, C The autoimmune diseases are SLE, type 1 DM, and RA. DIF: Cognitive Level: Knowledge REF: p. 574 OBJ: 5 TOP: Autoimmune Diseases KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. A nurse explains that HIV is introduced to the systemic circulation by the _ , which is found in the mucous membranes. ANS: macrophage The macrophage introduces HIV into the system. DIF: Cognitive Level: Knowledge REF: p. 578 OBJ: 1 | 2 TOP: Macrophage KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse explains to a pregnant patient with AIDS that her baby will be treated with antiretroviral drugs for _ weeks after birth. (Use numeric characters only.) ANS: 6 The usual antiretroviral protocol for an infant born to a mother with AIDS is for 6 weeks. DIF: Cognitive Level: Knowledge REF: p. 584 OBJ: 4 TOP: Treatment of Newborns of AIDS Patients KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 33: Cardiovascular System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse performs an apical-radial pulse evaluation, with the result of 100/88. What is the pulse deficit? a. 12 b. 24 c. 76 d. 88 ANS: A To detect an apical-radial pulse deficit, the rates should be counted simultaneously and compared for differences. If a difference exists between the apical rate and the radial rate, then a pulse deficit is present. For example, in atrial fibrillation, a pulse deficit exists. DIF: Cognitive Level: Analysis REF: p. 603 OBJ: 3 TOP: Vital Sign Assessment: Pulse Deficit KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. What is increased in hypertension that in turn causes an increase in the work of the heart? a. Preload b. Stroke volume c. Contractility d. Afterload ANS: D An increase blood pressure creates an increase in afterload because the heart must work harder to push the blood out of the left ventricle into the circulating volume. DIF: Cognitive Level: Comprehension REF: p. 597 OBJ: 4 TOP: Hypertension Effect on Afterload KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. Which heart sound should the nurse record as normal? a. Ventricular gallop in a 20-year-old patient b. Atrial gallop in a 25-year-old patient c. Friction rub in a 45-year-old patient d. Medium diastolic murmur in a 50-year-old patient ANS: A Ventricular gallops are considered normal in individuals younger than 30 years of age. All other options are pathologic abnormalities. DIF: Cognitive Level: Application REF: p. 604 OBJ: 3 TOP: Heart Sound Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A patient asks what a transesophageal echocardiogram (TEE) is and what it is expected to do? What is the best explanation by the nurse? a. Measures conductivity b. Records the force of contraction c. Evaluates the efficiency of the valves d. Checks the volume of the preload ANS: C TEE evaluates the efficiency of the valves. DIF: Cognitive Level: Application REF: p. 607 OBJ: 4 TOP: TEE KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A nurse records the finding of a normal sinus rhythm (NSR) when the P, Q, R, S, and T are all present in the electrocardiographic complex. What additional information should the nurse document? a. Rate of 82 seconds b. PR interval of 0.36 second c. QRS complex of 0.16 second d. Inverted T ANS: A NSR requires the presence of P, Q, R, S, and T waves, in that order, and all pointing in the same direction, with a rate of 60 to 100 seconds. Normal intervals are a PR interval of 0.12 to 0.20 seconds and a QRS complex less than 0.10 second. DIF: Cognitive Level: Application REF: p. 609 OBJ: 1 TOP: Normal Sinus Rhythm KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A nurse should anticipate that a patient taking Vasotec, an angiotensin-converting enzyme (ACE) inhibitor, should have which positive outcome to this drug? a. Increased fluid retention b. Decreased blood pressure c. Decreased urine output d. Increased appetite ANS: B ACE inhibitors suppress the excretion of angiotensin, which lowers the blood pressure, reduces fluid retention, and leads to increased urine output. DIF: Cognitive Level: Application REF: p. 629 OBJ: 5 TOP: ACE Inhibitors KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 7. A 29-year-old patient is to receive cardioversion for a dysrhythmia. What should the nurse instruct the patient to expect? a. Administration of a short-acting sedative b. Digoxin dose to be taken as scheduled c. Procedure to be completely safe d. Pacemaker spikes to be carefully monitored ANS: A A cardioversion has risks, such as ventricular fibrillation. Emergency equipment should be available. The digoxin dose is held before a cardioversion, and the patient is given a short-acting sedative such as Versed or Valium, which will require recovery. The electrocardiogram R wave is synchronized via the computer, and no pacemaker is involved. DIF: Cognitive Level: Comprehension REF: p. 631 OBJ: 5 TOP: Cardioversion KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. A 68-year-old patient is scheduled for open heart surgery in the morning and is crying. What is the most appropriate response by the nurse? a. “Everything will go great! Dr. C. is the best!” b. “I know how you feel, so do not cry.” c. “Tell me what concerns you the most.” d. “I will call the physician for a sedative. You are too upset.” ANS: C Therapeutic implementations identify and acknowledge feelings. Do not assume that you know how the patient feels and do not give false assurances. DIF: Cognitive Level: Application REF: p. 635 OBJ: 5 TOP: Open Heart Surgery KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 9. A nurse explains that cardiac rehabilitation lasts from the end of acute care to the return to home and beyond. What does this service include? a. One-on-one individualized care b. Focus on the patient rather than the family c. Telemetry-monitored exercise d. Rejection from the program for noncompliance ANS: C Cardiac rehabilitation programs are supervised by a team of experts who arrange for telemetry-supervised exercise and other modalities, such as diet and medical protocol management. The focus is on the family, as well as the patient. Although some patients reject the program, they are rarely rejected by the rehabilitation center. DIF: Cognitive Level: Comprehension REF: p. 632 OBJ: 5 TOP: Cardiac Rehabilitation KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. On auscultation, a nurse detects a heart murmur. What should the nurse know that a heart murmur indicates? a. Valves that do not close correctly b. Pericardium that is inflamed c. Decrease in pacemaker cells d. Loud ventricular gallop ANS: A Heart murmurs indicate turbulent blood flow and can be caused by valves that are stiff and do not shut correctly; consequently, blood flows back into the chamber. DIF: Cognitive Level: Comprehension REF: p. 604 OBJ: 1 TOP: Heart Murmur KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. A physician has ordered continuous pulse oximetry. What should the nurse explain to the patient about this procedure? a. Involves a single prick b. Measures the amount of oxygen in the blood c. Is applied to the wrist d. Identifies damaged cells in the myocardium ANS: B Pulse oximetry measures arterial oxygen saturation noninvasively by attaching a clip to a digit, an ear, or a nose. DIF: Cognitive Level: Comprehension REF: p. 605 OBJ: 3 TOP: Pulse Oximetry KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. A stress test is scheduled for a 41-year-old patient. What action should the nurse implement to prepare the patient for the examination? a. Have the patient sign a consent form. b. Give the patient a special heart diet. c. Prepare the patient for sedation. d. Remove all metal objects. ANS: A A stress test is a noninvasive test that consists of a patient walking on a treadmill while an electrocardiogram records the activity. A consent form is required. DIF: Cognitive Level: Application REF: p. 606 OBJ: 3 TOP: Stress Test KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 13. What action should a nurse expect to implement when a patient returns from a cardiac catheterization? a. Ambulate the patient in the hall. b. Check the puncture site. c. Monitor the gag reflex. d. Remove the gel from all sites on the skin. ANS: B Cardiac catheterizations are invasive procedures during which a catheter is threaded through an artery. Postprocedure care requires bed rest and monitoring the puncture site. DIF: Cognitive Level: Application REF: p. 607 OBJ: 5 TOP: Cardiac Catheterization KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 14. A nurse assesses an inverted T wave on the ECG of a patient who had an acute MI two days earlier. How should the nurse interpret this finding? a. Normal recovery b. New MI c. Abnormal waveform d. Congestive heart failure ANS: C The abnormal waveform of the inverted T wave is an indicator that tissue death has occurred in part of the cardiac wall. The cardiac wall now has no ability to conduct or to contract and sends that message to the ECG via the inverted T. The tissue will take 6 weeks to regenerate. DIF: Cognitive Level: Analysis REF: p. 614 OBJ: 4 TOP: Significance of Inverted T Wave KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 15. Laboratory tests are performed to identify damage to the heart muscle. Which test is elevated the earliest with heart damage? a. Creatine phosphokinase-MB (CPK-MB) b. Lactate dehydrogenase (LDH) c. Lipid profile d. Troponin ANS: D Troponin is elevated within 3 to 6 hours and is often measured in the emergency department. CPK-MB is elevated in 12 to 24 hours. Three serial samples are drawn. The LDH increases with heart damage within 3 to 6 days. The lipid profile is not elevated with heart damage. DIF: Cognitive Level: Knowledge REF: p. 618 OBJ: 1 TOP: Cardiac Enzymes KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 16. A patient is scheduled for a heart catheterization. What action should the nurse implement in preparation for this examination? a. Ask the patient about allergies to seafood or iodine. b. Remove all metal objects. c. Give the patient a special heart diet. d. Test arterial blood gases (ABGs). ANS: A The dye injected during the cardiac catheterization is iodine based. An allergy to seafood is correlated with a reaction to this dye as well. DIF: Cognitive Level: Application REF: p. 617 OBJ: 5 TOP: Cardiac Catheterization KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 17. A patient has had atropine sulfate that has been administered intravenously to treat a dysrhythmia. What should the nurse assess this patient for after administration? a. Weight gain b. Tachycardia c. Muscle twitching d. Incontinence of urine ANS: B Atropine increases the heart rate. The nurse should watch for tachycardia, which increases the workload of the heart. This medication causes urinary retention. DIF: Cognitive Level: Application REF: p. 625 OBJ: 5 TOP: Drugs for Dysrhythmias KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 18. A dopamine infusion is being administered to a patient with shock. For what should the nurse be alert? a. Sharp spike in blood pressure b. Tremor of the hands c. Increasing urinary output d. Hyperirritability of the patient ANS: A Dopamine has a direct effect by elevating the blood pressure. The criterion is to titrate to the target blood pressure. Urinary output should also be monitored for a decreased amount because a heightened blood pressure may slow urine filtration and reduce urine output. DIF: Cognitive Level: Application REF: p. 625 OBJ: 5 TOP: Dopamine KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 19. A patient with atrial fibrillation is prescribed amiodarone for the dysrhythmia. Which potential adverse reaction should the nurse report? a. Ataxia b. Decreasing pulse rate c. Decreasing blood pressure d. Increase in cardiac output ANS: A The drug amiodarone is meant to quiet atrial activity and modify rapid pulse rate, high blood pressure, and decreased cardiac output caused by the dysrhythmia. The drug interferes with the thyroid and causes an ataxic gait and trembling of hands as adverse effects. DIF: Cognitive Level: Application REF: p. 623 OBJ: 5 TOP: Atrial Fibrillation with Amiodarone KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 20. A medication, simvastatin (Zocor), is administered to lower a patient’s cholesterol level. Follow-up lipid levels are reviewed by the nurse. Which level indicates the desired therapeutic range? a. High-density lipoprotein (HDL), 29 mg/dL; low-density lipoprotein (LDL), 160 mg/dL b. HDL, 38 mg/dL; LDL, 120 mg/dL c. HDL, 56 mg/dL; LDL, 106 mg/dL d. HDL, 42 mg/dL; LDL, 98 mg/dL ANS: D The reading that has both an HDL level above 40 mg/dL and an LDL level below 100 mg/dL is in the therapeutic target range. DIF: Cognitive Level: Knowledge REF: p. 624 OBJ: 5 TOP: Drug Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 21. A diuretic medication, furosemide (Lasix), is being administered for congestive heart failure. Which assessment is not an anticipated consequence of the therapy? a. Increased urinary output b. Weight loss c. Thirst d. Muscle weakness ANS: D Increased urinary output, weight loss, and thirst are all anticipated consequences of the therapy. Muscle weakness is a sign of hypokalemia. DIF: Cognitive Level: Comprehension REF: p. 630 OBJ: 5 TOP: Diuretic Therapy KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 22. A patient is receiving digoxin 0.25 mg/day. What should the nurse do prior to administering this medication? a. Count an apical pulse for 15 seconds. b. Hold the dose if the apical rate is 57 beats/min. c. Give the dose if the apical rate is 59 beats/min. d. Double the dose if the rate is 62 beats/min. ANS: B The dose should be held if the apical rate is less than 60 beats/min for 1 minute. DIF: Cognitive Level: Application REF: p. 621 OBJ: 5 TOP: Drug Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 23. A 46-year-old patient is receiving propranolol (Inderal), a nonselective beta-adrenergic blocker, for a heart condition. What patient teaching is most appropriate? a. Sit or lie down when taking the drug. b. Limit caffeine intake. c. Double the dose if symptoms occur. d. Never stop taking the drug abruptly. ANS: D Beta-blockers should never be stopped abruptly because they can cause angina or MI. Patients are gradually weaned off these medications. DIF: Cognitive Level: Comprehension REF: p. 622 OBJ: 5 TOP: Drug Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 24. Which assessment should be immediately addressed in a patient on lidocaine? a. Slowed ventricular rate b. Occasional PVCs c. Increase in temperature to 102 F d. Nausea and vomiting ANS: C A temperature that goes up drastically indicates an adverse reaction to lidocaine, malignant hyperthermia. The slowed ventricular rate, even with occasional PVCs, is an expected outcome of lidocaine infusion. Nausea and vomiting are adverse effects. DIF: Cognitive Level: Application REF: p. 623 OBJ: 5 TOP: Drug Therapy KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 25. A nurse records a “1” for the pulse quality of the pedal pulse. What interpretation is correct regarding the pulse? a. Absent b. Normal c. Thready d. Forceful ANS: C A “1” in a pulse evaluation indicates a thready pulse that is easily obliterated by pressure. DIF: Cognitive Level: Application REF: p. 603 OBJ: 1 TOP: Pulse Quality KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 26. A patient with an irregular sinoatrial (SA) node conduction has a permanent pacemaker with the code AAIOO and is now going home. The patient asks, “What happens when my real SA node fires on its own?” How should the nurse respond regarding what the pacemaker should do? a. Not fire b. Fire only the ventricles c. Change the rate of firing d. Fire both the atria and the ventricles. ANS: A The code is A (chamber-paced) atria, A (sense impulse) atria only, I (inhibit) inhibit firing from the pacemaker, O (rate modification) no rate modification, and O (multichamber) no other chambers to be stimulated by the pacemaker. If the SA fires on its own, the pacemaker does nothing until it fails to sense an impulse. DIF: Cognitive Level: Application REF: p. 632 OBJ: 5 TOP: Permanent Pacemaker Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 27. What is a normal age-related change in older adults that makes them susceptible to cardiovascular disease? a. Increase in cardiac output b. Increase in stroke volume c. Stiff peripheral vessels d. Oxygen capacity improvement ANS: C As adults age, their peripheral vessels become stiff, their oxygen capacity and stroke volume are reduced, and their aorta thickens and calcifies. DIF: Cognitive Level: Knowledge REF: p. 601 OBJ: 2 TOP: Changes in Older Adults KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 28. A nurse assesses a patient’s capillary refill time as less than 3 seconds. What does this assessment indicate? a. Hypertension b. Tissue perfusion c. Fluid volume excess d. Increased blood viscosity ANS: B Capillary refill is determined by compressing the nail bed until it blanches. With a normal capillary refill, color returns to the blanched skin within 3 seconds. DIF: Cognitive Level: Comprehension REF: p. 604 OBJ: 1 TOP: Capillary Refill KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 29. A nurse performs Homans maneuver by flexing the knee and sharply dorsiflexing the foot. What response indicates a positive Homans sign? a. Cramping of the toes b. Resisting dorsiflexion c. Pain in the calf area d. Blanching of the sole ANS: C A positive Homans sign indicates the possible presence of a DTV because of the pain produced in the calf of the leg when the foot is dorsiflexed. DIF: Cognitive Level: Comprehension REF: p. 604 OBJ: 1 TOP: Homans Sign KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 30. Which technique should the nurse implement when performing the Allen test on a patient to evaluate the adequacy of circulation in the radial artery? a. Asks the patient to relax the hand by the side b. Compresses only the ulnar artery to blanch the hand c. Releases pressure on both arteries at the same time d. Observes whether the color is returning to the hand, which indicates perfusion ANS: D The Allen test is performed to evaluate circulation in the hand, both in the radial and the ulnar arteries. The patient is asked to make a fist. The nurse compresses both the ulnar and the radial artery to blanch the hand. The patient is asked to open the hand as the nurse releases pressure on one or the other of the arteries. Color returning to the hand confirms perfusion. DIF: Cognitive Level: Application REF: p. 605 OBJ: 1 TOP: Allen Test KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 31. A nurse records that a patient has a 3+ edema to the right foot. How deep did the nurse’s thumb depress the edematous area? a. More than 1 inch b. To 1 inch c. To inch d. Less than inch ANS: B Edema is measured by the depth of the depression of the thumb: 1 = less than inch, 2 = to inch, 3 = to 1 inch, and 4 = more than 1 inch. DIF: Cognitive Level: Comprehension REF: p. 604 OBJ: 1 TOP: Assessing for Edema KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 32. A nurse is caring for a patient who has had an angiogram. What should the nurse make a point of care to assess and document on this patient? a. Fluid intake b. Peripheral pulses in the affected leg c. Inquiring about an allergy to iodine d. Decreased blood pressure ANS: B Checking and recording the presence and strength of the pulses in the affected leg ensure that the injection site has not occluded the vessel and that vascular spasm has not impaired circulation. An inquiry about an iodine allergy is made before the procedure. DIF: Cognitive Level: Application REF: p. 608 OBJ: 4 TOP: Postangiogram Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 33. A nurse is educating a patient regarding a stress test on a treadmill. Teaching includes that this test is a noninvasive procedure. What additional information is appropriate for the nurse to include? a. Is monitored continuously by blood pressure and an electrocardiogram b. Will last about 1 hour c. Is meant to stimulate claudication and dyspnea d. Will require a period of bed rest afterward ANS: A The examination requires the patient to walk at a rate of approximately 1.5 miles per hour. The exercise is continually monitored and is terminated if the patient experiences pain or dyspnea. DIF: Cognitive Level: Comprehension REF: p. 616 OBJ: 4 TOP: Treadmill Stress Test KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 34. A patient inquires how something as simple as walking could help his venous vascular disorder. What is the best response by the nurse when explaining the benefits of walking? a. Improves the strength of the vascular walls b. Boosts venous circulation through leg muscle activity c. Increases cardiac output d. Clears plaques from the veins ANS: B Walking is helpful because the muscle action of the legs that massage the valves of the veins boosts circulation. DIF: Cognitive Level: Comprehension REF: p. 632 OBJ: 5 TOP: Benefits of Walking KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 35. What is contraindicated for a patient performing Buerger-Allen exercises? a. Lying on the stomach b. Raising legs for 2 minutes until they blanch c. Lowering the legs until the color returns d. Keeping legs flat for 5 minutes and then repeat the exercise ANS: A Buerger-Allen exercises promote emptying of the blood vessels by gravity. Initially, lying on the back and elevating the legs will result in pallor, and then lowering the legs will allow color to return. DIF: Cognitive Level: Comprehension REF: p. 632 OBJ: 5 TOP: Buerger-Allen Exercises KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 36. A nurse cautions a patient with peripheral vascular disease (PVD) that continued smoking causes detrimental vasoconstriction for up to after only one cigarette. a. 10 minutes b. 20 minutes c. 30 minutes d. 1 hour ANS: D Smoking restricts circulation by vasoconstriction and lasts up to 1 hour after a cigarette; it also causes vasospasm. DIF: Cognitive Level: Knowledge REF: p. 633 OBJ: 5 TOP: Smoking Cessation KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 37. A nurse is performing an intake examination on a patient with peripheral vascular disease (PVD). Which lifestyle information identified by the patient aggravates vascular disease? a. Riding a bicycle to work b. Drinking red wine every day c. Being employed as an air traffic controller d. Eating chocolate candy every day ANS: C Employment as an air controller is a stressful occupation. Stress increases vasoconstriction and increases vascular resistance. Wine and chocolate actually have beneficial effects on circulation, as does bicycle riding. DIF: Cognitive Level: Application REF: p. 635 OBJ: 5 TOP: Stress and PVD KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 38. Vascular disease disorders often require the use of elastic stockings. Which action should the nurse implement when caring for a patient with elastic stockings? a. Apply the stockings and roll down the cuff. b. Remove the stockings for skin inspection two times a day. c. Remove the stockings when the patient is ambulating. d. Inspect the skin for pressure or irritation daily. ANS: B Elastic stockings improve blood flow. They should be applied early in the morning. They should be removed twice daily for 20 to 30 minutes, and the skin integrity of the feet should be examined. DIF: Cognitive Level: Application REF: p. 634 OBJ: 5 TOP: Vascular Disease and Elastic Stockings KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 39. Which instruction is most appropriate for a patient with arterial insufficiency? a. Frequently allow the legs to dangle dependently. b. Rub the legs vigorously. c. Stand often to keep blood flow in the legs. d. Walk barefoot. ANS: A Dangling legs can use gravity to help with arterial circulation. Vigorous rubbing of the legs is contraindicated, and prolonged standing strains the vascular system. The patient should never walk barefoot. DIF: Cognitive Level: Comprehension REF: p. 602 OBJ: 5 TOP: Home Instruction for the Patient with a Vascular Disorder KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 40. A nurse is preparing to administer low-molecular-weight heparin (LMWH). What is a major advantage related to the administration of LMWH? a. It can be given orally. b. It is provided fixed doses. c. It is given only after partial thromboplastin time (PTT) laboratory work. d. It provides an immediate effect. ANS: B LMWH can be given as a fixed dose without waiting for the results of the PTT. It is only given subcutaneously and does not have an immediate effect. PTT is not done to monitor LMWH. DIF: Cognitive Level: Comprehension REF: p. 652 OBJ: 5 TOP: Anticoagulant Drug Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 41. Which statement made by a patient indicates to the nurse that a teaching plan for the use of warfarin was not effective? a. “I don’t take aspirin anymore.” b. “I read that grapefruit interferes with warfarin.” c. “I’m drinking too much tea. My urine looks like tea.” d. “I wear my medical alert bracelet all the time.” ANS: C Anticoagulants, such as warfarin (Coumadin), can cause bleeding. A sign of bleeding may be bruising, tea- or cola-colored urine, or dark-colored stool. DIF: Cognitive Level: Application REF: p. 629 OBJ: 5 TOP: Anticoagulant Therapy KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 42. What medication obtained in a patient’s history will lessen the effects of warfarin (Coumadin)? a. Iron supplement for anemia b. Simvastatin (Zocor) for the control of cholesterol c. Furosemide (Lasix) for fluid retention d. Yaz (drospirenone/estradiol) as an oral contraceptive ANS: D Oral contraceptives lessen the effects of warfarin (Coumadin). DIF: Cognitive Level: Knowledge REF: p. 629 OBJ: 5 TOP: Drug Therapy KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies MULTIPLE RESPONSE 1. Which factors affect stroke volume? (Select all that apply.) a. Contractility b. Climate c. Age d. Preload e. Afterload ANS: A, D, E Stroke volume is dependent on contractility, preload, and afterload. Age may affect all three, but the stroke volume, regardless of age, is dependent on these three factors. DIF: Cognitive Level: Knowledge REF: p. 597 OBJ: 1 TOP: Stroke Volume KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Which age-related changes in the heart should a nurse take into consideration? (Select all that apply.) a. Decrease in contractility b. Thickened valves c. Stiffened valves d. Decreased SA node cells e. Increased nerve fibers in ventricles ANS: A, B, C, D Aging thickens and stiffens the valves and reduces the cells in the SA node. Age decreases the nerve fibers in the ventricles. DIF: Cognitive Level: Knowledge REF: p. 601 OBJ: 2 TOP: Age-Related Cardiac Changes KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. Why do older persons adapt more slowly to changes in the peripheral vascular system? (Select all that apply.) a. Slowing heart rate b. Decreasing cardiac output c. Increasing stroke volume d. Stiffening of blood vessels e. Thickening of aorta ANS: A, B, D, E Age-related changes include a slowing of the heart rate, a decrease in both cardiac output and stroke volume, and a stiffening and thickening of blood vessels. DIF: Cognitive Level: Comprehension REF: p. 601 OBJ: 2 TOP: Age-Related Changes to the Cardiovascular System KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A nurse suspects a circulatory disorder in one leg. Which assessments should the nurse include when comparing both legs? (Select all that apply.) a. Color b. Warmth c. Muscle strength d. Pulse quality e. Hair loss on extremity ANS: A, B, D, E Muscle strength is not a circulatory assessment. Color, warmth, pulse quality, and loss of superficial hair are indicators of decreased arterial perfusion. DIF: Cognitive Level: Application REF: p. 601 OBJ: 3 TOP: Circulatory Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. At rest, the cardiac cells in the myocardium are electrically polarized, with the inside of the cell being more than the outside of the cell. ANS: negative When the heart is at rest, the inside of the cell is negatively charged. DIF: Cognitive Level: Comprehension REF: p. 609 OBJ: 1 TOP: Polarization of Myocardium KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse explains that the lining of a vessel that allows for smooth blood flow and also reduced resistance in the vessel is the of the vessel. ANS: intima The interior lining of a blood vessel is referred to as the intima. DIF: Cognitive Level: Knowledge REF: p. 598 OBJ: 1 TOP: Intima KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A nurse explains that when a patient history reveals a recent episode of vomiting and diarrhea, the nurse anticipates that this fluid loss will cause and increased blood viscosity. ANS: hemoconcentration Hemoconcentration occurs when fluid is lost through dehydration, which makes the blood more viscous and shows an inaccurately high value of hemoglobin. DIF: Cognitive Level: Comprehension REF: p. 600 OBJ: 1 TOP: Hemoconcentration KEY: Nursing Process Step: Intervention MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A nurse uses a picture to demonstrate the conduction pathway through the chambers of the heart. (Arrange the following options in the correct sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. The atria contract. b. Conduction occurs through the bundle branches. c. The AV node fires. d. The Purkinje fibers conduct. e. The SA node fires. f. The ventricles contract. ANS: EACBDF The conduction pathway begins in the SA node, travels down the atrial wall, depolarizing the atria, to the AV node, bundle branches, and Purkinje fibers, contracting the ventricles. DIF: Cognitive Level: Comprehension REF: p. 595 OBJ: 1 TOP: Conduction Pathway for Cardiac Contraction KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 34: Cardiac Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A 49-year-old patient has multiple risk factors for coronary artery disease. Which risk factor is considered modifiable? a. Family history b. Age c. Smoking d. Male gender ANS: C Smoking, a high-fat diet, hypertension, sedentary lifestyle, and stress are considered modifiable risk factors. DIF: Cognitive Level: Comprehension REF: p. 639 OBJ: 1 TOP: Coronary Artery Disease Risk Factors KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What do fibrous plaques of atherosclerosis serve as when they are laid down in the vessels? a. Stent to keep the vessel open b. Trap to which other substances adhere c. Threat to the integrity of the vessel wall d. Embolus ANS: B The plaque surface acts as a trap to which fibrous plaques can adhere, causing more narrowing of the vessel. The enlarging plaque can become a thrombus but not an embolus because emboli are usually considered to be traveling aggregations that lodge in a small arteriole. DIF: Cognitive Level: Comprehension REF: p. 640 OBJ: 1 TOP: Atherosclerosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A patient with angina pectoris complains of chest pain at rest and needs to take three nitroglycerin (NTG) pills to relieve the pain. Of what should the nurse assess this as a major symptom? a. Stable angina b. Unstable angina c. Full-blown acute myocardial infarction (MI) d. Pulmonary embolus ANS: B A patient with angina who has pain at rest that is not relieved with one NTG pill is considered to have unstable angina, a precursor to an acute MI. DIF: Cognitive Level: Comprehension REF: p. 640 OBJ: 1 TOP: Unstable Angina KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. What is an important teaching point for a patient with mitral stenosis? a. Obtain a place on the heart transplant list. b. Balance activity with oxygen supply. c. Increase daily fluid intake to over 2000 mL. d. Have an annual electrocardiogram. ANS: B Patients with mitral stenosis need to balance their activity with their oxygen supply and avoid overhydration. DIF: Cognitive Level: Application REF: p. 657 OBJ: 1 TOP: Mitral Stenosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. What information should a nurse include in a patient’s discharge instruction after an acute myocardial infarction (MI)? a. Cautions about the use of morphine b. Detailed symptoms that indicate impending MI c. Written instructions on diet and follow-up appointments d. High-energy exercise program directions ANS: C The patient needs written instructions for diet, follow-up appointments, and exercise protocols. Giving detailed information about symptoms is not necessary other than to remind the patient about reporting chest pain and shortness of breath. A high-energy exercise program is not appropriate. Morphine is not part of the home care after an MI. DIF: Cognitive Level: Application REF: p. 647 OBJ: 1 TOP: Myocardial Infarction KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 6. A patient with acute congestive heart failure has jugular vein distention, crackles bilaterally, and dyspnea. Which nursing diagnosis should have the highest priority? a. Inadequate mobility b. Fluid volume excess c. Anxiety d. Inadequate coping ANS: B Fluid volume excess increases the workload of the heart and interferes with breathing. DIF: Cognitive Level: Application REF: p. 646 OBJ: 1 TOP: Congestive Heart Failure KEY: Nursing Process Step: Nursing Diagnosis MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. What actions should a nurse implement to decrease the workload of the heart in a patient with acute congestive failure? (Select all that apply.) a. Eliminate unnecessary activities. b. Direct the patient in active range-of-motion exercises. c. Help the patient change positions every 2 hours. d. Assist the patient to ambulate to the bathroom. e. Give a partial bed bath rather than full bed bath. ANS: A, C, E To minimize the workload of the heart, the nurse would adjust nursing care to eliminate all unnecessary activities, assist in position changes, and give a minimal bath. Ambulation and active range-of-motion exercises are unnecessary activities at this time. DIF: Cognitive Level: Application REF: p. 650 OBJ: 1 TOP: Nursing Care of Congestive Failure KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A nurse urges a 50-year-old overweight executive who had a myocardial infarction (MI) 3 months earlier to take up some conditioning exercises for 30 minutes a day. What rationale supports this suggestion? (Select all that apply.) a. Lose weight. b. Improve cardiac dysrhythmia. c. Decrease workload of the heart. d. Decrease cholesterol levels. e. Increase cholesterol levels. ANS: A, C, D Conditioning exercises performed daily for 30 minutes can reduce weight, decrease the workload of the heart, and decrease LDLs. Exercise does not affect dysrhythmias. DIF: Cognitive Level: Comprehension REF: pp. 646-647 OBJ: 3 TOP: Effects of Conditioning Exercises KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. is an abnormal thickening, hardening, and loss of elasticity of arterial walls. ANS: Arteriosclerosis Arteriosclerosis is an abnormal thickening, hardening, and loss of elasticity of arterial walls. DIF: Cognitive Level: Comprehension REF: p. 639 OBJ: 1 TOP: Arteriosclerosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. Stable angina (also called chronic stable angina) occurs most often with exercise or activity and usually subsides with . ANS: rest Stable angina (also called chronic stable angina) occurs most often with exercise or activity and usually subsides with rest. DIF: Cognitive Level: Comprehension REF: p. 640 OBJ: 1 TOP: Angina KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 35: Vascular Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What should a nurse ask a patient related to past history of deep-vein thrombosis (DVT) and other vascular problems? a. An aneurysm b. Rheumatoid arthritis c. A peptic ulcer d. Recurring chest pain ANS: D Pain in the chest or dyspnea suggests that a pulmonary embolism may have occurred from the presence of a DVT. Approximately 10% of individuals with DVT develop pulmonary emboli. DIF: Cognitive Level: Application REF: p. 670 OBJ: 4 TOP: Venous Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A 69-year-old patient reports a burning, aching pain in the legs when walking to the mailbox. These symptoms are relieved with rest. What should the nurse suspect? a. Venous insufficiency b. Claudication c. Phlebitis d. Rest pain ANS: B Arterial vascular disorders that produce pain with activity are defined as claudication, which is the result of ischemia of the tissues caused by a lack of adequate perfusion. DIF: Cognitive Level: Application REF: p. 671 OBJ: 4 TOP: Claudication KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A nurse records the assessment of stasis dermatitis on an intake assessment for a patient with peripheral vascular disease (PVD). What is the best way to describe this finding? a. Brownish skin discoloration on the lower legs b. Ulceration on medial surface of the lower legs c. Edema in the lower legs d. Purple rash on medial surface of the lower legs ANS: A Stasis dermatitis is a brownish skin discoloration on the lower legs, which is indicative of venous stasis. DIF: Cognitive Level: Application REF: p. 672 OBJ: 2 TOP: Vascular Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A nurse notes ulcerations on the surfaces of a patient’s toes. What should this assessment most likely indicate? a. Skin breakdown from pressure b. Nutritional deficit c. Venous stasis d. Arterial stasis ANS: D Arterial stasis ulcers on the tips of the patient’s toes are indicators of arterial insufficiency. This is a serious and probably progressive disorder that leads to further potential skin breakdown. DIF: Cognitive Level: Application REF: p. 671 OBJ: 2 TOP: Arterial Toe Ulcers KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. What is a characteristic of a venous stasis ulcer? a. Painlessness b. Poikilothermy c. Pale color d. Location near the groin ANS: A Venous ulcers are painless ulcers near the ankle that are warm and have a ruddy color. DIF: Cognitive Level: Knowledge REF: p. 675 OBJ: 3 TOP: Venous Stasis Ulcer KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. A patient has returned from a vein ligation and stripping. What are the appropriate instructions for a nurse to provide? a. Dangle the legs to prevent edema. b. Cross the legs to apply pressure. c. Wear compression stockings to promote circulation. d. Remove the drain after 24 hours. ANS: C Postoperative care of a patient with a vein ligation and stripping includes elevating the extremity, wearing compression stockings, taking anticoagulant therapy, and assessing the circulation of the affected extremity. DIF: Cognitive Level: Application REF: p. 670 OBJ: 4 TOP: Vein Ligation and Stripping KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. An obese postsurgical patient complains of sudden discomfort in her leg. The nurse assesses the leg and finds it cold and pale with no pedal or popliteal pulse. What should the nurse suspect? a. Venous thrombosis b. Arterial occlusion c. Vascular spasm d. Paresthesia ANS: B Signs of an acute arterial occlusion can include severe pain, absent pulses, or very pale or mottled skin. DIF: Cognitive Level: Application REF: p. 661 OBJ: 4 TOP: Acute Arterial Occlusion KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. Which postoperative sign should a nurse report immediately when caring for a patient with an endarterectomy with a synthetic graft? a. Headache b. Fever c. Edema d. Pain ANS: B A fever in a patient with a synthetic graft is a serious postoperative event. The infection may lead to an amputation. DIF: Cognitive Level: Comprehension REF: p. 663 OBJ: 4 TOP: Surgical Repair with Synthetic Graft KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. A patient with Raynaud disease has poor tissue perfusion and is being given discharge instructions. What should the nurse include when providing this information? a. Avoid sun exposure. b. Wear gloves and warm socks when outdoors. c. Chafe hands frequently to warm them. d. Wash dishes in warm water. ANS: B Chafing hands to warm them does not provide vasodilation and may cause tissue damage. Avoiding exposure to cold is paramount to prevent pain and tissue damage. Raynaud disease involves the constriction of the arterioles of the hands, toes, and nose. Pain is a cardinal symptom and can be relieved with methods to promote vasodilation. DIF: Cognitive Level: Application REF: p. 666 OBJ: 4 TOP: Raynaud Disease KEY: Nursing Process Step: Nursing Diagnosis MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. What assessment should a nurse perform on a patient after the repair of an abdominal aortic aneurysm? a. Periorbital edema b. Tremor or facial twitching c. Rising blood pressure d. Bowel sounds ANS: D Repair of aortic abdominal aneurysms causes a temporary cessation of peristalsis. Although this condition is expected, the beginning of bowel sounds indicates important progress in the recovery. Rising blood pressure is an expected recovery indication from surgery. DIF: Cognitive Level: Application REF: p. 668 OBJ: 4 TOP: Aneurysm of the Abdominal Aorta KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. What patient teaching should be included for a patient with varicose veins? a. Weight reduction b. Decreasing exercise c. Wearing a panty girdle d. Standing rather than sitting ANS: A Varicose veins are caused by a dilation of incompetent valves. Obesity, pregnancy, restrictive clothing, and prolonged standing aggravate the condition. DIF: Cognitive Level: Application REF: p. 669 OBJ: 4 TOP: Varicose Veins KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. The nurse is caring for a patient diagnosed with arterial embolism. What patient teaching information will the nurse anticipate providing to the patient? (Select all that apply.) a. Protect affected limbs from pressure. b. Apply ice packs to affected extremity as needed. c. Gradually increase activity as tolerated. d. Avoid exercise. e. Report any pain or numbness to health care provider. ANS: A, C, E Patient Teaching for Arterial Embolism should include to protect affected limbs from pressure, trauma, and temperature extremes; exercise to improve blood flow; gradually increase activity as you are able to tolerate it; report pain, numbness, coolness, and pale or bluish skin color to your health care provider. DIF: Cognitive Level: Comprehension REF: p. 662 OBJ: 1 TOP: Arterial Embolism KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. is intermittent constriction of arterioles that affects the hands primarily, although it can affect the toes and tip of the nose. ANS: Raynaud phenomena Primary and secondary Raynaud phenomena are forms of an intermittent constriction of arterioles that affects the hands primarily, although it can affect the toes and tip of the nose. DIF: Cognitive Level: Knowledge REF: p. 666 OBJ: 1 TOP: Raynaud phenomena KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. Hyperbaric O2 therapy may be prescribed in an attempt to promote healing of the ulcer by reducing capillary pressure and the blood. ANS: hyperoxygenating Hyperbaric O2 therapy may be prescribed in an attempt to promote healing of the ulcer by reducing capillary pressure and hyperoxygenating the blood. DIF: Cognitive Level: Comprehension REF: p. 673 OBJ: 2 TOP: Hyperbaric O2 Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 36: Hypertension Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient inquires if his blood pressure is normal. What is the nurse’s most accurate response regarding the definition of normal blood pressure? a. Less than 144/90 mm Hg b. Less than 138/86 mm Hg c. Less than126/82 mm Hg d. Less than 120/80 mm Hg ANS: D Normal blood pressure is defined as a systolic pressure of less than 120 mm Hg and a diastolic blood pressure of less than 80 mm Hg. DIF: Cognitive Level: Knowledge REF: p. 677 OBJ: 1 TOP: Normal Blood Pressure KEY: chapter_50 MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. An obese African-American man reports that he smokes. How should the nurse stage this patient’s hypertension? a. Grade A b. Grade B c. Grade C d. Grade D ANS: B Criteria for grade B are that the patient has more than one risk factor (African American, obese, smoker), with no target organ damage and no clinical cardiovascular problems. Criteria for grade A indicate that no risks have been assessed, and the criteria for grade C include target organ damage and clinical cardiovascular disease or diabetes mellitus. DIF: Cognitive Level: Application REF: p. 677 OBJ: 3 TOP: Staging of Hypertension KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. Which is true regarding hypertension in older adults? a. It is age related. b. It is unavoidable. c. It is progressively disabling. d. It improves with treatment. ANS: D Older adults with hypertension have good results with aggressive therapy, although the age-related changes cannot be avoided. DIF: Cognitive Level: Comprehension REF: p. 684 OBJ: 3 TOP: Hypertension and Older Adults KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A patient is being evaluated every week for possible hypertension and is classified as prehypertensive. Which assessment would support this conclusion? a. Blood pressure reading over 120/80 mm Hg for two consecutive visits b. Blood pressure reading over 130/85 mm Hg for over 2 months c. Blood pressure reading over 140/95 mm Hg for 2 months d. Blood pressure reading over 144/100 mm Hg at one visit ANS: A Prehypertension is diagnosed after two readings of over 120/80 mm Hg. The reading of 135/85 mm Hg for 2 months is longer than the diagnostic criteria require. Blood pressures consistently over 140/90 mm Hg are classified as hypertension. DIF: Cognitive Level: Comprehension REF: p. 677 OBJ: 3 TOP: Risk Factors for Hypertension KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A patient with hypertension reports the symptom of headache. How do headaches related to hypertension characteristically occur? a. Frontal in the afternoon b. Temporal on exertion c. Occipital on arising d. Frontal at night ANS: C Hypertension occipital headaches occur on awakening. DIF: Cognitive Level: Comprehension REF: p. 679 OBJ: 3 TOP: Symptoms of Hypertension KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. What does treatment for essential hypertension focus on? a. Daily medication with mild diuretics b. Low-dose vasodilators c. Reduction of modifiable risks d. Combination of vasodilators and diuretics ANS: C The therapeutic approach to essential hypertension is a nonpharmacologic treatment. The treatment plan is to identify and reduce the modifiable risks, which include weight loss, dietary changes, and increased exercise. DIF: Cognitive Level: Comprehension REF: p. 680 OBJ: 1 | 6 TOP: Pathophysiology of Hypertension KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. What is the focus of treatment for secondary hypertension? a. Smoking cessation program b. Strenuous exercise program c. Weight loss program designed to reduce weight rapidly d. Specific etiologic disease ANS: D Secondary hypertension has an identifiable cause. Treating the cause is the focus of care for secondary hypertension. DIF: Cognitive Level: Comprehension REF: p. 685 OBJ: 1 | 6 TOP: Hypertension Treatment KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. What do blood pressure readings need to exceed for a patient to be diagnosed with hypertension? a. 120/80 mm Hg b. 130/90 mm Hg c. 140/90 mm Hg d. 150/100 mm Hg ANS: C The official diagnosis of hypertension is dependent on a period of observation during which the BP is consistently higher than 140/90 mm Hg. DIF: Cognitive Level: Comprehension REF: p. 677 OBJ: 5 TOP: Parameters for Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. A patient is taking hydrochlorothiazide (HydroDIURIL) for hypertension. When providing dietary teaching what should the nurse encourage the patient to increase the intake of? a. Bananas b. Apple juice c. Sugar-free foods d. Low-fat milk ANS: A Diuretics reduce fluid volume and can cause hypokalemia. Encourage foods high in potassium, such as bananas and orange juice. DIF: Cognitive Level: Comprehension REF: p. 684 OBJ: 4 TOP: Drug Therapy for Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 10. An obese 38-year-old African-American patient with diabetes is being evaluated for the use of propranolol (Inderal) in controlling hypertension. What is a contraindication for the use of propranolol (Inderal) in this patient? a. Race b. Age c. Diabetes d. Weight ANS: C Hypoglycemia can occur with this medication and places those with diabetes at high risk for adverse effects. DIF: Cognitive Level: Application REF: p. 682 OBJ: 4 TOP: Drug Therapy for Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 11. An 89-year-old patient is taking an antihypertensive medication. What should the nurse include when providing home care teaching? a. Get up out of bed slowly. b. Take hot baths. c. Report sexual dysfunction immediately. d. Stop taking the drug if side effects occur. ANS: A Patients taking antihypertensive medications should get up slowly to prevent falling. They should avoid hot baths because they promote vasodilatation, and they should never stop the drug abruptly. Sexual dysfunction is a possible side effect, but it does not have to be reported immediately. DIF: Cognitive Level: Application REF: p. 683 OBJ: 4 TOP: Drug Therapy in Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 12. What should a nurse instruct a patient who has been started on verapamil (Calan) for elevated blood pressure to monitor? a. Urine output b. Pulse c. Stool for blood d. Edema ANS: B Verapamil (Calan) is a calcium channel blocker and most often causes bradycardia. DIF: Cognitive Level: Application REF: p. 683 OBJ: 4 TOP: Drug Therapy in Hypertension KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 13. A patient is prescribed an angiotensin-converting enzyme (ACE) inhibitor, enalapril (Vasotec). What is an appropriate instruction for the nurse to provide? a. Monitor potassium intake. b. Report asthma symptoms. c. Return for follow-up visits. d. Assess blood sugar closely. ANS: C ACE inhibitors can cause neutropenia or other blood dyscrasias, and follow-up with blood assessments should be periodically performed. DIF: Cognitive Level: Application REF: p. 683 OBJ: 4 TOP: Drug Therapy in Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 14. An 87-year-old patient is taking furosemide (Lasix) for elevated blood pressure. What should the nurse know that older patients are at risk for? a. Falls b. Hypokalemia c. Reflex tachycardia d. Neutropenia ANS: B Older adults are at greater risk for side effects, especially hypokalemia. DIF: Cognitive Level: Comprehension REF: p. 684 OBJ: 4 TOP: Drug Therapy in Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 15. A nurse is providing patient education regarding a low-sodium diet. In addition to the use of spices, what should the nurse recommend to help decrease sodium in the diet? a. Catsup b. Garlic c. Soy sauce d. Cheese ANS: B Spices, garlic, and onions are good substitutes for sodium as flavorings. Catsup, soy sauce, and cheese all have large amounts of sodium. DIF: Cognitive Level: Comprehension REF: p. 688 OBJ: 4 TOP: Sodium-Free Seasoning KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 16. Which lifestyle change has the greatest effect on reducing hypertension? a. Sodium restriction b. Reduction in alcohol consumption c. Daily aerobic exercise d. Weight reduction ANS: D Weight reduction has the greatest effect on reducing hypertension. DIF: Cognitive Level: Comprehension REF: p. 681 OBJ: 3 TOP: Blood Pressure Screening KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. A nurse is educating a group of patients regarding Dietary Approaches to Stop Hypertension (DASH) diet. What recommendation should the nurse include as a source of protein and fat? a. Lean red meat b. Whole grains c. Low fiber d. Sugar ANS: B The DASH diet uses whole grains as a source of protein and fat. DIF: Cognitive Level: Comprehension REF: p. 687 OBJ: 6 TOP: DASH Diet KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 18. Which antihypertensive medication is contraindicated in patients who have chronic obstructive pulmonary disease (COPD) and asthma? a. Propranolol (Inderal): beta-adrenergic receptor blocker b. Hydrochlorothiazide (HydroDIURIL): diuretic c. Diltiazem (Cardizem): calcium antagonist d. Captopril (Capoten): ACE inhibitor ANS: A Beta-blocking adrenergic agents block stimulation of catecholamine receptors and cause bronchoconstriction. DIF: Cognitive Level: Comprehension REF: p. 683 OBJ: 4 TOP: Drug Therapy in Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 19. A nurse is caring for a patient who is taking antihypertensive therapy. The patient reports fatigue and has a pulse of 54 beats/min. Which medication administered is most likely the cause of these symptoms? a. Diltiazem (Cardizem) b. Furosemide (Lasix) c. Hydrochlorothiazide (HydroDIURIL) d. Methyldopa (Aldomet) ANS: A Calcium channel blockers such as diltiazem and verapamil can cause bradycardia because conduction is slowed in the heart. These drugs also reduce stroke volume and cardiac output, which may result in fatigue. DIF: Cognitive Level: Application REF: p. 683 OBJ: 4 TOP: Drug Therapy for Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 20. What should a nurse include when developing a teaching plan for a patient with hypertension? a. Stop medications if side effects occur. b. Maintain a diet high in unsaturated fat. c. Advise no further visits if no other symptoms occur. d. Encourage relaxation techniques. ANS: D Patients with hypertension should never stop medications without discussing it with their physicians. A diet low in saturated and unsaturated fat should be followed. Visits to monitor blood pressure should continue because hypertension is often asymptomatic. Stress can aggravate hypertension; stress management or relaxation strategies should be implemented. DIF: Cognitive Level: Application REF: p. 680 OBJ: 7 TOP: Care Plan for Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 21. A patient reports drowsiness after initiating atenolol (Tenormin) for the treatment of hypertension. What is the nurse’s best response when educating this patient about atenolol (Tenormin)? a. Take the medication at bedtime. b. Reduce the dose of the medication until the desired effect occurs. c. Avoid activities that require alertness. d. Talk to the physician because drowsiness is not an anticipated side effect. ANS: A Sedation is an expected side effect of atenolol. This medication can be taken daily at bedtime. Doses should not be changed without talking to the physician. Activities requiring that the patient be alert should be postponed until later in the day. DIF: Cognitive Level: Application REF: p. 683 OBJ: 4 TOP: Drug Therapy and Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 22. A patient taking methyldopa (Aldomet) for hypertension reports to the emergency department with a severe headache, blurred vision, and a blood pressure reading of 200/94 mm Hg. What should the nurse suspect is happening to this patient? a. Hyperglycemia b. Inadequate coping with sedation c. Abrupt cessation of medication d. Sexual dysfunction ANS: C Abruptly stopping antihypertensive medications can result in a hypertensive crisis. The patient’s presenting symptoms may include rebound hypertension and reports of confusion, nausea, restlessness, headache, and vision abnormalities. DIF: Cognitive Level: Application REF: p. 683 OBJ: 7 TOP: Drug Therapy and Hypertension KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 23. Which patient is at the highest risk for malignant hypertension? a. White postmenopausal women b. Obese Asians c. Young African-American adults d. Older Latino men ANS: C Malignant hypertension occurs suddenly and usually exhibits a diastolic blood pressure higher than 140 mm Hg. It most commonly occurs in young African-American adults. DIF: Cognitive Level: Comprehension REF: p. 689 OBJ: 5 TOP: Hypertensive Crisis KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 24. A patient with hypertension comes to the emergency department and is experiencing nausea and vomiting and is restless and confused. Vital signs are assessed at blood pressure, 220/130 mm Hg; pulse, 120 beats/min; and respirations, 32 breaths/min. What should the nurse conclude the patient is experiencing based on these assessments? a. Hypertension crisis from the cessation of a drug b. Stroke from increased blood pressure c. Adverse drug reaction d. Onset of diabetes ANS: A Patients with a hypertensive crisis usually experience nausea and vomiting, headache, and elevated vital signs because of an abrupt cessation of the hypertensive drug. DIF: Cognitive Level: Analysis REF: p. 689 OBJ: 6 TOP: Care of the Patient in Hypertensive Crisis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 25. What should be the nursing priority when caring for a patient with a hypertensive crisis? a. Suctioning secretions b. Monitoring for seizure activity c. Monitoring fluid volume d. Preventing hyperthermia ANS: B The care of a patient with hypertensive crisis focuses on monitoring for seizure activity and level of consciousness, which would suggest the occurrence of a stroke. DIF: Cognitive Level: Application REF: p. 689 OBJ: 6 TOP: Care of Patient with Hypertensive Crisis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. What are the advantages of hydrochlorothiazide (HydroDIURIL)? (Select all that apply.) a. Is potassium sparing b. Is effective for African Americans c. Consistently controls blood pressure d. Has no side effects e. Decreases heart rate ANS: B, C Hydrochlorothiazide is a potassium-sparing diuretic that provides consistent blood pressure control and is effective for African Americans. It does have side effects, however, and does nothing to decrease heart rate directly. DIF: Cognitive Level: Knowledge REF: p. 684 OBJ: 4 TOP: Diuretic Drugs KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. A nurse is providing care to a patient diagnosed with essential hypertension. What should the nurse know is included in a first-line therapeutic approach to lowering this patient’s blood pressure? (Select all that apply.) a. Smoking cessation b. Beta-blockers c. Exercise programs d. Weight loss e. Decreased sodium intake ANS: A, C, D, E The first methodology is a nonpharmacologic approach, using lifestyle changes rather than drugs. DIF: Cognitive Level: Comprehension REF: p. 680 OBJ: 3 TOP: Essential Hypertension Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. Which conditions are considered potential causes of secondary hypertension? (Select all that apply.) a. Renal disease b. Coarctation of the aorta c. Colon cancer d. Increased intracranial pressure (ICP) e. Rheumatoid arthritis ANS: A, B, D Renal disorders, constriction or stiffening of the aorta, and conditions that result in ICP are common causes of secondary hypertension. DIF: Cognitive Level: Knowledge REF: p. 678 OBJ: 3 TOP: Secondary Hypertension KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. A nurse explains that the force against which the left ventricle must work to force the blood into the circulation is called . ANS: peripheral vascular resistance Peripheral vascular resistance is the pressure against which the left ventricle must work to put blood in the circulating volume. DIF: Cognitive Level: Knowledge REF: p. 677 OBJ: 2 TOP: Peripheral Vascular Resistance KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse explains that hypertension occurs when a chain reaction of events takes place. (Place the following options in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Ephedrine constricts vessels and increases the heart rate. b. Renin constricts vessels and decreases the blood flow to the kidneys. c. Angiotensin constricts vessels in response to renin. d. Norepinephrine constricts vessels, increasing peripheral vascular resistance. e. The adrenal cortex produces aldosterone, causing fluids and sodium to be retained. ANS: DABCE The sequence is that norepinephrine, in response to the sympathetic nervous system, constricts vessels, causing an increase in peripheral vascular resistance; epinephrine constricts vessels and increases the heart rate; and renin is released because of the reduced blood flow to the kidneys, which stimulates the production of an angiotensin. Angiotensin stimulates the adrenal cortex to excrete aldosterone, causing retention of fluid and sodium. DIF: Cognitive Level: Comprehension REF: p. 678 OBJ: 2 TOP: Pathophysiologic Sequence of Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 37: Digestive System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is preparing to give a tube feeding using a large syringe. What action should the nurse implement before starting the infusion? a. Roll the patient flat. b. Check for a residual formula and return the residual to his or her stomach. c. Place the end of the tube in water and check for bubbles. d. Flush the tube. ANS: B Verifying tube placement by pulling up the residual formula is a standard of care for a tube feeding. DIF: Cognitive Level: Application REF: p. 708 OBJ: 4 TOP: Tube Feeding KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 2. After receiving a tube feeding, a nurse assesses the patient to be sweaty with abdominal distention and diarrhea. What is the most likely cause of this response? a. Expected reaction to the tube feeding b. Dumping syndrome c. Gastric reflux syndrome d. Onset of gastroenteritis ANS: B Dumping syndrome is caused by infusing a tube feeding too fast or infusing a tube feeding that is too rich a formula. DIF: Cognitive Level: Application REF: p. 708 OBJ: 3 TOP: Dumping Syndrome KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A nurse administers promethazine (Phenergan) for nausea. Which extra precautionary action should the nurse implement because of the common side effect of antiemetic medications? a. Check vital signs for erratic blood pressure. b. Add a blanket to prevent chilling. c. Provide extra water to combat thirst. d. Put up side rails to prevent falls. ANS: D Most antiemetic medications cause drowsiness because of their effects on the central nervous system, resulting in dizziness and confusion. DIF: Cognitive Level: Application REF: p. 714 OBJ: 4 TOP: Antiemetic Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 4. A patient complains about the placement of the total parenteral nutrition (TPN) line and asks why it cannot be inserted in the arm. What fact regarding the placement of this line should the nurse base a response on? a. Arm would limit patient mobility. b. Subclavian artery allows for ease in dressing the puncture site. c. Arm prevents the use of large-bore cannulas. d. Subclavian artery allows for rapid dilution. ANS: D The rich TPN solution is rapidly diluted in the larger vessel, preventing phlebitis. DIF: Cognitive Level: Comprehension REF: p. 709 OBJ: 3 TOP: TPN KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A patient inquires if this newer type of gastric analysis is going to require passage of a nasogastric tube. What is the nurse’s most accurate reply? a. “Yes, but just for the instillation of the dye.” b. “No. You take a dye orally, which will be excreted in the urine in approximately 2 hours.” c. “Yes. You will take the dye orally, and then several gastric withdrawals through the tube will show the dye.” d. “Yes. Only one withdrawal will be made through the tube, which will be treated with dye and read in approximately 2 hours.” ANS: B Dye is given orally, and if hydrochloric acid is present, the dye will be excreted in the urine in approximately 2 hours. The older method of taking serial gastric samples every 15 minutes through a nasogastric tube may still be used. DIF: Cognitive Level: Application REF: p. 702 OBJ: 1 TOP: Newer Method of Gastric Analysis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 6. A nurse is caring for a patient receiving total parenteral nutrition (TPN). Which nursing action is most appropriate to implement? a. Use a clean technique for site care. b. Infuse the solution rapidly. c. Administer medications through the TPN line. d. Monitor the temperature for elevation. ANS: D Temperature should be monitored for signs of potential infection. When caring for a patient receiving TPN, sterile technique is used for site care. If solution is given too rapidly, the patient may have circulatory overload. The TPN catheter should never be used for medication administration. DIF: Cognitive Level: Application REF: p. 710 OBJ: 4 TOP: TPN KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. Which patient assessment indicates hyperglycemia with TPN feeding? a. Increase of urine output b. Sudden diarrhea c. Abdominal distention d. Tachycardia ANS: A Increased urine output would indicate a probable increase in blood glucose. DIF: Cognitive Level: Comprehension REF: p. 710 OBJ: 3 TOP: TPN KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. The TPN feeding is running at 20 mL and is 1 hour behind schedule. What is the most appropriate initial nursing intervention? a. Increase the flow rate to 22 mL/hr (10%) and inform the charge nurse. b. Reposition the patient to the right side and lower the head of the bed. c. Dilute the thick feeding formula with 10 mL of sterile water and inform the charge nurse. d. Document the event and inform the charge nurse. ANS: D Increasing the speed of giving TPN feedings is never a consideration because doing so will cause hyperglycemia. The event should be documented and the charge nurse informed. DIF: Cognitive Level: Application REF: p. 710 OBJ: 3 | 4 TOP: TPN KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 9. What is the most current endoscopic procedure for examining the small intestine? a. Capsule camera b. Fiberoptic light probe c. Rigid lighted tubes d. Flat plate ANS: A The capsule camera is swallowed and transmits information about the small bowel to a receiver on a belt around the patient’s waist. DIF: Cognitive Level: Knowledge REF: p. 700 OBJ: 1 TOP: Endoscopy KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. A nurse has collected several stool specimens for ova and parasites that are to be sent to the laboratory. What action is most appropriate for the nurse to implement? a. Immediately take the specimens to the laboratory to be tested for parasites and ova. b. Take the specimens to the laboratory to be tested for culture and sensitivity and leave them for later pickup. c. Take the specimens to the refrigerator to be tested later for parasites and ova. d. Leave the specimens in a warm place until convenient time to deliver to the laboratory. ANS: A Parasite and ova specimens should be immediately taken to the laboratory while the parasites are still alive. Specimens for evaluating pathogenic organisms should be kept cool. DIF: Cognitive Level: Application REF: p. 706 OBJ: 1 TOP: Care of Stool Specimens KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. Stool softeners are prescribed to promote normal elimination of feces. What is the most appropriate way to ensure effectiveness of this type of drug? a. Mouth care b. Ambulation c. Adequate fluid intake d. High-fiber diet ANS: C Adequate fluids must be maintained to ensure the liquid is available; otherwise, the fecal mass will remain hard. DIF: Cognitive Level: Comprehension REF: p. 713 OBJ: 3 TOP: Constipation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. Which set of findings best indicates that a patient with intestinal obstruction has achieved normal hydration? a. Pulse and blood pressure are within the patient’s norms, mucous membranes are moist, and fluid intake and output are equal. b. Pulse rate is strong (at least 60 beats/min), bowel sounds are normal, and a respiratory rate of 22 breaths/min is recorded. c. Blood pressure is within the patient’s norm, the temperature is below normal, and adequate tissue turgor is observed. d. Mucous membranes are moist, the 24-hour fluid intake is higher than the 24-hour output, and the pulse rate is elevated. ANS: A Vital sign within normal limits, moist mucous membranes, and equal fluid intake and output are indicative of normal hydration. DIF: Cognitive Level: Comprehension REF: p. 698 OBJ: 4 TOP: Hydration KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. After abdominal surgery, a patient must cough and take deep breaths. How can the nurse best achieve this with this patient? a. Withhold analgesics until the patient performs this task. b. Help the patient splint the incision with a pillow. c. Explain that pneumonia occurs if deep breathing is not carried out every 4 hours. d. Ambulate the patient 40 feet to increase his need for oxygen. ANS: B Splinting decreases pain by supporting the muscles, thereby allowing for better lung expansion. DIF: Cognitive Level: Application REF: p. 701 OBJ: 3 | 4 TOP: Abdominal Surgery KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 14. A patient is being seen for the first time at a physician’s office. When assisting with the assessment, a nurse notices abdominal striae. What alternative term should the nurse use when the patient asks what it is all over her abdomen? a. Scarring b. Lesions c. Rashes d. Stretch marks ANS: D Striae is the medical term for stretch marks. DIF: Cognitive Level: Knowledge REF: p. 698 OBJ: 3 TOP: Inspection KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. What information about when and where specific digestion of food takes place should be included in a patient teaching plan? (Select all that apply.) a. Renin breaks down milk protein in the stomach. b. Lipase breaks down fats in the stomach. c. Pepsin begins to break down proteins in the stomach. d. Liver and pancreatic secretions break down fats in the small bowel. e. Ptyalin (amylase) breaks down carbohydrates in the colon. ANS: A, B, C, D Ptyalin (amylase) breaks down carbohydrates in the mouth. DIF: Cognitive Level: Knowledge REF: p. 692 OBJ: 4 TOP: Digestive Process KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 38: Upper Digestive Tract Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is assessing a patient for risk factors that increase the chances of developing oral cancer. Which information from this patient’s history indicates a risk factor? a. Alcohol consumption b. Chewing gum c. Environmental pollution d. Consumption of a high-fat diet ANS: A Alcohol is statistically proven to be a factor because of irritation of the oral mucosa. DIF: Cognitive Level: Comprehension REF: p. 722 OBJ: 1 TOP: Oral Cancer KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A home health nurse observes a patient with esophageal cancer tilt his head back while eating. What might this cause? a. Narrowing of the esophagus b. Limiting the types of food that can be consumed c. Increased risk of aspiration d. A neck injury ANS: C Tilting the head back not only makes it more difficult to eat, but it also increases the risk of aspiration. DIF: Cognitive Level: Comprehension REF: p. 726 OBJ: 2 TOP: Feeding Technique with Esophageal Cancer KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A nurse is caring for a patient with esophageal surgery who has had stents placed in the esophagus and instructs the patient how best to avoid regurgitation. What should the nurse include in this instruction? a. Keep the bed flat. b. Eat only small meals. c. Lie on the right side after meals. d. Drink three glasses of fluid with each meal. ANS: B Eating small meals will help with reflux. Keeping the head of the bed raised and not taking in excessive fluid with meals should be practiced. DIF: Cognitive Level: Application REF: p. 727 OBJ: 1 TOP: Gastroesophageal Reflux KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A nurse is constructing a teaching plan for a patient with a hiatal hernia. What should be included in this plan to help reduce the complaints of heartburn, regurgitation, and eructation? a. Eating three well-balanced meals b. Lying down 1 hour after eating c. Sleeping without pillows d. Eating nothing for several hours before bedtime ANS: D Eating just before bedtime encourages reflux into the hernia and possible aspiration. DIF: Cognitive Level: Application REF: p. 730 OBJ: 1 TOP: Hiatal Hernia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A 60-year-old patient who has just been diagnosed with cancer of the stomach says, “I feel blank and numb.” What is the best nursing response? a. “Shock affects everyone that way.” b. “I’m sure you are considering what you should do now that you have cancer.” c. “Would you like me to bring you a sedative?” d. “What do you mean when you say ‘blank and numb’?” ANS: D Patients who seem overwhelmed often need to talk and express their feelings even if they are not sure of what their feelings are. DIF: Cognitive Level: Application REF: p. 740 OBJ: 2 TOP: Ineffective Coping KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 6. A goal for a patient with gastritis who has experienced nausea, vomiting, and diarrhea is to have a return of normal elimination patterns. Which statement best reflects this goal in a measurable manner? a. The patient will have fewer stools. b. Diarrhea will be controlled and not return. c. The patient will have no more than one stool per day. d. The patient’s bowel pattern will return to normal. ANS: D Goals are to be specific and measurable. The patient knows his or her normal pattern. DIF: Cognitive Level: Application REF: p. 732 OBJ: 1 TOP: Gastritis KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. A nurse is caring for a patient hemorrhaging from a peptic ulcer when the patient complains of a sharp sudden pain and has a rapidly deteriorating condition. What is the best first action of the nurse? a. Roll the patient flat and assess the vital signs. b. Notify the charge nurse. c. Suction the mouth. d. Prepare for intravenous infusions. ANS: A With a rapidly deteriorating patient, the nurse should collect all the information that will need to be reported, such as vital signs, patient condition, and subjective complaints. DIF: Cognitive Level: Application REF: p. 732 OBJ: 1 TOP: Perforated Ulcer KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. A long-term care nurse is assisting a well-nourished, 80-year-old resident with the diagnosis of esophageal cancer on methods to deal with dysphagia. What nursing intervention will best help to improve the resident’s condition? a. Instruct the patient to tilt his or her head slightly forward. b. Assist patient to a semi-Fowler position. c. Encourage the resident to eat meals in the main dining area. d. Insert a nasogastric tube for feedings. ANS: A General interventions helpful in managing dysphagia include a quiet, relaxed environment and an erect position with the head slightly tilted forward. If dysphagia prevents adequate nutritional intake, then alternative feeding method must be used and ordered by the health care provider. DIF: Cognitive Level: Application REF: p. 726 OBJ: 1 TOP: Esophageal Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. A home health nurse is assigned to follow-up on a patient recently diagnosed with gastroesophageal reflux disease (GERD). Which primary symptom should the nurse take into consideration when updating the nursing interventions on this patient’s care plan? a. Nausea b. Vomiting c. Anorexia d. Heartburn ANS: D The onset of GERD symptoms may be sudden or gradual. Patients typically report a painful burning sensation that moves up and down, commonly occurs after meals, and is relieved by antacids. Acid regurgitation, intermittent dysphagia, and belching are also common. DIF: Cognitive Level: Comprehension REF: p. 728 OBJ: 1 TOP: GERD KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. A patient experiencing nausea reports to the nurse that she adds ginger root to her morning tea to calm her stomach. Which classification of medication in the patient history alerts the nurse to provide further education? a. Antidepressants b. Proton pump inhibitors c. Anticoagulants d. Narcotics ANS: C Ginger root is effective in calming upset stomach, reducing flatulence, and preventing motion sickness. It enhances the action of anticoagulant and antiplatelet agents. DIF: Cognitive Level: Application REF: p. 728 OBJ: 1 TOP: Complementary and Alternative Therapies KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. When assessing the tongue of patient in the outpatient clinic, a nurse observes bluish-white lesions on the mucous membranes. When reviewing the patient history, the nurse notes the patient has been on long-term antibiotic therapy for chronic prostatitis. What should the nurse suspect? a. Thrush b. Aphthous stomatitis c. Herpes simplex type I d. Oral cancer ANS: A Candida albicans, a yeast-like fungus, causes the oral condition known as thrush or candidiasis. Bluish-white lesions can be seen on the mucous membranes of the oral cavity. Patients at high risk for candidiasis include those on steroids or long-term antibiotic therapy. DIF: Cognitive Level: Comprehension REF: p. 721 OBJ: 1 TOP: Oral Infections KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 12. When assisting with the admission of a new resident to a long-term care facility, a nurse notes a current history of peptic ulcer disease. What type of pain should the nurse expect the resident to describe? a. Sharp b. Dull c. Burning d. Stabbing ANS: C Some patients with gastric ulcers have no pain, but others experience a burning or cramping pain 2 to 4 hours after meals. DIF: Cognitive Level: Comprehension REF: p. 733 OBJ: 1 TOP: Peptic Ulcer KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. A nurse is caring for a patient with achalasia. What nursing actions should be implemented to help the patient reduce swallowing difficulty? (Select all that apply.) a. Identify foods that cause the problem. b. Experiment with different eating positions. c. Elevate the head of the bed at night. d. Suggest eating more rapidly. e. Offer small bites of fresh vegetables. ANS: A, B, C Eating rapidly and eating small bites increase swallowing difficulties. DIF: Cognitive Level: Application REF: p. 724 OBJ: 1 TOP: Achalasia KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 39: Lower Digestive Tract Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Which instruction given to a patient with irritable bowel syndrome (IBS) should lessen discomfort? a. Eat only whole grains. b. Take small bites and chew well. c. Include dietary fiber in at least two meals per day. d. Drink herbal teas and low-calorie cola drinks. ANS: B Taking small bites, chewing food well, and eating slowly will reduce some of the discomfort associated with IBS. Caffeine and high-fiber foods should be avoided. DIF: Cognitive Level: Comprehension REF: p. 757 OBJ: 3 | 4 TOP: IBS KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A nurse is caring for a 34-year-old patient admitted with severe diarrhea that has been going on for 2 weeks. What assessment should the nurse anticipate? a. Edema of lower legs and feet b. Hypotension and fatigue c. Hypertension and hunger d. Metabolic alkalosis ANS: B Diarrhea of long-standing duration will cause dehydration and fatigue with accompanying hypotension. The patient will most likely be in metabolic acidosis as a result of the loss of the essentially basic bowel contents. DIF: Cognitive Level: Application REF: p. 757 OBJ: 3 TOP: Diarrhea KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A nurse describes a patient as morbidly obese because the patient has a weight of 387 lb and a height of 2 meters. What is the patient’s body mass index (BMI)? a. 58.4 b. 52.8 c. 43.9 d. 31.6 ANS: C Body mass index is calculated by dividing the weight in kilograms by the height in meters squared. Anyone weighing more than 30 kg is considered obese; 387 lb ÷ 2.2 lb/kg = 176 kg; 176 kg ÷ 4 m = BMI of 43.9. DIF: Cognitive Level: Analysis REF: p. 742 OBJ: 4 TOP: Body Mass Index KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. Which statement by a patient with an ileostomy as a remedy for ulcerative colitis indicates the need for further teaching? a. “I will avoid milk products.” b. “I should select food with less dietary fiber.” c. “I’ll miss my martini before dinner.” d. “I will be glad when the surgeon closes this ileostomy.” ANS: D The ileostomy is permanent. The diet of a person prone to ulcerative colitis is low roughage, no milk products, and no alcohol. DIF: Cognitive Level: Comprehension REF: p. 757 OBJ: 4 TOP: Inflammatory Bowel Disease KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A nurse identifies a risk factor in an older man that places him at risk for developing diverticulosis. What patient information indicates such a risk factor? a. Eats a low-fiber diet b. Chronic diarrhea c. History of using nonsteroidal anti-inflammatory drugs (NSAIDs) d. Family history of colon cancer ANS: A A low-fiber diet increases the risk for diverticulitis. DIF: Cognitive Level: Comprehension REF: p. 757 OBJ: 4 TOP: Diverticulitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. Which foods should an individual with diverticulosis avoid? a. Peanuts and raspberries b. Apples and pears c. Red meat and dairy products d. Bran and whole grains ANS: A Foods containing seeds or small hard particles could become lodged in small pouches. DIF: Cognitive Level: Application REF: p. 758 OBJ: 3 | 4 TOP: Diverticulosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. Colonoscopy results indicate the diagnosis of irritable bowel disease (IBD) in a patient admitted to the hospital with diarrhea. What information should the nurse include when preparing patient education regarding diet? a. Dairy products are encouraged. b. No added salt is required. c. Low roughage should be followed. d. Protein foods are restricted. ANS: C A low-roughage diet without milk products is prescribed for mild to moderate IBD. DIF: Cognitive Level: Comprehension REF: p. 756 OBJ: 3 | 4 TOP: IBD KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. A nurse is caring for a patient diagnosed with diverticulosis and assesses a temperature of 102.4 F and abdominal rigidity. What should the nurse be aware is the most likely cause of these signs and symptoms? a. Infection b. Constipation c. Perforation d. Obstruction ANS: C The nurse caring for a patient diagnosed with diverticulosis should be alert for signs of perforation including fever, abdominal distention, and rigidity. DIF: Cognitive Level: Application REF: p. 759 OBJ: 3 | 4 TOP: Diverticulosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. A patient is diagnosed with cancer of the large intestine. What is the most likely initial recommended medical intervention? a. Repeat colonoscopy b. Surgery c. Radiation therapy d. Chemotherapy ANS: B Colorectal cancers are usually initially treated surgically. DIF: Cognitive Level: Knowledge REF: p. 759 OBJ: 3 | 4 TOP: Colorectal Cancer KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. A nurse is performing an assessment of a patient after an abdominoperineal resection. How many incision sites will be present? a. Two b. Three c. Four d. Five ANS: B After an abdominoperineal resection, the patient will have three incisions: one on the abdomen, a second for the colostomy, and a third on the perineum. DIF: Cognitive Level: Knowledge REF: p. 759 OBJ: 3 | 4 TOP: Abdominoperineal resection KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. A patient reports severe pain after an abdominoperineal resection. What position should the nurse assist this patient into in order to promote comfort? a. Side-lying b. Supine c. Prone d. Semi-Fowler ANS: A Pain is severe for several days after an abdominoperineal resection. At first, the patient will be most comfortable in a side-lying position. DIF: Cognitive Level: Application REF: p. 760 OBJ: 3 | 4 TOP: Abdominoperineal resection KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 12. A nurse provides education to a patient after a hemorrhoidectomy. Which statement by the patient demonstrates the need for further instruction? a. “Sitz baths are ordered to soothe the area.” b. “Imagery may help control pain.” c. “Bleeding should be reported.” d. “Fluids are restricted.” ANS: D After hemorrhoidectomy, the patient should be encouraged to ingest a high-fiber diet and drink plenty of fluids to promote regular, soft stools. DIF: Cognitive Level: Comprehension REF: p. 762 OBJ: 3 | 4 TOP: Hemorrhoidectomy KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. A nurse notes a diagnosis of pilonidal cyst on a patient’s admission assessment. What anatomical location should the nurse expect to assess this cyst? a. Rectum b. Sacrococcygeal area c. Abdomen d. Anus ANS: B A pilonidal cyst is located in the sacrococcygeal area. DIF: Cognitive Level: Knowledge REF: p. 762 OBJ: 3 TOP: Pilonidal Cyst KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. A home health nurse is instructing an older adult patient regarding dietary changes to help prevent constipation. What changes should the nurse indicate when providing this education? (Select all that apply.) a. Addition of whole-grain cereal b. Cessation of laxative use c. Increase in liquid intake d. Increase in sugar intake e. Eating fresh vegetables ANS: A, B, C, E A decrease in sugar intake will help stem diarrhea. DIF: Cognitive Level: Comprehension REF: p. 745 OBJ: 3 | 4 TOP: Nutrition to Avoid Constipation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 40: Liver, Gallbladder, and Pancreatic Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. For which complication should a nurse be careful to monitor a patient after a liver biopsy? a. Headache b. Muscle cramps c. Bleeding d. Respiratory distress ANS: C Liver biopsy places the patient at risk for hemorrhage. Liver disorders make patients especially vulnerable to hemorrhage. DIF: Cognitive Level: Comprehension REF: p. 772 OBJ: 1 TOP: Liver Biopsy KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. What is pruritus related to in the patient diagnosed with hepatitis? a. Decreased fat intake b. Poor appetite and therefore poor protein intake c. Accumulation of bile salts under the skin d. Altered urinary output of bile ANS: C Bile salts accumulate under the skin, causing irritation. DIF: Cognitive Level: Comprehension REF: p. 771 OBJ: 1 TOP: Hepatitis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A young woman with severe jaundice has an altered body image. The patient says, “Will I always be this horrible color?” What is the best response by the nurse? a. “Yes, but your sclera will return to their previous white color.” b. “No. The color will fade gradually as liver inflammation decreases.” c. “Yes, but cosmetics can disguise the color.” d. “No. The color will change to freckles.” ANS: B Jaundice causes patients to be self-conscious and reclusive because of the change in physical appearance. Patients can be reassured that the color improves as liver function improves, usually in 2 to 4 weeks. DIF: Cognitive Level: Comprehension REF: p. 767 OBJ: 1 TOP: Hepatitis and Jaundice KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 4. What action should a nurse implement to prevent complications in a patient with hepatitis who has been prescribed bed rest? a. Raise the knee gatch to prevent the patient from sliding down in bed. b. Provide undisturbed periods of 6 hours to encourage rest. c. Restrict fluids. d. Encourage turning, coughing, and deep breathing every 2 hours. ANS: D The nurse must encourage measures that will prevent pneumonia and improve impaired skin integrity because of the increased risk factors associated with bed rest. DIF: Cognitive Level: Application REF: p. 777 OBJ: 2 TOP: Bedrest for Hepatitis KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. Which sign indicates that the need for increased fluid intake would be contraindicated in a patient diagnosed with a hepatic disorder? a. Low blood pressure b. Increased urinary output c. Signs of edema d. Bradycardia ANS: C Edema may indicate fluid overload; therefore, question the intake, as well as electrolyte and cardiac status. DIF: Cognitive Level: Comprehension REF: p. 769 OBJ: 2 TOP: Fluid Volume and Hepatitis KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. What intervention should a nurse implement when assessing a patient with jaundice who has been given the nursing diagnosis of disrupted skin integrity? a. Sedate the patient. b. Apply mittens or socks to the hands. c. Restrain the hands. d. Distract the patient with conversation. ANS: B Jaundice causes itching, which can cause the patient to scratch and create a break in the skin. Mittens provide some comfort without causing further skin impairment. DIF: Cognitive Level: Application REF: p. 769 OBJ: 1 TOP: Jaundice KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. Which vaccination does the Occupational Health and Safety Administration (OSHA) require all health care providers to receive? a. Hepatitis A b. Hepatitis B c. Hepatitis C d. All strains of hepatitis ANS: B OSHA requires that all health care providers be vaccinated against hepatitis B. DIF: Cognitive Level: Knowledge REF: p. 765 OBJ: 2 TOP: OSHA Requirements KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 8. What is the meaning of a dropping bilirubin level in a patient diagnosed with hepatitis? a. Red blood cell destruction is decreasing. b. Liver function is improving. c. Kidneys are compensating for liver dysfunction. d. Kupffer cell damage is continuing. ANS: B As liver function improves, the bilirubin level will decrease because of the liver’s ability to conjugate and excrete the bilirubin. The flow of bile out of the liver increases. DIF: Cognitive Level: Comprehension REF: p. 765 OBJ: 1 TOP: Liver Disease KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. A goal of medical treatment for patients with cirrhosis is to prevent complications and limit cell damage. A major approach is to promote rest. What rationale supports this approach? a. Allows time for a transplant b. Allows the liver to regenerate c. Prevents red cell destruction d. Decreases the risk of trauma ANS: B With rest, the liver will regenerate healthy tissue and return to normal functioning. Rest must include other measures to promote healing, such as dietary measures and no alcohol. DIF: Cognitive Level: Comprehension REF: p. 768 OBJ: 1 TOP: Cirrhosis KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. What is necessary to restrict when the ammonia level of a patient diagnosed with cirrhosis continues to rise? a. Protein b. Carbohydrates c. Fats d. Water-soluble vitamins ANS: A Ammonia is the waste product of protein breakdown. Decreasing protein intake will decrease the end product. DIF: Cognitive Level: Comprehension REF: p. 771 OBJ: 1 TOP: Cirrhosis KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. What actions should a nurse implement to correctly assess the progress of ascites on a daily basis? a. Daily weights and abdominal girth measurements b. Intake-output and electrolyte levels c. Blood pressure and pulse d. Daily temperatures and oxygen levels ANS: A Daily weights and abdominal girth measurements will accurately measure the fluid accumulating in the peritoneal cavity. DIF: Cognitive Level: Application REF: p. 773 OBJ: 1 TOP: Ascites KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. A patient with ascites is scheduled for a LeVeen peritoneal-venous shunt. The patient asks why this needs to be done instead of a paracentesis. What is the best response by the nurse? a. “It helps the kidneys retain needed sodium.” b. “It will decrease the need for analgesics.” c. “This procedure will prevent the loss of protein.” d. “The risk of infection is lessened with this procedure.” ANS: C Fluids containing protein are returned to the vascular compartment to retain important elements such as albumin. The retention of albumin reduces fluid accumulation. DIF: Cognitive Level: Comprehension REF: p. 773 OBJ: 1 TOP: Ascites KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. A high ammonia level contributes to hepatic encephalopathy. Which nursing implementation needs to be added to the nursing care plan as this level continues to increase? a. Mouth care b. Increased frequency of neurologic checks c. Oxygen saturation monitoring d. Intake and output ANS: B As the ammonia level rises, the patient becomes at greater risk for confusion and hepatic coma related to encephalopathy. DIF: Cognitive Level: Comprehension REF: p. 772 OBJ: 2 TOP: Seizure Precautions KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 14. A nurse is educating a patient diagnosed with hepatitis A. What should the nurse instruct this patient to avoid sharing? a. Food b. Bodies c. Needles d. Housing ANS: A Hepatitis A is spread from contact with saliva, which can be transmitted by shared food or drinks. DIF: Cognitive Level: Comprehension REF: p. 765 OBJ: 1 TOP: Hepatitis A KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 15. Which dietary selection should lead the nurse to conclude that the dietary teaching is successful for a patient on a low-sodium diet? a. Bologna sandwich with tomato juice b. Hotdog on a bun with pickle relish and skim milk c. Baked chicken, white rice, and apple juice d. Peanut butter and jelly sandwich with tomato soup ANS: C A meal of baked chicken, white rice, and apple juice has the lowest sodium levels. DIF: Cognitive Level: Comprehension REF: p. 768 OBJ: 2 TOP: Nutrition: Low-Sodium Diet KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. Which nursing measure takes priority in relation to the care of a patient with a gastroesophageal balloon tube? a. Deflate the balloon periodically. b. Advance the tube as instructed. c. Monitor respiratory status. d. Withhold medications that could decrease restlessness. ANS: C Because of the close proximity of the esophagus and trachea, any upward movement of the tube could cause airway obstruction. DIF: Cognitive Level: Application REF: p. 776 OBJ: 1 TOP: Esophageal Balloon KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 17. Which instruction should be given to a patient with portal hypertension to reduce the threat of hemorrhage? a. Eat bland foods. b. Avoid straining to have a bowel movement. c. Increase fluid intake. d. Use an electric razor to shave. ANS: B Straining can increase pressure and may cause the dilated vessels in the gastrointestinal tract to bleed. Shaving with an electric razor does not prevent serious bleeding. DIF: Cognitive Level: Comprehension REF: p. 772 OBJ: 1 TOP: Portal Hypertension KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 18. What precaution should a nurse initiate when caring for a patient with hepatitis B? a. Reverse isolation b. Standard Precautions c. Respiratory precautions d. Enteric precautions ANS: B Standard Precautions protect the nurse from organisms that may be in all body fluids. DIF: Cognitive Level: Comprehension REF: p. 765 OBJ: 1 TOP: Hepatitis B KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 19. A patient was positive for hepatitis B virus, although she had the disease 4 years ago and now is symptom free. What is the nurse aware is true regarding this patient? a. Is likely to have hepatitis B again b. Now has noninfectious hepatitis c. Is an infectious carrier and always will be d. Is at risk for hepatitis E ANS: C A certain percentage of persons who have had hepatitis B convert to carriers. They have the live virus, which causes no symptoms in them, but they are able to transmit the disease and always will be infectious. DIF: Cognitive Level: Comprehension REF: p. 766 OBJ: 2 TOP: Carrier State for Hepatitis B KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 20. A patient in acute pain is admitted with pancreatitis. A nurse reviews a laboratory report showing an elevation that is diagnostic for acute pancreatitis. Which laboratory report did the nurse most likely review? a. Serum bilirubin b. Serum calcium c. Serum lipids d. Serum amylase ANS: D Serum amylase is the most significant of the diagnostic findings. DIF: Cognitive Level: Knowledge REF: p. 783 OBJ: 1 TOP: Pancreatitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 21. What is the highest nursing priority outcome when planning the care for the patient with pancreatitis? a. Patient claims satisfaction with pain control. b. Patient states an understanding of medications needed on discharge. c. Patient’s activity level tolerance shows an increase. d. Patient can maintain a normal bowel pattern. ANS: A Pain control is the most important priority. DIF: Cognitive Level: Analysis REF: p. 783 OBJ: 1 TOP: Pancreatitis KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 22. What should a nurse often find in the medical history of a patient diagnosed with pancreatic disease? a. Liver disorders b. Drug abuse c. Alcohol abuse d. Excessive sugar intake ANS: C Pancreatic disease is often related to alcohol abuse. DIF: Cognitive Level: Comprehension REF: p. 783 OBJ: 1 TOP: Pancreatic Disease KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 23. Which observation by a nurse would indicate blocked flow of bile from the liver to the intestine? a. Clay-colored stools b. Jaundice c. High blood pressure d. Tachycardia ANS: A Bile is unable to get to feces to give it the normal brown color. DIF: Cognitive Level: Comprehension REF: p. 767 OBJ: 1 TOP: Biliary Disease KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 24. Which chronic condition is related to the presence of chronic pancreatitis? a. Chronic obstructive pulmonary disease (COPD) b. Urinary tract infection (UTI) c. Diabetes mellitus (DM) d. Arteriosclerotic heart disease (ASD) ANS: C Patients with chronic pancreatitis are at risk for developing DM because of the destruction of the insulin-secreting cells in the pancreas. DIF: Cognitive Level: Knowledge REF: p. 783 OBJ: 2 TOP: Chronic Pancreatitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 25. Which risk is significantly increased in patients diagnosed with liver disease? a. Urinary infections b. Systemic infection c. Drug toxicity d. Drug allergy ANS: C Because many drugs are metabolized in the liver and a diseased liver does not adequately clear the system of drugs, drug toxicity is an ongoing problem. DIF: Cognitive Level: Comprehension REF: p. 777 OBJ: 1 TOP: Risk for Drug Toxicity KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 26. What should a nurse include in the discharge teaching for a patient after a laparoscopic procedure for cholelithiasis? a. Take water-soluble vitamins. b. Follow a low-fat diet. c. Expect light-colored stools for several days. d. Keep dressing over the T-tube dry. ANS: B After the laparoscopic procedure, the patient is to follow a low-fat diet and take fat-soluble vitamins. Placement of the T-tube is not done with the laparoscopic procedure. DIF: Cognitive Level: Application REF: p. 778 OBJ: 1 TOP: Laparoscopic Procedure for Cholelithiasis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort COMPLETION 1. A nurse reminds a patient with liver disease that the level of in the blood is an indicator of the how well the liver is functioning. ANS: bilirubin The level of indirect bilirubin indicates the effectiveness of the metabolism of proteins by the liver. DIF: Cognitive Level: Knowledge REF: p. 771 OBJ: 1 TOP: Bilirubin as an Indicator of Liver Function KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. In assessing a dark-skinned patient for jaundice, the nurse would assess the for a yellow color. ANS: sclera Jaundice can be assessed by the yellow pigment on the sclera of a dark-skinned person. DIF: Cognitive Level: Application REF: p. 790 OBJ: 1 TOP: Assessing Jaundice in Dark-Skinned Persons KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 41: Urologic System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is assessing a patient with renal impairment. Which facial characteristic is a sign of fluid retention? a. Broken blood vessels around the nose b. Periorbital edema c. Rash on cheeks and neck d. Facial twitching ANS: B Periorbital edema is a sign of fluid retention. Because the patient with renal impairment has generalized edema, this facial feature is extremely significant in assessing edema. DIF: Cognitive Level: Comprehension REF: p. 798 OBJ: 1 TOP: Sign of Fluid Retention KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. What laboratory value change should indicate to a nurse that a patient with renal failure has entered the oliguric stage? a. Blood urea nitrogen (BUN) level rises. b. Serum calcium increases. c. Blood volume decreases. d. Urine osmolality increases. ANS: A In the oliguric stage of renal failure, the urine output decreases to less than 400 mL/day; the BUN, creatinine, and potassium increase; and the serum calcium decreases. The patient becomes hypervolemic as the urine osmolality increases. DIF: Cognitive Level: Comprehension REF: p. 799 OBJ: 1 TOP: Oliguric Stage of Renal Failure KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. What should nursing care focus on when caring for a patient with a ureteral catheter in place after the removal of a kidney stone? a. Irrigating the catheter regularly b. Assessing for patency c. Including ureteral output with the bladder output d. Early ambulation ANS: B Patency of the ureteral catheter is essential to prevent injury to the kidney. The patient is on bed rest until the ureteral catheter is removed. The output from the ureteral catheter is measured and recorded separately, and irrigation, if performed, is not done on a regular schedule and is not more than 5 mL. DIF: Cognitive Level: Application REF: p. 806 OBJ: 2 TOP: Ureteral Catheter KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. What is true about the urine osmolality when the kidney is adequately functioning? a. Equal to the osmolality of the serum b. Approximately half of the serum c. In a ratio of 10:1 with the serum d. Equal to the excretion of urea ANS: A If the blood osmolality is high, the kidneys need to dilute the blood and excrete more concentrated urine, and the reverse is true. The osmolality of the serum and the urine should be equal. DIF: Cognitive Level: Comprehension REF: p. 803 OBJ: 2 TOP: Kidney Function Tests KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. Which urine test provides the most accurate measurement of renal function? a. BUN b. Phosphates c. Specific gravity d. Creatinine ANS: D Creatinine is not affected by diet, hydration, or liver function and is a better measurement of liver function than the BUN. DIF: Cognitive Level: Knowledge REF: p. 803 OBJ: 2 TOP: Creatinine KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 6. A nurse is caring for a patient after urinary diversion surgery. What postoperative nursing assessment is the priority? a. Level of fluid intake b. Position on the left side c. Keep the bed flat d. Bowel sounds ANS: D The bowel is manipulated during urinary diversion surgeries and frequently leads to the patient with a paralytic ileus. DIF: Cognitive Level: Application REF: p. 806 OBJ: 4 TOP: Urinary Diversion KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. A nurse is performing frequent catheterizations for residual urine. What causes the greatest concern for the nurse? a. Introduction of pathogens into the bladder b. Frequent genital exposure of the patient c. Presence of the indwelling catheter d. Causing urethral erosion ANS: A The frequency of introducing a catheter into the bladder offers a very real risk of infection. DIF: Cognitive Level: Application REF: p. 805 OBJ: 4 TOP: Urinary Catheterization KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 8. A patient has a nephrostomy tube that has been inserted because of an obstruction in the ureter. What special precautions in the care of the nephrostomy tube should the nurse implement? a. Clamping every 2 hours to allow expansion of the kidney pelvis b. Instilling no more than 50 mL of sterile water if sterile irrigations are ordered c. Being certain the tube is connected, not kinked, or not clamped to ensure that it continually drains d. Leaving the nephrostomy site open to air ANS: C Because of the small capacity of the renal pelvis, drainage must be continuous; otherwise, the urine may back up and destroy the kidney. DIF: Cognitive Level: Application REF: p. 806 OBJ: 2 TOP: Nephrostomy Tube KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. Which statement by a patient on dialysis, taking gentamicin (Garamycin), should cause the nurse the most concern? a. “I have a horrible headache.” b. “Speak up! I can’t hear you.” c. “I’ve had diarrhea once or twice today.” d. “I’m thirsty. I can’t get enough water.” ANS: B Garamycin is ototoxic. Indication of hearing impairment suggests drug toxicity. DIF: Cognitive Level: Comprehension REF: p. 809 OBJ: 2 TOP: Garamycin KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 10. Erythropoietin is a hormone produced by the kidney. What will a deficiency of erythropoietin in a patient in chronic renal failure result in? a. Diminished immunologic function with fewer white blood cells b. Elevated lipid levels in the bloodstream, contributing to accelerated atherosclerosis c. Anemia as a result of the diminished number of red blood cells being produced d. Hypertension as a result of the increased, concentrated blood volume ANS: C Erythropoietin is excreted by the kidneys and stimulates bone marrow to produce red blood cells. DIF: Cognitive Level: Comprehension REF: p. 797 OBJ: 1 TOP: Erythropoietin KEY: Nursing Process Step: N/A MSC: NCLEX: N/A MULTIPLE RESPONSE 1. A nurse is planning the care for an older adult patient. Which age-related changes in kidney function should the nurse consider when providing care to this patient? (Select all that apply.) a. Thinning of nephron membranes b. Sclerosis of renal blood vessels c. Decreasing glomerular filtrations d. Decreasing ability to concentrate or dilute urine e. Decreasing erythropoietin ANS: B, C, D, E Sclerosis of renal blood vessels, decreasing glomerular filtration, decreasing ability to concentrate urine, and decreasing erythropoietin are associated with aging. DIF: Cognitive Level: Knowledge REF: p. 797 OBJ: 1 TOP: Age-Related Changes to the Kidney KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse is caring for a patient with a Foley catheter. What actions should the nurse implement to decrease this patient’s risk for infection? (Select all that apply.) a. Keep the bag below the level of the bed. b. Provide perineal care twice a day. c. Flush the tubing as needed. d. Use Standard Precautions when handling urine and tubing. e. Keep the drainage system open. ANS: A, B, D Keeping the bag below the level of the bed, providing perineal care twice daily, and using Standard Precautions will assist in decreasing infection risk. Tubing is only flushed with a physician’s order if required. The drainage system should be closed. DIF: Cognitive Level: Application REF: p. 805 OBJ: 4 TOP: Foley Catheter KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance 3. A nurse reads the serum calcium laboratory report of a patient as 4.2 mEq/L. Which symptoms should the nurse anticipate that the patient might exhibit? (Select all that apply.) a. Irritability b. Tingling sensations in limbs c. Tetany d. Nausea e. Visual disturbances ANS: A, B, C Symptoms of hypocalcemia include irritability, tingling sensations, tetany, muscle twitching, and muscle contractions. DIF: Cognitive Level: Comprehension REF: p. 808 OBJ: 1 TOP: Hypocalcemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 42: Urologic Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient comes to the medical clinic with complaints of urgency, frequency, pain in the area of the symphysis pubis, and dark cloudy urine. What should the nurse suspect that this patient has? a. Urinary calculi, probably located in the ureter b. Kidney infection, most likely pyelonephritis c. Cystitis, probably from bacterial contamination d. Interstitial cystitis (although rare in a male patient) ANS: C Cystitis causes urgency, dysuria, and pain behind the symphysis pubis. Cystitis is usually caused by bacterial infection. DIF: Cognitive Level: Analysis REF: p. 813 OBJ: 1 TOP: Urinary Tract Infection KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A patient who has cystitis has been told to drink at least 30 mL for each kilogram of body weight. Her weight is 154 lb. How many mL/day should the nurse instruct the patient to drink? a. 1500 b. 2100 c. 2700 d. 3100 ANS: B 154 lb ÷ 2.2 lb/kg = 70 kg; 70 kg 30 mL = 2100 mL. DIF: Cognitive Level: Analysis REF: pp. 813-814 OBJ: 1 TOP: Cystitis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A home health patient diagnosed with cystitis has been prescribed the medication phenazopyridine (Pyridium). When providing patient teaching, what should the nurse caution the patient about? a. Staying out of the heat b. Nausea c. Staining of clothing d. Skin rash ANS: C Pyridium causes the urine to be a bright orange color, which can stain clothing. DIF: Cognitive Level: Comprehension REF: p. 814 OBJ: 2 TOP: Urinary Drugs KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 4. A nurse is collecting data from a hospital patient who has been admitted with pyelonephritis. He is acutely ill with a high fever, chills, nausea, and vomiting. He also has severe pain in the flank area. What is the primary goal of treatment? a. Provide adequate nutrition with a stable body weight. b. Provide adequate hydration with pulse and blood pressure within patient norms. c. Give pain relief with analgesics and antispasmodics. d. Prevent further damage to his kidneys that could lead to renal failure. ANS: D Pyelonephritis can cause scarring of the renal parenchyma and result in atrophy of the affected kidney, which means the kidney is failing. DIF: Cognitive Level: Application REF: p. 815 OBJ: 2 TOP: Pyelonephritis KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. What is the usual cause of the autoimmune disease of acute glomerulonephritis? a. Frequent cystitis b. Streptococcal infection c. Childhood disease of mumps d. Recent wound infection ANS: B The cause is an upper respiratory infection caused by a beta-hemolytic Streptococcus. DIF: Cognitive Level: Comprehension REF: p. 816 OBJ: 1 TOP: Acute Glomerulonephritis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A nurse is caring for a patient with acute glomerulonephritis. What should the nurse be aware that the inflammation of the capillary loops in the glomeruli will lead to? a. Moderate to high blood pressure b. Low blood volume with polyuria c. Irritability and hyperactivity d. Low levels of BUN and creatinine ANS: A The inflammatory process in the glomeruli decreases the filtration rate, and the blood volume increases, raising the patient’s blood pressure. DIF: Cognitive Level: Comprehension REF: p. 816 OBJ: 1 TOP: Acute Glomerulonephritis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A 16-year-old patient with acute glomerulonephritis complains of boredom with bed rest and asks when he can become more active. He asks, “What has to happen for me to get off of bed rest?” What is the most accurate statement by the nurse? a. Dialysis starts. b. The antibiotic protocol is completed. c. Potassium levels are normal. d. Blood pressure drops to normal levels. ANS: D Bed rest, when ordered, is for the protection of the patient because of high blood pressure. Bed rest will continue until the treatment causes diuresis and a drop in the blood pressure. DIF: Cognitive Level: Application REF: p. 817 OBJ: 2 TOP: Glomerulonephritis with Bed Rest KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Physiological Adaptation 8. What discharge teaching is appropriate for the nurse to provide to a patient who has had a lithotripsy? a. Check for edema of the legs and ankles. b. Watch for stone debris in the urine in 1 to 4 weeks. c. Decrease fluid intake to 1000 mL/day. d. Remain on restricted activity for a week. ANS: B The stones that have shattered with the sound waves will show up as debris in 1 to 4 weeks. Fluid intake is encouraged, and activity is resumed the next day. Edema is not a concern. DIF: Cognitive Level: Application REF: p. 819 OBJ: 1 TOP: Extracorporeal Shock Wave Lithotripsy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. Which outcome is most necessary for a patient diagnosed with renal calculi? a. Patient states an awareness of signs and symptoms of kidney stones and knows where to find pain relief. b. Patient will measure intake and output so that they will be approximately equal. c. Patient will avoid infections and situations that would increase stress. d. Patient is able to describe measures to prevent recurrence of calculi. ANS: D Recurrence of renal calculi is common. The patient needs to possess the information necessary to understand the formation of stones to reduce the risk of their recurrence. DIF: Cognitive Level: Application REF: p. 821 OBJ: 2 TOP: Renal Calculi KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 10. A nurse is caring for a patient with an atrioventricular (AV) fistula in the forearm and assesses that a trill is absent when palpating the venous side of the fistula. What action should the nurse implement? a. Inject the ordered amount of heparin into the fistula. b. Apply warm compresses and lower the arm below the heart level. c. Send the patient to dialysis for remedy. d. Report to the charge nurse that the fistula is occluded. ANS: D If the trill is absent, the fistula is occluded and should be reported. Dialysis is not possible with the occlusion. Injecting the shunt is not in the scope of practice of the licensed practical nurse (LPN). Warm compresses are not helpful. DIF: Cognitive Level: Application REF: p. 834 OBJ: 1 TOP: Occluded Fistula KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. A patient on dialysis asks why he is receiving aluminum hydroxide gel (Amphojel), a phosphate binder, for his renal disorder. What should the nurse explain regarding the action of that Amphojel? a. Calms the frequent upset stomach experienced by patients on dialysis b. Binds with phosphorus to increase the serum calcium level c. Increases the appetite d. Corrects the pH of the bowel ANS: B Amphojel binds phosphorus, which increases the serum calcium level and decreases hypocalcemia. DIF: Cognitive Level: Comprehension REF: p. 832 OBJ: 1 TOP: Use of Aluminum Hydroxide Gel in Patients on Dialysis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. Which statement by a patient on dialysis, taking gentamicin (Garamycin), should cause the nurse the most concern? a. “I have a horrible headache.” b. “Speak up! I can’t hear you.” c. “I’ve had diarrhea once or twice today.” d. “I’m thirsty. I can’t get enough water.” ANS: B Garamycin is ototoxic. Indication of hearing impairment suggests drug toxicity. DIF: Cognitive Level: Comprehension REF: p. 809 OBJ: 2 TOP: Garamycin KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 13. A family member of a patient who has returned to the special unit after renal transplantation is alarmed by blood in the urine of the patient. What is the nurse’s best explanation when explaining the reason for hematuria in this patient? a. “It is related to the immunosuppressant drugs taken before transplantation.” b. “It is a normal postoperative expectation.” c. “It is caused by dye injected during surgery.” d. “It is caused by a small vessel that may be bleeding but will coagulate as urine flow increases.” ANS: B Blood in the urine is an expected postoperative expectation and will gradually clear up. DIF: Cognitive Level: Comprehension REF: p. 823 OBJ: 1 TOP: Postoperative Care for Transplant Recipients KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A 10-year-old boy tells a nurse that he wants to give his kidney to his grandfather. How many years of age should the nurse explain that kidney donors must be? a. At least 14 years old b. At least 16 years old c. At least 18 years old d. At least 21 years old ANS: C The donor must be at least 18 years old, have no systemic disease, and have normal renal function. DIF: Cognitive Level: Knowledge REF: p. 839 OBJ: 1 TOP: Kidney Donor KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 15. A patient with chronic renal failure is to begin renal dialysis treatment and asks for advice about which type of dialysis would be best. The patient is considering peritoneal dialysis because it is less expensive and has fewer dietary and fluid restrictions. What is the most accurate information for the nurse to provide about peritoneal dialysis? a. It has literally no drawbacks. b. It gives more independence and more closely resembles normal kidney function. c. It is a lot more work than hemodialysis, in which the health care staff takes care of everything. d. It usually does not work very well and has many complications, such as a high blood sugar level. ANS: B Peritoneal dialysis increases independence and resembles normal kidney function. It can be performed in any hospital or at home. DIF: Cognitive Level: Comprehension REF: p. 834 OBJ: 1 TOP: Peritoneal Dialysis KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. Why are patients diagnosed with chronic renal failure and on dialysis prone to injury? a. Bone demineralization and peripheral neuropathy b. Fatigue and drug side effects c. Impaired immune response and malnutrition d. Multiple life changes and hormone deficiencies ANS: A Loss of calcium from the bones leaves them weak, and the lack of sensation in the hands and feet leaves patients with a lack of proprioception. Realizing these factors, the nurse can draw up implementations to help prevent injuries. DIF: Cognitive Level: Knowledge REF: p. 831 OBJ: 2 TOP: Chronic Renal FailureKEY: Nursing Process Step: Nursing Diagnosis MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 17. A nurse assesses a Grey Turner sign in a patient who was admitted 2 days earlier after an automobile accident. What does this finding indicate? a. Retroperitoneal bleeding and bruising over the flank b. Hematuria with abdominal bruising c. Distended bladder with painful urination d. Bladder spasms on palpation of abdomen ANS: A The Grey Turner sign is bruising over the flank and retroperitoneal bleeding. This is observed in blunt trauma to the kidney. DIF: Cognitive Level: Comprehension REF: p. 823 OBJ: 1 TOP: Grey Turner Sign KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. A female patient reports very painful urethritis. What should the home health care nurse question the patient about the use of? (Select all that apply.) a. Bubble bath b. Vitamin preparations c. Herbal remedies d. Vaginal sprays e. Exercise machines ANS: A, D Bath additives and vaginal sprays are causative for urethritis. Vitamins, herbal preparations, and exercise machinery are noncontributory. DIF: Cognitive Level: Comprehension REF: p. 812 OBJ: 1 TOP: Urethritis KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control COMPLETION 1. The major risk of peritoneal dialysis is . ANS: peritonitis Peritonitis is the major risk of peritoneal dialysis. DIF: Cognitive Level: Comprehension REF: p. 834 OBJ: 1 TOP: Risk of Peritoneal Dialysis KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. A nurse is aware that if a ureter is blocked by a kidney stone, the urine backs up into the kidney, causing . ANS: hydronephrosis Hydronephrosis results when a ureter is obstructed and urine backs up into the pelvis of the kidney. If unrelieved, this condition will require the removal of the kidney. DIF: Cognitive Level: Comprehension REF: p. 820 OBJ: 1 TOP: Topic: Hydronephrosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 43: Musculoskeletal System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is collecting a health history from a patient with a connective tissue disease. What is the most important inquiry by the nurse? a. Family history of atherosclerosis b. Last time the patient had his or her blood tested c. History of a prior injury to a specific body part d. Family history of a fracture ANS: C Previous injuries may be relevant to a patient’s current problem. DIF: Cognitive Level: Comprehension REF: p. 847 OBJ: 2 TOP: Connective Tissue Disease Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse is educating an osteoporotic patient taking alendronate (Fosamax). Which instruction should the nurse stress? a. Take the drug after breakfast. b. Avoid the use of supplemental vitamin D. c. Decrease fluid intake. d. Sit or stand for 30 minutes after administration. ANS: D After taking the drug Fosamax with 8 oz of fluid, the patient should sit or stand for 30 minutes so the drug will be evenly distributed. The drug is taken on an empty stomach. DIF: Cognitive Level: Application REF: p. 856 OBJ: 4 TOP: Fosamax KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. Which diagnostic test result should the nurse expect for a patient with polymyositis? a. Muscle biopsy positive for muscle degeneration b. Positive antinuclear antibody (ANA) blood test result c. Positive 24-hour urine test result for urate crystals d. Urate crystals in the synovial fluid ANS: A A biopsy, positive for muscle degeneration, is the only result that pertains to polymyositis. DIF: Cognitive Level: Comprehension REF: p. 851 OBJ: 3 TOP: Polymyositis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A nurse is educating a patient with gout about the medication probenecid (Benemid). What active effect should the nurse relay when explaining why this medication is prescribed? a. Reduces inflammation in the affected joint b. Relieves pain c. Diminishes swelling d. Increases excretion of uric acid ANS: D Probenecid (Benemid) increases the excretion of uric acid to reduce the symptoms of gout. DIF: Cognitive Level: Comprehension REF: p. 855 OBJ: 4 TOP: Probenecid KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 5. The physician orders antinuclear antibodies for a patient with suspected rheumatoid arthritis. What information will the nurse provide to the patient in preparation for this study? a. Fast for 8 hours before test. b. Refrain from exercise the day before test. c. Do not take medications 24 hours before test. d. Void prior to test. ANS: A Patients should be instructed to fast for 8 hours before antinuclear antibodies. DIF: Cognitive Level: Application REF: p. 849 OBJ: 3 TOP: Antinuclear antibodies KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. A patient is preparing for tomography as ordered to enhance visualization of tissue hidden by bone. What assessment by the nurse should be immediately addressed? a. History of recent urinary tract infection b. Allergy to Sulfa c. Reports of claustrophobia d. Diagnosis of bipolar disorder ANS: C Tomography requires lying in a cylindric scanner. The nurse should assess for claustrophobia and inform the radiologist. DIF: Cognitive Level: Analysis REF: p. 850 OBJ: 3 TOP: Tomography KEY: Nursing Process Step: Implementation MSC: NCLEX:: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. A nurse questions an older patient about the age-related changes she has experienced in her connective tissue, which have lessened her mobility. What do these changes most commonly include? (Select all that apply.) a. Loss of bone mass, which may cause fragile bones b. Decline in muscle mass, causing loss of strength c. Bony deposits in the joints, causing pain and altered movement d. Loss of cartilage, causing more friction in joints e. Diminished energy, causing decreased activity ANS: A, B, C, D Reduced energy, although observed in older adults, is not caused by a change in connective tissue. DIF: Cognitive Level: Comprehension REF: p. 846 OBJ: 1 TOP: Age-Related Changes in Connective Tissue KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. Immobility reduces muscle contractions and can produce muscle . ANS: atrophy Immobility reduces muscle contractions and can produce muscle atrophy. DIF: Cognitive Level: Comprehension REF: p. 845 OBJ: 1 TOP: Immobility KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A(n) measures the range of movement of the joints. ANS: goniometer A goniometer measures the range of movement of the joints. DIF: Cognitive Level: Knowledge REF: p. 847 OBJ: 2 TOP: Joint Motion KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. uses sound waves to determine the presence of pulses in the extremities. ANS: Doppler ultrasound Doppler ultrasound uses sound waves to determine the presence of pulses in the extremities. DIF: Cognitive Level: Comprehension REF: p. 848 OBJ: 2 TOP: Diagnostic Tests KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 44: Connective Tissue Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A 51-year-old professional tennis instructor is newly diagnosed with osteoarthritis. What is the nurse’s best explanation to the patient when asked what this diagnosis means? a. Presence of antibodies in the synovial fluid b. Dislocation of the patella over the tibia c. Degeneration of articular cartilage d. Body’s autoimmune response ANS: C Degeneration of articular cartilage is one of the pathophysiologic changes of arthritis. DIF: Cognitive Level: Knowledge REF: p. 857 OBJ: 2 TOP: Osteoarthritis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse explains to a patient with rheumatoid arthritis that the drug leflunomide (Arava) is a disease-modifying antirheumatic drug (DMARD). What is the action of this medication? a. Retards the progress of the disease b. Builds new bone c. Decreases inflammation d. Increases flexibility ANS: A Arava is a DMARD and slows the progression of the disease. DIF: Cognitive Level: Knowledge REF: p. 865 OBJ: 2 TOP: DMARDs KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. A nurse is caring for a patient with osteoarthritis. What is the best recommendation by the nurse to this patient to control chronic pain? a. Administer analgesics only when needed. b. Administer analgesics as prescribed on a routine basis. c. Plan activities with no rest periods to complete the activities quickly. d. Wear high-heeled shoes to keep the body in alignment. ANS: B The routine administration of prescribed analgesic medications is the most appropriate treatment for chronic pain. DIF: Cognitive Level: Application REF: p. 869 OBJ: 2 TOP: Osteoarthritis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 4. An older patient with osteoarthritis complains of stomach discomfort and shortness of breath after years of taking aspirin for pain relief. What change in pain control medication would be most appropriate for the home health care nurse to suggest? a. Nonsteroidal anti-inflammatory drugs (NSAIDs) b. Oral corticosteroids c. Mild exercise d. Warm baths ANS: A The use of NSAIDs is less irritating than aspirin or glucocorticoids. Mild exercise is good but not for pain relief. DIF: Cognitive Level: Application REF: p. 867 OBJ: 2 TOP: Drug Therapy for Connective Tissue Disorders KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 5. A home health care nurse is visiting a patient after a total hip replacement. What should the nurse include when teaching the patient how to protect the new joint? a. Put an extension on the toilet seat. b. Keep the legs crossed when at rest. c. Frequently change positions from side to side. d. Slowly pull the knee to the chest twice a day to stretch the hip abductors. ANS: A Placing an extender on the toilet seat will assist in the objective of not flexing the hip more than 90 degrees. Crossing the legs adducts the hip, which is contraindicated. DIF: Cognitive Level: Comprehension REF: p. 862 OBJ: 2 TOP: Total Hip Replacement and Nursing Implementations KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. After a knee replacement, an 87-year-old patient rejects the use of the continuous passive motion (CPM) machine, saying, “I did not march when I was a child, and I am not marching now.” What benefits of CPM should the nurse point out to encourage patient use? a. Decrease in pain b. Increase in circulation in the new joint c. Increase in leg strength d. Increase in flexibility for the new joint ANS: D The CPM machine’s major benefit is to increase flexibility, although it does cause discomfort. No strength-building potential is present with passive motion. DIF: Cognitive Level: Application REF: p. 863 OBJ: 2 TOP: Total Hip Replacement KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. What do connective tissue diseases affect? a. Bones, ligaments, cartilage, and tendons b. Bones, ligaments, and tendons c. Spurs, ligaments, cartilage, and tendons d. Tendons, cartilage, and tophi ANS: A Connective tissue diseases affect bones, ligaments, cartilage, and tendons. DIF: Cognitive Level: Knowledge REF: p. 857 OBJ: 1 TOP: Connective Tissue Disease KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. Which patient is most likely to develop a connective tissue disease? a. A teenage girl who swims b. A 30-year-old woman who plays tennis c. A 35-year-old male golfer d. A 40-year-old male computer analyst ANS: B Women have a greater chance than men of developing connective tissue disease. DIF: Cognitive Level: Comprehension REF: p. 868 OBJ: 1 TOP: Connective Tissue Disease KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. Which is true regarding connective tissue function? a. Helps provide a source of storage for calcium b. Stores hormones in the pores of bone tissue c. Controls the distribution of minerals d. Provides protection to body parts ANS: D Providing protection is a function of connective tissue. DIF: Cognitive Level: Knowledge REF: p. 857 OBJ: 2 TOP: Connective Tissue Function KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. Which characteristic should a nurse recognize as diagnostic of rheumatoid arthritis? a. Absence of pain b. Symmetric bilateral joint swelling c. Evening stiffness that improves with activity d. Increased appetite ANS: B Symmetric bilateral joint swelling is a classic symptom of rheumatoid arthritis. DIF: Cognitive Level: Comprehension REF: p. 864 OBJ: 1 TOP: Rheumatoid Arthritis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. A patient asks why systemic glucocorticoid medications are used as the last choice for the treatment of rheumatoid arthritis. What is the nurse’s most informative reply? a. “The other drugs are just as effective and work in similar ways.” b. “They are used as a last choice or for short periods because they have many side effects.” c. “Those drugs are given three or four times daily, which is more difficult for patients to remember.” d. “A higher incidence of vomiting occurs with prolonged use.” ANS: B Glucocorticoids are used as a last choice because they have many side effects. DIF: Cognitive Level: Comprehension REF: p. 872 OBJ: 2 TOP: Drug Therapy of Rheumatoid Arthritis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. A nurse, in conjunction with a patient, establishes a plan to treat the pain associated with arthritis. What is the most effective strategy? a. Avoid exercise to spare painful joints. b. Use narcotics for pain relief. c. Apply warm, moist compresses before doing activity. d. Avoid assistive devices that encourage dependence. ANS: C Applying heat before exercise loosens the joints and decreases pain. DIF: Cognitive Level: Comprehension REF: p. 866 OBJ: 2 TOP: Arthritis KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. What is the best physiologic reason for a patient with osteoporosis to maintain a regular exercise regimen? a. Involves the patient in her or his own care b. Increases cardiac output c. Promotes better mental health d. Promotes bone formation and improves strength ANS: D Regular exercise promotes bone formation, which is important for patients with osteoporosis for physiologic reasons. DIF: Cognitive Level: Comprehension REF: p. 869 OBJ: 2 TOP: Osteoporosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A nurse is organizing a teaching plan for a patient with gout. What should the nurse caution this patient he is at an increased risk for? a. Kidney stones b. Tophi c. Visual disturbances d. Facial lesions ANS: A The threat of kidney stones is a lifelong problem for patients with gout. Tophi are symptomatic of the disease but are not a complication. Facial lesions and visual disturbances are noncontributory. DIF: Cognitive Level: Comprehension REF: p. 871 OBJ: 2 TOP: Gout Complications KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 15. A nurse is educating a patient with gout about a low-purine diet. Which food choice by the patient would indicate the need for further teaching? a. Pizza with pepperoni b. Seafood platter with scallops and mussels c. Chicken salad with nuts d. Tuna sandwich with potato chips ANS: B Seafood, such as scallops and mussels, are high in purine. DIF: Cognitive Level: Application REF: p. 872 OBJ: 2 TOP: Low-Purine Diet KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 16. A nurse is caring for a patient immediately after total knee replacement surgery. What assessment requires priority? a. Quality of pulses in the affected limb b. Degree of nausea and vomiting c. Understanding of the procedure d. Amount of pain ANS: A Assessments related to postoperative circulatory efficiency are priority assessments. DIF: Cognitive Level: Application REF: p. 863 OBJ: 3 TOP: Postoperative Care of Total Knee Replacement KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 17. Inadequate nutrition is the patient problem applicable to a patient with progressive systemic sclerosis. What is the most important point for the nurse to teach this patient? a. Eat three large meals spaced throughout the day. b. Schedule rest periods to prevent overtiring. c. Severe stress can trigger vasospasm. d. Eat smaller, more frequent meals. ANS: D Smaller, more frequent meals may be better tolerated by a patient who has esophageal involvement. DIF: Cognitive Level: Application REF: p. 873 OBJ: 2 TOP: PSS KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 18. What instruction should a nurse include in a teaching plan for a patient with carpal tunnel syndrome? a. Anticoagulants and glucocorticoids b. Methotrexate c. Lubricating ointments d. Splinting to prevent flexion and hyperextension ANS: D Resting and supporting the joint are first-line treatments. DIF: Cognitive Level: Comprehension REF: p. 875 OBJ: 2 TOP: Carpal Tunnel Syndrome KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 19. Two days after a total hip replacement, a patient is being discharged. Which statement indicates that the patient understands the discharge teaching? a. “I can sit comfortably with my legs crossed.” b. “I will ask my husband to tie my shoes for me.” c. “I am glad I won’t have to use that bulky pillow between my legs at night.” d. “My straight dining room chair will be helpful when I do the hip flexion exercises.” ANS: B If the patient bends over to tie her own shoes, her hips would have more than 90 degrees of flexion. DIF: Cognitive Level: Comprehension REF: p. 862 OBJ: 2 TOP: Hip Arthroplasty KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. What action would best benefit the patient diagnosed with bursitis of the shoulder? a. Lifting a 5-lb weight as a daily exercise b. Walking the fingers of the affected arm up the wall c. Splinting the affected arm to keep the shoulder immobile d. Performing gentle push-ups on the floor ANS: B Walking the fingers up the wall is a gentle exercise to increase range of motion. DIF: Cognitive Level: Comprehension REF: p. 875 OBJ: 3 TOP: Exercises for Bursitis KEY: Nursing Process Step: N/A MSC: NCLEX: N/A MULTIPLE RESPONSE 1. What are the goals of therapy for patients with rheumatic arthritis? (Select all that apply.) a. Decrease inflammation. b. Balance activity and rest. c. Promote adaptation to limitations. d. Plan frequent periods of bed rest. e. Supply patient education and support. ANS: A, B, C, E Bed rest of any long period increases the problems of immobility. DIF: Cognitive Level: Comprehension REF: p. 877 OBJ: 3 TOP: Goals for Therapy for Rheumatoid Arthritis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What actions would be best for patients with osteoarthritis to seek the assistance of physical therapy? (Select all that apply.) a. Isotonic exercises b. Moist heat application c. Instruction with a transcutaneous electrical nerve stimulation (TENS) unit d. Measures to increase range of motion e. Measures to increase strength ANS: B, C, D, E Isotonic exercises place increased stress on the joints. DIF: Cognitive Level: Comprehension REF: p. 858 OBJ: 3 TOP: Benefits of Physical Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. What signs of progressive systemic sclerosis does the anonym CREST represent? (Select all that apply.) a. Calcinosis b. Rash c. Esophageal dysfunction d. Sore joints e. Telangiectasis ANS: A, C, E CREST stands for calcinosis, Raynaud phenomenon, esophageal dysfunction, sclerodactyly, and telangiectasis. DIF: Cognitive Level: Knowledge REF: p. 872 OBJ: 3 TOP: CREST KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. To decrease osteoporosis, a nurse explains that women can benefit from for 15 years after the onset of menopause. ANS: estrogen A program of oral estrogen replacement therapy can decrease the occurrence of osteoporosis. DIF: Cognitive Level: Comprehension REF: p. 868 OBJ: 2 TOP: Hormone Replacement Therapy (HRT) KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse assesses ischemic spots around the nail beds of a patient with rheumatoid arthritis and recognizes that these are a complication of medical diagnosis, rheumatoid arthritis, related to . ANS: vasculitis Vasculitis occurs when the vessels become inflamed and cause ischemia and necrosis. DIF: Cognitive Level: Comprehension REF: p. 864 OBJ: 3 TOP: Vasculitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A nurse clarifies that a postmenopausal woman who is not taking hormone replacement therapy should take mg elemental calcium on a daily basis. (Use numeric characters only.) ANS: 1500 Women who are not taking hormone replacements need calcium, 1500 mg/day. DIF: Cognitive Level: Knowledge REF: p. 869 OBJ: 2 TOP: Osteoporosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies Chapter 45: Fractures Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Two days after surgery for a crushed pelvis, a certified nursing assistant (CNA) reports that the patient is complaining of a shortness of breath and is demonstrating signs of confusion and restlessness. What should a nurse suspect, from these signs alone, that the patient has developed? a. Impending shock b. Fat embolus c. Anxiety d. Neurovascular compromise ANS: B These are the classic symptoms of a fat embolus that has escaped from the crushed marrow. DIF: Cognitive Level: Analysis REF: p. 881 OBJ: 3 | 6 TOP: Complications: Fat Embolism KEY: Nursing Process Step: Assessment| Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What should a nurse teach an older patient with a newly casted Colles fracture? a. Apply cool compresses to the cast. b. Let the hand and arm dangle to increase the drainage. c. Keep the hand immobile to reduce swelling. d. Move the shoulders to reduce contractures. ANS: D Movement of the shoulders will help decrease the threat of contracture from immobility. DIF: Cognitive Level: Comprehension REF: p. 891 OBJ: 7 TOP: Colles Fracture KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A patient who has osteomyelitis after multiple fractures inquires what the physician meant when he said that surgery would follow the antibiotic therapy. What is the nurse’s most helpful reply to explain why this surgery will be performed? a. To remove dead bone b. To close the open draining wound c. To close the area with casting material d. To amputate ANS: A After the antibiotic has controlled the infection in the bone, surgery will be performed to remove the dead bone. DIF: Cognitive Level: Comprehension REF: p. 882 OBJ: 4 TOP: Osteomyelitis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A patient with a crushed forearm cannot get pain relief with opioid medications. The injury is swollen, cool, and cyanotic, with weak distal pulses. What should the nurse suspect? a. Compartment syndrome b. Overwhelming infection c. Fat embolus d. Osteomyelitis ANS: A Compartment syndrome may occur after a massive injury or an inappropriately tight cast. The tissues become swollen to the point that they cut off their own circulation. DIF: Cognitive Level: Analysis REF: p. 882 OBJ: 3 TOP: Compartment Syndrome KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A patient who sustained a simple fracture of the left fibula 7 days earlier asks in what stage of bone healing he might be. What stage of healing should the nurse relay to the patient? a. Hematoma formation b. Ossification c. Callus formation d. Fibrocartilage formation ANS: C Callus formation occurs at the end of the first week after injury. DIF: Cognitive Level: Comprehension REF: p. 880 OBJ: 2 TOP: Healing Process of Fractures KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. Which assessment is of the greatest concern to a nurse when caring for a patient just admitted with a pelvic fracture? a. Pain level rating of 8 on a scale of 1 to 10 b. No urinary output for 8 hours c. Evidence of bruising along the patient’s hips and buttocks d. Complaints of the need for back care from resting in bed ANS: B The absence of urinary output could indicate a perforated bladder. DIF: Cognitive Level: Analysis REF: p. 896 OBJ: 3 TOP: Pelvic Fracture KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. An older woman falls down at church and immediately complains of severe pain in her left hip. Which observation is recognized as the cardinal sign of a fractured hip? a. Shortened left leg compared with the right b. Downward curled toes c. Internal rotation of the left leg d. Hematoma on the left hip ANS: A The classic sign of a fractured hip is a shortened limb on the affected side, with an externally rotated limb. DIF: Cognitive Level: Comprehension REF: p. 896 OBJ: 1 TOP: Fractured Hip KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. A patient has just had a plaster of Paris upper extremity cast placed because of a fractured radius. Which statement indicates that the patient understands the discharge teaching related to cast care? a. “When I get home, I will remove some of the padding if it feels tight so my fingers don’t swell.” b. “When I get home, I will wrap the cast in plastic so it will conserve the heat.” c. “When I get home, I will use a spoon handle to scratch inside if my arm itches.” d. “When I get home, I am going to rest in bed with my arm elevated above my heart.” ANS: D Resting with the limb elevated above the heart helps prevent swelling. DIF: Cognitive Level: Comprehension REF: p. 887 OBJ: 5 TOP: Cast Care KEY: Nursing Process Step: Evaluation MSC: NCLEX: Psychosocial Integrity: Physiological Adaptation 9. What special precaution should a nurse implement when assisting with the application of a short arm plaster cast? a. Dampen the skin to make the stockinette adhere. b. Tape the arm before applying the stockinette. c. Smooth the stockinette to prevent a pressure ulcer. d. Roll the stockinette tightly above and below the margins of the cast. ANS: C The stockinette is smoothed on the limb before applying the casting material to help reduce the threat of a pressure ulcer. DIF: Cognitive Level: Application REF: p. 885 OBJ: 5 TOP: Cast Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. An older patient who sustained a fractured hip and femur in a motor vehicle accident is to be in Russell traction for several weeks. What should be the focus of care for the nurse? a. Offering frequent distractions b. Encouraging nutrition c. Offering pain relief d. Preventing deep vein thrombosis (DVT) ANS: D DVT is a threat for the person who is going to experience lengthy periods of inactivity. Although nutrition, pain relief, and boredom will be nursing concerns as well, the prevention of DVT is the priority. DIF: Cognitive Level: Application REF: p. 893 OBJ: 3 | 5 TOP: Long-Term Complications of Fractures KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. A 78-year-old retired teacher with a history of osteoporosis has fallen in her bathroom and sustained a subcapital femoral fracture. She is scheduled for an open reduction and internal fixation (ORIF) procedure in the morning. Which type of traction will most likely be implemented? a. Bryant b. Buck c. Pelvic d. Crutchfield tongs ANS: B Buck traction is used to stabilize the fracture. The other options are not applicable. DIF: Cognitive Level: Application REF: p. 888 OBJ: 5 TOP: Traction KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. A nurse is told that a patient has a compound comminuted fracture. What characteristic of the bone in this type of fracture causes the nurse to be concerned? a. It is bent but not completely broken, and the bent piece protrudes through the skin. b. It is compressed, and bone pieces protrude through the skin. c. It is twisted, and the fragments are separated. d. It is broken into two or more pieces, and bone fragments protrude through the skin. ANS: D A compound comminuted fracture is a severe fracture with the bone broken in two or more pieces, with the pieces broken into small fragments and a portion of the bone protruding through the skin. DIF: Cognitive Level: Comprehension REF: p. 879 OBJ: 1 TOP: Fracture Types KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. A patient with bilateral avascular necrosis of the hips is to walk with crutches using a four-point gait for 6 weeks after her bone decompression surgeries. Which statement would indicate that the patient understands this technique? a. “The axillary bars on the crutches should support my weight when I walk.” b. “I will move both crutches and then swing my legs to the crutches—2 and 2 equals 4!” c. “I will move my right crutch and then my left leg and then the left crutch and my right leg.” d. “I will move both crutches and then swing my legs through the crutches together.” ANS: C This option describes the correct sequence for a four-point gait, which allows bearing of weight and one foot to be placed in front of the other. DIF: Cognitive Level: Comprehension REF: p. 889 OBJ: 5 TOP: Crutch Walking KEY: Nursing Process Step: Evaluation MSC: NCLEX: Psychosocial Integrity: Physiological Adaptation 14. What action should a nurse implement when caring for a patient diagnosed with a compound fracture? a. Limit narcotics for 8 hours after surgery. b. Monitor the patient’s respirations every hour. c. Assess for pulses distal to the injury. d. Verify that the patient is not allergic to sulfa. ANS: C Assessing for pulses distal to the injury is performed to monitor for inadequate circulation. DIF: Cognitive Level: Application REF: p. 884 OBJ: 6 TOP: Care of the Patient after Surgery for a Fracture KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 15. Assistive devices such as canes, crutches, and walkers are used for people who need to limit weight-bearing activities on joints. Which statement by a nurse best illustrates an understanding of the appropriate use of these devices? a. “Canes provide minimal support and balance and are carried on the unaffected side.” b. “When using a cane, slide it as you go to decrease the arm strain.” c. “A three-point gait is used when walking with a walker.” d. “When using crutches, the unaffected leg goes down the steps first.” ANS: A “Canes provide minimal support and balance and are carried on the unaffected side” is the only true statement. DIF: Cognitive Level: Comprehension REF: p. 890 OBJ: 5 TOP: Assistive Devices KEY: Nursing Process Step: Evaluation MSC: NCLEX: Psychosocial Integrity: Basic Care and Comfort 16. Which patient is most appropriate for a nurse to refer to home health care? a. A married man with a laundry room on the first floor b. A single woman with a bedroom in a rooming house c. A student living in a college dormitory but going home to stay with parents d. A woman staying with her daughter and son-in-law at their one-story home ANS: B The patient will need help with laundry and other activities of daily living. DIF: Cognitive Level: Analysis REF: p. 891 OBJ: 6 TOP: Nursing Assessment of a Patient with a Fracture KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 17. What should a nurse who is documenting and reporting the signs and symptoms of an infection underneath a cast include in the medical record? a. Elevated temperature b. Tingling and decreased sensation c. Full pulses and absence of pain d. Swelling and diminished motor function ANS: A Elevated temperature on the affected extremity may be a symptom of an infection under the cast. DIF: Cognitive Level: Application REF: p. 893 OBJ: 3 TOP: Complications of a Fracture KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 18. Which patient problem has the highest priority after surgery for the open reduction and external fixation of an ankle? a. Potential activity intolerance b. Potential for infection c. Immobility d. constipation ANS: B Potential for infection would have the highest priority because bone infections are serious complications. DIF: Cognitive Level: Analysis REF: p. 892 OBJ: 6 TOP: Post-operative care KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 19. A patient in a full body cast (spica) complains of nausea and abdominal distention. What potential complication should a licensed vocational nurse (LVN) suspect? a. Constipation b. Compartment syndrome c. Cast syndrome d. Shock ANS: C Cast syndrome is an uncommon complication for a person in a spica cast, in which compression of a portion of the duodenum occurs between the mesenteric artery and the spinal column. DIF: Cognitive Level: Analysis REF: p. 885 OBJ: 6 TOP: Cast Syndrome KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 20. An older adult patient is at risk for constipation after sustaining a pelvic fracture. Which nutritional suggestion by the nurse is most appropriate? a. Select food with high sodium content. b. Avoid foods high in dietary fiber. c. While immobilized, drink at least 2 to 3 L of fluids daily. d. Include milk products at every meal. ANS: C During periods of immobilization, a daily fluid intake of 2 to 3 L is recommended to promote bowel and bladder function. Food with sodium causes fluid retention. Dietary fiber helps diminish constipation. DIF: Cognitive Level: Application REF: p. 893 OBJ: 6 TOP: Nutrition Concepts with Fractures KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 21. Which finding should produce the most concern when performing pin care for a patient with an external fixator? a. Crusts around the pin b. Serous drainage on the dressing c. Purulent drainage d. Absence of pain ANS: C Purulent drainage is the only abnormal finding. DIF: Cognitive Level: Comprehension REF: p. 884 OBJ: 5 | 6 TOP: Pin Care KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 22. Which assessment is considered abnormal when a nurse performs a neurovascular assessment on a patient in skeletal traction? a. Delayed capillary refill b. Bilateral equal pulses c. Absence of pain and swelling d. Limb is the same color as the unaffected side ANS: A Delayed capillary refill reflects possible inadequate circulation. DIF: Cognitive Level: Comprehension REF: p. 891 OBJ: 5 | 6 TOP: Traction KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 23. What action should a nurse implement when dealing with the weights that are applying traction to a patient? a. Remove them to pull the patient up in bed. b. Hold them while the patient is changing positions in bed. c. Hold them for a few minutes if the patient complains of pain. d. Allow them to hang freely. ANS: D Weights must always hang freely to prevent complications. DIF: Cognitive Level: Application REF: p. 887 OBJ: 5 | 6 TOP: Traction KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 24. Which is true about a greenstick fracture? a. Line of the fracture goes across the bone in right angles to the longitudinal axis. b. Periosteum is not torn away from the bone. c. Fracture is incomplete, and one side is bent. d. Fracture occurred in one of the long bones of the body. ANS: C Greenstick fractures are most commonly seen in children, with the bone broken on one side but only bent on the other. DIF: Cognitive Level: Knowledge REF: p. 879 OBJ: 1 TOP: Fracture Healing KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 25. A patient with a fractured pelvis says that she will not ambulate because of pain. What should a nurse inform the patient can be prevented with early ambulation? a. Back injury b. DVT c. Callus formation d. Disuse syndrome ANS: B Early ambulation, although painful, avoids many of the complications of immobility such as DVT, constipation, and atrophy. DIF: Cognitive Level: Comprehension REF: p. 882 OBJ: 3 | 5 TOP: Early Ambulation with Fractured Pelvis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. To what can delayed union of a fracture be attributed? (Select all that apply.) a. Inadequate immobilization b. Hormone replacement therapy c. Long-term use of corticosteroids d. Infection e. Poor nutrition ANS: A, D, E Delayed union can be caused by inadequate immobilization, infection, poor nutrition, and poor alignment of the bone fragments. DIF: Cognitive Level: Knowledge REF: p. 882 OBJ: 3 TOP: Delayed Union KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. Which characteristics are present when crutches are properly fitted? (Select all that apply.) a. The axilla piece is 3 to 4 fingerbreadths below the axilla. b. They fit close to the axilla for secure support. c. They are measured and adjusted when the patient is in the tripod position. d. Adjusted hand grips allow for a 45-degree flexion of the elbow. e. They are padded so patient can bear weight on the axilla piece when ambulating. ANS: A, C Crutches should allow for 3 to 4 fingerbreadths between the axilla and the axilla piece, the crutches should be adjusted when the patient is in the tripod position, the elbow flexion should be adjusted for a 30-degree flexion, and the weight should not be borne on the axilla because of the possibility of nerve damage. DIF: Cognitive Level: Comprehension REF: p. 888 OBJ: 5 TOP: Crutch Adjustment KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. A fracture that occurs because of osteoporosis is classified as a(n) fracture. ANS: pathological A fracture that occurs as a result of a tumor of another pathologic condition is classified as a pathologic fracture. DIF: Cognitive Level: Knowledge REF: p. 879 OBJ: 3 TOP: Pathological Fracture KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. A nurse uses a diagram to show the process of a fractured bone healing. (Arrange the options in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Ossification b. Hematoma c. Fibrocartilage d. Consolidation e. Callus ANS: BCEAD The sequence of healing is hematoma, fibrocartilage, callus, ossification, and consolidation. DIF: Cognitive Level: Comprehension REF: p. 880 OBJ: 2 TOP: Bone Healing KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. Arrange the process of stair climbing with crutches in the correct sequence: (Arrange the options in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Body weight is supported with crutches. b. Crutches are moved to the next step. c. The affected leg moves to the next step. d. The unaffected leg is moved to the next step. e. Body weight is transferred to the unaffected leg. ANS: ADEBC When climbing steps on crutches, the body weight is supported with the crutches. While the unaffected leg is moved to the next step, the body weight is transferred to the unaffected leg; while the crutches are moved up, the affected leg moves up. DIF: Cognitive Level: Comprehension REF: p. 889 OBJ: 5 TOP: Stair Climbing with Crutches KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 46: Amputations Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is aware that a patient who is having his leg amputated is also having a prosthesis fitted during at the same time as the surgery. Which fact should the preoperative teaching plan include? a. Extra preoperative medications will be needed. b. A rigid dressing will be applied to accommodate the prosthesis. c. A series of temporary prostheses will be put in place before the permanent one. d. Wiring the residual limb will be needed to ensure acceptance of the prosthesis. ANS: B A rigid dressing will be applied to the residual limb to accommodate the prosthesis immediately after surgery. DIF: Cognitive Level: Application REF: p. 900 OBJ: 3 TOP: Preoperative Teaching KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A patient asks when he should expect to be up and walking after his below-the-knee amputation. When should the nurse assure him that most people with amputations can fully bear weight? a. 3 weeks b. 1 month c. 6 weeks d. 3 months ANS: D Most people with amputations can fully bear weight 3 months after surgery. DIF: Cognitive Level: Comprehension REF: p. 900 OBJ: 5 TOP: Amputation Recovery KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A nurse is conducting a safety seminar and reminds the audience that upper extremity amputations are most frequently caused by trauma. Which population has the highest incidence of this type of amputation? a. School-aged girls b. School-aged boys c. Young men d. Young women ANS: C Young men are at greater risk from work trauma because they are traditionally the ones working with farm and heavy machinery. DIF: Cognitive Level: Comprehension REF: p. 898 OBJ: 1 TOP: Incidence KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. An 80-year-old man with diabetes has had vascular problems with his feet and lower legs for 10 years and is scheduled for a left below-the-knee amputation. Which remark by the patient indicates an understanding of the procedure? a. “I am glad this amputation will end my diabetic problems.” b. “After they have hacked my leg, I won’t be able to drive.” c. “If this heals well, how long until I get a prosthesis?” d. “I hate that my left knee is going to be useless without a foot.” ANS: C Only this option indicates that the patient realizes the extent of the surgery. DIF: Cognitive Level: Comprehension REF: p. 902 OBJ: 4 TOP: Amputation KEY: Nursing Process Step: Evaluation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 5. What routine preoperative diagnostic tests are appropriate for a patient anticipating a below-the-knee amputation? a. Pulse volume recording and white blood cell (WBC) count b. Cardiac catheterization and WBC count c. Pulse volume recording and radiographic images d. Thermography and cardiac catheterization ANS: A Pulse volume recording and WBC count are two diagnostic tests for patients anticipating a below-the-knee amputation. DIF: Cognitive Level: Comprehension REF: p. 903 OBJ: 4 TOP: Diagnostic Tests and Procedures KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 6. Where is the limb severed with an elbow disarticulation? a. Just above the elbow joint b. Just below the elbow joint c. Between the shoulder and elbow d. Through the elbow joint ANS: D Disarticulations sever the limbs through the joints. DIF: Cognitive Level: Knowledge REF: p. 898 OBJ: 2 TOP: Type of Amputation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. A patient with peripheral vascular disease (PVD) and diabetes asks what he can do to help prevent an amputation. What is the best response of the nurse? a. “There is not really anything you can do to help.” b. “Stopping smoking would help prevent vasoconstriction.” c. “You will not need to check your blood glucose levels.” d. “It is important to eat big meals so your body can heal.” ANS: B Smoking causes vasoconstriction, which aggravates PVD. DIF: Cognitive Level: Comprehension REF: p. 899 OBJ: 3 TOP: Prevention of Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. Why is a closed amputation usually performed? a. To create a weight-bearing residual limb b. To alleviate the effects of trauma c. To allow infection to heal and drain d. To treat a limb with gangrene ANS: A A closed amputation is performed to create a weight-bearing limb. DIF: Cognitive Level: Comprehension REF: p. 900 OBJ: 3 TOP: Surgical Treatment KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 9. What controls the movement with a myoelectrically controlled prosthesis? a. Patient’s muscle movement and the prosthesis b. Battery-operated muscles implanted in the prosthesis c. Motion-sensing mechanism that swings the prosthesis forward d. Internal computer chip in the prosthesis ANS: A A patient’s muscle movement and the prosthesis control movement with a myoelectrically controlled prosthesis. DIF: Cognitive Level: Knowledge REF: p. 900 OBJ: 3 TOP: Prostheses KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. A patient who had a below-the-knee amputation 24 hours earlier is complaining of burning pain in his left foot. Which intervention is most appropriate for the nurse to implement? a. Remind the patient that it is only phantom pain. b. Medicate the patient with the prescribed pain remedy. c. Remind him that such sensations will go away in a few weeks. d. Distract the patient with conversation. ANS: B The nurse should medicate a patient for pain. Phantom pain is real. Although distraction is a possible intervention, it is not the most effective. DIF: Cognitive Level: Application REF: p. 904 OBJ: 4 TOP: Phantom Pain KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Basic Care and Comfort 11. During the admission of a patient scheduled for an amputation, a patient relates that she is a practicing Orthodox Jew. What arrangements are appropriate for the nurse to make for this patient? a. A veil should cover the amputated part. b. A rabbi must be present for the surgery. c. The amputated part should be buried. d. A family member should be present to read the Torah. ANS: C Orthodox Jews bury all body parts. DIF: Cognitive Level: Application REF: p. 905 OBJ: 4 TOP: Nursing Care for the Orthodox Jew KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Basic Care and Comfort 12. What is an appropriate outcome for a patient with feelings of anxiety related to a perceived threat of disability?” a. Comfort is increased; verbalized pain is less. b. Anxiety is relieved; the patient verbalizes concern related to disability. c. Grief is resolved; the patient expresses an acceptance of loss. d. Residual limb is cleaned; no exudate, redness, or edema is observed. ANS: B The relief of anxiety speaks directly to the patient’s feelings of anxiety. Other options are possible outcome goals but do not pertain to anxiety. DIF: Cognitive Level: Application REF: p. 906 OBJ: 4 | 5 TOP: Nursing Care KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 13. What is the greatest danger in the early postoperative period after an amputation? a. Infection b. Hemorrhage c. Pain d. Edema ANS: B Hemorrhage is the greatest danger in the early postoperative period after an amputation. DIF: Cognitive Level: Comprehension REF: p. 902 OBJ: 4 TOP: Complications KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 14. A nurse is caring for a patient who has undergone replantation of a body part. What might the saliva of leeches be used to treat in this patient? a. Inadequate arterial blood flow b. Venous insufficiency c. Venous congestion d. Increased arterial blood flow ANS: C Leeches are used to treat venous congestion. DIF: Cognitive Level: Comprehension REF: p. 907 OBJ: 4 | 5 TOP: Replantation KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 15. A patient who amputated his thumb in a lawnmower accident hands the emergency department nurse his thumb in a glass jar. What is the best action for the nurse to implement? a. Place the thumb in a baggie with iced lactated Ringer solution. b. Wrap the thumb in plastic wrap and place it on ice. c. Leave the thumb in the jar and place it in the refrigerator. d. Wrap the thumb in a cloth saturated with normal saline and place it in a baggie. ANS: D The amputated part should be wrapped in a towel soaked with normal saline solution, placed in a baggie, and put in a cool bath. DIF: Cognitive Level: Application REF: p. 906 OBJ: 4 TOP: Care of the Amputated Thumb KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. A patient who has a below-the-elbow prosthesis shows the home health care nurse the residual limb, which is red, edematous, and warm to touch. What should the nurse instruct this patient to do? a. Apply soothing lotion to the residual limb before replacing the prosthesis. b. Dampen the prosthetic limb sock to hydrate and cool the residual limb. c. Pad the socket with lamb’s wool and replace the prosthesis. d. Leave the prosthesis off and notify physician. ANS: D An inflamed residual limb suggests an infection. The prosthesis should be removed, the limb should be gently cleansed with soap and water, and the physician should be notified. DIF: Cognitive Level: Application REF: p. 903 OBJ: 5 TOP: Infection KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. A child comes to the school nurse with his index finger partially amputated and hanging by a shred of skin and muscle. What is the best action by the nurse? a. Flush the hand with warm water and wrap it in a towel. b. Carefully cut the skin holding the finger and wrap the finger and hand in a clean towel. c. Pinch the finger to stop the bleeding and take the child to the hospital. d. Wrap the hand and finger securely and place it on an ice water–filled plastic bag. ANS: D The nurse should leave the shred of skin and muscle intact, wrap the hand and finger in a towel soaked in normal saline, and place it on a cool surface. DIF: Cognitive Level: Application REF: p. 906 OBJ: 4 TOP: Partial Amputation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 18. What nursing action should be implemented in the postoperative care for a patient with replantation of the right thumb? a. Decreasing the temperature of the room to 70 F b. Elevating the hand but keeping it below the level of the heart c. Offering coffee, tea, or cola to help increase fluid intake d. Placing an antiembolus sleeve on the right arm ANS: B Slight elevation of the hand will encourage drainage but not affect arterial perfusion. The room temperature should be 80 F. The patient should avoid all caffeine drinks and tight clothing or dressings. DIF: Cognitive Level: Application REF: p. 907 OBJ: 4 TOP: Nursing Care of Replantation KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 19. A nurse is caring for a patient with a recent below-the-knee amputation. What should the nurse recommend to this patient to prevent the loss of calcium and protein? a. Drink 1 to 2 L of fluid daily. b. Ingest at least four milk products each day. c. Ambulate 30 minutes a day. d. Take vitamin supplements daily. ANS: C Even a small amount of ambulation will decrease the loss of calcium and protein. DIF: Cognitive Level: Application REF: p. 906 OBJ: 4 TOP: Postoperative Ambulation KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 20. What are late signs of hemorrhage in the postoperative period after an amputation? a. Restlessness and increased respirations b. Cyanosis and hypotension c. Confusion and seizures d. Headache and hypertension ANS: B Cyanosis and hypotension are late signs of hemorrhage in the postoperative period after an amputation. DIF: Cognitive Level: Comprehension REF: p. 902 OBJ: 4 TOP: Complications KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 21. The verbalization of microvascular precautions is a criterion for measuring the achievement of which outcome? a. Adequate circulation in the replanted limb b. Pain relief c. Patient knowledge of therapeutic measures d. Adjustment to change in appearance and function ANS: C Verbalizing the information related to microvascular precautions is evidence of the patient’s achievement of having acquired the necessary knowledge. DIF: Cognitive Level: Knowledge REF: p. 907 OBJ: 5 TOP: Nursing Care Planning KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 22. Which postoperative observation must be reported to the physician immediately? a. Brownish-red drainage on the dressing, which is damp b. Respirations of 20 breaths/min c. Pulse of 72 beats/min d. Bright-red bleeding ANS: D Bright-red bleeding is not expected and indicates hemorrhage. Direct pressure should be applied over the dressing and the physician or charge nurse should be notified. DIF: Cognitive Level: Comprehension REF: p. 902 OBJ: 4 TOP: Complications KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 23. A home health care nurse suspects a neuroma in a patient who had an above-the-knee amputation 1 month earlier. Which complaint by the patient led the nurse to suspect a neuroma? a. Area of swelling and bruising on distal portion of residual limb b. Prickling sensation over residual limb c. Sharp severe pain in the residual limb d. Area of numbness on distal portion of residual limb ANS: C A neuroma causes sharp severe pain in the residual limb. A neuroma occurs when severed nerve endings attempt to regenerate. The neuroma requires excision by the surgeon. DIF: Cognitive Level: Comprehension REF: p. 901 OBJ: 4 TOP: Neuroma KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 24. Which action should a nurse implement to diminish swelling of the residual limb in the postoperative period after an above-the-knee amputation? a. Elevate the foot of the bed on blocks. b. Elevate the residual limb on pillows. c. Elevate the head of the bed 15 degrees. d. Turn the patient on the affected side. ANS: A Elevating the foot of the bed on blocks will help diminish edema and will not cause hip contracture deformity. DIF: Cognitive Level: Application REF: p. 901 OBJ: 4 TOP: Prevention of Postoperative Edema KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. Which major situational occurrences might lead to amputations? (Select all that apply.) a. Trauma b. Disease c. Tumors d. Congenital defects e. Carelessness ANS: A, B, C, D The categories of occurrences that lead to amputation are trauma, disease, tumors, and congenital defects. Carelessness frequently leads to trauma. DIF: Cognitive Level: Knowledge REF: p. 898 OBJ: 1 TOP: Causes for Amputation KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What is a closed amputation designed to do? (Select all that apply.) a. Prepare a weight-bearing limb. b. Cover the stump with tissue and muscle. c. Place sutures immediately over the bone. d. Be staged to closure. e. Be immediately ready for a prosthesis. ANS: A, B Closed amputations are meant to prepare the limb for weight-bearing activities with tissue and muscle applied to the residual limb. Sutures are not placed over the bone for future comfort and better healing. Closed amputations are not staged because they are open amputations, and they may or may not be prepared for an immediate prosthesis. DIF: Cognitive Level: Comprehension REF: p. 900 OBJ: 2 TOP: Closed Amputation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. How should a nurse modify a teaching plan for an older adult who has had an above-the-knee amputation? (Select all that apply.) a. Offer smaller units of information at a time. b. Increase time for learning. c. Place less emphasis on chronic health problems. d. Clarify the reality of phantom pain. e. Include frequent repetition. ANS: A, B, D, E Older adults are quite capable of learning, but the amount of information offered at one time should be lessened, the time for learning should be increased, the probability of phantom pain should be clarified, and repetition should be frequently used. DIF: Cognitive Level: Application REF: p. 905 OBJ: 4 TOP: Teaching the Older Adult KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. A nurse clarifies that the precise term for the patient’s amputation, which will be through the knee joint, is called _ . ANS: disarticulation Disarticulation is the appropriate term for an amputation through the knee joint. DIF: Cognitive Level: Knowledge REF: p. 898 OBJ: 2 TOP: Disarticulation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. An amputation of a gangrenous limb that is left open for 10 days before closure is classified as a staged or _ amputation. ANS: guillotine A staged or guillotine amputation is one in which the wound is left open until the area is free of infection or evidence of gangrene. DIF: Cognitive Level: Knowledge REF: p. 900 OBJ: 1 TOP: Staged Amputation KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 3. To reduce the possibility of hip contractures in a patient with an above-the-knee amputation, a nurse periodically places the patient in a(n) position. ANS: prone The prone position will cause the muscles of the thigh to stretch and prevent contracture. DIF: Cognitive Level: Application REF: p. 901 OBJ: 4 TOP: Nursing Care to Prevent Contractures KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. Preoperative exercises for a patient undergoing a lower-extremity amputation include training. ANS: upper body Upper body training will strengthen the arms to aid in movement after the loss of a lower extremity. DIF: Cognitive Level: Knowledge REF: p. 904 OBJ: 4 TOP: Upper Body Training KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 47: Endocrine System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient is receiving the medication octreotide (Sandostatin) as a treatment for acromegaly. What should the nurse explain regarding this medication? a. It reverses the effects of acromegaly. b. It should be given on a daily basis by injection. c. It increases insulin secretion causing hypoglycemia. d. It suppresses the growth hormone. ANS: D Sandostatin will suppress growth hormone, but it will not reverse the effects of acromegaly. It is administered three times a week and suppresses insulin secretion causing hyperglycemia. DIF: Cognitive Level: Comprehension REF: p. 922 OBJ: 3 TOP: Growth Hormone Suppression KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. Which instruction should a nurse provide when a patient starts taking a saturated solution of potassium iodide (SSKI)? a. Sip medication through a straw to prevent tooth staining. b. Double the dose if a dose is missed. c. Expect excessive salivation. d. Take before meals. ANS: A SSKI can discolor teeth if not sipped through a straw; no iodide drug should be doubled; excessive salivation is a sign of toxicity; and the medication should be taken after meals. DIF: Cognitive Level: Comprehension REF: p. 925 OBJ: 4 TOP: SSKI KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. Which significant need should be included in instructions to a patient scheduled for a thyroid scan (123I)? a. Provide a special container to collect urine for the next 24 hours. b. Wear a protective apron to shield him or her from radiation for the next 24 hours. c. Request that visitors keep a distance of at least 6 feet away for the next 24 hours. d. Do not consume iodine for one week before the test.. ANS: D The patient should not consume iodine for one week before the test. Iodine is in radiographic dyes, some oral contraceptives, weight control drugs, multivitamins, all thyroid drugs, and some food, especially seafood. DIF: Cognitive Level: Application REF: p. 916 OBJ: 2 TOP: Thyroid Diagnostic Tests KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 4. A patient asks about his laboratory test, which showed a high level of thyroid-stimulating hormone (TSH) and a low level of T4. What is the most accurate explanation? a. “It means that you have an inconsistency in your thyroid tests, and you will need more testing.” b. “I am sorry. You will have to ask your physician about your laboratory results. We are not allowed to discuss them.” c. “The TSH is sending a message to your thyroid gland to increase production, but your thyroid isn’t producing enough hormone.” d. “That means that you will have to go on hormone therapy for the rest of your life.” ANS: C The test determines whether the problem is in the pituitary gland or in the thyroid gland. In this patient, the high level of TSH is coming from the pituitary gland as it should, but the thyroid gland is not responding with adequate hormone production. DIF: Cognitive Level: Comprehension REF: p. 917|p. 922 OBJ: 2 TOP: Thyroid Laboratory Tests KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. A patient has been given an antithyroid drug called methimazole. What appropriate nursing implementations should be included? a. Using special radioactive precautions for her urine for the first 24 hours b. Monitoring her vital signs and withholding the medications if her pulse is greater than 100 beats/min c. Teaching her to watch for and report any signs and symptoms of hypothyroidism or infections d. Keeping her on a low-calorie, low-protein diet ANS: C The drug targets the thyroid gland to slow its function, so signs and symptoms of hypothyroidism or infections need to be reported. Thionamides may cause suppression of neutrophils leading to a lowered resistance. DIF: Cognitive Level: Application REF: p. 924 OBJ: 3 | 4 TOP: Antithyroid Medications KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 6. An older patient with hypothyroidism asks why her daily dose of thyroid hormone, which she has taken for 15 years, has been reduced. What is nurse’s best rationale when explaining what the decreased dose is related to? a. Improved efficacy of the thyroid preparation b. Age-related reduction in metabolic rate c. Drug-related hypertrophy of the thyroid d. Changes in your diet and activity level ANS: B Older patients have slower drug metabolism; consequently, the drug stays in their systems. All patients receiving hormone replacement need to be periodically evaluated. DIF: Cognitive Level: Comprehension REF: p. 924 OBJ: 3 TOP: Age-Related Changes in Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies MULTIPLE RESPONSE 1. A nurse makes a list of symptoms that a patient who is taking methimazole (Tapazole), a thionamide drug, should report. What should this list include? (Select all that apply.) a. Becoming pregnant b. Jaundice c. Blood in the stool d. Rash e. Urine retention ANS: A, B, C, D Urine retention is not a side effect of methimazole (Tapazole). DIF: Cognitive Level: Knowledge REF: p. 924 OBJ: 4 TOP: Patient Education for Thionamides KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. What are the common age-related changes in the endocrine system? (Select all that apply.) a. Diminished response to antidiuretic hormone (ADH). b. Decline in growth hormone (GH) production. c. Reduction in protein synthesis. d. Decreased risk for hypothyroidism. e. Decline in cortisol secretion. ANS: A, B, C, E Endocrine function usually remains adequate in healthy older adults, but small changes are important when an illness alters homeostasis. Age-related endocrine changes include dimished response to ADH; decline in GH production, which leads to a reduction in protein synthesis; and a decline in cortisol secretion. Although not normal, hypothyroidism is more common in older adults, especially in women. DIF: Cognitive Level: Comprehension REF: p. 919 OBJ: 1 TOP: Hypothyroidism KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 48: Pituitary and Adrenal Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What should preoperative teaching for a patient scheduled for a transsphenoidal hypophysectomy include that the patient should do postoperatively? a. Avoid sneezing. b. Drink through a straw. c. Cough forcefully. d. Wash mouth out with peroxide. ANS: A The patient should be taught to avoid sneezing, coughing, drinking through a straw, and using a stringent mouthwash that might dislodge the graft. DIF: Cognitive Level: Comprehension REF: p. 930|p. 934 OBJ: 1 TOP: Pituitary Surgery KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. What hormone causes the features of a patient with acromegaly? a. Prolactin b. Growth hormone c. Thyroid-stimulating hormone d. Adrenocorticotropic hormone ANS: B Excess growth hormone in an adult will cause the flat bones to grow because the adult has little capacity for heightened growth. In a child, this same excess would cause giantism. DIF: Cognitive Level: Knowledge REF: p. 930 OBJ: 1 TOP: Acromegaly KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. What are the classic symptoms of diabetes insipidus (DI)? a. Diuresis, dehydration, and thirst b. Dizziness, hypertension, and excitability c. Stress incontinence, vomiting, and edema d. Bradycardia, insomnia, and muscle cramps ANS: A Common signs and symptoms of DI are massive diuresis, dehydration, and thirst. Dehydration is characterized by hypotension, tachycardia, dizziness, decreased skin turgor, weakness, and possible fainting episodes. DIF: Cognitive Level: Knowledge REF: p. 937 OBJ: 1 TOP: Diabetes Insipidus KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A patient states that he is confused because the physician told him that his diabetes insipidus (DI) is nephrogenic. What should the nurse state when describing the difference between nephrogenic DI and neurogenic DI? a. Nephrogenic DI will eventually resolve without medication. b. Nephrogenic DI requires the nasal spray lypressin. c. Nephrogenic DI does not respond to ADH. d. Nephrogenic DI will require dialysis. ANS: C Nephrogenic DI does not respond to ADH. DIF: Cognitive Level: Comprehension REF: p. 936 OBJ: 1 TOP: Addison Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. A 14-year-old adolescent male patient has been diagnosed with Addison disease. Which effect of Addison disease should this patient be aware of? a. He will not develop pubic hair. b. He will grow a heavy beard. c. He will become bald at an early age. d. He will have enlarged joints. ANS: A The boy with Addison disease will not grow facial, axillary, or pubic hair. Balding and enlarged joints are not associated with Addison disease. DIF: Cognitive Level: Comprehension REF: p. 940 OBJ: 1 TOP: Addison Disease KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. What is the cardinal indication of a pheochromocytoma? a. Significant hypertension b. Extreme nausea c. Abdominal pain d. Edema in the legs ANS: A The patient with a pheochromocytoma exhibits dangerously high hypertension. Hypertension and its attendant symptoms are what bring the patient to the physician. The tumor is found incidentally. DIF: Cognitive Level: Knowledge REF: p. 947 OBJ: 1 TOP: Adrenal Tumor KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A nurse is caring for a patient diagnosed with Addison disease. Which signs and symptoms should lead the nurse to suspect an adrenal crisis? a. Hypertension and abdominal pain b. Confusion and tachycardia c. Bradycardia and nausea d. Widening pulse pressure and shortness of breath ANS: B Confusion and tachycardia are signs that the patient may be in adrenal crisis, which is a medical emergency and should be brought to the attention of the charge nurse. DIF: Cognitive Level: Application REF: p. 940 OBJ: 1 TOP: Adrenal Crisis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. A nurse includes in the discharge plan for a patient with Addison disease, “Potential for injury.” What should measures to deal with this include? a. Arranging for uncluttered floor space b. Rising slowly from a lying position c. Keeping the room well lit d. Providing instructions in the use of a walker ANS: B Hypovolemia lowers the blood pressure and may cause orthostatic (postural) hypotension, which may cause sudden profound weakness. DIF: Cognitive Level: Comprehension REF: p. 943 OBJ: 2 TOP: Addison Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. What should a nurse include when planning education to a patient with Addison disease? a. Discontinue hormonal replacement therapy if the patient becomes nauseated or has diarrhea. b. Decrease medication if the patient is under stress or is being treated for an infection. c. Wear a medical alert tag and carry emergency dexamethasone. d. Begin a vigorous exercise program to overcome weakness and muscle wasting. ANS: C The medical alert bracelet will reduce the patient’s risk of not receiving appropriate and timely care in an emergency situation. DIF: Cognitive Level: Application REF: p. 942 OBJ: 2 TOP: Addison Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. A patient with long-term asthma develops Cushing syndrome. What is the cause of this condition? a. Taking corticosteroids for many years b. Abruptly withdrawing cortisone therapy c. Lacking ACTH, related to the pituitary gland d. Poorly functioning adrenal glands ANS: A Long-term corticosteroid use is a prime cause of Cushing syndrome. DIF: Cognitive Level: Comprehension REF: p. 944 OBJ: 1 TOP: Cushing Syndrome KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 11. Which findings are expected when assessing a patient with Cushing syndrome? a. Edema of the trunk, extremities, and face b. Wasting of the abdomen with thick, calloused skin c. Excess adipose tissue in the trunk, slender extremities, and moon face d. High levels of potassium and low levels of sodium, weakness, and wasting ANS: C Truncal obesity, thin extremities, and moon face are the classical signs of Cushing syndrome caused by long-term corticosteroid therapy. DIF: Cognitive Level: Comprehension REF: p. 944 OBJ: 1 TOP: Cushing Syndrome KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. Which statement by a patient diagnosed with Cushing syndrome leads a nurse to conclude that teaching has been effective? a. “I know I should add salt to everything I eat.” b. “I make a point to avoid excessive exposure to sun.” c. “I avoid being exposed to anyone with an infection.” d. “I am careful to wear well-fitting shoes.” ANS: C Patients with Cushing syndrome are especially prone to infection. Adding salt would increase fluid retention. Sun exposure and well-fitting shoes are not significant for Cushing syndrome. DIF: Cognitive Level: Comprehension REF: p. 946 OBJ: 2 TOP: Cushing Syndrome KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 13. A nurse is assessing a patient with Simmonds cachexia. What symptom should the nurse anticipate the patient will exhibit? a. High body temperature b. Ruddy complexion c. Silky body hair d. Muscle wasting ANS: D Simmonds cachexia is a panhypopituitarism condition in which muscle wasting, small organs, very pale complexion, virtually no body hair, and subnormal body temperature are symptoms. DIF: Cognitive Level: Comprehension REF: pp. 934-935 OBJ: 1 TOP: Panhypopituitarism KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A nurse making a care plan for a 10-year-old boy with hyperpituitarism identifies an altered body image. What should the nurse relate this nursing diagnosis to? a. Lack of facial hair b. Excessive height c. Small genitalia d. Skin eruptions on the face ANS: B A 10-year-old boy will be excessively tall for his age. Hair is not lacking, and skin eruptions associated with giantism are observed. Most 10-year-old boys have small genitalia. DIF: Cognitive Level: Application REF: p. 930 OBJ: 2 TOP: Hyperpituitarism KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 15. What should a nurse include when caring for a patient after a hypophysectomy, during which the entire pituitary was removed? a. Maintaining strict intake and output fluids b. Keeping the patient flat in bed for the first 24 hours c. Withholding analgesics to assess the level of consciousness d. Providing mouth care with thorough cleansing of the oral cavity ANS: A With the removal of the entire pituitary gland, the patient will have no effective ADH and will excrete large amounts of urine. The patient is usually kept in a semi-Fowler position and is medicated as needed for pain. Because of the graft, mouth care is minimal, if provided at all. DIF: Cognitive Level: Application REF: p. 933 OBJ: 2 TOP: Hypophysectomy KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. What can bring on an addisonian crisis? a. Sudden atmospheric temperature change b. Hyperglycemia c. Infection d. Change of altitude ANS: C Infection is one of the many stresses that can bring on an addisonian crisis. DIF: Cognitive Level: Knowledge REF: p. 940 OBJ: 1 TOP: Addisonian Crisis KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. A 6-foot, 2-inch, 16-year-old girl who is being treated for hyperpituitarism says, “I can’t stand it that I look like a freak.” What is the nurse’s best response? a. “Gigantism is treatable.” b. “Your height could help you be a basketball star or a model.” c. “What is it about your height that makes you a freak?” d. “Your height is something you will have to get used to.” ANS: C Using a question that encourages further discussion will help the nurse understand the distress that the patient is trying to convey. Listening to patients’ concerns helps them get in touch with their own feelings. DIF: Cognitive Level: Application REF: p. 932 OBJ: 2 TOP: Gigantism KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 18. A patient with hypopituitarism must take medications for the rest of his or her life. What should the patient teaching plan include? a. “Constipation must be prevented because straining increases intracranial pressure.” b. “You must become familiar with the signs and symptoms of inadequate or excessive hormone replacement.” c. “It is not necessary to wear a medical alert bracelet or necklace.” d. “Your self-image is important. Take positive steps to improve your appearance.” ANS: B To prevent complications, recognizing the importance of continuing to replace the missing hormones is essential for the patient. DIF: Cognitive Level: Comprehension REF: p. 936 OBJ: 2 TOP: Hypopituitarism KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 19. Two days after a hypophysectomy a patient complains of a headache and nuchal rigidity. What action should the nurse take based on these assessments? a. Medicate with the prescribed analgesic. b. Report suspected meningitis to the head nurse. c. Closely monitor the patient’s blood pressure. d. Elevate the head of the bed to 45 degrees. ANS: B The headache and the nuchal rigidity are signs of meningitis. DIF: Cognitive Level: Application REF: p. 933 OBJ: 1 TOP: Signs of Meningitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 20. A nurse is caring for a patient with diabetes insipidus (DI). Which signs should the nurse report that indicate a change in condition? a. Dropping blood pressure b. Light clear urine c. Moist mucous membranes d. Excessive thirst e. Large urine output ANS: A A dropping blood pressure is an indication that the hypovolemia with DI has reached a significant point and will require medical implementation. All other options are the expected signs of this disorder or an indication that therapy is effective. DIF: Cognitive Level: Comprehension REF: p. 937 OBJ: 1 TOP: Diabetes Insipidus KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. What symptoms should a nurse expect a patient with the diagnosis of SIADH to report during an intake interview? (Select all that apply.) a. Headache b. Hypotension c. Weight gain d. Muscle cramps e. Weakness ANS: A, C, D, E Retained fluid and hyponatremia cause weight gain and elevated blood pressure with an attendant headache. The hyperkalemia causes the patient to feel weak and have muscle cramps. DIF: Cognitive Level: Comprehension REF: p. 938 OBJ: 1 TOP: Signs of SIADH KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. An 18-year-old girl is diagnosed with adenoma of the pituitary gland. What signs of this diagnosis should the nurse assess? (Select all that apply.) a. Cessation of menses b. Milk production c. Excess body hair d. Excessive urine output e. Weight loss ANS: A, B Pituitary adenomas that secrete hormones may cause amenorrhea (cessation of menses), galactorrhea (abnormal milk production), hyperthyroidism, and Cushing syndrome. DIF: Cognitive Level: Comprehension REF: p. 929 OBJ: 1 TOP: Signs of Adenoma of Anterior Pituitary KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation COMPLETION 1. A nurse noting a peaked T wave on the electrocardiogram (ECG) of a patient with Addison disease recognizes this complex as suggestive of . ANS: hyperkalemia Hyperkalemia will cause an elevated, peaked T wave. DIF: Cognitive Level: Comprehension REF: p. 941 OBJ: 1 TOP: Hyperkalemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A nurse prepares a family for the altered appearance of the patient returning from stereotactic radiosurgery to see a(n) in place. ANS: stereotactic frame The stereotactic frame, which helps direct the radiation, is attached to the patient’s head with pins. DIF: Cognitive Level: Comprehension REF: p. 933 OBJ: 2 TOP: Stereotactic Radiosurgery KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 49: Thyroid and Parathyroid Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A physician ordered T3 and T4 tests for a young woman complaining of fatigue, weight gain, muscle aches and pains, and constipation. Which laboratory test results will help confirm the diagnosis of hypothyroidism? a. Both tests show decreases. b. Both tests show increases. c. The T3 test elevates, and the T4 test decreases. d. The level of thyroxin rises and then falls back to subnormal levels. ANS: A These complaints are strongly suggestive of thyroid disorder; T3 and T4 laboratory diagnostic tests are the most useful. DIF: Cognitive Level: Knowledge REF: p. 950 OBJ: 1 TOP: Thyroid Diagnostic Tests KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance 2. A patient with a hyperthyroid complains of fatigue but still cannot get to sleep. What is the best suggestion by the nurse? a. Taking “cat naps” during the day b. Adhering to a bedtime ritual c. Drinking a cup of cocoa before bedtime d. Performing mild prebedtime exercises ANS: B Bedtime rituals such as a warm bath, reading, and listening to music cue the body for sleep. Naps during the day may make nighttime sleep difficult; exercising and drinking caffeine-filled drinks are stimulating and should be avoided by the person with insomnia. DIF: Cognitive Level: Comprehension REF: p. 953 OBJ: 2 TOP: Hyperthyroidism Insomnia KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 3. A patient with exophthalmos is distressed about her appearance and asks when it will go away. What is the best response by the nurse? a. It is not reversible. b. It can be disguised with sunglasses and makeup. c. It usually subsides after medication for hyperthyroidism is started. d. It can be minimized with plastic surgery to the eyelids. ANS: C The “startled” appearance of the patient with exophthalmos usually subsides several weeks after therapy for hyperthyroidism becomes effective. DIF: Cognitive Level: Comprehension REF: p. 954 OBJ: 2 TOP: Exophthalmia KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 4. A nurse is explaining Graves disease to a newly diagnosed patient. Which statement by the nurse best clarifies the pathophysiologic changes of Graves disease? a. “Your thyroid gland is not producing enough hormones; consequently, you will need replacement therapy.” b. “Your thyroid gland is overactive, but there are ways to treat it through medicine or surgery.” c. “It’s an autoimmune disorder that has no satisfactory treatment.” d. “Graves disease is a temporary disorder that will gradually subside.” ANS: B The patient needs to recognize the nurse’s role in giving accurate, timely information. DIF: Cognitive Level: Comprehension REF: p. 951 OBJ: 1 TOP: Graves Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Physiological Adaptation 5. A nurse assessing a patient 1 day after a subtotal thyroidectomy notes that the patient’s color is poor, the pulse and respirations are rapid, and the patient feels warm to the touch. The patient says that she feels frightened. What is the best initial implementation by the nurse? a. Tell her that there is nothing to be afraid of and stay to calm her. b. Ask her if she would like pain medication. c. Call the charge nurse; these are signs of a thyroid storm. d. Get a tracheostomy set at the bedside. ANS: C Call the charge nurse; these signs and symptoms suggest excessive stimulation caused by an elevated level of thyroid hormones, and the patient needs immediate care. DIF: Cognitive Level: Application REF: p. 956 OBJ: 1 TOP: Thyroid Storm KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. What is the most appropriate nursing concern for the patient recently diagnosed with hyperthyroidism? a. Hypothermia b. Constipation c. Disturbed body image d. Disturbed sleep pattern ANS: D The patient with hyperthyroidism has trouble staying asleep because of the metabolic disorder. Persons with hyperthyroidism feel uncomfortably warm, which also contributes to their sleeping difficulty. DIF: Cognitive Level: Application REF: p. 951 OBJ: 1 TOP: Hyperthyroidism KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A patient, newly diagnosed with hypothyroidism, is anxious to begin her drug regimen. What should the nurse’s instructions relative to hormone replacement include? a. “Be certain that no dose is skipped.” b. “Be sure and take these drugs just before bedtime.” c. “Know the signs and symptoms of hyperthyroidism.” d. “You will be able to notice the benefits of thyroid replacement therapy right away.” ANS: C Overdosing on the thyroid replacement medication will lead to signs and symptoms of hyperthyroidism. The medication is best taken every morning so as not to unduly interrupt sleep patterns. DIF: Cognitive Level: Application REF: p. 951 OBJ: 2 TOP: Thyroid Replacement Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 8. What patient recommendation should a nurse include when preparing to present presurgical teaching of a patient scheduled for a subtotal thyroidectomy? a. Lie flat on her back for 24 hours to prevent undue strain on the suture line. b. Be able to verbalize the signs and symptoms of thyroid crisis. c. Demonstrate how to deep breathe and support her head during position changes. d. Have a tube in her trachea to assist in breathing. ANS: C Teaching the patient to hold and support the head after a thyroidectomy will ease the postoperative period. Consistently supporting the head will prevent stress on the suture line. DIF: Cognitive Level: Application REF: p. 953 OBJ: 2 TOP: Thyroidectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. On returning from surgery after undergoing a thyroidectomy, a patient is alarmed about the large tracheostomy tray on the bedside table. What is the nurse’s most reassuring response when the patient asks why it is there? a. “We have it there as a precautionary measure in the unlikely event that you have difficulty breathing.” b. “If you start bleeding, we’ll be able to take care of it right here at the bedside.” c. “We have to keep it there in case of an emergency and the physician needs it.” d. “It’s hospital policy to have it available for persons who are likely to have respiratory arrest.” ANS: A The honest answers without any embellishments are best. Suggesting that any emergency is imminent will alarm the patient further. The presence of the tray is an item that should be covered in preoperative teaching. DIF: Cognitive Level: Comprehension REF: p. 955 OBJ: 1 TOP: Postoperative Care: Thyroidectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. What is the appropriate action of the nurse when assessing for hemorrhage in a post-thyroidectomy patient? a. Assess upper chest for the patient positioned in high Fowler position. b. Turn the patient to the side to check; the patient must be kept flat in the bed. c. Lift up the neck dressing to assess for excessive bleeding. d. Examine behind patient’s neck and upper back to assess for hemorrhage. ANS: D Because the dressing is on the front of the neck, blood might flow under the dressing to the back of the neck, since it flows to the most-dependent position. Patients are positioned in a high Fowler position after a thyroidectomy to diminish swelling. DIF: Cognitive Level: Application REF: p. 954 OBJ: 1 TOP: Post-thyroidectomy Care KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity 11. How do foods such as soybeans, turnips, and rutabagas affect people with thyroid disorders? a. Suppress thyroid hormone. b. Decrease the hypothermia of the person with hypothyroidism. c. Supplement the diet of a person with hypothyroidism. d. Counteract the effect of iodide therapy. ANS: A Turnips, rutabagas, and soybeans are goitrogen substances that suppress the thyroid hormone. Such foods would synergize iodides and increase the symptoms of the patient with hypothyroidism. DIF: Cognitive Level: Comprehension REF: p. 957 OBJ: 1 TOP: Goitrogen Substances KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. A nurse taking the blood pressure of a patient who had a total thyroidectomy 2 days earlier notes that the patient’s hand goes into a carpopedal spasm. What should the nurse recognize this movement as an indication of? a. Hyperkalemia, called the Allen sign b. Hypernatremia, called the Hogan sign c. Hypocalcemia, called the Trousseau sign d. Hypokalemia, called the Chvostek sign ANS: C The carpopedal spasm is the Trousseau sign, which indicates hypercalcemia. Chvostek sign also signals hypocalcemia. DIF: Cognitive Level: Application REF: p. 961 OBJ: 1 TOP: Hypothyroidism KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. What action should a nurse implement to address dry skin in the patient with hypothyroidism? a. Increase the frequency of bathing to get rid of dry skin. b. Apply lotions and creams to help maintain moisture. c. Increase activities to stimulate circulation in the skin. d. Take antihistamines to prevent itching. ANS: B The skin requires moisturizing lotion to decrease the risk breakdown. Frequent bathing and antihistamines will dry the skin. Exercise does little for skin perfusion. DIF: Cognitive Level: Application REF: p. 960 OBJ: 1 TOP: Hypothyroidism KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 14. What action should a nurse implement to initiate the Chvostek sign? a. Ask the patient to grimace and note if the facial response is symmetrical. b. Inflate a blood pressure cuff to the systolic level and watch for a carpopedal spasm. c. Tap the face over the facial nerve and watch for a spasm of the facial muscle. d. Check the pupillary response to light and determine whether the pupil accommodates and reacts. ANS: C Spasm of the facial muscles is an indicator of low serum calcium levels. DIF: Cognitive Level: Application REF: p. 956 OBJ: 1 TOP: Hypocalcemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 15. What symptoms should a nurse anticipate in the history of a patient with hyperparathyroidism? a. Fatigue, hyperactive reflexes, muscle cramps, and twitching b. Poor muscle tone, bone pain, urinary calculi, and fractures c. Hunger, thirst, and urinary retention d. Tachycardia, air hunger, and nervousness ANS: B The calcium has been leeched from the bones, leading to hypercalcemia and leaving the patient with multiple problems such as a risk for fractures, urinary calculi, and bone pain. DIF: Cognitive Level: Comprehension REF: p. 962 OBJ: 1 TOP: Hyperparathyroidism KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 16. What is the priority nursing concern for a patient with hyperparathyroidism? a. Potential urinary obstruction b. Decreased cardiac output c. Potential for injury d. Inadequate nutrition ANS: A Excessive calcium in the bloodstream leads to the formation of calcium stones in the urinary system. DIF: Cognitive Level: Application REF: p. 962 OBJ: 1 TOP: Hyperparathyroidism KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. What is the nurse aware is happening when the patient with hypoparathyroidism complains of fatigue and a lack of energy? a. Hypertension is the cause of the fatigue. b. Hypocalcemia has caused decreased cardiac output. c. Dyspnea has sapped the patient’s energy. d. Poor muscle tone makes any activity tiring. ANS: B A decreased amount of calcium in the bloodstream decreases the contractility of the heart and, consequently, reduces cardiac output. DIF: Cognitive Level: Comprehension REF: p. 962 OBJ: 1 TOP: Hypoparathyroidism KEY: Nursing Process Step: Nursing Diagnosis MSC: NCLEX: Physiological Integrity: Physiological Adaptation 18. Which intervention is necessary to assist a patient with hypothyroidism to understand how he can live a full and normal life? a. Teach the importance of taking antithyroid medication until it is no longer needed. b. Encourage exercise to burn extra calories and maintain a normal weight. c. Teach him to take care of energy needs through adequate nutrition. d. Encourage treatment with thyroid replacement therapy. ANS: D Hormones can adequately and effectively replace the missing thyroid hormone. DIF: Cognitive Level: Application REF: p. 958 OBJ: 2 TOP: Hypothyroidism: Pharmacology KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. Why are antithyroid medications provided presurgically to a patient with hyperthyroidism? (Select all that apply.) a. To decrease the level of hormone in the blood before surgery b. To help reduce the risk of hemorrhage during surgery c. To decrease the threat of a thyroid storm d. To reduce exophthalmia e. To increase weight ANS: A, B, C, D The antithyroid medication will do all of the above except increasing weight in a patient with hyperthyroidism. DIF: Cognitive Level: Comprehension REF: p. 953 OBJ: 1 TOP: Presurgical Use of Antithyroid Drugs KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. What should a nurse caring for a patient with hyperthyroidism include when developing a plan of care? (Select all that apply.) a. Decreasing weight b. Provision of a cool environment c. Eye care d. Nutritional support e. Prevention of diarrhea ANS: B, C, D, E A patient with hyperthyroidism does not need to lose weight, but he or she needs to gain it. All other options are appropriate concerns for such a patient. DIF: Cognitive Level: Application REF: p. 958 OBJ: 2 TOP: Care Plan for Patient Hyperthyroidism KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort COMPLETION 1. To meet the nutritional needs of a patient with Graves disease, the nurse recommends a diet of 4,000 to calories. (Use numeric characters only, no punctuation.) ANS: 5000 The patient with Graves disease has a high metabolism, which requires a large caloric intake. These patients need 4000 to 5000 calories a day. DIF: Cognitive Level: Knowledge REF: p. 954 OBJ: 1 TOP: Nutritional Needs of the Patient with Graves Disease KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. Congenital hypothyroidism, if left untreated, will result in . ANS: cretinism Cretinism is the result of untreated congenital hypothyroidism. DIF: Cognitive Level: Knowledge REF: p. 960 OBJ: 1 TOP: Cretinism KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 50: Diabetes and Hypoglycemia Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse explains that type 1 diabetes mellitus is a disease in which the body does not produce enough insulin. What is the reason that the blood glucose is elevated? a. Prolonged elevation of stress hormone (cortisol, epinephrine, glucagon, growth hormone) levels b. Malfunction of the glycogen-storing capabilities of the liver c. Destruction of the beta cells in the pancreas d. Insulin resistance of the receptor cells in the muscle tissue ANS: C Type 1 diabetes mellitus is a disease in which the pancreas does not produce adequate insulin because of the destruction of beta cells. DIF: Cognitive Level: Comprehension REF: p. 968 OBJ: 2 TOP: Type 1 Diabetes Mellitus KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A patient newly diagnosed with type 2 diabetes mellitus asks the nurse why she has to take a pill instead of insulin. The nurse explains that in type 2 diabetes mellitus, the body still makes insulin. What other information is pertinent for the nurse to relay? a. Overweight and underactive people cannot simply use the insulin produced. b. Metabolism is slowed in some people, so they have to take a pill to speed up their metabolism. c. Sometimes the autoimmune system works against the action of the insulin. d. The cells become resistant to the action of insulin. Pills are given to increase the sensitivity. ANS: D Type 2 diabetes mellitus is a disease in which the cells become resistant to the action of insulin and the blood glucose level rises. Oral hyperglycemic agents make the cells more sensitive. DIF: Cognitive Level: Comprehension REF: pp. 981-982 OBJ: 2 TOP: Type 2 Diabetes Mellitus KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A patient tells a nurse that she eats “huge” amounts of food but stays hungry most of the time. What should the nurse explain as the cause of hunger experienced by persons with type 1 diabetes? a. Excess amount of glucose b. Need for additional calories to correct the increased metabolism c. Fact that the cells cannot use the blood glucose d. Need for exercise to stimulate insulin secretion ANS: C The cells cannot use the glucose without insulin, so the patient with diabetes still feels hungry even though abundant glucose is circulating in the blood. DIF: Cognitive Level: Comprehension REF: p. 968 OBJ: 1 TOP: Hunger in the Patient with Diabetes KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. What does the lack of insulin in patients with type 1 diabetes cause that increases the risk for cardiovascular disorders? a. High glucose levels that irritate and shrink the vessels b. Inadequate metabolism of proteins, which causes ketosis c. Increased fatty acid levels d. Increased metabolism of ketones, which causes hypertension ANS: C The increase in fatty acid levels causes an increase in the level of triglycerides and an attendant rise in low-density lipoprotein levels. DIF: Cognitive Level: Knowledge REF: pp. 968-969 OBJ: 1 TOP: Diabetes: Complications KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. The self-care goal of a patient with diabetes is to keep the blood sugar within normal limits. What causes hyperglycemia to occur? a. Blood glucose levels rise, stimulating the production of insulin. b. Insulin conversion of glycogen to glucose is inhibited. c. The body responds to glucose-starved tissues by changing stored glycogen into glucose. d. Glycogen is unable to be stored in the liver and muscles. ANS: C The hypothalamus is receiving a message that the cells need glucose, so it responds by adding more glucose to the already overburdened blood. DIF: Cognitive Level: Comprehension REF: p. 968 OBJ: 1 TOP: Hyperglycemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A young patient complains that diabetes is causing her to “have no life at all. It’s too hard.” What is the most helpful response by the nurse? a. “Yes, you must make some sacrifices.” b. “It’s hard, but with significant alterations in your lifestyle, you can live a long life.” c. “What’s hard about exercise, diet, and medicine?” d. “Let’s talk about what makes it so hard.” ANS: D Involving the patient in decisions about how she will cope with her diabetes will make the goals more realistic and personal, which will give her a greater chance of success in meeting them. DIF: Cognitive Level: Application REF: p. 990 OBJ: 7 TOP: Diabetes Lifestyle KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 7. When a patient with type 2 diabetes says, “Why in the world are they looking at my hemoglobin? I thought my problem was with my blood sugar.” What should the nurse explain about the level of hemoglobin A1c? a. Shows how a high level of glucose can cause a significant drop in the hemoglobin level b. Shows what the glucose level has done during the past 3 months c. Indicates a true picture of the patient’s nutritional state d. Reflects the effect of a high level of glucose on the ability to produce red blood cells (RBCs) ANS: B By analyzing the amount of glucose bound to the hemoglobin, the level of blood glucose can be evaluated for the past 3 months because the glucose stays bound to the hemoglobin for the life of the RBC. DIF: Cognitive Level: Comprehension REF: p. 983 OBJ: 1 TOP: Hemoglobin A1c: Glycosylated Hemoglobin Level KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. A patient with type 2 diabetes shows a blood sugar reading of 68 at 6 AM. What action should the nurse implement based on the reading of 72 mg/dL? a. Notify the charge nurse of the reading. b. Give regular insulin per a sliding scale. c. Give him 8 oz of skim milk. d. Administer the oral glucose tablet. ANS: C The patient is hypoglycemic and needs an immediate source of glucose, such as milk or orange juice. The oral hypoglycemic agent will not work quickly enough. The charge nurse can be notified later. Giving insulin per a sliding scale would lower the blood sugar level. DIF: Cognitive Level: Application REF: p. 991 OBJ: 6 TOP: Hypoglycemic Reaction KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. A nurse assigned to care for a patient with diabetic ketoacidosis (DKA) is aware that this is a life-threatening condition. What will DKA result in? a. Disorder of carbohydrates, fats, and proteins metabolism b. Storage of glycogen, resulting in a severe shortage of glucose in the bloodstream c. Dangerously elevated pH and bicarbonate levels in the blood d. Severe hypoglycemia, which can result in coma and convulsions ANS: A DKA is mainly related to the use of fat as an energy source because of an inability of the body to use glucose. The metabolism of fat produces ketones. DIF: Cognitive Level: Knowledge REF: p. 973 OBJ: 4 TOP: Diabetic Ketoacidosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. A patient has been admitted to the hospital with the diagnosis of DKA. What vital signs should a nurse anticipate that the patient will exhibit? a. Temperature, 99 F; pulse, 62 beats/min; respirations, 16 breaths/min and shallow b. Temperature, 98.6 F; pulse, 76 beats/min; respirations, 16 breaths/min and deep c. Temperature, 98 F; pulse, 84 beats/min; respirations, 18 breaths/min and shallow d. Temperature, 97.4 F; pulse, 110 beats/min; respirations, 26 breaths/min and deep ANS: D DKA is caused by the attempt of the body to metabolize fat for energy, which results in an acidotic state. The classic signs of DKA are hypothermia, tachycardia, and Kussmaul respirations (rapid and deep) to blow off the acid ions via respirations. The respirations will have a fruity odor. DIF: Cognitive Level: Analysis REF: p. 973 OBJ: 4 TOP: Diabetic Ketoacidosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. A home health care nurse is assessing a patient with type 1 diabetes who has been controlled for 6 months. The nurse is surprised and concerned about a blood glucose reading of 52 mg/dL. What action by this patient most likely caused this episode of hypoglycemia? a. Taking a new form of birth control pill this morning b. Using large amounts of sugar substitute in her tea this morning c. A 2-hour long exercise class at the spa this morning d. Administering an insufficient dose of insulin this morning ANS: C Excessive exercise used up the glucose that was made available by the insulin taken by the patient. The patient now has too much insulin for the available glucose and has become hypoglycemic. DIF: Cognitive Level: Application REF: p. 977 OBJ: 6 TOP: Diabetes: Treatment KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. As part of a teaching plan in preparation for discharge, a patient with type 1 diabetes needs guidelines for exercise. Which guideline should be included? a. Plan exercise so that it coincides with the peak action of insulin. b. Insulin should be injected into the lower extremity before exercise because that site provides the greatest absorption. c. Exercise should be performed daily at the same time of day and at the same intensity. d. Keep exercise at a minimum to conserve your energy. ANS: C If the body is using more glucose than available, the body will draw on fatty acids, which will give off ketones. DIF: Cognitive Level: Application REF: p. 977|p. 900 OBJ: 7 TOP: Exercise KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 13. A patient has come into the emergency department accompanied by a friend who states that the patient had been acting very strangely and seems confused. The friend states that the patient has diabetes and takes insulin. Which signs of hypoglycemia might the nurse assess? a. Slow pulse rate and low blood pressure b. Irritability, anxiety, confusion, and dizziness c. Flushing, anger, and forgetfulness d. Sleepiness, edema, and sluggishness ANS: B When blood sugar levels fall, hormones are activated to increase serum glucose. One of the hormones is epinephrine, which causes these symptoms. DIF: Cognitive Level: Comprehension REF: p. 991 OBJ: 1 TOP: Hypoglycemia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A patient has come to the physician’s office after finding out that her blood glucose level was 135 mg/dL. She states that she had not eaten before the test and was told to come and see her physician. She asks the nurse if she has diabetes. What is the most accurate nursing response? a. “Having a fasting serum glucose that high certainly indicates diabetes.” b. “That test indicates that we need to perform more tests that are specific for diabetes.” c. “How do you feel? Do you have any other signs of diabetes?” d. “Do you have a family history of diabetes, stroke, or heart disease? We need to know before making a diagnosis.” ANS: B The nurse needs to answer the patient’s question in a way that gives information and is not misleading. Although 135 mg/dL is high, a nonpathologic explanation may be found. More tests should be performed to evaluate the patient. DIF: Cognitive Level: Comprehension REF: p. 975 OBJ: 9 TOP: Laboratory Tests for Diabetes KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 15. A nurse is formulating a teaching plan for a 22-year-old woman taking rosiglitazone (Avandia). What should the nurse include information about in this plan to caution this patient? a. Decreased effectiveness of her birth control pills b. Excessive exposure to the sun c. Sudden drop in blood pressure with dizziness d. Possible severe diarrhea ANS: A Avandia causes some birth control pills to be less effective. DIF: Cognitive Level: Application REF: p. 982 OBJ: 10 TOP: Side Effects of Avandia KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 16. A patient with type 1 diabetes has an insulin order for NPH insulin, 35 U, to be given at 0700. The patient has also been instructed not to take anything by mouth (NPO) in preparation for laboratory work that will not be drawn until 1000. What action should the nurse implement? a. Give the insulin as ordered. b. Give the insulin with a small snack. c. Inform the charge nurse. d. Hold the insulin until after the blood draw. ANS: D Holding the insulin to adhere to the NPO order is appropriate. The patient will not be getting food until after the laboratory work; consequently, the insulin will not be needed until then. Giving the insulin as ordered will create a possibility of hypoglycemia before the blood is drawn. Giving a snack to a patient who is NPO is inappropriate. DIF: Cognitive Level: Application REF: p. 986 OBJ: 8 TOP: Insulin with NPO Order KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 17. A patient comes to the diabetes clinic and confides to the nurse that she does not follow the diet exchange program that she was given. What is the best response by the nurse? a. “The exchange program is a carefully developed and very important program that allows you to take control of your disease.” b. “A lot of people have trouble with that program. You aren’t the first one to go off your diet.” c. “We had better check your blood work to see what you’ve done to yourself.” d. “Okay. Let’s talk about what you do eat and drink and how you manage your diabetes.” ANS: D To evaluate the effectiveness of treatment, the nurse must first find out how the patient perceives the importance of diet, drugs, and exercise. DIF: Cognitive Level: Application REF: p. 990 OBJ: 8 TOP: Nutrition KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 18. A patient with type 1 diabetes asks why his 0700 insulin has been changed from NPH insulin to 70/30 premixed insulin. What is the best explanation by the nurse that explains about 70/30 insulin mixture? a. It is absorbed more rapidly into the bloodstream. b. It has no peak action time and lasts all day. c. It makes insulin administration easier and safer. d. It provides a bolus of rapid-acting insulin to prevent hyperglycemia after breakfast. ANS: C 70/30 insulin is 30% rapid-acting insulin and 70% intermediate-acting insulin. The rapid action of the 0700 premixed insulin prevents hyperglycemia after the morning meal and the mixed drug reduces the risk of error in drawing up two insulins. DIF: Cognitive Level: Comprehension REF: p. 978 OBJ: 8 TOP: Use of 70/30 Insulin KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 19. What should a nurse include when drawing up a patient’s diabetes teaching plan? a. Develop an exercise plan because regular exercise helps control blood glucose levels. b. Monitor blood sugar levels only if not feeling well to ensure that the fingertips are not pricked too much. c. If nervousness, palpitations, or hunger is experienced, take a small dose (1 to 2 U) of regular insulin and call the physician. d. Use over-the-counter measures for any foot blisters, calluses, or wounds before seeking medical help. ANS: A Exercise is an integral part of the patient’s ability to take charge of his or her diabetes and needs to be included in the teaching plan. DIF: Cognitive Level: Application REF: p. 977|p. 990 OBJ: 8 TOP: Diabetes Teaching Plan KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. What has most likely occurred in a patient who has been diagnosed with endogenous hypoglycemia? a. Taken an overdose of hypoglycemic drugs b. Been following a very restricted fasting diet or is malnourished c. Excessive secretion of insulin or an increase in glucose metabolism d. Exercised unwittingly without replenishing needed fluids and nutrients ANS: C Endogenous refers to within; in this patient, it refers to internal factors, such as an increase of insulin or glucose metabolism. Both conditions would lead to hypoglycemia. DIF: Cognitive Level: Application REF: p. 991 OBJ: 1 TOP: Hypoglycemia KEY: Nursing Process Step: Evaluation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 21. How long does it take for Humulin R 20 units to peak? a. 15 minutes b. 30 minutes c. 1 hour d. 2 hours ANS: D Humulin R has its onset in approximately 30 minutes, but its peak is in 2 hours. DIF: Cognitive Level: Knowledge REF: p. 979 OBJ: 8 TOP: Humulin R Insulin Peak KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 22. A nurse suspects that a patient with type 1 diabetes may be experiencing the Somogyi phenomenon. What symptom supports this suspicion? a. Headache on awakening and enuresis b. 6 AM blood sugar of 58 mg/dL and nausea c. Abdominal pain and elevated blood pressure d. Drowsiness and disorientation after eating ANS: A The Somogyi phenomenon occurs because of a rebound hyperglycemia after a period of hypoglycemia during the early morning. The patient wakes with a headache, enuresis, nausea and vomiting, nightmares, and a high level of blood sugar. DIF: Cognitive Level: Comprehension REF: p. 983 OBJ: 8 TOP: Somogyi Phenomenon KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 23. A patient has been admitted with hyperglycemic hyperosmolar nonketotic syndrome (HHNS). The blood glucose level is very high (880 mg/dL) on admission. The physician believes that the condition is the result of large amounts of glucose solutions administered intravenously (IV) during renal dialysis. What should the nurse anticipate that the patient would exhibit? a. Fruity breath and a high level of ketones in her urine b. Severe dehydration and hypernatremia caused by the hyperglycemia c. Exactly the same symptoms and signs as DKA d. Kussmaul respirations, nausea, and vomiting ANS: B IV solutions containing glucose bypass the digestive system; consequently, the pancreas is not triggered to release insulin. However, just enough insulin is present to prevent the breakdown of fatty acids and the formation of ketones. DIF: Cognitive Level: Application REF: pp. 974-975 OBJ: 5 TOP: Hyperglycemic Hyperosmolar Nonketotic Syndrome KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. What are functional causes of hypoglycemia? (Select all that apply.) a. Dumping syndrome b. Overdose of insulin c. Addison disease d. Prolonged muscular exercise e. Chronic alcoholism ANS: A, C, D Dumping syndrome, Addison disease, and prolonged exercise are functional causes of hypoglycemia. Overdose of insulin and chronic alcoholism are exogenous causes. DIF: Cognitive Level: Knowledge REF: p. 991 OBJ: 1 TOP: Functional Causes of Hypoglycemia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What should a teaching plan about foot care include for a patient with diabetes? (Select all that apply.) a. Wash and carefully dry the feet every day. b. Apply lotion between the toes. c. Protect the feet from extreme temperatures. d. Walk barefoot only indoors. e. Buy shoes that are comfortable and supportive. ANS: A, C, E Washing, inspecting, and drying the feet, especially between the toes, are essential. Protecting the feet from heat and cold and wearing supportive shoes are important to good foot health. Lotion can be applied to the soles and tops of the feet but not between the toes. Walking barefoot is contraindicated for a person with diabetes. DIF: Cognitive Level: Knowledge REF: pp. 971-972 OBJ: 5 TOP: Foot Care KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A teaching plan for a patient with diabetes is focused on smoking cessation and the control of hypertension for the avoidance of microvascular complications. What are examples of microvascular complications? (Select all that apply.) a. Macular degeneration b. End-stage renal disease (ESRD) c. Coronary artery disease (CAD) d. Peripheral vascular disease (PVD) e. Cerebrovascular accident (CVA) ANS: A, B Macular degeneration and ESRD are both microvascular complications. CAD, PVD, and CVA are all macrovascular complications. DIF: Cognitive Level: Comprehension REF: p. 970 OBJ: 5 TOP: Microvascular Complications KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. How is the Whipple triad described? (Select all that apply.) a. Symptoms of hypoglycemia are present. b. Low blood glucose levels are documented when symptoms are present. c. Symptoms can be reproduced with an injection of regular insulin, 10 units. d. Muscular activity does not have any effect on blood glucose. e. Symptoms improved when the blood glucose level rises. ANS: A, B, E Whipple triad is the presence of the symptoms of hypoglycemia (e.g., diaphoresis, pallor, tachycardia), the documentation of low blood glucose levels when symptoms are present, and the improvement of symptoms as the blood glucose level rises. DIF: Cognitive Level: Comprehension REF: p. 991 OBJ: 9 TOP: Whipple Triad KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. A nurse reminds a patient with type I diabetes to rotate the insulin injection sites to prevent . ANS: lipohypertrophy Using the same area for insulin injections causes swollen lumpy areas that interfere with the absorption of insulin. DIF: Cognitive Level: Comprehension REF: p. 980 OBJ: 5 TOP: Lipohypertrophy KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse instructs a patient about how insulin affects blood glucose. (Arrange the events in sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Beta cells are stimulated to release insulin. b. Glucose enters the bloodstream. c. Glycogen is converted to glucose by alpha cells (glycogenesis). d. Glycogen is stored in the liver. e. Insulin transports glucose to muscle cells. ANS: BAEDC Insulin transports the glucose to muscle cells or converts it to glycogen, which is stored in the liver to be accessed when hypoglycemia occurs. DIF: Cognitive Level: Analysis REF: pp. 967-968 OBJ: 3 TOP: Insulin’s Effect on Glucose KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 51: Female Reproductive System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Which potential side effect should a nurse caution a patient who is taking danazol (Danocrine), an androgenic steroid, for the treatment of menorrhagia to be prepared for? a. Heavy menses b. Masculinizing c. Acnelike skin eruptions d. Anemia ANS: B Androgenic steroids cause masculinizing. The distressing signs are a deepening voice, development of chest hair, coarsening of the skin, clitoral enlargement, and hot flashes. Many patients reject the drug on the basis of these side effects. DIF: Cognitive Level: Knowledge REF: p. 1009 OBJ: 3 TOP: Androgenic Steroid Therapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. What instruction should a nurse provide to a patient after a culdoscopy? a. Clean the incision site daily with hydrogen peroxide. b. Avoid vaginal intercourse. c. Return to the clinic for suture removal in 7 days. d. Use tampons. ANS: B Nothing should be inserted into the vagina (e.g., intercourse, tampons) for the time specified by the physician. No incision or sutures are present. DIF: Cognitive Level: Application REF: p. 1003 OBJ: 2 TOP: Culdoscopy KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A patient asks a nurse, “Will the laparoscopy be painful?” What is the best reply by the nurse? a. “You will probably have some pain below the rib cage and around the shoulder.” b. “Most patients state that the procedure is painless during and afterward.” c. “You may have some mild to moderate pain around the umbilicus and in the back.” d. “Every person is different. It’s difficult to say whether you’ll have pain.” ANS: A During the immediate postoperative period, the patient tends to experience pain below the rib cage and in the shoulder area from the air injected into the abdominal cavity. The air is absorbed in 24 hours, and the pain disappears. DIF: Cognitive Level: Application REF: p. 1003 OBJ: 2 TOP: Laparoscopy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. A nurse is instructing a patient on breast self-examination. When is the best time of the month to instruct this patient to perform a breast self-examination? a. Before the menstrual period b. During the menstrual period c. After the menstrual period d. On the first day of the month ANS: C Breast self-examination should be performed at the same time each month, at the end of the menstrual cycle. DIF: Cognitive Level: Knowledge REF: p. 1004 OBJ: 2 TOP: Breast Self-Examination KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. Conjugated estrogen (Premarin) is indicated for treatment of menopause. Which side effects should a nurse explain before administering the medication to a woman who has just had a hysterectomy? a. Breast tenderness b. Hypotension c. Arthralgia d. Skin rash ANS: A A side effect of conjugated estrogen (Premarin) is breast tenderness. DIF: Cognitive Level: Comprehension REF: p. 1007 OBJ: 3 TOP: Drugs Used to Treat Menopause KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 6. A female student, seen in the campus clinic, states that she uses feminine hygiene douches every day and after intercourse. What is the best response from the nurse? a. “Douching has been used as an effective means of birth control for years.” b. “Commercially prepared douches will neutralize the female vaginal tract.” c. “Douching should only be done when ordered by a physician or nurse practitioner.” d. “Douching protects the vaginal tract from microorganisms.” ANS: C Women should not douche unless it is ordered by a physician or nurse practitioner. DIF: Cognitive Level: Comprehension REF: p. 1005 OBJ: 4 TOP: Douching KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. Which medication is used to stimulate or mimic actions of natural pituitary gonadotropins in the treatment of infertility? a. Estrogen only (diethylstilbestrol) b. Danazol (Danocrine) c. Clomiphene citrate (Clomid) d. Raloxifene (Evista) ANS: C Clomid stimulates the actions of natural pituitary gonadotropins. DIF: Cognitive Level: Knowledge REF: p. 1010 OBJ: 4 TOP: Ovulatory Stimulant Drugs KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies COMPLETION 1. The nurse recommends that an annual mammogram be performed for women older than years of age. (Use numeric characters only.) ANS: 45 The American Cancer Society (ACS) recommends that mammograms be obtained in women at the age of 45 years with subsequent testing done annually thereafter until age 54 at which time the woman may be transitioned to biennial screening or continued annually for as long as they are otherwise in good health (ACS, 2015). DIF: Cognitive Level: Knowledge REF: p. 1003 OBJ: 2 TOP: Mammograms KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 52: Female Reproductive Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is teaching a health class for 12- and 13-year-old girls about routine vaginal hygiene. What should the nurse be sure to include? a. Wear clean polyester panties daily and at night. b. Douche weekly with a mild vinegar solution. c. Wash the external and internal genitalia daily. d. Wipe the perineal–anal area from front to back. ANS: D Transfer of Escherichia coli from the anus to the vagina or to the urinary system can be avoided by wiping the perineal–anal area from front to back. DIF: Cognitive Level: Comprehension REF: p. 1017|p. 1021 OBJ: 2 TOP: Infections of the Reproductive Tract KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse is teaching patients with endometriosis. What signs and symptoms of common complications should be included? a. Pelvic inflammatory disease b. Obstruction of the bowel and ureters c. Cancer of the endometrium d. Ovarian cancer ANS: B A common complication of endometriosis is obstruction of bowel, ureters, or both, from the endometrial deposits, creating a medical emergency. DIF: Cognitive Level: Knowledge REF: p. 1023 OBJ: 1 TOP: Endometriosis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. After a mastectomy, many patients experience lymphedema. What action can the patient take to minimize this problem? a. Keep the arm elevated as much as possible. b. Take Lasix, 20 mg twice daily as ordered. c. Use a sling during the day to rest the arm. d. Avoid exercising the arm for several weeks. ANS: A To manage lymphedema, the patient should elevate the arm to a height above the level of the heart. DIF: Cognitive Level: Comprehension REF: p. 1037 OBJ: 2 TOP: Postoperative Care for Mastectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A patient tells a nurse that she is afraid of getting cervical cancer because her mother died of cervical cancer. What is the most appropriate response by the nurse? a. “You need to a have a pelvic examination every 6 months because of your history.” b. “If you have regular Pap stain, cervical cancer is usually diagnosed early and cured.” c. “There’s no need to worry so much. Cervical cancer does not run in families.” d. “Cervical cancer is sexually transmitted. Don’t switch partners often, and you don’t have to worry.” ANS: B For patients who have regular annual pelvic examinations and Papanicolaou (Pap) stain, cervical cancer is usually diagnosed and treated in its early stage. DIF: Cognitive Level: Comprehension REF: p. 1038 OBJ: 2 TOP: Cervical Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A nurse is caring for a patient after a modified radical mastectomy for a breast tumor that has been determined to be positive for estrogen receptors (ER positive) and has been placed on a protocol of tamoxifen. The patient then asks the nurse, “Do you think I should take this medication?” Which statement is the most appropriate? a. “Tamoxifen will probably not be effective because your tumor was ER positive.” b. “If I were you, I would do what the physician recommends.” c. “I think that you should take tamoxifen, because the tumor was ER positive.” d. “Tamoxifen is an option to consider, because your tumor was ER positive.” ANS: D For tumors that are ER positive, tamoxifen citrate may be prescribed because such drugs interfere with estrogen production. ER-positive tumors need estrogen to grow. DIF: Cognitive Level: Comprehension REF: p. 1034 OBJ: 2 TOP: Drugs Used in Treatment for Breast Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 6. A 16-year-old girl seen in the student health clinic has been diagnosed with Trichomonas vaginalis and given medication for the infection. What should a nurse explain about treatment of the girl’s sexual partner? a. He will require a 1-day treatment with the same drug. b. He will not develop the infection or require treatment. c. He will be treated, although he is asymptomatic. d. He is required by law to be examined by a physician. ANS: C The woman’s sexual partner(s) may be treated for some infections to avoid reinfection. DIF: Cognitive Level: Comprehension REF: p. 1017 OBJ: 1 TOP: Trichomonas vaginalis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. A patient makes an appointment with her gynecologist because she is having difficulty conceiving. Which laboratory test should the nurse anticipate the physician will order? a. Complete blood count b. Progesterone level c. Prothrombin time d. Erythrocyte count ANS: B Evaluation of the female partner includes basal body temperature, serum progesterone level, and endometrial biopsy to assess for infertility. DIF: Cognitive Level: Comprehension REF: p. 1043 OBJ: 1 TOP: Infertility Diagnostic Tests KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. What action should a nurse implement when assessing for abnormal bleeding in a patient following a hysterectomy? a. Record the number of perineal pads used. b. Assess vital signs every 8 hours. c. Place the patient’s bed in a high Fowler position. d. Apply an abdominal binder. ANS: A Recording the number of pads used and the appearance of the discharge is primary in posthysterectomy care. The abdominal dressing and perineal pad are checked every hour for the first 12 hours. Any excess bleeding is reported. The patient should be placed on her side in a semi-Fowler position. An abdominal binder, if used, has no effect on hemorrhage. DIF: Cognitive Level: Application REF: p. 1027 OBJ: 1 TOP: Hysterectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. A nurse collecting data on the reproductive system from a female patient is told that the patient has a vaginal discharge that is cottage cheese–like in appearance. What should the nurse recognize this as a common sign of? a. Pelvic inflammatory disease (PID) b. Trichomonas vaginalis infection c. Atrophic vaginitis d. Candida albicans infection ANS: D Candida albicans infection has a distinctive odor and a cottage cheese–like appearance. DIF: Cognitive Level: Comprehension REF: p. 1016 OBJ: 1 TOP: Sexually Transmitted Infections KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. What must be true for a woman to be diagnosed with primary infertility? a. She has never been able to conceive after 1 year of regular, unprotected sex. b. She conceived once but did not deliver a viable infant. c. She conceived once but was unable to conceive again. d. She conceived three times in 1 year without a viable birth. ANS: A To be diagnosed with infertility, the patient must have been unable to conceive after 1 year of regular, unprotected sex. Primary infertily is when the woman has never conceived; secondary infertility refers to a woman who has conceived at least once but is unable to conceive again. All other options are definitions of secondary infertility. DIF: Cognitive Level: Comprehension REF: p. 1042 OBJ: 1 TOP: Infertility KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 11. A patient is admitted with possible cancer of the ovary. What fact should a nurse know about malignant tumors of the ovary? a. They are frequently advanced and inoperable by the time they are diagnosed. b. The respond well to radiation and chemotherapy because of early detection. c. They are easily detected because symptoms appear early in a woman’s life. d. They are directly related to PID and other infections. ANS: A The high mortality rate for women with ovarian cancer is due to the fact that a malignant tumor of the ovary is asymptomatic until it is advanced. DIF: Cognitive Level: Knowledge REF: p. 1039 OBJ: 1 TOP: Ovarian Cancer KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. A mastectomy care plan should address psychosocial problems of the patient. What should this be directed toward? a. Caring for the wound and dressings b. Finding an appropriate support group c. Educating for methods for controlling edema d. Helping the patient express feelings and concerns ANS: D The nurse should gently explore how the patient is feeling about the surgery and encourage her to express her concerns. The other options are significant care concerns but are not psychosocial in nature. DIF: Cognitive Level: Comprehension REF: p. 1037 OBJ: 2 TOP: Breast Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 13. A nurse reads that a patient’s breast tumor is a stage II. What should the nurse realize about this tumor? a. It is smaller than 2 cm, with no positive lymph node involvement and no metastasis evident. b. It measures between 2 and 5 cm, with no or one positive lymph node involvement and no metastasis evident. c. It is larger than 5 cm, with no positive lymph node involvement and no metastasis evident. d. It measures between 2 and 5 cm, with positive axillary lymph node involvement and metastasis evident. ANS: B A stage II tumor is between 2 and 5 cm with no or one lymph node positive for cancer and no metastases present. All other options are for different stages of tumors. DIF: Cognitive Level: Comprehension REF: p. 1036 OBJ: 1 TOP: Staging of a Breast Tumor KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. A nurse teaching a seminar on breast cancer lists the signs that would alert a woman to the possibility of a tumor. What should those signs include? (Select all that apply.) a. Dimpling b. Nipple discharge c. Thickening of tissue d. Red bruise e. Dry rash around nipple ANS: A, B, C, E Signs of breast cancer that should be investigated are dimpling of the skin of the breast, any discharge from the nipple, any thickening of breast tissue, or a dry rash in the areola. Although it should be investigated, bruising is not a classic sign of breast cancer. DIF: Cognitive Level: Knowledge REF: p. 1034 OBJ: 1 TOP: Signs of Breast Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What do the causes for menorrhagia include? (Select all that apply.) a. Hormonal dysfunction b. Tumors c. Coagulation disorders d. Endometrial hyperplasia e. Excessive exercising ANS: A, B, C, D Common causes for menorrhagia include hormonal dysfunction, tumors (both benign and malignant), coagulation disorders, and endometrial hyperplasia. Excessive exercise is far more likely to cause amenorrhea than menorrhagia. DIF: Cognitive Level: Knowledge REF: p. 1014 OBJ: 1 TOP: Menorrhagia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. A nurse is aware that a tumor determined to be ER positive indicates that the tumor needs for growth. ANS: estrogen A tumor that is classified as ER positive requires estrogen to grow. DIF: Cognitive Level: Knowledge REF: p. 1034 OBJ: 1 TOP: ER+ Tumors KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Because small nonnodal metastases may be present, is recommended after a lumpectomy. ANS: radiotherapy Radiotherapy is recommended after a lumpectomy even when no indication of metastasis is evident because of the threat of small metastases without nodal involvement. DIF: Cognitive Level: Comprehension REF: p. 1034 OBJ: 1 TOP: Radiation KEY: Nursing Process Step: N/A MSC: NCLEX: N/A Chapter 53: Male Reproductive System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. What should a nurse explain to a young man being treated for infertility as the purpose of a semen analysis? a. Determine the history of sexually transmitted infections. b. Evaluate the potential for genetic problems. c. Determine whether any urethral obstructions are present. d. Microscopically assess the sperm for number and motility. ANS: D Analysis of the semen is performed to assess male fertility based on number, appearance, and motility of the sperm. DIF: Cognitive Level: Knowledge REF: p. 1054 OBJ: 3 TOP: Semen Analysis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. What is the purpose of the urethral smear? a. Screens for human immunodeficiency viral (HIV) infection. b. Detects sexually transmitted infections. c. Verifies fertility through a sperm count. d. Eliminates concerns of prostate problems. ANS: B A sterile swab is inserted into the urethra to obtain a specimen to detect sexually transmitted infections. DIF: Cognitive Level: Knowledge REF: p. 1057 OBJ: 3 TOP: Diagnostic Tests KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A patient is placed on estramustine (Emcyt) for prostate cancer. What should the nurse explain as a possible side effect of the medication? a. Gynecomastia b. Pruritus c. Constipation d. Tinnitus ANS: A Gynecomastia is a side effect of estramustine (Emcyt). DIF: Cognitive Level: Knowledge REF: p. 1061 OBJ: 4 TOP: Drug Therapy for Male Reproductive System KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 4. When conducting an initial assessment on a 65-year-old male patient, a nurse assesses a mass in the left testicle that on transillumination glows red. What should the nurse note this indicates the presence of? a. Phimosis b. A hydrocele c. Smegma d. A hematocele ANS: B A hydrocele will glow red on transillumination, but a hematocele will not. Phimosis is a foreskin that will not retract over the glans, and smegma is a cheeselike substance found under the foreskin. DIF: Cognitive Level: Comprehension REF: p. 1053 OBJ: 3 TOP: Health Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. What should a nurse inform a 50-year-old patient who has been prescribed nilutamide (Nilandron), a testosterone blocker, to expect while taking this drug? a. His urine will have a fishy odor. b. Liver functions will need to be monitored. c. Skin rash will appear on his face. d. Episodes of hypotension will occur. ANS: B The drug nilutamide (Nilandron) is hepatoxic. While taking the drug, the patient will have to have periodic evaluations of his liver function. The patient should also be informed to report any jaundice or darkening of the urine. DIF: Cognitive Level: Comprehension REF: p. 1059 OBJ: 4 TOP: Testosterone Blockers KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Pharmacological Therapies 6. A patient has been prescribed flutamide (Eulexin) for the treatment of prostate cancer. What possible side effect should the nurse remind the patient might occur? a. Incontinence b. Insomnia c. Weight loss d. Hot flashes ANS: D Hot flashes, ED, edema, hypertension, and confusion are some of the side effects of flutamide. DIF: Cognitive Level: Knowledge REF: p. 1059 OBJ: 4 TOP: Flutamide KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 7. What instruction should a nurse include when giving education about taking sildenafil (Viagra)? a. No more than two tablets should be taken in a 24-hour period. b. Erection occurs without stimulation. c. Nitrates should be taken at least 4 hours before taking Viagra. d. Tablet should be taken 1 hour before sexual activity. ANS: D Viagra should be taken 1 hour before sexual activity. Erection depends on stimulation. No more than one tablet a day should be taken. Persons taking nitrates should not take Viagra because of the risk of a possibly fatal myocardial infarction. DIF: Cognitive Level: Comprehension REF: p. 1060 OBJ: 4 TOP: Sildenafil (Viagra) KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 8. When completing a health history with a patient, a nurse should encourage the patient to describe the symptoms in objective terms. Which statement is a good example of the description of pain? a. “This spot seems to hurt more right here.” b. “This pain is the worst pain in the world.” c. “My pain reminds me of when I hurt my foot last year.” d. “I would say my pain is a 5 on a scale from 1 to 10.” ANS: D Encourage the patient to use descriptive terms such as stinging or aching and ask him to indicate the intensity on a scale from 1 to 10. DIF: Cognitive Level: Application REF: p. 1052 OBJ: 2 TOP: Health History KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. What direction should a nurse provide when instructing a patient who is to have a semen analysis? (Select all that apply.) a. Collect specimen in a rubber condom. b. Keep the specimen at room temperature until given to the laboratory. c. Keep the specimen container in warm tap water. d. Bring the specimen to the laboratory within 4 hours. e. Abstain from sexual activity 2 to 3 days before the test. ANS: B, E Sexual activity should be avoided for 2 to 3 days before collection. The specimen should be collected in a clean container, not a rubber condom, and presented to the laboratory within 1 hour of collection. DIF: Cognitive Level: Application REF: p. 1054 OBJ: 3 TOP: Semen Collection KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A nurse is performing the initial assessment on a man with a reproductive disorder. What type of interview techniques should be used to demonstrate a sensitive approach? (Select all that apply.) a. Use open-ended questions. b. Pin the patient down for truthful and specific information. c. Leave sensitive questions until later in the interview. d. Share her or his professional opinion. e. Start most questions with “why.” ANS: A, C The use of open-ended questions encourages the patient to explain his problem in greater detail, especially if sensitive issues are left until later in the interview. Pinning the patient down, sharing professional opinion, and asking why are not therapeutic. DIF: Cognitive Level: Application REF: p. 1052 OBJ: 2 TOP: Initial Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. When a significant elevation in the human chorionic gonadotropin (hCG) level is noted on a laboratory report, the nurse is aware that this is a marker for cancer. ANS: testicular An elevation in the hCG is a marker for testicular cancer. DIF: Cognitive Level: Knowledge REF: p. 1056 OBJ: 3 TOP: Human Chorionic Gonadotropin Report KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 54: Male Reproductive Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is reviewing the drugs taken by a 50-year-old male patient. What medication should the nurse recognize as the most probable cause of erectile dysfunction (ED)? a. Vasodilator for hypertension b. Antibiotic for an upper respiratory infection c. Antihistamine for allergies d. Glucophage for type 2 diabetes ANS: A Vasodilators taken for the control of hypertension frequently cause ED. DIF: Cognitive Level: Knowledge REF: pp. 1072-1073 OBJ: 1 TOP: Male Sexual Dysfunction KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. A nurse is caring for a patient 2 hours after a transurethral resection and immediately reports to the charge nurse the presence of large clots in the catheter and drainage bag. What should the nurse anticipate the physician will order? a. Instill ice water into the bladder. b. Decrease the amount of fluid in the balloon of the indwelling catheter. c. Apply traction to the catheter by taping it to the patient’s thigh. d. Prescribe a potent vasoconstrictor to reduce hemorrhage. ANS: C Applying traction to the catheter may reduce the bleeding. An increase of fluid in the catheter balloon is also helpful, but ice water will have no better effect than the continuous bladder irrigation that is already in place. DIF: Cognitive Level: Application REF: p. 1067 OBJ: 1 TOP: Transurethral Resection of the Prostate KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A male student comes to the campus clinic complaining of painful scrotal edema, nausea, vomiting, chills, and fever. What should the nurse recognize these signs and symptoms as being associated with? a. Orchitis b. Epididymitis c. Urethritis d. Cystitis ANS: B Signs and symptoms of epididymitis are painful scrotal edema, nausea, vomiting, chills, and fever. DIF: Cognitive Level: Comprehension REF: p. 1064 OBJ: 1 TOP: Epididymitis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. Which instruction should increase the comfort of a patient who is recovering from prostatitis? a. Avoid bathing for 2 days b. Exercise c. Take stool softeners d. Limit fluid intake ANS: C Stool softeners may be prescribed to prevent constipation, which is painful with prostatitis. Fluid intake is also encouraged to reduce the risk of constipation. DIF: Cognitive Level: Comprehension REF: p. 1063 OBJ: 2 TOP: Prostatitis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 5. Which statement by a patient indicates he understands the teaching relative to how to perform a testicular self-examination? a. “It’s not necessary to feel the testes; just look at them in a mirror.” b. “The best time to do a self-examination is after a shower, when my body is warm.” c. “It doesn’t really matter when I do it; just do it sometime.” d. “The physician is really the best person to check this for me.” ANS: B The examination is best done after a warm bath or shower. DIF: Cognitive Level: Comprehension REF: p. 1077 OBJ: 3 TOP: Testicular Cancer KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. What should a patient’s home instructions following a vasectomy include? a. Postoperative care consists of warm sitz baths. b. Vasectomies should be seen as usually permanent but are sometimes reversible. c. Sexual intercourse should be delayed for up to 3 months. d. The surgical procedure may interfere with ejaculation. ANS: B Although a vasectomy can sometimes be successfully reversed, it should be considered permanent. DIF: Cognitive Level: Comprehension REF: p. 1077 OBJ: 3 TOP: Vasectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. A mother of a newborn with cryptorchidism asks if this condition will be permanent. What is the nurse’s best response? a. “Yes, but your child can develop normally with hormone replacement therapy.” b. “No, several medical and surgical remedies can be performed after your baby’s first birthday.” c. “Yes, but the undescended testicle is still able to function in a normal manner.” d. “No, the process of sexual maturity will cause it to descend at puberty.” ANS: B Partial or incomplete descent of the testicles may be resolved by medical or surgical implementation. Medical implementation starts between the first and second years of life. DIF: Cognitive Level: Comprehension REF: p. 1075 OBJ: 3 TOP: Cryptorchidism KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. A 60-year-old man who had a prostatectomy 3 weeks earlier asks if the ongoing incontinence will ever stop. What should the nurse understand about this procedure in order to answer the patient? a. Postprostatectomy incontinence is usually permanent. b. Postprostatectomy incontinence usually clears up in 6 months. c. Although the constant dribbling will stop, stress incontinence will continue. d. Postprostatectomy incontinence frequently requires a second surgery to correct the problem. ANS: B Postprostatectomy incontinence clears up in approximately 6 months in most patients. DIF: Cognitive Level: Knowledge REF: p. 1070 OBJ: 1 TOP: Postprostatectomy Incontinence KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. After an accident at a track meet, a young male runner is brought to the emergency department complaining of intense pain in his scrotum and nausea and vomiting. What should the nurse suspect based on these initial findings? a. Cryptorchidism b. Testicular torsion c. Varicocele d. Epididymitis ANS: B Symptoms of testicular torsion are intense pain, often accompanied by nausea and vomiting. DIF: Cognitive Level: Comprehension REF: p. 1076 OBJ: 1 TOP: Testicular Torsion KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. After a physician has left the room of a 30-year-old man who has been diagnosed with testicular cancer, the patient covers his face with both hands and sighs. What is the nurse’s most therapeutic intervention at this time? a. Ask the patient, “Do you want to talk about your cancer?” b. Leave the room and pull the door closed. c. Go to the nurse’s station and call the patient’s wife. d. Complete the patient care as quickly as possible. ANS: A You can help the patient through active listening, providing information, and referring him for counseling as needed. DIF: Cognitive Level: Application REF: p. 1078 OBJ: 3 TOP: Patient with Testicular Cancer KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 11. A nurse is formulating a teaching plan for a patient with acute prostatitis. What information should be included regarding treatment? a. There will be a 2-week period with a temporary catheter and the instillation of antibiotics in the bladder. b. There will be a 6-week course of antibiotics and anti-inflammatory drugs. c. There will be a 6-week course of broad-spectrum antibiotics followed by a prostatectomy. d. There will be a 16-week protocol of sitz baths and the use of a sturdy scrotal support. ANS: B Acute bacterial prostatitis is treated with antibiotics, analgesics, anti-inflammatory drugs, and sitz baths for a period of 6 weeks. Chronic prostatitis requires a 16-week period of antibiotic therapy. DIF: Cognitive Level: Comprehension REF: p. 1063 OBJ: 1 TOP: Prostatitis KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 12. A patient is recovering after surgery to correct a testicular torsion. Which possibility should the nurse caution the young patient about? a. Reoccurrence b. Infertility c. Orchiditis d. Significant risk of prostatic hypertrophy ANS: B After testicular torsion is corrected, lower sperm counts and infertility may follow. DIF: Cognitive Level: Knowledge REF: p. 1076 OBJ: 1 TOP: Testicular Torsion KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 13. What can men who have sustained spinal cord injuries with resultant ED use to aid in the ability to have sexual intercourse? a. Testosterone injections b. Papaverine penile injections c. Inflatable penile implants d. Antihypertensives ANS: C Penile implants may be prescribed for patients with the inability to initiate, fill, or restore an erection. DIF: Cognitive Level: Knowledge REF: p. 1072 OBJ: 1 TOP: Erectile Dysfunction KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. A nurse is assessing a young man who is being treated for sterility and inquires whether the young man had any common childhood disease that may be the cause of sterility. What childhood disease might result in sterility? a. Mumps b. Chickenpox c. Measles d. Scarlet fever ANS: A Mumps in a man or pubescent boy may result in acute orchitis or epididymitis. Infections that ascend to the epididymis may result in decreased fertility. DIF: Cognitive Level: Knowledge REF: p. 1064 OBJ: 1 TOP: Mumps KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 15. A patient has an elevation in the prostatic-specific antigen (PSA) level from 4 to 6 ng/L. What should the nurse suspect to be the cause? a. Possibility of prostatic cancer b. ED c. Probability of orchiditis d. Significant indication of Peyronie disease ANS: A PSA levels over 4 ng/L may indicate cancer of the prostate; further studies are needed. DIF: Cognitive Level: Comprehension REF: p. 1070 OBJ: 1 TOP: PSA KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. What should instructions relate to for a discharge teaching plan for a patient after undergoing a prostatectomy? (Select all that apply.) a. Remedy for bladder spasm b. Catheter care c. Delay of sexual activity for 3 months d. Perineal exercises e. Avoidance of heavy lifting ANS: A, B, D, E Instruction relative to relieving bladder spasms, catheter care, perineal exercises to help reduce incontinence, and the avoidance of heavy lifting are appropriate. Sexual activity is usually resumed in 6 weeks. DIF: Cognitive Level: Comprehension REF: p. 1152 OBJ: 6 TOP: Discharge Instructions for Prostatectomy KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 55: Sexually Transmitted Infections Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse in the outpatient clinic notes that a patient has been treated for syphilis three separate times in the past 2 years. What should the antibiotic treatment for this patient consist of this time? a. Penicillin G b. Penicillin G today and a follow-up with another injection in 1 month c. Penicillin G today and 3 months of oral tetracycline antibiotic medications d. Penicillin G today and a 2-month protocol of oral antiviral agents ANS: C The patient who has had syphilis for more than 1 year will need a long-term antimicrobial remedy, as well as an initial dose of penicillin G. Antiviral agents are not used in the treatment of a bacterial disease. DIF: Cognitive Level: Comprehension REF: p. 1084|p. 1089 OBJ: 4 TOP: Drug Protocol for Syphilis KEY: Nursing Process Step: Planning MSC: NCLEX: Psychosocial Integrity: Pharmacological Therapies 2. A nurse is completing a history of illnesses for a young woman who suspects she may have a sexually transmitted infection (STI). What specific symptom(s) should the nurse ask this patient if she experienced? a. Lethargy and fatigue b. Genital discharge c. Abdominal cramps d. Heavy menses ANS: B With an STI, the patient usually complains of genital discharge. DIF: Cognitive Level: Application REF: p. 1093 OBJ: 7 TOP: Collecting Data KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Physiological Adaptation 3. A patient has been diagnosed with herpes simplex virus, type 2 (HSV type 2). What instruction should the nurse provide? a. Avoid telling anyone about the condition. b. Wear close-fitting undergarments. c. Wash towels and personal items daily. d. Soak the sores with peroxide every day. ANS: C Inform the patient that the virus can survive on objects such as towels. DIF: Cognitive Level: Application REF: p. 1091 OBJ: 8 TOP: Herpes Simplex Virus, Type 2 KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A nurse is caring for a patient taking acyclovir (Zovirax). Which side effects of this drug should the nurse be alert for? a. Fever and bone marrow suppression b. Vaginal burning and skin irritation c. Dizziness, headache, and nausea d. Leukopenia and peripheral neuropathy ANS: C Side effects include dizziness, headache, nausea and vomiting, renal failure, and seizures. DIF: Cognitive Level: Comprehension REF: p. 1085 OBJ: 6 TOP: Drugs to Treat STIs KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 5. A woman diagnosed with gonorrhea is astounded and states that she had no idea that she had an STI. What should the nurse explain about gonorrhea? a. It produces no symptoms in half of those in the early stages of the infection. b. It always produces a foul vaginal discharge. c. It causes a vaginal chancre that is not easily detected. d. It may appear to be an upper respiratory infection in the early stages of the infection. ANS: A More than half of those in the early stages of gonorrhea have no symptoms at all. Symptoms of gonorrhea typically occur 3 days to 3 weeks after exposure and are more apparent in men than in women. No chancre is exhibited, as with syphilis, and gonorrhea does not produce a foul discharge. DIF: Cognitive Level: Application REF: p. 1087 OBJ: 4 TOP: Gonorrhea KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 6. A nurse giving instruction to a patient with an STI says, “I am supposed to tell you about STIs, but you probably know more about them than I do.” What is this nurse doing? a. Admitting her own ignorance about STIs b. Trying to get the patient’s attention c. Referencing current statistics d. Making a judgmental statement ANS: D Judgmental behavior on the part of health care providers discourages people from seeking appropriate medical care. DIF: Cognitive Level: Comprehension REF: pp. 1082-1083 OBJ: 5 TOP: Behavior of Health Care Workers KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Basic Care and Comfort 7. A patient at the outpatient clinic is reluctant to identify her sexual contacts. Why is the reporting of contacts essential? a. Slows transmission and spread of infections. b. Increases public awareness. c. Increases state funding for treatment. d. Collects data for research. ANS: A Confirmed cases are reported to the health department. The purpose is to identify and treat infected individuals so that transmission can be slowed. DIF: Cognitive Level: Comprehension REF: p. 1083 OBJ: 2 TOP: Reporting STIs KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. A patient with gonorrhea is taking a protocol of tetracycline antibiotics. Which statement by the nurse is most likely to help overcome patient noncompliance? a. “You should take all of this medicine.” b. “Failing to take the entire medicine amount will make your disease resistant to it.” c. “You will become sterile if you do not complete the supply of medicines.” d. “The doctor wants you to take all of this medication.” ANS: B Explain to the patient that medication-resistant disease is a real possibility if the entire amount of the prescription is not taken. Sterility is not related to noncompliance with the medication, but it is related to repeated occurrence of the gonorrhea. DIF: Cognitive Level: Application REF: p. 1084 OBJ: 8 TOP: Treatment Noncompliance KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. A patient with syphilis is seen at the clinic and complains of body aches, pustules, fever, and sore throat. Which stage of syphilis should the nurse recognize these symptoms identify? a. Primary b. Secondary c. Latent d. Late ANS: B Symptoms in the secondary stage are body aches, rash, pustules, fever, and sore throat. DIF: Cognitive Level: Comprehension REF: p. 1088 OBJ: 4 TOP: Syphilis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity 10. Doxycycline (Vibramycin) has been prescribed for a patient who has gonorrhea. What instruction should the nurse provide to the patient before beginning the medication? a. Take the medication with food or crackers. b. Refrain from sexual relations for 4 weeks. c. Follow-up to determine if the treatment was effective. d. Keep the medication in the refrigerator. ANS: C Follow-up examinations are important to determine whether treatment has been effective to prevent reinfection of the partner. DIF: Cognitive Level: Application REF: p. 1087 OBJ: 6 TOP: Drugs to Treat STIs KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. A couple comes to the emergency department for the treatment of an STI. The man’s presenting symptoms include a creamy penile discharge and frequent urination. The woman has lower abdominal pain and a vaginal discharge. What should the nurse recognize these symptoms to characterize? a. Chlamydial infection b. Gonorrhea infection c. HSV type B d. Trichomoniasis ANS: A Symptoms in men are penile discharge, thin at first and then creamy, and frequent urination. Symptoms in women are a vaginal discharge and lower abdominal pain. DIF: Cognitive Level: Comprehension REF: p. 1086 OBJ: 4 TOP: Chlamydia KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 12. A pregnant patient with HSV type 2 has a Herp-Test performed in the physician’s office 1 day before she is due to deliver by cesarean section. The test result is negative. What should the nurse know this means? a. The delivery must be by cesarean section. b. The patient must start on an antiviral protocol today. c. The baby will have to have antiviral medication 24 hours after birth. d. The delivery may be accomplished vaginally. ANS: D A negative Herp-Test result shows no active viral disease, and the birth can be accomplished vaginally if the physician prefers. DIF: Cognitive Level: Comprehension REF: p. 1091 OBJ: 4 TOP: Herp-Test KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 13. Which method is used to identify organisms of gonorrhea? a. Smears and cultures b. Serologic tests c. Antibody screening d. Sensitivity testing ANS: A Smears from genital discharge can be studied on a smear. DIF: Cognitive Level: Knowledge REF: p. 1087 OBJ: 1 TOP: Tests Used to Diagnose STIs KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 14. What instruction should be included by a health educator giving a presentation on how to use condoms correctly? a. Condoms are 100% effective when used correctly. b. The effectiveness of condoms deteriorates in heat. c. Any style and material of condom is safe to use. d. Use of petroleum jelly will ease application. ANS: B Protect condoms from heat and sunlight to keep them from deteriorating. DIF: Cognitive Level: Comprehension REF: p. 1098 OBJ: 9 TOP: Condoms KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 15. A nurse asks a patient to repeat the instructions to evaluate her knowledge about safe sex practices. Which statement indicates an understanding? a. “Body massage would be considered safe.” b. “Mutual open-mouth kissing is safe.” c. “Vaginal intercourse with a properly used condom is safe.” d. “Anal sex with a condom made of latex is a safe sex practice.” ANS: A Body massage is considered a safe sex practice. DIF: Cognitive Level: Comprehension REF: p. 1097 OBJ: 9 TOP: Safety of Various Sexual Practices KEY: Nursing Process Step: Evaluation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 16. A female patient, newly diagnosed with gonorrhea, screams, “I am going to kill my husband. I mean it.” What is the nurse’s best response? a. “Are you sure it is your husband who gave you gonorrhea?” b. “Yikes! Killing your spouse seems extreme.” c. “Shall I report your spouse as a sexual contact?” d. “I can understand your anger. How best can you deal with it?” ANS: D Provide an opportunity to talk. Help the patient focus on the source of anxiety with the use of open-ended questions. DIF: Cognitive Level: Application REF: p. 1096 OBJ: 9 TOP: STI Implementations KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 17. What is characteristic of the primary stage syphilis? a. Chancre b. Alopecia c. Pruritus d. Dry skin ANS: A A typical lesion, a chancre, is the first sign of syphilis. DIF: Cognitive Level: Knowledge REF: p. 1088 OBJ: 4 TOP: Syphilis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 18. What does diagnosis with the human papilloma virus (HPV) increase a person’s risk for? a. Uterine fibroids b. Chronic vaginitis c. Premature menopause d. Cervical cancer ANS: D Women with HPV or condylomata acuminate are advised to have annual Pap stain because they are at an increased risk for cervical cancer. DIF: Cognitive Level: Knowledge REF: p. 1092 OBJ: 9 TOP: Human Papilloma Virus KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 19. Which antiviral drug is commonly used to relieve symptoms of herpes simplex virus (HSV)? a. Tetracycline (Achromycin) b. Acyclovir (Zovirax) c. Erythromycin (E-Mycin) d. Metronidazole (Flagyl) ANS: B No cure is available for HSV infection, but oral antiviral drugs similar to acyclovir (Zovirax) help partially control the signs and symptoms during initial and recurrent episodes. DIF: Cognitive Level: Knowledge REF: p. 1091 OBJ: 4 TOP: Drugs to Treat STIs KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 20. What does chlamydial infection place a person at greater risk for? a. HIV if exposed to it b. Urinary infections c. Hepatitis B if exposed to it d. Opportunistic bacterial infections ANS: A Patients who have a chlamydial infection are five times more likely to contract HIV if exposed to it. DIF: Cognitive Level: Knowledge REF: p. 1086 OBJ: 8 TOP: Chlamydia KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 21. A patient at the outpatient clinic who has received an intramuscular dose of ceftriaxone sodium (Rocephin) calls and complains of pain and induration at the injection site. What should the nurse advise the patient to do? a. Undergo 30 minutes of active exercise to speed absorption of the drug. b. Make an appointment at the clinic for evaluation to initiate another drug. c. Immediately come to the clinic for treatment of the allergic reaction. d. Place a warm compress on the area. ANS: D A warm compress may be applied to the area because these symptoms are the expected results of the injection, not allergic reactions. Another drug is not needed. DIF: Cognitive Level: Application REF: p. 1084 OBJ: 6 TOP: Rocephin KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 22. What should a nurse caution a patient taking Flagyl for Trichomonas to do? a. Double the dose if any doses are missed. b. Report dark urine. c. Take the drug on an empty stomach. d. Abstain from alcohol while taking the drug. ANS: D The use of alcohol while taking Flagyl has serious side effects. Dark urine is expected, doses should not be doubled, and the drug should be taken with a full glass of water. DIF: Cognitive Level: Application REF: p. 1085 OBJ: 6 TOP: Flagyl KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 23. A patient with a chlamydial infection is taking a 7-day course of doxycycline (Vibramycin). What information should the nurse provide? a. Return in 1 month for a follow-up culture. b. Take the drug on an empty stomach with a minimum of fluid. c. Delay sexual activity until cured. d. Expect genital or anal itching or burning. ANS: C The patient with a chlamydial infection should delay sexual activity until completely clear. Follow-up cultures are obtained 4 to 7 days after the initiation of the drug, and the drug should be taken with food or milk. DIF: Cognitive Level: Application REF: p. 1086 OBJ: 6 TOP: Vibramycin KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease MULTIPLE RESPONSE 1. A nurse explains that STIs must be reported to the local public health department. Which are considered reportable diseases? (Select all that apply.) a. HIV b. Acquired immunodeficiency syndrome (AIDS) c. Gonorrhea d. Chlamydia e. Viral hepatitis ANS: A, B, C, D, E All confirmed cases of HIV, AIDS, gonorrhea, Chlamydia, and viral hepatitis are reportable. DIF: Cognitive Level: Knowledge REF: p. 1083 OBJ: 2 TOP: Reportable Diseases KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. What body areas might systemic (disseminated) gonorrhea involve? (Select all that apply.) a. Heart b. Eyes c. Meninges d. Skin e. Joints ANS: A, C, D, E Systemic gonorrhea may damage all of the body areas mentioned except the eyes. DIF: Cognitive Level: Knowledge REF: p. 1087 OBJ: 4 TOP: Systemic Gonorrhea KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A nurse recognizes that a patient with an STI may not cooperate in reporting sexual contacts. What fears might prevent reporting? (Select all that apply.) a. Judgment by health care workers b. Identifying self as infected c. Rejection by contacts d. Infecting others e. Reprisal from identified contacts ANS: A, B, C, E Infection of others has already occurred. DIF: Cognitive Level: Comprehension REF: p. 1096 OBJ: 2 TOP: Impediments to Reporting STIs KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation COMPLETION 1. A patient who is using imiquimod (Aldara) for genital warts asks the outpatient clinic nurse how long she must use the medication. The nurse replies that she must apply the medication for weeks. (Use numeric characters only.) ANS: 16 The protocol for Aldara is application three times a day for 16 weeks. DIF: Cognitive Level: Knowledge REF: p. 1086 OBJ: 6 TOP: Genital Warts KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies Chapter 56: Integumentary System Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. Displaying her hands, a patient asks, “Do you think my liver is OK? Look at all these liver spots!” What is the most appropriate nursing response? a. “The spots could mean something is wrong; I will make a note of it.” b. “The spots are normal aging changes and have nothing to do with your liver.” c. “Have you recently been exposed to hepatitis?” d. “Don’t worry about them. They will fade during the winter.” ANS: B Lentigines on sun-exposed areas are called liver spots because of their color; they have nothing to do with the liver or any disease process. They are normal changes of aging. DIF: Cognitive Level: Comprehension REF: p. 1106 OBJ: 2 TOP: Liver Spots KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Physiological Adaptation 2. A confused patient has been restrained because of combativeness and hyperactivity. What skin assessment may occur as a result of the restraints? a. Lentigines b. Senile purpura c. Senile angiomas d. Seborrheic keratoses ANS: B Purpura are purple bruises that resolve very slowly and are usually the result of minor trauma. DIF: Cognitive Level: Comprehension REF: p. 1106 OBJ: 2 TOP: Senile Purpura KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. What should a nurse ask about when taking the functional assessment of a patient with a skin disorder? a. A sore that is slow to heal b. Unusual hair growth c. Previous skin disorders d. Exposure to chemicals or irritants ANS: D The functional assessment is a search for clues in the occupation and lifestyle of the patient. The other options are reference medical history and system review. DIF: Cognitive Level: Application REF: p. 1103 OBJ: 3 TOP: Functional Assessment KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. A daughter of an older adult patient who has just returned from surgery is distressed about her father’s pale, cold hands and feet. What is the best response by the nurse after covering the patient with an extra blanket? a. “Don’t be concerned. It is quite cold in the operating room. Your dad will be warm in a minute.” b. “Older patients like your dad get a little shocky during surgery.” c. “When patients have blood loss during surgery, superficial vessels close off temporarily, resulting in cold extremities.” d. “We are watching the disturbed circulation in your dad’s hands and feet very carefully.” ANS: C The 10% of the blood network that is in the skin can be reduced by constriction and shunted to the vital organs. DIF: Cognitive Level: Application REF: p. 1102 OBJ: 1 TOP: Skin Blood Reservoir KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. What information should a nurse provide to a patient with vitiligo receiving phototherapy? a. “Expose yourself to the sun for several hours before treatment to acclimate the skin surface.” b. “Wear protective clothing.” c. “Wear loose clothing such as sleeveless T-shirts and shorts after the treatment.” d. “Leave off sunglasses after treatment so your eyes can more quickly accommodate.” ANS: B Eight hours before and after each treatment, the patient should wear protective clothing, sunglasses, and sunscreen to decrease added ultraviolet exposure from other sources. DIF: Cognitive Level: Application REF: p. 1108 OBJ: 4 TOP: Phototherapy KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 6. A nurse is screening patients that the plastic surgeon is considering for phototherapy. Which patient should the nurse exclude? a. A 34-year-old woman with lupus erythematosus b. A 5-year-old child with pneumonia c. A 60-year-old man with a pacemaker d. A 23-year-old woman who is 3 months’ pregnant ANS: A Persons with lupus erythematosus should avoid exposure to UV light. DIF: Cognitive Level: Comprehension REF: p. 1108 OBJ: 4 TOP: Phototherapy KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. Which age-related skin changes should a nurse anticipate when performing a physical assessment on an 80-year-old man? (Select all that apply.) a. Increased nasal hair b. Flattened nails c. Small macular lesions at the hairline d. Increased hair on the helix of the ear e. Presence of seborrheic keratosis ANS: A, B, D, E Increased hair in the nostrils and ear, flattened discolored nails, and seborrheic keratosis are common age-related skin changes. Macular lesions are abnormal. DIF: Cognitive Level: Knowledge REF: p. 1106 OBJ: 2 TOP: Age-Related Skin Changes KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Which conditions can be improved with negative pressure therapy? (Select all that apply.) a. Pressure ulcers b. Skin grafts c. Burns d. Dehisced surgical wounds e. Eczema ANS: A, B, D All ulcers, skin grafts, and dehisced wounds respond well to negative pressure therapy. DIF: Cognitive Level: Comprehension REF: p. 1107 OBJ: 4 TOP: Negative Pressure Therapy KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. When assessing the capillary refill, a nurse should document as normal a refill time of seconds. (Use numeric characters only.) ANS: 3 Capillary refill is a method of quick assessment of perfusion to the extremities. A normal capillary refill time is 3 to 5 seconds or less. DIF: Cognitive Level: Comprehension REF: p. 1103 OBJ: 3 TOP: Capillary Refill KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse collecting tissue for a Tzanck test should: (Select the appropriate interventions and place the steps in sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Open the lesion with a hypodermic needle. b. Place the specimen in a culture tube and take it to the laboratory. c. Saturate the sterile swab with exudates. d. Wash the lesion. e. Place a pressure dressing on the lesion. ANS: DACB The nurse washes the lesion, punctures the lesion with a needle, saturates a sterile cotton swab, places the swab in a culture tube, and takes the collected tissue to the laboratory. A pressure dressing is not needed. DIF: Cognitive Level: Application REF: p. 1108 OBJ: 4 TOP: Tzanck Test KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 57: Skin Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse is caring for a patient with pruritus. Which implementation can the nurse perform without a physician’s order? a. Apply topical corticosteroids to affected areas. b. Administer an antihistamine. c. Apply lubricant to unbroken skin. d. Bathe the patient in an oatmeal bath. ANS: C Application of a lotion or lubricant to unbroken skin may be done without an order. DIF: Cognitive Level: Application REF: p. 1114 OBJ: 2 TOP: Pruritus KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. Which action should a nurse implement to make a patient with atopic dermatitis more comfortable? a. Instruct the patient to wear loose clothing. b. Add alcohol to the bath water. c. Provide a diet low in fat. d. Increase the room temperature between 78 F and 80 F. ANS: A Loose clothing and a cool atmosphere allow the skin to stay cool and reduce sweating. Alcohol is drying to the skin. DIF: Cognitive Level: Application REF: p. 1115 OBJ: 2 TOP: Atopic Dermatitis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 3. Which sign or symptom suggests that a patient with skin breakdown is developing a systemic infection? a. Lesion on the patient’s leg that is swollen and warm to the touch b. Temperature that has risen to 101 F c. Blood pressure that has risen from 126/84 to 130/86 mm Hg d. Request by the patient for medication for severe itching ANS: B A rise in temperature is a systemic response. Normal blood pressure, warmth, swelling, and itching are not evidence of a systemic skin infection. DIF: Cognitive Level: Comprehension REF: p. 1115 OBJ: 2 TOP: Systemic Infection KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. Which is an appropriate implementation for a patient with severe psoriasis who has an altered self-concept? a. Touching the patient often b. Reassuring the patient of a quick remission c. Reminding the patient to bathe often d. Promptly administering medications as needed ANS: A To touch, interact, and care attentively for a disfigured patient communicates acceptance. DIF: Cognitive Level: Application REF: p. 1117 OBJ: 2 TOP: Psoriasis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 5. A patient with severe psoriasis who is to be treated with the systemic drug methotrexate sodium anxiously asks, “Is this cancer drug safe? Are there some side effects I need to know about?” What is the best response by the nurse? a. “Yes, methotrexate is used to treat cancer and psoriasis, and it has no severe side effects.” b. “No, it is not a cancer drug, but you should ask your physician about concerns regarding your therapy.” c. “We use this drug to treat many kinds of patients, including patients with cancer. You will have periodic blood tests.” d. “I don’t know if it is used with patients with cancer, but the drug can be used when conditions are as severe as yours.” ANS: C Methotrexate is an immunosuppressive drug used to treat psoriasis that is nonresponsive to other protocols. Periodic blood tests are performed to assess for leukopenia. The other options either do not answer the patient’s question or offer erroneous information. DIF: Cognitive Level: Application REF: p. 1116 OBJ: 2 TOP: Methotrexate Sodium KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 6. A family member of an older patient with severe dermatitis says, “I was always so careful to bathe him every day. I guess I just wasn’t careful enough.” What is the best response by the nurse? a. “Dermatitis is not caused by poor hygiene.” b. “Don’t worry; we will bathe him thoroughly while he is here.” c. “You will have a chance to do better when he is back at home.” d. “You shouldn’t feel like the skin condition is your fault.” ANS: A Dermatitis is not a condition of poor hygiene. Implying that the family member is responsible for the condition is belittling and not therapeutic. DIF: Cognitive Level: Application REF: p. 1115 OBJ: 2 TOP: Dermatitis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. A nurse is caring for an obese patient who has been bedridden for a long time and who has a high risk for infection. Where is the best location for the nurse to assess for the moist red lesions of Candida albicans? a. Scalp, behind the ears b. Abdominal skinfolds c. Shaft of the penis d. Sacrum and bony prominences ANS: B C. albicans infection appears most often in skinfolds. DIF: Cognitive Level: Comprehension REF: p. 1118 OBJ: 2 TOP: Yeast Infection KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. What information is most essential for a nurse to gather when interviewing a young woman who is taking the drug isotretinoin (Accutane) for acne? a. Usual weight b. Family history of breast cancer c. Current method of birth control d. Drugs previously used ANS: C Accutane can cause severe fetal deformities. DIF: Cognitive Level: Comprehension REF: p. 1120 OBJ: 2 TOP: Acne Treatment KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 9. An excited mother of a teenage boy with severe acne furiously reports to the nurse, “I’ve told him a thousand times he should bathe more often! I’ve kept after him about all that junk food he eats. I jump on him when I see him squeezing his zits. I tried to get him to scrub his face three times a day!” Which statement indicates the most likely cause of the boy’s acne? a. Poor personal hygiene b. Ingestion of junk food c. Squeezing lesions d. Need for facial scrubs ANS: C Squeezing the lesions may cause them to spread and push the infection deeper into the follicles. Poor personal hygiene, eating junk food, and the need for facial scrubs are myths. DIF: Cognitive Level: Application REF: pp. 1120-1121 OBJ: 2 TOP: Acne KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 10. A patient who has undergone treatment for herpes simplex virus type 2 (HSV type 2) expresses relief that she is cured. What should the nurse include in her teaching? a. Daily douches of Burow solution are needed. b. HSV is permanently cured by acyclovir (Zovirax). c. Sexual partners are now safe from infection from her. d. HSV lies dormant and can be triggered without any sexual contact. ANS: D The virus goes dormant but can recur. Herpes is always present. DIF: Cognitive Level: Application REF: p. 1122 OBJ: 2 TOP: Herpes Simplex KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 11. An 80-year-old patient comes to the emergency department with extreme pain and itching in the hip and leg and has herpetic vesicular lesions on the left hip. What should the nurse inquire about patient exposure to? a. HSV, type 1 b. HSV, type 2 c. Smallpox d. Chickenpox ANS: D Chickenpox is a virus that lies latent in the neural sheath and can be activated as shingles in older adults. DIF: Cognitive Level: Application REF: p. 1122 OBJ: 2 TOP: Herpes Zoster KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 12. A physician asks a nurse to take a smear from herpetic lesions in an older patient’s hip to diagnose the disorder. What is the most probable test that will be performed? a. Culture and sensitivity test to a bactericide b. Tzanck test to test for viral culture c. Complete blood count to assess the white blood count for response to a pathogen d. Titration for the strength of the pathogen ANS: B The Tzanck test rapidly confirms the specific virus. The results are available sooner than they would be from a culture. DIF: Cognitive Level: Comprehension REF: p. 1122 OBJ: 2 TOP: Tzanck Test KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. How does cutaneous T-cell lymphoma differ from squamous cell and basal cell carcinomas? a. Does not metastasize. b. Has a cause unrelated to sun exposure. c. Can be treated with radiation. d. Can be treated topically. ANS: B Cutaneous T-cell carcinoma appears in areas protected from the sun. All three neoplasms can metastasize, and all three neoplasms can be treated by radiation or topically. DIF: Cognitive Level: Comprehension REF: p. 1124 OBJ: 1 TOP: Cutaneous T-Cell Carcinoma KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity 14. A nurse is caring for an adult patient with extensive burns on the front of the trunk, including the genitalia, and the fronts of both legs. How should the nurse document the burn size using the rule of nines? a. 13% b. 17% c. 25% d. 37% ANS: D Per the rule of nines, the front of the trunk equals 18%, the fronts of the legs equal 18%, and the genitalia equal 1%. DIF: Cognitive Level: Analysis REF: p. 1127 OBJ: 1 TOP: Burn Estimate KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 15. Which assessment by an emergency department nurse most indicates that a burn patient might be at risk for respiratory impairment? a. Burns on the face and neck b. Respiration of 18 breaths/min c. Flaring nares d. Sooty sputum ANS: D Sooty sputum is the most indicative. Facial burns and flaring nares are not conclusive in themselves. Respiration rate of 18 breaths/min is normal. DIF: Cognitive Level: Application REF: p. 1130 OBJ: 1 TOP: Burns: Respiratory Impairment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. What should a nurse be sure to frequently assess when caring for a burn patient with eschar formation around an entire arm? a. Urine output b. Pain level c. Capillary refill d. Breath sounds ANS: C Eschar that encompasses a limb can compromise circulation. DIF: Cognitive Level: Application REF: p. 1131 OBJ: 2 TOP: Eschar: Impaired Circulation KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. During the first 24 hours after a burn, fluid replacement is the treatment priority. Which assessment should alert the nurse that the fluid protocol is ineffective? a. Rectal temperature of 101 F b. Urine output of 20 mL/hr c. Crackles in the lower left lobe d. Significant edema in the burn area ANS: B Decreased urinary output indicates that poor perfusion to the kidney still remains. Temperature elevation and edema are to be expected. Crackles in a patient who is dormant are not causes for alarm. DIF: Cognitive Level: Application REF: p. 1129 OBJ: 2 TOP: Burns: Fluid Replacement KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. A nurse is alert for the expected fluid shift in the patient who was burned 24 hours earlier. (Place the events in the appropriate sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. Fluid volume deficit occurs. b. Blood is shunted from the kidneys to compensate for a loss of fluid volume. c. Urine output decreases. d. Generalized edema occurs. e. Hypoproteinemia causes fluid to move from the bloodstream to extracellular space ANS: EDABC Hypoproteinemia causes a fluid shift from the bloodstream to extracellular space, causing generalized edema; fluid volume deficit occurs; blood is shunted from the kidneys and gastrointestinal tract to make up for the fluid loss in the circulating volume; and urine output is decreased. DIF: Cognitive Level: Comprehension REF: p. 1129 OBJ: 2 TOP: Fluid Shift in Burn Patient KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort Chapter 58: Special Senses Introduction Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A nurse reads in a patient’s history that the patient has experienced otalgia. How should the nurse interpret this term? a. Difficulty hearing b. Buildup of cerumen c. Ear pain d. Ringing in the ears ANS: C Otic- is the root word for ear, and -algia is the root term for pain of any type. DIF: Cognitive Level: Knowledge REF: p. 1156 OBJ: 1 TOP: Definitions KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. A nurse is assisting with a caloric test and notes that the specific patient response that indicates a hearing disorder is a problem in the labyrinth. Which response did the nurse witness? a. Blinking b. Grimacing c. Headache d. Nystagmus ANS: D When warm or cold water is introduced into the ear, the appearance of nystagmus is a positive indication that the hearing problem has its cause in the labyrinth. DIF: Cognitive Level: Comprehension REF: p. 1158 OBJ: 2 TOP: Caloric Test KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 3. A 75-year-old patient has normal age-related changes in his ear. What change should not be considered a normal change in the aging patient? a. Dry and wrinkled skin on the auricle b. Otitis externa c. Dry cerumen d. Hair in the ear canal ANS: B Otitis externa is an outer ear infection and therefore an exception. The other three options are normal age-related changes. DIF: Cognitive Level: Comprehension REF: p. 1156 OBJ: 1 TOP: Age-Related Changes KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A patient reports that her hearing loss has become more severe over the past 3 months. The clinic nurse makes arrangements for an evaluation for a hearing aid. What health care provider should provide this service? a. Otologist b. Otolaryngologist c. Audiometrist d. Audiologist ANS: D Audiologists assess patients for hearing aids. The other specialists treat ear, nose, and throat (ENT) disorders. DIF: Cognitive Level: Knowledge REF: p. 1157 OBJ: 2 TOP: Audiometry KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. When a patient has a suspected vestibular disorder, the physician orders an electronystagmography test. Which instruction should the nurse include when educating the patient about this test? a. Use tea or coffee on the morning of test. b. Electrodes will be placed on the scalp. c. Air will be blown into the external ear. d. The patient should have nothing to eat or drink (NPO) 3 hours before the test. ANS: D Electronystagmography is used to detect vestibular lesions and requires a 3-hour period of NPO before the test. Coffee and tea should also be avoided before the test. DIF: Cognitive Level: Comprehension REF: p. 1158 OBJ: 2 TOP: Testing for Ear Disorders KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. A nurse assessing the results of a Rinne test sees the notation of BC > AC. How should the nurse translate this result? a. Conductive hearing loss b. Sensorineural hearing loss c. Normal hearing d. Cochlear defect ANS: A When the bone conduction (BC) is greater than the air conduction (AC), the results of the Rinne test will read, BC > AC, which means the patient has a conductive hearing loss. The normal finding for the Rinne test is that AC is greater than BC (AC > BC). DIF: Cognitive Level: Analysis REF: p. 1159 OBJ: 2 TOP: Rinne Test KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 7. A patient undergoing a Weber test says that the sound is louder in her left ear. What should this result indicate? a. Normal hearing b. Nerve damage from listening to loud music c. Blocked ear canal in the right ear d. Conductive hearing loss in the left ear ANS: D With the Weber test, a conductive hearing loss is determined by the sound being heard loudest in the affected ear. DIF: Cognitive Level: Comprehension REF: p. 1159 OBJ: 2 TOP: Weber Test KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. Which instruction should a nurse include when providing patient teaching information for a patient who will be self-administering ear drops for an ear infection? a. Tip the affected ear up and keep it in that position for several minutes after instilling the medication. b. Keep the medication in the refrigerator to preserve it. Instill the medication with the affected ear tilted upward. c. Touch the dropper to the opening of the ear canal to ensure that the drops are correctly instilled. d. Warm the ear drops and then tilt the head downward. ANS: A The head is kept in an upward position to ensure that the drops penetrate deep into the external ear. DIF: Cognitive Level: Application REF: p. 1160 OBJ: 3 TOP: Ear Drops KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. What nursing action should be implemented when irrigating a patient’s ear? a. Straighten the ear canal and irrigate with a large-tipped bulb syringe. b. Direct the solution to the middle of the canal to avoid damaging the ear. c. Use a body temperature solution and have the patient hold a basin under the ear while directing the solution toward the top of the canal. d. Repeat the irrigation with hotter water. ANS: C The irrigation is done with warm water using a small-tipped syringe. The flow is directed upward. If the cerumen does not wash out, the procedure can be repeated but with the same water temperature. DIF: Cognitive Level: Application REF: p. 1161 OBJ: 3 TOP: Irrigation KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. A nursing report on a newly admitted patient who is profoundly deaf says that the patient is confused and difficult to assess because she does not appropriately respond to questions or sometimes fails to respond at all. What should be the first action of the oncoming nurse? a. Consider asking the physician to assess the patient for dementia. b. Assess the patient to determine whether her hearing aids are in. c. Report to the physician that the patient is exhibiting signs of the sundown syndrome. d. Assess the patient’s medications to check for an overdose. ANS: B Profoundly deaf persons can be mistakenly assessed as being confused or disoriented when not wearing their hearing aids. DIF: Cognitive Level: Application REF: pp. 1161-1162 OBJ: 3 TOP: Hearing Aids KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 11. Which patient problem would the nurse prioritize for a patient having ear surgery? a. Altered self-concept b. Potential injury c. Knowledge deficit d. Inability to communicate effectively ANS: B Patients who have had ear surgery are at risk for vertigo, fluid accumulation, or pressure in the operative ear. Because of the surgery and potential postoperative conditions, the patient may be at risk for a fall. DIF: Cognitive Level: Application REF: p. 1167 OBJ: 3 TOP: Care Planning for Ear Surgery KEY: Nursing Process Step: Planning MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 12. What significant instruction should a nurse include to a patient being discharged after ear surgery? a. Use stool softeners with caution. b. Assume your usual activities. c. Avoid blowing your nose. d. Shampoo your hair with baby shampoo. ANS: C The patient should avoid blowing the nose to prevent back pressure in the eustachian tube. The patient should take stool softeners, limit activity until balance returns, and delay shampooing. DIF: Cognitive Level: Application REF: p. 1166 OBJ: 3 TOP: Nursing Diagnosis and Outcome Criteria KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 13. A patient with diabetes says that he needs a hearing aid because he cannot hear well, and everything sounds garbled and distant. What type of hearing loss should the nurse suspect? a. Mixed hearing loss b. Conductive hearing loss c. Central hearing loss d. Sensorineural hearing loss ANS: D A patient with long-term diabetes may have a sensorineural hearing loss that is not helped by hearing aids. DIF: Cognitive Level: Comprehension REF: p. 1162 OBJ: 3 TOP: Types of Hearing Loss KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 14. Which is the most appropriate concern when considering the impact of a hearing deficit when planning care for a child who has been diagnosed with a hearing impairment? a. Potential injury b. Decreased socialization c. Knowledge deficit d. Anxiety ANS: B The loss of hearing and the mild stigma associated with hearing impairment place the newly diagnosed child at risk for social isolation. DIF: Cognitive Level: Application REF: p. 1165 OBJ: 3 TOP: Impact of Hearing Impairment KEY: Nursing Process Step: N/A MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 15. An 85-year-old patient has had age-related changes in the cochlea. What is the most appropriate nursing action for the nurse to implement? a. Speak slowly. b. Provide assistance with ambulation. c. Speak in a lower tone. d. Communicate with the patient in writing. ANS: B Assisting the patient when ambulating will diminish the risk of a fall. Changes in the cochlea will cause dizziness and ataxia. DIF: Cognitive Level: Application REF: p. 1156 OBJ: 3 TOP: Age-Related Changes KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 16. A patient who has been taking opioid medication for postoperative pain exhibits pinpoint pupils. Which anatomic portion of the eye has been affected by the medication? a. Sclera b. Retina c. Choroid d. Bulbar conjunctiva ANS: C The choroid of the eye contains the pupil and iris. DIF: Cognitive Level: Comprehension REF: p. 1140 OBJ: 1 TOP: Anatomy and Physiology of the Eye: Eyeball KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 17. Which portion of the eye makes it possible for a person to see in a darkened environment? a. Macula b. Rods c. Cones d. Optic nerve ANS: B The eye uses rods to accommodate to dim light. Cones are the color receptors, the optic nerve transmits all sensory input from the eye to the brain, and the macula is an oval-shaped yellow spot near the center of the retina that mediates clear, detailed vision. DIF: Cognitive Level: Knowledge REF: p. 1141 OBJ: 1 TOP: Anatomy and Physiology of the Eye: Eyeball KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 18. When being interviewed, a 50-year-old patient says that he cannot see the newspaper as well as he used to. What is the reason this patient vision has changed from near to far? a. The ciliary muscle changes the pupil size. b. The lens of the eye changes shape as the ciliary muscle contracts and relaxes. c. Nearsightedness has set in. d. Clouding of the vitreous humor has occurred. ANS: B Accommodation or adjustment of the lens by contraction and expansion of the ciliary muscle allows an individual to see far or near. DIF: Cognitive Level: Comprehension REF: p. 1143 OBJ: 1 TOP: Lens Adjustment KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 19. During the initial assessment of a very thin patient at the eye clinic, a nurse notes that the patient has very prominent eyes. What medical diagnosis might the nurse find in this patient’s history? a. Diabetes b. Glomerulonephritis c. Hyperthyroidism d. Hypertension ANS: C The appearance of the patient and the prominence of the eye (exophthalmos) would lead the nurse to inquire about a thyroid disorder such as hyperthyroidism. DIF: Cognitive Level: Comprehension REF: p. 1143 OBJ: 1 TOP: Medical History KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity 20. When asked about his vision, a patient says that the last time he had it tested, his vision was recorded as 20/50. What does this mean? a. He can read at 20 feet what a person with normal vision can read at 50 feet. b. He can read at 50 feet what a person with normal vision can read at 20 feet. c. He needs to be 50 feet from objects to see them. d. He can see objects the best between 20 and 50 feet. ANS: A The Snellen eye chart is read at 20 feet. The last line the patient can read with no more than two errors is recorded. This patient was able to read the 50-foot line at 20 feet, which means that he is reading at 20 feet what a person with normal vision can read at 50 feet. DIF: Cognitive Level: Comprehension REF: p. 1145 OBJ: 1 TOP: Physical Examination: Eyes KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 21. Which intraocular pressure reading obtained by tonometry indicates a patient being evaluated for a visual impairment does not have glaucoma? a. 18 mm Hg b. 28 mm Hg c. 45 mm Hg d. 52 mm Hg ANS: A The normal intraocular pressure is between 10 and 20 mm Hg. If the patient had glaucoma, the intraocular pressure would be abnormally high. DIF: Cognitive Level: Comprehension REF: p. 1147 OBJ: 3 TOP: Tonometry KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 22. What does a pneumatonometric study of the eye require? a. Regional anesthesia b. A pneumotonometer to be placed into the eye c. A puff of air directed at the surface of the eye d. An applanation performed with a slit-lamp microscope ANS: C A pneumotonometer directs a puff of air at the surface of the eye, measuring intraocular pressure by measuring the resistance to the air. The eye is anesthetized before the evaluation. DIF: Cognitive Level: Comprehension REF: p. 1147 OBJ: 2 TOP: Tonometry KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 23. What is an appropriate nursing action to implement when performing eye irrigation? a. Ask the patient to tip up her head and run the irrigation fluid over her open eye. b. Direct the irrigating fluid from the inner canthus to the outer canthus. c. Not allow the patient to blink. d. Place the irrigating syringe directly onto the corner of the eye and allow the fluid to move across the eye. ANS: B The direction of the flow should be from the inner canthus to the outer canthus. DIF: Cognitive Level: Application REF: p. 1148 OBJ: 3 TOP: Eye Irrigation KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 24. What information should a nurse include when providing information to a patient using topical eye medications? a. Look upward and drop the medication into the inner canthus. b. Pull the lower eyelid down and drop the medication into the conjunctival sac. c. Hold both eyelids open and drop the medication onto the sclera. d. Tilt the head to the side and drop the medication into the outer canthus. ANS: B The eye drops should be dropped into the lower eyelid, and the nurse should press the tear duct to slow absorption. DIF: Cognitive Level: Comprehension REF: p. 1148|p. 1150 OBJ: 3 TOP: Topical Medications KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 25. What does electroretinography measure? a. A fluorescein dye is injected intravenously (IV) into a vein in the arm, and the retina is observed as the dye circulates. b. Electrodes are placed on the scalp, each eye is stimulated, and retinal activity is assessed. c. A small plunger is used to apply pressure on the sclera while the retinal vessels are evaluated. d. A contact lens electrode is placed on the eye and exposed to flashes of light to evaluate the retinal response. ANS: D A contact lens electrode is placed on the eye, and retinal activity is assessed as lights are flashed into the eye. The other three options describe fluorescein angiography, visual-evoked response, and tonometry. DIF: Cognitive Level: Knowledge REF: p. 1146 OBJ: 2 TOP: Electroretinography KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 26. What information should a nurse relay to a patient when providing education about protecting vision? a. After 40 years of age, eye examinations should be performed every 2 years. b. Crusted eyelids on awakening are caused by decreased tear production. c. Floaters are a sign of eye infection. d. Blurred vision without pain is temporary eye strain. ANS: A Eye examinations every 2 years are recommended for persons older than 40 years of age. All the other options are indications that the person should consult a physician for an eye disorder. DIF: Cognitive Level: Comprehension REF: p. 1151 OBJ: 2 TOP: Protection of the Eye and Vision KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 27. How should a nurse assist a visually impaired patient to ambulate? a. Hold the visually impaired person by his or her nondominant arm and walk side by side. b. Hold the nondominant hand, wrap the arm around his or her waist, and walk side by side. c. Allow the visually impaired person to hold the helper’s arm, with the helper slightly ahead. d. Allow the visually impaired person to hold the shoulder of the helper and walk slightly behind the helper. ANS: C Allowing the visually impaired person to walk slightly behind the helper and holding the helper’s arm is the most effective way to guide someone who is visually impaired. DIF: Cognitive Level: Application REF: p. 1152 OBJ: 3 TOP: Assisting the Visually Impaired with Ambulation KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 28. A newly diagnosed patient with macular degeneration flings her book at the television set and furiously says, “I can’t read this blasted book, and I can’t see what is on the stupid TV!” How should the nurse define this behavior? a. Anger stage of grieving b. Poor impulse control c. Ineffective management of a therapeutic regimen d. Psychotic reaction to loss ANS: A Frequently, a grieving process accompanies the realization that deteriorating vision and ultimate blindness are inevitable with macular degeneration. DIF: Cognitive Level: Application REF: p. 1151 OBJ: 3 TOP: Impact of Visual Impairment KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 29. What is the correct term to use for a patient with a vision disorder? a. Blind b. Handicapped c. Partially blind d. Visually impaired ANS: D The term visual impairment is a medically accepted term to use for patients with a vision loss. DIF: Cognitive Level: Knowledge REF: p. 1151 OBJ: 1 TOP: Nursing Care of the Visually Impaired Patient KEY: Nursing Process Step: N/A MSC: NCLEX: Psychosocial Integrity: Basic Care and Comfort 30. Which implementation is appropriate in the care plan for a visually impaired person? a. Leaving the bed in the highest position b. Keeping the door closed c. Announcing your presence when you enter and leave the room d. Leaving the radio on all the time to help the patient know the time of day ANS: C The nurse should announce her or his presence in the room and address the patient before touching him or her. The bed should be in the lowest position, and the door should be open to avoid social isolation. DIF: Cognitive Level: Application REF: p. 1152 OBJ: 3 TOP: Implementation KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control MULTIPLE RESPONSE 1. Which patient behaviors should alert a nurse to a possible hearing deficit? (Select all that apply.) a. Watches the speaker’s mouth. b. Gives inappropriate answers to questions. c. Pulls at the ears. d. Fails to respond when spoken to. e. Turns the good ear to the speaker. ANS: A, B, D, E Pulling at the ear is not a signal for hearing loss; all of the other options are. DIF: Cognitive Level: Comprehension REF: p. 1156 OBJ: 1 TOP: Behavioral Cues to Hearing Deficit KEY: Nursing Process Step: Assessment MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. Which common characteristics might a patient with conductive hearing loss display? (Select all that apply.) a. Hears adequately in noisy settings. b. Hears sounds but has difficulty understanding speech. c. Has improved hearing with hearing aids. d. Has a history of diabetes mellitus. e. Speaks in a normal volume. ANS: A, C, E Persons with conductive hearing loss can hear in a noisy setting and can have improved hearing with the use of hearing aids. Persons with conductive hearing loss speak at a normal or soft volume because they can hear themselves. Muffled sounds and a history of diabetes would be associated with sensorineural hearing loss. DIF: Cognitive Level: Comprehension REF: p. 1162 OBJ: 1 TOP: Common Characteristics in Persons with Conductive Hearing Loss KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A patient complains that his hearing aid is not working. What actions should a nurse implement to assess the device? (Select all that apply.) a. Check to see if the device is turned on. b. Clean the earpiece and remove cerumen clogged in the vent. c. Open the earpiece to see if the microphone wire is connected. d. Examine the interior of the earpiece for water. e. Validate that the battery is correctly placed. ANS: A, B, E Cleaning the earpiece to remove clogged cerumen and checking the device to see if it is turned on and if the battery is placed correctly are all good options. The earpiece should not be opened. If the hearing aid is still not working, it should be evaluated by the dealer. DIF: Cognitive Level: Application REF: pp. 1162-1163 OBJ: 3 TOP: Hearing Aids KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. A nurse assesses an 80-year-old patient for age-related changes to the eye. What potential changes should the nurse anticipate? (Select all that apply.) a. Decreased tear production b. Eyeball sunk deep in orbit c. Hyperopia d. Eyelashes diminished e. Arcus senilis ANS: A, B, C, E Eyelash diminution is not a consistent finding in older adults. All of the other options are common eye changes related to advancing age. DIF: Cognitive Level: Comprehension REF: p. 1143 OBJ: 1 TOP: Age-Related Changes in the Eye KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. What makes up the refractive media of the eye? (Select all that apply.) a. Aqueous humor b. Retina c. Vitreous humor d. Cornea e. Lens ANS: A, C, D, E The retina is not part of the refractive media. All of the other options are components of the refractive media. DIF: Cognitive Level: Knowledge REF: p. 1141 OBJ: 1 TOP: Refractive Media KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. What actions should a nurse implement when assessing a patient’s accommodation? (Select all that apply.) a. Hold his or her finger approximately 20 inches in front of the patient’s eyes. b. Observe for pupillary constriction. c. Assess for convergence. d. Note blinking. e. Move his or her finger slowly toward the patient’s nose. ANS: A, B, C, E Assessment for blinking is not part of the accommodation assessment. All of the other options are part of the accommodation assessment. The nurse holds his or her finger approximately 20 inches in front of the patient’s eyes and slowly moves the finger toward the patient’s nose, assessing for pupillary constriction and convergence. DIF: Cognitive Level: Application REF: p. 1145 OBJ: 2 TOP: Testing for Accommodation KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease COMPLETION 1. When planning care for a patient who cannot perceive or interpret sounds, a nurse takes into consideration that the patient may have a(n) _ hearing loss. ANS: central The inability to perceive or interpret sounds is referred to as a central hearing loss. DIF: Cognitive Level: Comprehension REF: p. 1163 OBJ: 1 TOP: Central Hearing Loss KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. A nurse uses a diagram to show the physiologic sequence of hearing. After entering the external ear, the sound is then conducted through the: (Arrange the options in sequence. Do not separate answers with a space or punctuation. Example: ABCD.) a. tympanic membrane b. sensory receptors c. oval window d. acoustic nerve to the brain e. malleus, incus, and stapes ANS: AECBD The sound impulse, after entering the external ear, is conducted through the tympanic membrane; into the malleus, incus, and stapes; through the oval window; into the sensory receptors in the inner ear; and then through the acoustic nerve to the brain. DIF: Cognitive Level: Comprehension REF: p. 1155 OBJ: 1 TOP: Physiology of Hearing KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 59: Eye and Vision Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A 60-year-old patient who has had an enucleation asks when he can get his prosthesis fitted. In approximately how many weeks should this patient expect to be fitted? a. 2 b. 4 c. 8 d. 12 ANS: B After an enucleation, the patient is fitted with a prosthesis in 1 month. DIF: Cognitive Level: Knowledge REF: p. 1183 OBJ: 2 TOP: Enucleation KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Basic Care and Comfort 2. A patient with glaucoma is taking a beta-adrenergic blocking agent, timolol (Timoptic). For which potential side effect should the nurse assess the patient? a. Wheezing b. Hypertension c. Sudden eye pain d. Blurred vision ANS: A Beta-adrenergic blocking agents cause bronchospasm and tachycardia. DIF: Cognitive Level: Comprehension REF: p. 1179 OBJ: 2 TOP: Beta-Adrenergic Blocking Agents KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 3. A 52-year-old patient reports that he must hold his paper farther and farther away from his face to read it. What is the nurse’s most informative response? a. “You are describing myopia. Glasses will help you read.” b. “You may have astigmatism, but your eyes will finally adjust.” c. “You have presbyopia. Nonprescription reading glasses will help you.” d. “An eye infection may be the problem. Check with your physician for medication.” ANS: C Presbyopia is a normal age-related change. Changes in the ciliary muscles cause the condition. Corrective lenses such as bifocals are used to correct this visual change. DIF: Cognitive Level: Application REF: pp. 1173-1174 OBJ: 2 TOP: Error of Refraction KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. A nurse explains that laser-assisted in situ keratomileusis (Lasik) and photorefractive keratectomy (PRK) are methods to correct refractive errors surgically. What do these procedures reshape? a. Cornea b. Lens c. Iris d. Pupil ANS: A Both surgical procedures are used to reshape the cornea. The clinician will need to determine which structure of the eye will need surgery to correct the vision. DIF: Cognitive Level: Knowledge REF: p. 1174 OBJ: 2 TOP: Surgical Treatment for Refractive Errors KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 5. A patient reports to a home health care nurse of having cloudy vision and seeing spots and halos around lights. What should the nurse suspect based on these patient symptoms? a. Cataracts b. Glaucoma c. Detached retina d. Macular degeneration ANS: A Cataracts are the cause of cloudy vision and seeing spots or halos. DIF: Cognitive Level: Comprehension REF: p. 1175 OBJ: 2 TOP: Internal Eye Disorders KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 6. How does closed-angle glaucoma differ from open-angle glaucoma? a. The onset is acute. b. Trabeculectomy is the initial treatment. c. Treatment can be conservative. d. Intraocular pressure drops suddenly. ANS: A Closed-angle glaucoma has an acute onset with eye pain and other systemic symptoms, such as nausea and vomiting. Reducing the intraocular pressure is an ocular emergency. DIF: Cognitive Level: Knowledge REF: p. 1178 OBJ: 2 TOP: Open-Angle versus Closed-Angle Glaucoma KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. What is the cause of glaucoma? a. Cloudiness in the lens b. Increase in intraocular pressure c. Failed eye surgery d. Retinal tears ANS: B Glaucoma is caused by an increase in intraocular pressure. DIF: Cognitive Level: Knowledge REF: p. 1178 OBJ: 2 TOP: Glaucoma KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Physiological Adaptation 8. A patient in the emergency department complains of severe pain in his eye and is seeing halos around lights and feeling nauseous. Which diagnosis should the nurse suspect? a. Open-angle glaucoma b. Angle-closure glaucoma c. Cataracts d. Retinal detachment ANS: B Sudden onset of acute eye pain with nausea and vomiting and halos around lights are all symptoms of angle-closure glaucoma. The acute pain is caused by sudden blockage of the fluid channels in the eye. DIF: Cognitive Level: Comprehension REF: p. 1178 OBJ: 2 TOP: Glaucoma KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. Which surgical implementation is most effective with retinal detachment? a. Removing the lens b. Macular bonding c. Lasik surgery d. Scleral buckling ANS: D Scleral buckling is used to hold the retinal repair in place. The band is left in place to keep together the layers of the eye tissue. DIF: Cognitive Level: Knowledge REF: p. 1182 OBJ: 2 TOP: Retinal Detachment KEY: Nursing Process Step: N/A MSC: NCLEX: Physiological Integrity: Basic Care and Comfort MULTIPLE RESPONSE 1. A patient who has had surgery this morning for cataracts is now going home. What should the nurse include when providing discharge instructions? (Select all that apply.) a. Sleep on the affected side. b. Use stool softeners. c. Avoid bending over. d. Avoid lifting anything heavier than 5 lb. e. Do not wear an eye shield at night. ANS: B, C, D After cataract surgery, the patient should sleep on the unaffected side with the eye shield in place. He or she should avoid heavy lifting and use stool softeners to prevent straining. DIF: Cognitive Level: Application REF: p. 1176 OBJ: 3 TOP: Discharge Instructions for Cataract Surgery KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 60: Ear and Hearing Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A 94-year-old patient is receiving gentamicin sulfate (Garamycin) in a continuous intravenous (IV) infusion. The nurse adds to the nursing care plan the patient problem “Potential injury.” What nursing action should be implemented? a. Pull side rails in place. b. Assist with ambulation. c. Measure intake and output. d. Provide for a possible seizure. ANS: C Reduced urine output would cause the drug to stay in the system rather than being excreted, which could result in a drug saturation. Gentamicin is ototoxic and can cause hearing impairment. DIF: Cognitive Level: Application REF: p. 1193 OBJ: 2 TOP: Gentamicin KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 2. A 75-year-old patient reports to a nurse that although she has cleaned her ears with cotton-tipped applicators for weeks, she still cannot hear her television unless the volume is loud, and she misses a great deal of conversations. What should the nurse anticipate when examining her ears? a. Otitis externa b. Purulent drainage c. Dry cerumen across the canal d. Pearly tympanic membrane ANS: C Obstruction of the external canal with cerumen will result in a hearing loss. Cleaning the ears with something such as an applicator will pack the cerumen in the canal. DIF: Cognitive Level: Comprehension REF: p. 1186 OBJ: 1 TOP: External Auditory Canal KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. Which patient problem should take priority in planning care for a patient with Ménière disease? a. Decreased socialization b. Potential injury c. Fluid volume deficit d. Inadequate nutrition ANS: B The patient problem that should take priority is that of preventing injury to the patient. A patient with Ménière disease is prone to falls because of dizziness. DIF: Cognitive Level: Application REF: p. 1191 OBJ: 2 TOP: Nursing Care Plan for Ménière Disease KEY: Nursing Process Step: Assessment MSC: NCLEX: Safe, Effective Care Environment: Safety and Infection Control 4. What information should a nurse stress when teaching a patient with Ménière disease about managing the disorder? a. Limiting fluid intake b. Avoiding the use of alcohol and tobacco c. Using antiemetic medications sparingly d. Staying active during the day ANS: B The use of alcohol and tobacco products affects the amount of fluid in the middle ear, worsening the symptoms of Ménière disease. The patient with Ménière disease should drink adequate fluid, use antiemetic medications as needed, and conserve energy during the day. DIF: Cognitive Level: Application REF: p. 1191 OBJ: 2 TOP: Ménière Disease KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. A patient comes to the primary care clinic complaining of a head cold and ear pain with drainage. What should the nurse suspect this patient is experiencing? a. Otitis externa b. Hearing loss c. Acute otitis media d. Mastoiditis ANS: C Acute otitis media is connected with colds and drainage from the ear. A hearing loss may be experienced as well, but the pain and drainage place the need to intervene for the infection first. DIF: Cognitive Level: Comprehension REF: p. 1187 OBJ: 1 TOP: Middle Ear KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 6. A young woman being admitted to the clinic service states that all the members of her family have been hard of hearing. She says her hearing loss became more pronounced when she was pregnant. What term explains this type of hearing loss? a. Otosclerosis b. Ototoxicity c. Otalgia d. Otitis media ANS: A Otosclerosis is hereditary, develops in young women, and worsens with pregnancy. DIF: Cognitive Level: Comprehension REF: p. 1188 OBJ: 1 TOP: Otosclerosis KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. What should a nurse include when educating a patient with Ménière disease? a. “When you feel dizzy, just stay in bed and take your medications.” b. “Decrease your sodium intake and take your diuretic medication between attacks.” c. “Vestibular rehabilitation might help, and you can still drink your morning coffee.” d. “Your vertigo will get better if you take your medications. You won’t need any relaxation techniques.” ANS: B A low-sodium diet and diuretic medications between attacks will prevent edema, which could cause an attack. DIF: Cognitive Level: Application REF: p. 1190 OBJ: 2 TOP: Inner Ear KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 8. A 75-year-old patient reports having difficulty hearing in crowds but can hear just fine at home with his wife. What hearing disorder should the nurse suspect? a. Otitis media b. Presbycusis c. Ototoxicity d. Central deafness ANS: B Presbycusis is a conductive hearing loss associated with normal aging and is caused by changes in the cochlea. DIF: Cognitive Level: Comprehension REF: p. 1191 OBJ: 1 TOP: Presbycusis KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. During an intake physical examination, a patient reports that he has been taking 10 aspirin tablets a day for his arthritis. What question should the nurse ask based on this information? a. “Can you hear high-pitched sounds?” b. “Have you noticed deafness in just one ear?” c. “Do you have ringing in your ears?” d. “Do you experience dizziness when you stand?” ANS: C A ringing in the ears (tinnitus) is an indication of aspirin toxicity. The patient should be advised to stop taking aspirin. DIF: Cognitive Level: Application REF: p. 1192 OBJ: 1 TOP: ASA Toxicity KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies COMPLETION 1. is the creation of a small opening in the tympanic membrane to reduce pressure and allow fluid to drain. ANS: Myringotomy Myringotomy is the creation of a small opening in the tympanic membrane to reduce pressure and allow fluid to drain. DIF: Cognitive Level: Knowledge REF: p. 1187 OBJ: 1 TOP: Myringotomy KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. are often formed when excess cells accumulate in a cyst or sac formed near the tympanic membrane. ANS: Cholesteatomas Cholesteatomas are often formed when excess cells accumulate in a cyst or sac formed near the tympanic membrane. DIF: Cognitive Level: Knowledge REF: pp. 1187-1188 OBJ: 1 TOP: Cholesteoatomas KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation Chapter 61: Psychobiological Disorders Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient is given anxiolytic medications for a mental disorder. What type of approach is this considered? a. Analytical b. Interpersonal c. Biologic d. Psychoanalytic ANS: C The biologic approach attempts to manage the physiologic effects of mental illness using medications. DIF: Cognitive Level: Comprehension REF: p. 1196 OBJ: 2 TOP: Psychiatric Disorders KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 2. A patient states that he feels angry at work for no reason and often yells at his co-workers. The therapist asks the patient to describe events and then tells the patient to try different strategies to cope with these angry outbursts. What type of approach is this considered? a. Biologic b. Analytical c. Cognitive or behavioral d. Interpersonal ANS: D The interpersonal approach helps the patient develop new coping skills. DIF: Cognitive Level: Comprehension REF: p. 1196 OBJ: 2 TOP: Psychiatric Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 3. What is the best action for the nurse to implement to effectively listen therapeutically to a patient? a. Concentrate on the patient and not think of responses to the patient while he or she is speaking. b. Determine the cause of the patient’s problem while the patient is speaking. c. Ask the patient why he thinks he feels the way he does. d. Tell the patient that you have had similar experiences. ANS: A To listen therapeutically, the nurse needs to concentrate on the patient and refrain from making up responses to the patient while he is speaking. DIF: Cognitive Level: Application REF: p. 1196 OBJ: 2 TOP: Establishing Therapeutic Relationships KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. A nurse speaking to a patient who is depressed says, “So what you are saying is that you are feeling very sad today.” What is this considered? a. Listening b. Sharing observations c. Clarifying d. Being available ANS: C By reflecting the meaning of the patient’s statement, the nurse is using clarification. This technique validates that the therapist understands what the patient is saying, and it provides validation for the patient. DIF: Cognitive Level: Comprehension REF: p. 1197 OBJ: 2 TOP: Establishing Therapeutic Relationships KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 5. When performing a mental status examination, a nurse notes that the patient keeps repeating, “I didn’t do it. I didn’t do it. I didn’t do it.” This response would be an example of which one of the components of the mental status examination? a. Appearance b. Mood and affect c. Thought content d. Memory and attention ANS: C Repetitive statements and thoughts are considered to be obsessive. This would be an element of the thought content component of the mental status examination. DIF: Cognitive Level: Comprehension REF: p. 1198 OBJ: 3 TOP: Mental Status Examination KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 6. A patient says, “I just don’t think I can keep going on. I just want it all to end.” The nurse assesses that this patient has suicidal ideation. What is the nurse’s best response? a. “Do you have any thoughts of harming yourself?” b. “Have you felt like this before?” c. “You are just depressed. When you feel better, you won’t think that way.” d. “We will keep you safe here.” ANS: A The best response to a patient who may have suicidal ideation is to ask a simple direct question to determine the patient’s true intent. Having done that, this should be reported at once. All suicidal threats, even mild ones, should be reported and taken seriously. DIF: Cognitive Level: Application REF: p. 1199 OBJ: 3 TOP: Mental Status Examination KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 7. What should a nurse suspect a patient diagnosis might be when the patient states, “I often feel restless, have a tight sensation in my chest, and have an increased heart rate at times”? a. Anxiety disorder b. Depressive disorder c. Agoraphobia d. Obsessive-compulsive disorder ANS: A The patient is reporting symptoms that reflect signs of an anxiety disorder. DIF: Cognitive Level: Comprehension REF: p. 1200 OBJ: 6 TOP: Anxiety Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 8. A group of nursing students are taking their first major examination. What should the nursing instructor expect the students might experience? a. Posttraumatic stress disorder b. Panic disorder c. Mild anxiety d. Moderate anxiety ANS: C The students are usually experiencing mild anxiety, which can be beneficial as a motivator. DIF: Cognitive Level: Comprehension REF: p. 1204 OBJ: 6 TOP: Anxiety Disorders KEY: Nursing Process Step: N/A MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 9. A patient who is admitted with posttraumatic stress disorder (PTSD) says he had a very stressful experience when in high school and has never really recovered. What is the most appropriate nursing action? a. Encourage the patient to talk about what caused the traumatic event. b. Guide the patient in relaxation techniques to distract him when flashbacks occur. c. Provide sleeping medication so that he can sleep at night. d. Allow the patient to talk about his condition as often as he likes. ANS: B Patients with PTSD should not be encouraged to talk about the traumatic event. The patient should learn relaxation techniques to distract themselves when anxiety symptoms begin. Sedation does not address the problem of anxiety. DIF: Cognitive Level: Application REF: p. 1202 OBJ: 7 TOP: Posttraumatic Stress Disorder KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 10. A patient admitted with a conversion disorder after an automobile accident insists he is paralyzed, although no physical cause for his paraplegia can be found. What is the best nursing response when the patient asks the nurse to push him to his room? a. “There is nothing wrong with your arms. Roll yourself to your room.” b. “I will help you to walk to your room. I know you can walk.” c. “Let me lift the foot rests so you can move your chair with your feet.” d. “OK. I am going that way myself.” ANS: D The patient is experiencing dysfunction without a discernible cause, but this dysfunction is very real to him. The less attention brought to his coping mechanism, the better. DIF: Cognitive Level: Application REF: p. 1203 OBJ: 7 TOP: Somatoform Disorders KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 11. Which combination of medications could be used to treat an anxiety disorder? a. Librium and Xanax b. Effexor and Ativan c. Effexor and Haldol d. Klonopin and Valium ANS: B A combination of an antidepressant and anxiolytic medication is recommended as the appropriate drug therapy for the patient with an anxiety disorder. Xanax, Librium, Ativan, Valium, and Klonopin are all anxiolytic medications. Haldol is a neuroleptic medication, and Effexor is an antidepressant. DIF: Cognitive Level: Knowledge REF: pp. 1203-1204 OBJ: 4 TOP: Drug-Related Responses KEY: Nursing Process Step: N/A MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 12. A patient who went away to college in September returns in October, thinking that he is a drummer in a popular rock band. What is this most likely a manifestation of? a. Dissociative disorder b. Conversion disorder c. Schizophrenia d. Amnesia ANS: C Schizophrenia occurs in adolescence or early adulthood. The patient experiences delusions that are characteristic of schizophrenia in a classic stress situation, which may have been the precipitating event that caused the thought disorder. DIF: Cognitive Level: Comprehension REF: p. 1205 OBJ: 6 TOP: Schizophrenia KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity 13. A patient is receiving large doses of chlorpromazine (Thorazine) and begins to exhibit extrapyramidal signs of involuntary muscle movement. Which classification of drugs should the nurse anticipate will be added to the patient’s protocol? a. Antiparkinsonian b. Antihypertensive c. Anticonvulsant d. Antiemetic ANS: A Antiparkinsonian drugs will control the muscle movement and drooling that are the major signs of neuroleptic toxicity. DIF: Cognitive Level: Comprehension REF: pp. 1206-1207 OBJ: 7 TOP: Neuroleptic Medications KEY: Nursing Process Step: N/A MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 14. A long-time patient with schizophrenia in the inpatient unit has developed involuntary movements of his tongue. What has this patient developed? a. Acute dystonic reaction b. Tardive dyskinesia c. Neuroleptic malignant syndrome d. Laryngospasm ANS: B Tardive dyskinesia is a side effect of continued use of neuroleptic medications to control schizophrenia. DIF: Cognitive Level: Knowledge REF: pp. 1206-1207 OBJ: 4 TOP: Schizophrenia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 15. Which is not considered as a probable cause of mood disorders? a. Loss of significant others b. Learned helplessness c. Neurotransmitter dysregulation d. Traumatic event in childhood ANS: D A traumatic event in childhood could, most likely, cause PTSD. All other options are causes of mood disorders. DIF: Cognitive Level: Knowledge REF: p. 1209 OBJ: 5 TOP: Mood Disorders KEY: Nursing Process Step: N/A MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 16. A patient with bipolar disorder is being treated with tricyclic medications. What should the nurse inform the patient to expect when teaching information concerning side effects? a. Orthostatic hypotension b. Hypercholesterolemia c. Fatigue d. Blurred vision ANS: A Orthostatic hypotension and urinary retention are side effects of tricyclic antidepressants. These drugs are commonly used to treat the depressant effects of bipolar disorders. DIF: Cognitive Level: Comprehension REF: p. 1211 OBJ: 4 TOP: Drug Treatment KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 17. A patient is hyperactive with mania and has poor nutritional intake due to hyperactivity. What implementation is most appropriate when considering this diagnosis? a. Offer nutritious finger foods and high-protein milk shakes to eat on the go. b. Spoon-feed the patient while the patient is seated at the table. c. Arrange for one large meal at noon to be eaten in the company of others. d. Limit fluid intake to make the patient hungry at mealtime. ANS: A Patients with mania are on the go. Nutritious foods that can be eaten while the patient is moving around will meet their dietary needs. The patient’s short attention span prevents him or her from sitting long enough to eat or to be fed by spoon. Limiting fluids is contraindicated for the patient who is hyperactive. DIF: Cognitive Level: Application REF: p. 1213 OBJ: 7 TOP: Manic Behavior KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 18. A patient is brought in from the emergency department after telling the physician that he is a relative of the president of the United States. He says that he should not be detained because he has important business to attend to that involves national security. He is dressed in a bright coat with plaid pants and gets very angry when you try to question him. What is this patient is experiencing? a. Panic attack b. Hyperactive episode c. Extrapyramidal effect d. Manic episode ANS: D Inappropriate dress, self-aggrandizement, hyperactivity, and frustration are elements of a manic episode. DIF: Cognitive Level: Comprehension REF: p. 1213 OBJ: 6 TOP: Nursing Care of the Patient with Bipolar Disorder with Manic Episodes KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 19. While in the dayroom, one of the patients becomes very agitated and begins to threaten to harm the other patients and is directing violence at the other patients and staff. What is the most appropriate nursing implementation? a. Decrease the stimuli and use restraints if all other measures fail. b. Offer to call the physician and ask another staff member to call security. c. Remove harmful objects and try to perform relaxation exercises with the patient. d. Restrain the patient and do not allow him or her to eat or drink anything by mouth. ANS: A Because the patient is threatening to harm others, decreasing stimuli will be helpful to decrease the behavior and, if everything else fails, restraints will be needed. Restraints should be applied according to current policy. Patients who are being restrained need to have frequent checks and their nutritional and elimination needs monitored. DIF: Cognitive Level: Application REF: p. 1213 OBJ: 7 TOP: Nursing Implementations for Manic Episodes KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 20. Since the summer weather began, a patient taking lithium for manic episodes has been walking daily. What important instruction should the nurse provide to this patient? a. Stay in the shade when walking. b. Stop walking. c. Maintain hydration. d. Wear sunscreen. ANS: C Lithium toxicity can occur if the patient becomes dehydrated. The therapeutic range of lithium is narrow; consequently, toxicity to this drug is common. DIF: Cognitive Level: Application REF: p. 1210 OBJ: 7 TOP: Medications for Manic Episodes KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 21. A patient who has a history of episodes of road rage thinks that she is a very good driver and does not understand why she keeps being told she is a poor driver. She is losing her license now, and she tells the nurse that she is feeling very unhappy and abandoned. She feels like she might hurt herself. The nurse realizes that the patient is exhibiting which personality disorder? a. Narcissistic b. Paranoid c. Schizoid d. Borderline ANS: D Difficulty controlling anger and an unstable sense of self are elements of a borderline personality disorder. DIF: Cognitive Level: Comprehension REF: p. 1215 OBJ: 6 TOP: Personality Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity 22. A co-worker is noted to be very organized. However, you see that he is always making lists and citing the rules of the organization. He wants all his projects to be perfect and gets very upset when things happen that make him miss his deadlines. The co-worker is exhibiting signs of which personality disorder? a. Avoidant b. Obsessive-compulsive c. Histrionic d. Dependent ANS: B Patients who have a preoccupation with perfectionism, orderliness, and control have an obsessive-compulsive personality disorder. These patients may be anxious and attempt to maintain the perfectionism. The patient data in this question demonstrate the elements of obsessive-compulsive disorder. DIF: Cognitive Level: Comprehension REF: p. 1201 OBJ: 6 TOP: Personality Disorders KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 23. What is a common cause of delirium? a. Overuse of steroids b. Liver abnormalities c. Parkinson disease d. Neoplasms ANS: D Neoplasms and Alzheimer disease are two causes of delirium. All of the other options are causes of dementia. DIF: Cognitive Level: Knowledge REF: p. 1214 OBJ: 6 TOP: Cognitive Disorders KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Physiological Adaptation MULTIPLE RESPONSE 1. A nurse is assessing a patient with an acute stress disorder. What characteristics of this disorder should the nurse assess? (Select all that apply.) a. Diminished awareness of surroundings b. Derealization c. Depersonalization d. Amnesia e. Irritability ANS: A, B, C, D Individuals who have been overcome by an acute stress disorder exhibit diminished orientation, reality testing, and personal awareness, and they frequently experience amnesia. Irritability is not part of the syndrome. DIF: Cognitive Level: Comprehension REF: p. 1202 OBJ: 6 TOP: Acute Stress Disorder KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 2. A nursing instructor is explaining the difference between illusion and hallucination. Which examples provided by students in the class indicate an illusion? (Select all that apply.) a. A car backfiring being perceived as gunfire b. The television news being perceived as someone talking to you c. Hearing God’s voice directing you to drive your car off the road d. Seeing your dead spouse smile at you from a flower e. A spot on the wall being perceived as a spider ANS: A, B, E An illusion has an external stimulus that causes an erroneous translation. Anyone, even a person with intact sensorium, can have an illusion. An example of an illusion is seeing water on the highway, which is really only heat waves. A hallucination has no external stimulus. An example of a hallucination is a person with alcoholism seeing spiders crawling on the ceiling. DIF: Cognitive Level: Comprehension REF: p. 1199 OBJ: 6 TOP: Hallucinations versus Illusions KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation COMPLETION 1. When a nurse asks questions like, “What day is today?” or “What time is it now?” the nurse is testing the patient’s . ANS: sensorium The sensorium is also referred to as orientation. The sensorium orients the person to person, place, and time. DIF: Cognitive Level: Comprehension REF: p. 1198 OBJ: 6 TOP: Sensorium KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity Chapter 62: Substance Abuse Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient has been diagnosed with alcoholism. A nurse tells him that he has a physical illness with a genetic predisposition to alcoholism, and the only effective treatment is total abstinence from alcohol. This type of approach characterizes which theory? a. Biologic b. Behavioral c. Sociocultural d. Intrapersonal ANS: A The biologic approach is based on the theory that there is a faulty physiologic process that causes a predisposition to an addiction. This theory includes the belief that such an addition is incurable and only total abstinence will be effective. DIF: Cognitive Level: Comprehension REF: p. 1220|p. 1240 OBJ: 1 TOP: Etiology and Risk Factors KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 2. During the taking of a medical history, a patient who is addicted to heroin reports he only uses the drug a few times a week. What is the nurse’s best response when trying to disclose more precise information? a. “OK. You only use heroin two times a week?” b. “What do you mean when you say ‘a few?’” c. “Are you saying that in a week’s time would you use heroin only two times?” d. “Rate your weekly usage on a scale of 1 to 15.” ANS: D When trying to get a health history on a patient with a substance abuse problem, the best method is an open discussion of the drug use. The discussion should be open and nonjudgmental. By requesting a scale, the patient’s response will be more informative. DIF: Cognitive Level: Application REF: p. 1221 OBJ: 5 TOP: Nursing Assessment of the Substance Abuser KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. A patient who has alcoholism with a history of heavy drinking is brought to the inpatient psychiatric unit saying that he does not know where he is or what day it is. What should the nurse suspect he is exhibiting? a. Delirium b. Alcoholic dementia c. Blackout d. Amnesia ANS: C Blackouts are common with heavy drinking over time. The patient data support that the memory loss is associated with the alcohol use and that blackouts would be an expected outcome. DIF: Cognitive Level: Comprehension REF: p. 1222 OBJ: 3 TOP: Patterns and Consequences of Abuse KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 4. A nurse is discharging a patient with a pulmonary disorder to return home with her family. She has had a difficult time while in the hospital and has experienced withdrawal from tobacco. When the nurse tells her that community resources are available to help her to stop smoking, she says, “That’s OK. I can stop whenever I want to.” What does this exemplify? a. Rationalization b. Denial c. Intellectualization d. Projection ANS: B Denial is a common defense mechanism used by substance abusers. DIF: Cognitive Level: Application REF: p. 1222 OBJ: 3 TOP: Defense Mechanisms KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 5. A patient with an alcohol addiction says, “My drinking is all my wife’s fault. She makes me so crazy I just have to have a drink.” What does this exemplify? a. Rationalization b. Denial c. Intellectualization d. Projection ANS: D The patient in this scenario is projecting. He is blaming his wife for his drinking problem, rather than accepting that the drinking is his problem. DIF: Cognitive Level: Application REF: p. 1222 OBJ: 3 TOP: Defense Mechanisms KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 6. Which information about a patient should lead a nurse to suspect substance abuse? a. Abnormal liver function test result and a gastrointestinal (GI) bleed b. Positive syphilis screening result and varicose veins c. Fungal infection and a potassium level of 4.2. mEq/L d. Decreased albumin level and creatinine level of 1.2 mg/dL ANS: A An abnormal liver function test result and a gastrointestinal bleed indicate substance abuse. DIF: Cognitive Level: Comprehension REF: p. 1223|p. 1225 OBJ: 5 TOP: Diagnostic Tests KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 7. A urine drug screen is ordered for a patient suspected of a driving while intoxicated (DWI). What drugs are included in this screening? a. Lysergic acid diethylamide (LSD), Valium, and Percocet b. Crack, heroin, and nonsteroidal anti-inflammatory drugs (NSAIDs) c. Marijuana, amphetamines, and Elavil d. Librium, cocaine, and Zoloft ANS: A LSD, Valium, and Percocet have the correct combination of an illicit drug, an anxiolytic medication, and an opioid. DIF: Cognitive Level: Knowledge REF: p. 1223 OBJ: 5 TOP: Urine Drug Screening KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 8. An alcoholic is brought into the emergency department in an intoxicated state at 2000. The day shift nurse assesses the patient to exhibit tremors, have increased blood pressure, and agitation at 0800 rounds. What do these signs and symptoms indicate? a. Major withdrawal b. Early withdrawal c. Delirium tremens d. Minor withdrawal ANS: B The signs of early withdrawal from alcohol are agitation and elevated vital signs. These warning signs usually occur 6 to 12 hours after the last drink. DIF: Cognitive Level: Comprehension REF: p. 1225 OBJ: 3 TOP: Alcoholism KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 9. Which syndrome of alcoholism is related to thiamine deficiency? a. Fetal alcohol syndrome b. Wernicke encephalopathy c. Korsakoff psychosis d. Alcoholic dementia ANS: B Wernicke encephalopathy is a vitamin B1 (thiamine) deficiency. If not treated with vitamin supplements, the condition can progress to a more serious form. DIF: Cognitive Level: Knowledge REF: p. 1225 OBJ: 3 TOP: Medical Complications KEY: Nursing Process Step: N/A MSC: NCLEX: Physiological Integrity: Physiological Adaptation 10. A wife of a man with long-term alcoholism wants to help her husband quit drinking. The nurse tells her that an initial approach might be for a group of friends and family to confront the patient with his alcoholism. What should this group be prepared to indicate during this confrontation? a. He needs help; his drinking is out of hand. b. They are fed up with him and will no longer be his friend. c. They reject his drinking but think he is a valuable person. d. He is still their friend even if he does not stop drinking. ANS: C The implementation for encouraging an alcoholic to go into treatment consists of a group of people telling the alcoholic that they think his drinking is destructive, but they do not reject him as a person. DIF: Cognitive Level: Comprehension REF: p. 1228 OBJ: 6 TOP: Implementation KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 11. A nurse recommends to an alcoholic that he join Alcoholics Anonymous. What is true about this organization? a. Based on a 12-step approach with a strong religious base b. A social group of ex-drinkers who befriend one another in the process of maintaining sobriety c. A religious support group that assists alcoholics during rehabilitation d. An anonymous group of sponsors who offer help to alcoholics ANS: A Alcoholics Anonymous is a group of people who come together to offer support to each other to stay sober. It has a religious base, recognizes a higher power, and uses a 12-step approach to sobriety. DIF: Cognitive Level: Comprehension REF: p. 1228 OBJ: 6 TOP: Rehabilitation KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychological Integrity: Coping and Adaptation 12. What should be avoided to prevent the accidental activation of Antabuse? a. Aged cheese b. Pickled foods c. Mouthwash d. Chocolate candy ANS: C Mouthwash contains alcohol and can trigger the effect of an Antabuse reaction. The alcoholic taking Antabuse needs to be aware of the hidden alcohol in some commonly used mouthwashes and other over-the-counter drugs. DIF: Cognitive Level: Application REF: p. 1231 OBJ: 6 TOP: Medications KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 13. A nurse in the admissions unit is informed that a patient is being brought in who has been using “ice.” What should the nurse assess? a. Extreme dehydration b. Coma c. Dangerous hypertension d. Violent behavior ANS: D Persons who use “ice,” a form of methamphetamine, are frequently violent while under its influence. The effect of “ice” can last as long as 12 to 14 hours. DIF: Cognitive Level: Comprehension REF: p. 1234 OBJ: 3 TOP: Stimulants KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 14. An LPN is assisting with the development of a nursing care plan for a patient who has been using cocaine for 5 years. What should the nurse consider will most commonly need to be dealt with in this patient? a. Depression b. Violent behavior c. Nasal erosion d. Suicide attempts ANS: A Cocaine users can be depressed for as long as 2 years after quitting drug use. An antidepressant such as bupropion (Wellbutrin) is helpful in treating the depression. DIF: Cognitive Level: Comprehension REF: p. 1234 OBJ: 6 TOP: Cocaine KEY: Nursing Process Step: Planning MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 15. What might the positive effects of marijuana be used to treat? a. Diet control in morbidly obese patients b. Chemotherapy-induced nausea and vomiting c. Air hunger in patients with end-stage emphysema d. Early diabetic-induced cataracts ANS: B Marijuana has been studied for use to reduce nausea and vomiting in patients with cancer. Marinol (Dronabinol) is a marijuana derivative that is currently used to reduce chemotherapy-induced nausea and vomiting. DIF: Cognitive Level: Comprehension REF: p. 1232 OBJ: 6 TOP: Hallucinogens KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 16. A nurse is counseling a pregnant cocaine abuser. What should the nurse inform this patient that she is placing her baby at significant risk for? a. Severe allergies b. Neurologic impairments c. Hearing impairment d. Higher birth weights ANS: B Babies born to mothers who are addicted to cocaine have a higher incidence of hyperactivity and neurologic problems. DIF: Cognitive Level: Comprehension REF: p. 1235 OBJ: 7 TOP: Disorders Associated with Cocaine Use KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 17. What is the rationale for using methadone in the treatment of heroin abuse? a. Substitutes one opioid for another. b. Is less constipating than heroin. c. Does not give the “rush” that a person addicted to heroin is looking for. d. Is a synthetic opioid, which makes it less addicting. ANS: C Methadone, as an extended-release medication, does not give the “rush” that addicts enjoy. It maintains the opioid level in the body but does so at a steady state and decreases cravings. DIF: Cognitive Level: Application REF: p. 1235 OBJ: 6 TOP: Medications KEY: Nursing Process Step: N/A MSC: NCLEX: N/A 18. Narcan has been given to a person with respiratory depression who is addicted to heroin. What should the nurse be alert for indications of? a. Acute withdrawal symptoms b. Respiratory arrest c. Hypotensive crisis d. Cardiac arrest ANS: A Narcan is an opioid antagonist that causes the opioid to fall from receptor sites. When the antagonist is given, the sudden loss of the opioid causes acute withdrawal to occur. DIF: Cognitive Level: Application REF: p. 1236 OBJ: 6 TOP: Medications: Narcan KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 19. Two treatment plans for abusers of alcohol and drugs are similar—90 meetings in 90 days and 12-step programs. What is the major difference in the success of the two types of programs? a. One program uses a 12-step approach, and the other program has a religious base. b. Heroin addicts have a higher success rate. c. Alcohol abusers have an easier time staying with the program. d. Relapse rates for patients using drugs other than alcohol alone are much higher. ANS: D One difference between alcohol and drug rehabilitation programs is that drug abusers will have a lower success rate. Alcohol abusers have a higher rate of success when they follow the Alcoholics Anonymous program. DIF: Cognitive Level: Comprehension REF: p. 1236 OBJ: 6 TOP: Rehabilitation KEY: Nursing Process Step: Evaluation MSC: NCLEX: Psychosocial Integrity: Psychosocial Adaptation 20. Which implementation can be used to help prevent relapse in a patient who has a substance abuse problem? a. Self-hypnosis b. Imagery c. Stress management d. Blocking ANS: C Teaching stress management techniques to patients who have a substance abuse problem will assist them in managing the conflict and stress in their daily lives, which previously triggered the substance abuse. DIF: Cognitive Level: Comprehension REF: p. 1229 OBJ: 6 TOP: Implementation KEY: Nursing Process Step: Implementation MSC: NCLEX: Psychosocial Integrity: Coping and Adaptation 21. In some cases, patients will use drugs or alcohol to treat the disturbing symptoms of a psychiatric disease. What can occur in this scenario? a. A mixed-drug reaction, which may heighten the effects of both drugs b. Decreased psychiatric symptoms, which makes the psychiatric condition harder to treat c. An accidental overdose by mixing alcohol with anxiolytic medications, antipsychotic medications, or antidepressants d. An increase in psychiatric symptoms because the psychiatric drugs become less effective in the presence of alcohol ANS: C Combining alcohol and psychiatric drugs, anxiolytics, or antidepressants may cause an accidental overdose by increasing the central nervous system effects. DIF: Cognitive Level: Application REF: pp. 1239-1240 OBJ: 7 TOP: The Dually Diagnosed KEY: Nursing Process Step: Assessment MSC: NCLEX: Psychosocial Integrity: Pharmacological Therapies MULTIPLE RESPONSE 1. A nurse indicates that a urine sample is needed for screening in a case of DWI. What actions should be implemented? (Select all that apply.) a. Collection and witnessing by a staff member of the same gender b. Documented with a chain-of-custody form signed by all who handle the specimen c. Keep specimen under secure conditions if temporary storage is necessary d. Never be out of sight until someone from law enforcement takes it e. Place in a specially marked container ANS: A, B, C The specimen, if placed in secure storage, does not have to be in sight nor does it need a specially marked container. DIF: Cognitive Level: Application REF: p. 1223 OBJ: 5 TOP: Urine Screening KEY: Nursing Process Step: Implementation MSC: NCLEX: Safe, Effective Care Environment: Prevention and Early Detection of Disease 2. A nurse documents signs of Wernicke encephalopathy in a patient with long-term alcoholism. What do these signs include? (Select all that apply.) a. Confabulation b. Ataxia c. Delirium d. Decreasing level of consciousness e. Projectile vomiting ANS: A, B, C, D The signs of Wernicke encephalopathy do not include projectile vomiting. DIF: Cognitive Level: Knowledge REF: p. 1225 OBJ: 5 TOP: Wernicke Encephalopathy KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 3. What does alcohol abuse in the older adult place him or her at risk for? (Select all that apply.) a. Falls b. Malnutrition c. Respiratory infections d. Bone demineralization e. Cirrhosis ANS: A, B, D, E Alcohol abuse in the older adult makes the person at risk for falls, malnutrition, cirrhosis, and bone demineralization. DIF: Cognitive Level: Knowledge REF: p. 1238 OBJ: 7 TOP: Alcohol Abuse in the Older Adult KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 4. What is true regarding hair analysis done on an alcoholic? (Select all that apply.) a. Requires sensitive technology b. Is not reliable on treated or dyed hair c. Can determine addiction d. Can be informative in the treatment of a short-term abuser e. Can assess relapse ANS: A, E Hair analysis requires sensitive technology, can be used on treated or dyed hair, and can assess a relapse. Hair analysis cannot confirm addiction, only use, and it is not informative on short-term abusers. DIF: Cognitive Level: Knowledge REF: p. 1223 OBJ: 2 TOP: Hair Analysis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 5. What factors make the adolescent extremely vulnerable to substance abuse (Select all that apply.) a. Egocentricity b. Ability to use good judgment c. Poor impulse control d. Awareness of possible consequences e. Desire for peer identification ANS: A, C, E Adolescents are prone to substance abuse because of peer pressure and their basic egocentrism, which interferes with good judgment, prediction of consequences, and impulse control. DIF: Cognitive Level: Comprehension REF: p. 1239 OBJ: 7 TOP: Adolescents KEY: Nursing Process Step: N/A MSC: NCLEX: N/A COMPLETION 1. A nurse explains that a test that can detect substance abuse for up to 1 year after only 2 or 3 days of use is performed on . ANS: hair Hair can indicate drug abuse up to a year even if the abuse was only a matter of days. DIF: Cognitive Level: Knowledge REF: p. 1223 OBJ: 2 TOP: Hair Analysis KEY: Nursing Process Step: Implementation MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease Chapter 63: First Aid, Emergency Care, and Disaster Management Linton: Medical-Surgical Nursing, 7th Edition MULTIPLE CHOICE 1. A patient is present with signs of severe airway obstruction. What term accurately describes the high-pitched noise the patient is exhibiting with inhalation? a. Stridor b. Tachypnea c. Wheezing d. Rhonchi ANS: A Signs of severe airway obstruction are poor or no air exchange, poor or no cough, high-pitched noise known as stridor on inhalation, respiratory distress, cyanosis, inability to speak, inability to move air, and clutching the neck. DIF: Cognitive Level: Comprehension REF: p. 1246 OBJ: 3 TOP: Airway Obstruction KEY: Nursing Process Step: Knowledge MSC: NCLEX: Physiological Integrity: Physiological Adaptation 2. Standing in a fast-food line, the person in front, while munching on a cookie, begins to cough heavily, takes deep inspirations, and waves his arms around wildly. What should be the nurse’s first action? a. Start rescue breathing as quickly as possible. b. Start chest compressions as quickly as possible. c. Perform abdominal thrusts. d. Do nothing at this point as long as air is exchanged. ANS: D When a person is choking but alert enough to attempt to cough and force the obstruction up and out by himself, allowing him to do so alone is best because more expelling force occurs that way. Only when the person shows signs of not being able to breathe beyond the obstruction should abdominal thrusts be applied. DIF: Cognitive Level: Application REF: p. 1246 OBJ: 4 TOP: Immediate Intervention for a Choking Victim KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 3. What is the initial intervention for an unconscious patient who is not breathing according to one-person CPR principles, as taught and practiced by professional nurses? a. Lift the jaw to clear the airway. b. Call for assistance. c. Start chest compressions. d. Remove patient clothing to visualize the chest. ANS: B With one-person CPR, when the patient is unconscious and not breathing, the first thing to do is to call for help. DIF: Cognitive Level: Comprehension REF: p. 1245 OBJ: 3 | 4 TOP: CPR Guidelines KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 4. While ambulating, a patient gasps and drops to the floor unconscious with no pulse or respiration. When is the nurse aware that brain cells begin to die? a. 1 minute b. 2 minutes c. 3 minutes d. 4 minutes ANS: D Without adequate perfusion, the brain cells begin to die in 4 minutes. DIF: Cognitive Level: Comprehension REF: p. 1245 OBJ: 3 TOP: Brain Damage KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Physiological Adaptation 5. A nurse follows the protocol of SAMPLE when speaking to a victim of a fall in the parking lot of the hospital. What does the P stand for? a. Pills taken today b. Personal physician c. Past illnesses d. Preference for emergency transportation ANS: C The acronym SAMPLE that guides the victim interview means allergies, medications, past illness or pregnancy, last food and drink, and events related to injury. DIF: Cognitive Level: Knowledge REF: p. 1244 OBJ: 3 TOP: SAMPLE Protocol KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 6. What instructions should the nurse provide for immediate treatment for epistaxis? a. “Stand still, lean your head back so that the blood won’t get all over everything, and pinch your nose shut for at least 10 minutes.” b. “Stand still, lean your head forward, and pinch your nose tightly for at least 10 minutes.” c. “Sit down on a solid surface, lean your head forward to let the blood run out, and then pinch your nose closed for at least 30 minutes.” d. “Sit down on a solid surface, lean your head forward so you don’t choke on the blood, and pinch your nose shut for at least 10 minutes.” ANS: D Blood from a nosebleed in the anterior portion of the nasal cavity will usually stop with pinch pressure within 10 minutes. Blood from a nosebleed should not be swallowed. DIF: Cognitive Level: Application REF: p. 1247 OBJ: 4 TOP: First Aid for a Nosebleed KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 7. Which condition may complicate the assessment of an older adult patient with a suspected head injury? a. Sensory deficits b. Slowed metabolism c. Preexisting cerebral dysfunction d. Decreased pulmonary function ANS: A Sensory deficits, circulatory disorders, and communication problems make it more difficult to assess an older adult patient with a suspected head injury. DIF: Cognitive Level: Comprehension REF: p. 1248 OBJ: 3 TOP: Head Injury in Older Adults KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 8. A nurse is called on to assist a neighbor who needs first aid. What should the nurse know is the legal responsibility for this action? a. Is legally bound to help in any way possible. b. Is expected to demonstrate the same skill, knowledge, and care that would be provided by other nurses in the same community with the same credentials. c. Has no legal responsibilities outside the hospital setting and would be held accountable for nothing. d. Can legally perform any aid skill, even those not allowed the nurse in the hospital. ANS: B U.S. laws protect nurses when they act in the same manner as others licensed at their level would do in the same circumstances. DIF: Cognitive Level: Comprehension REF: p. 1260 OBJ: 6 TOP: Legal Assistance KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 9. A nurse comes upon a traffic accident where injured, unconscious people are lying on the highway. What should the nurse be aware of regarding the sanctioning of first-aid interventions in this scenario? a. Good Samaritan Law b. Emergency Care Doctrine c. Fifth Amendment d. Liability Protection against Malpractice Act ANS: A Most states have Good Samaritan Acts, which protect voluntary caregivers from malpractice claims. DIF: Cognitive Level: Knowledge REF: p. 1260 OBJ: 7 TOP: First Aid for an Unconscious Patient KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 10. What will the nurse giving discharge instructions to a patient who is severely allergic to insect stings caution the patient to do? a. Wear bright colors to repel insects. b. Apply perfume liberally as a protection. c. Dress in sleeveless, easily removeable garments. d. Obtain an emergency treatment kit. ANS: D An emergency kit with Benadryl or injectable epinephrine or both are recommended. Insects are attracted by bright colors and perfume. Arms and legs should be covered with clothing. DIF: Cognitive Level: Application REF: p. 1256 OBJ: 4 TOP: Severe Allergic Reaction Prevention KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Pharmacological Therapies 11. A patient is admitted to the emergency department after having been bitten on the hand by a black widow spider. Which nursing intervention should the nurse initiate? a. Monitor for respiratory distress. b. Wrap the hand in a warm compress. c. Seat the patient upright in a chair. d. Elevate the patient’s hand above his or her heart. ANS: A Neurotoxins frequently cause anaphylaxis with severe respiratory distress and seizure. Therefore, the patient should be protected from falls, and the hand kept cool and below the heart to delay the spread of the toxin. DIF: Cognitive Level: Application REF: p. 1258 OBJ: 4 TOP: Neurotoxins KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 12. A nurse who is assisting victims of an automobile collision has already placed a towel secured with a belt on a bleeding leg wound. What action should the nurse take when the towel becomes saturated? a. Do nothing. b. Remove the towel and use the belt as a tourniquet. c. Remove the towel and place the victim’s jacket over the wound and secure it. d. Reinforce the towel with the victim’s jacket. ANS: D Direct and continuous pressure is the intervention for a bleeding wound. The original dressing should not be removed but should be reinforced. DIF: Cognitive Level: Application REF: p. 1247 OBJ: 4 TOP: Bleeding Wound KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 13. An accident victim comes to the emergency department with an open chest wound. What should the nurse apply to the wound? a. Occlusive dressing taped on four sides b. Tight Ace wrap c. No dressing of any sort d. Vented dressing, taped on three sides ANS: D A vented dressing taped on three sides allows no more air to enter the pleural space but allows the expanding lung to push air out. A four-sided dressing allows the trapped air to remain and possibly collapse the lung. DIF: Cognitive Level: Application REF: p. 1251 OBJ: 4 TOP: Open Chest Wound KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 14. A homeless person is brought to the emergency department after having been found asleep on a park bench under a layer of snow. He has a rectal temperature of 95 F. Which additional symptoms should the nurse anticipate? a. Diminished breath sounds and inadequate chest expansion b. Shivering, decreased heart rate, and increased blood pressure (BP) c. Confusion, increased hunger, and hypertension d. Decreased irregular heart and respiratory rates and decreased BP ANS: D A patient with hypothermia will continue to chill as his or her vital signs deteriorate. DIF: Cognitive Level: Comprehension REF: p. 1253 OBJ: 4 TOP: Hypothermia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 15. A mother brings in her 2-year-old who has ingested gasoline 1 hour earlier. What should the nurse implement following the initial assessment? a. Prepare to administer syrup of ipecac. b. Turn the patient on his or her stomach to induce vomiting. c. Prepare to administer Milk of Magnesia. d. Prepare to administer bowel lavage and cathartics. ANS: D Bowel lavage and cathartics will rid the body of the petroleum product. Inducing vomiting when the patient has consumed petroleum products is contraindicated. Ipecac is no longer recommended, and Milk of Magnesia will not be effective. DIF: Cognitive Level: Application REF: p. 1255 OBJ: 2 TOP: Poisoning KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 16. While at the local pool on an extremely hot day, a nurse is called on to care for a woman who has evidently developed heat exhaustion. What is the initial nursing care for this person? a. Obtain vital signs. b. Move the patient into an air-conditioned or shaded area. c. Give her several glasses of ice water. d. Cover her with a wet towel. ANS: B The goal for treatment of heat exhaustion is to cool the body initially and slowly in an air-conditioned or shaded area. After the patient is moved, applying wet towels and giving cool drinks are appropriate. DIF: Cognitive Level: Application REF: p. 1253 OBJ: 4 TOP: Heat Exhaustion KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 17. A patient comes to the emergency department with an evisceration after a knife attack. What is the best nursing intervention related to the exposed bowel? a. Gently replace the bowel into the abdominal cavity. b. Place a sterile wrapped sandbag on the abdomen to prevent further evisceration. c. Place the patient in a high Fowler position to allow the bowel to drop back into the abdominal cavity. d. Cover the bowel with a moist saline dressing. ANS: D The nurse protects the tissue from further injury and drying out by the application of a sterile saline dressing. DIF: Cognitive Level: Application REF: p. 1251 OBJ: 4 TOP: Abdominal Injury KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 18. A patient visits the industrial nurse after an accident on the factory floor, which has amputated three toes. What is the most effective nursing intervention for the amputated toes? a. Rinsing with normal saline and placing on a sterile towel b. Placing toes as they are on ice in a sterile container c. Placing the unwrapped toes in a saline bath d. Placing the saline-wrapped toes in a plastic bag in a saline bath ANS: D The toes should be wrapped in a saline dressing and placed in an airtight bag in a cool saline bath. The toes should not be in direct contact with ice or be placed in the freezer. DIF: Cognitive Level: Application REF: p. 1251 OBJ: 4 TOP: Hypothermia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 19. Six hours after a beach picnic on a hot afternoon, a young man enters the emergency department with nausea and vomiting, headache, and diarrhea. On interview, the patient says that he ate potato salad and tuna fish sandwiches. What should the nurse suspect is the causative organism for these symptoms? a. Clostridium botulinum b. Clostridium perfringens c. Salmonella d. Staphylococcus aureus ANS: D Staphylococcus aureus incubates in undercooked foods, especially eggs and mayonnaise, and can cause gastrointestinal symptoms in as little as 6 hours after ingesting the food. DIF: Cognitive Level: Comprehension REF: p. 1255 OBJ: 4 TOP: Food Poisoning KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 20. A child is brought to the emergency department with several deep dog bites on her legs. After cleaning the wounds, what should the nurse be primarily concerned with ascertaining? a. The whereabouts of the dog b. The status of tetanus inoculation c. The rabies status of the animal d. The child’s allergy to the rabies vaccine ANS: B Tetanus prophylaxis should be confirmed so that it can be brought up to date, if necessary. The whereabouts of the dog will be the responsibility of the proper authorities, who will also observe it for rabies. Inoculation for rabies is not an immediate concern unless the bites were on the head or face and can be delayed until the dog is found to be rabid or not. DIF: Cognitive Level: Application REF: p. 1257 OBJ: 4 TOP: Dog Bite KEY: Nursing Process Step: Planning MSC: NCLEX: Health Promotion and Maintenance: Prevention and Early Detection of Disease 21. A patient is brought to the emergency department having had a rock chip embedded in the right eye. What should be the nurse’s initial action? a. Turn the patient to the left side and prepare to remove the chip. b. Flush the right eye with normal saline. c. Keep the patient flat. d. Cover both eyes. ANS: D Stabilizing the rock chip is essential to prevent further damage; it should not be removed. Flushing the eye is done for chemical burns. Patient should not be kept flat. Covering both eyes is recommended to prevent eye movement, which could cause further damage. DIF: Cognitive Level: Application REF: p. 1250 OBJ: 4 TOP: Eye Wound KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 22. A hospital visitor cuts herself on the arm and is bleeding profusely. What should be the immediate treatment by the nurse? a. Call any physician and immediately send the visitor to the emergency department. b. Apply direct pressure to the arm with sterile dressing. c. Take the visitor’s blood pressure and pulse. d. Immobilize the injured arm and send the visitor immediately to the emergency department. ANS: B The first actions should be to stop the blood flow, protect the wound from infection, and call for more help or assist the visitor to the emergency department. DIF: Cognitive Level: Application REF: p. 1247 OBJ: 2 | 4 TOP: Bleeding KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 23. A young man is staggering out of a partially closed doorway to a garage, where a car is running inside. He speaks slowly in a very low voice, telling the nurse that he fell asleep in the car with the engine running. What is the immediate action? a. Ask the person to lie flat right where he is; begin rescue breathing. If the nurse sees anyone else, the nurse should ask the individual to call someone who knows CPR. b. Lead the patient away from the garage and call for help. Stay with the patient and continually assess level of consciousness and respirations. c. Have the patient lie flat. Keep the patient still and call for help. d. Have the patient breathe deeply and continually into a brown paper bag. Assess pulse, respirations, and color of conjunctiva. Check the patient’s pockets for a cellphone to call 9-1-1. ANS: B The man is still conscious enough to speak, but slowly, and therefore does not yet need CPR. Fumes from the garage are entering the air around them. Therefore, getting the nurse and the man away from the fumes is necessary. The man may, at any time, lose consciousness. Sitting down would prevent a fall; consequently, the nurse should call for help. Staying with the young man reassures him and lessens his anxiety response. DIF: Cognitive Level: Application REF: p. 1254 OBJ: 4 TOP: Carbon Monoxide Poisoning KEY: Nursing Process Step: Implementation MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 24. What should the emergency department nurse anticipate on the initial assessment of a patient with carbon monoxide poisoning? a. Blood pressure will be low. b. Oxygen saturation will be low. c. Mucous membranes will be blue. d. Respirations will be less than 10 breaths/min. ANS: B Carbon monoxide binds to the hemoglobin more readily than oxygen, which causes hypoxemia. The mucous membranes will be cherry red, and the blood pressure will be elevated because of hypoxia. DIF: Cognitive Level: Comprehension REF: p. 1254 OBJ: 4 TOP: Carbon Monoxide Poisoning KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort COMPLETION 1. A nurse in the emergency department knows that tissue damage has probably occurred in a person with hypothermia when a rectal temperature of F is assessed. (Use numeric characters only.) ANS: 95 When a patient has a rectal temperature of 95 F, tissue damage from hypothermia has probably occurred. DIF: Cognitive Level: Comprehension REF: p. 1253 OBJ: 4 TOP: Hypothermia KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort 2. A nurse has assessed the patient with a left-sided head injury and records this information: decreasing level of consciousness; slow pupillary response on the right side; blood pressure, 167/80 mm Hg; previous blood pressure, 160/72 mm Hg; and gradually decreasing respiratory and pulse rates. The nurse is aware that these assessments are indicators of increased _ . (Use the full name, not the acronym.) ANS: intracranial pressure All of the listed assessments indicate increased intracranial pressure. DIF: Cognitive Level: Analysis REF: p. 1248 OBJ: 4 TOP: Increasing Intracranial Pressure KEY: Nursing Process Step: Assessment MSC: NCLEX: Physiological Integrity: Basic Care and Comfort [Show More]
Last updated: 1 year ago
Preview 1 out of 480 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Apr 24, 2021
Number of pages
480
Written in

Additional information
This document has been written for:
Uploaded
Apr 24, 2021
Downloads
0
Views
64
.png)
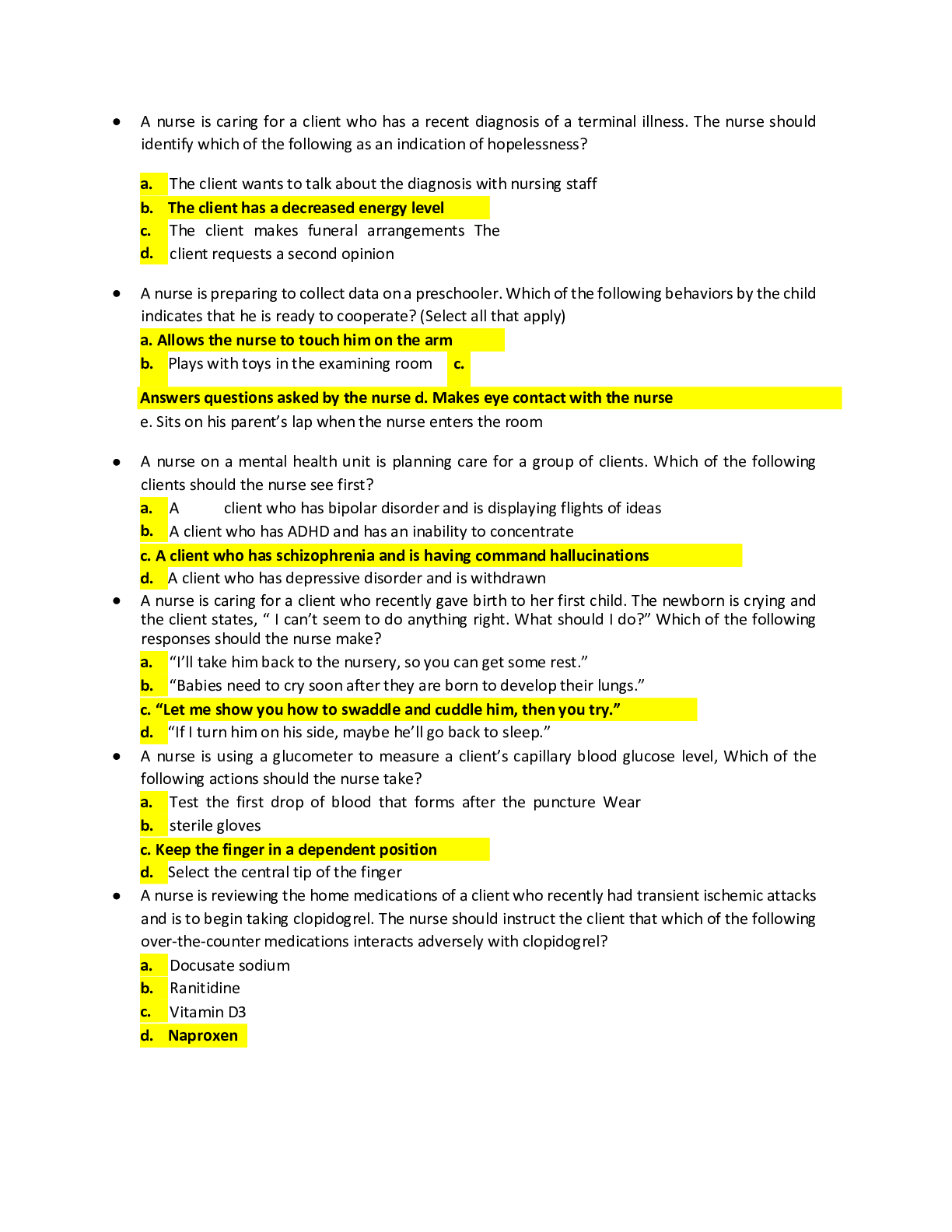
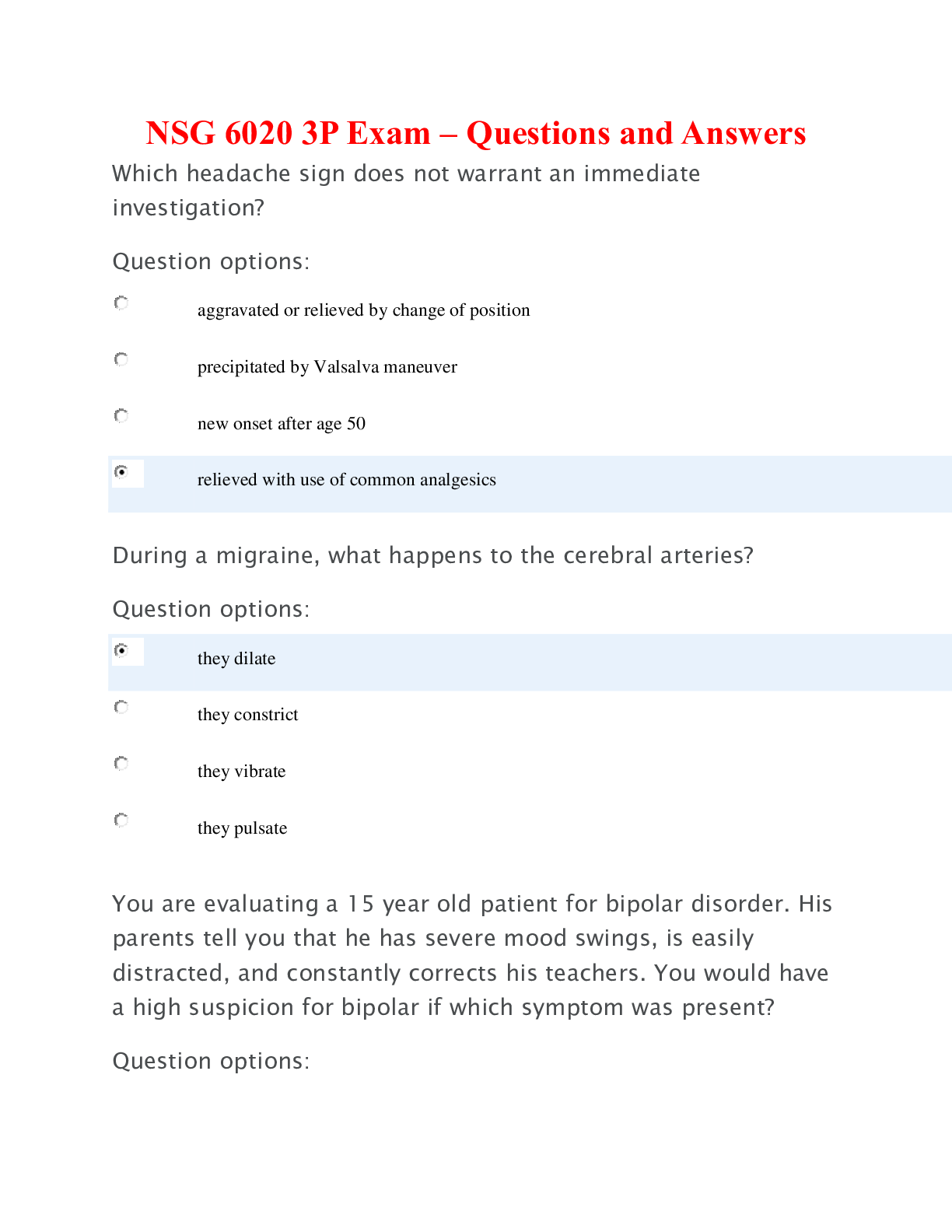
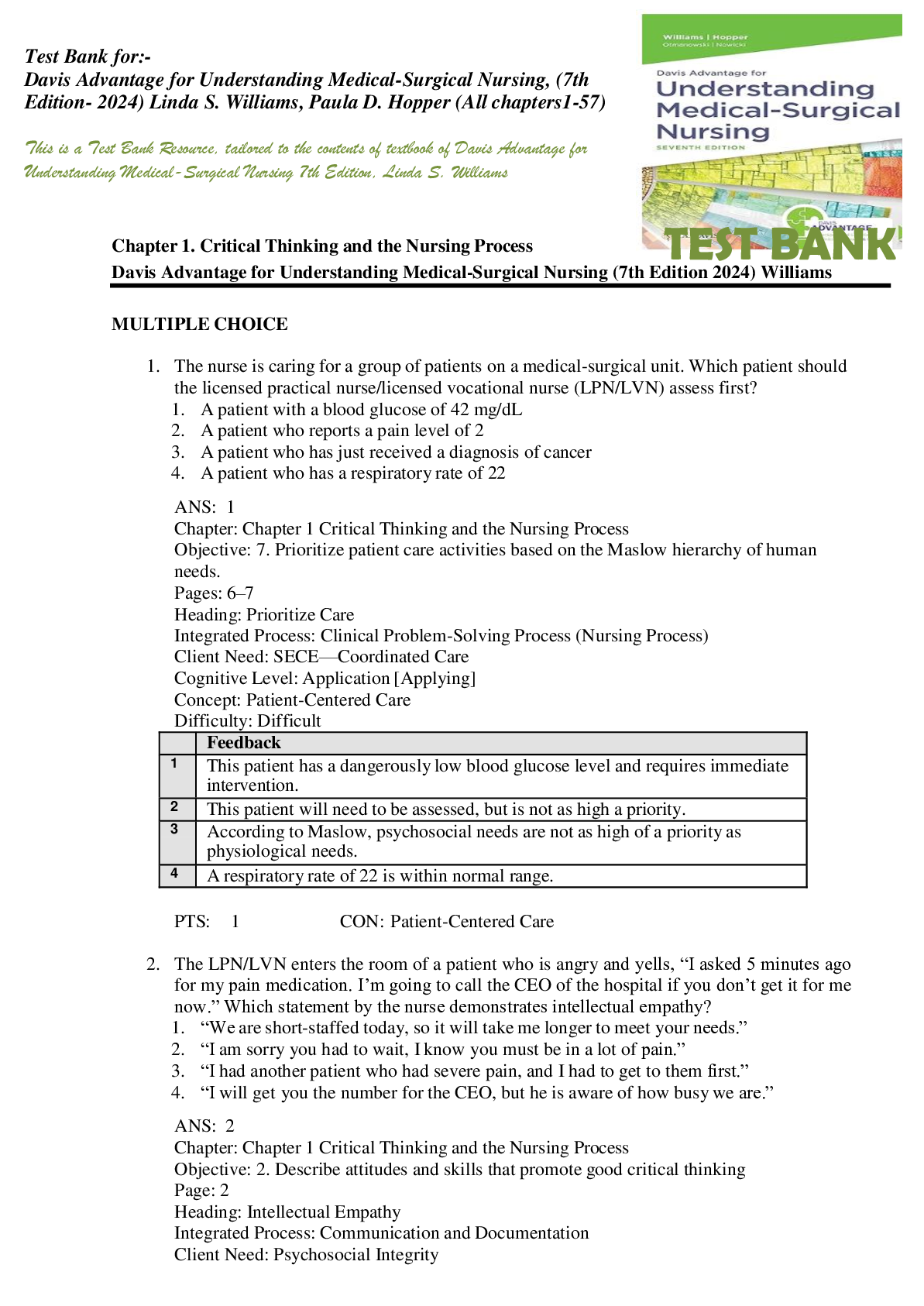




 (1).png)
