*NURSING > CASE STUDY > OB CLINICAL 316 - Swift River OB day 1 (All)
OB CLINICAL 316 - Swift River OB day 1
Document Content and Description Below
Swift River OB day 1 Chastidy Haswell A G1P0 at 40 weeks gestational age presents to OB Triage with complaints of a constant leakage of small amounts of clear fluid vaginally for the last 3 ho... urs. She denies any foul odor to the fluid and denies any sensation of contractions. The physician checked her cervix yesterday in the office and found it to be 1-2 cm. dilated and 50% effaced. The position of the fetus had been at a -3 station. Vickie Dunn A G1P0 presents at 35 weeks pregnant with complaints of decreased fetal movements and severe upper right quadrant pain that has persisted for 24 hours. She denies bloody show, uterine contractions or tightening of any kind. She has a “migraine headache and seeing spots” that has not been relieved with OTC Tylenol and Ice packs for the last 8 hours. She states she weighs 5 pounds more in the office than last week and has had “a lot more swelling” than before. Her BP in the office is 160/98; pulse 90, and 2+ protein was shown in her urine. She states she feels ill and tired but is not sure exactly what is causing her to feel this way, as she has been resting for the last 2 days. Linda Hunter A G1P0 at 41 1/7 weeks gestational age presents to the OB triage desk with complaints of active labor that has lasted for the last 20 hours. Her doctor has sent her over from the office and when checking the cervix noted that the patient had an intact bulging bag of amniotic membrane and a cervical exam of 3-4 cm. dilation and 80% effacement. The patient states active fetal movements and FHR of 120’s in the doctor’s office. This report was confirmed by the physician over the phone. Phyliss Deisenroth A G5P4 presents to OB triage at 32 weeks gestational age with complaints of leakage of a moderate amount of clear fluid vaginally that “soaked her jeans” She states her last baby was born at 33 weeks gestational age. She states a discomfort when her abdomen “tightens up” and states her contractions/tightening are regular every 3-4 minutes. She has a history of rapid labors. She is crying and upset and states that she felt some loose stools and cramping last night but thought it was just “the spicy food” that she had eaten. When she awoke this morning, she reported the cramping had remained the same, but now the loose stools and regular tightening of her abdomen began. She states she currently feels active fetal movements. Sally Johnson A G1P0 patient at 35 weeks gestational age patient presents to the Maternity unit from her Obstetrician’s office with complaints of a lack of sensation of fetal movement for an 8-hour period while at home. Fetal heart rate was 120’s by Doppler assessment. She has had little to drink and has been shopping most of the day. She denies having any symptoms of contractions. Kate Nelson A G4P2 presents to OB triage with gestational age of 39 weeks with complaints of warm, green fluid leaking for the last 1 hour “a little at a time” from her vagina, appearing on her sanitary pad. She states that the fluid has a greenish color but denies foul odor. She has been feeling uterine contractions coming irregularly every 5 min for the last 5-6 hours and over the last hour they have become much more uncomfortable. She states that the infant is moving “as he usually does Jordan Wright A G1PO at 38 weeks presents to the Emergency department with no history of prenatal care other than an ultrasound in the first trimester that confirmed gestational age. The patient has admitted to a history of cocaine abuse and states that she had her last incident of use approximately 1 hour ago. The pt. complains of sudden stabbing pain to the abdomen 30 min after snorting cocaine, and continues to complain of bright red vaginal bleeding of large amount persistently for the last 30 min, Bright red bleeding is currently pooling on the water- resistant pad on the stretcher. She is crying out in intense pain as report from the ER nurse is received. The fetal monitor strip taken in the ER indicates a sudden drop in the fetal heart rate of 40-50 beats per minute as a baseline with minimal variability. Uterine resting tone is absent, and the abdomen is hard and board-like Ann Freeman A G1PO at 40 weeks with diagnosed Fetal Macrosomia has been pushing for over 2 ½ hours in labor and delivery. The station persists at a +2 for the last 3 hours and there is a large caput succedaneum on the presenting part of the fetus. Hydramnios was noted with the spontaneous rupture of membranes earlier and large amounts of fluid have persisted to leak out vaginally. The fetus has a heart rate of 120’s with deep variable decelerations to the 40’s lasting 60-80 seconds only during the contractions and then recovers to 120’s by the end of the contraction. The variability is minimal and there are no accelerations of the heart rate present between the contractions. Joey Kelly A G1P0 was admitted to the high-risk antepartum unit due to signs and symptoms of Preeclampsia yesterday. She has received Magnesium Sulfate IV and her blood pressure and reflexes have decreased. She is 41 weeks gestational age and an ultrasound has shown that the infant has intrauterine growth restriction. A nonstress test was done and the fetus is reactive, and movements are regular. Jennifer Holly A G3P2 at 42 2/7 weeks gestational age presents to labor and delivery from her obstetrician’s office. She has had no signs of labor. She has not been sleeping well and states she “is exhausted”. She has noticed a decrease in fetal movements over the last 24 hours and she was concerned. Monitoring in the office resulted in a non-reactive nonstress test. An ultrasound was done that showed a decrease in amniotic fluid or oligohydramnios. Currently, she denies any signs of labor or vaginal discharge or fluid. occurs in one in every 300 births and presents a great danger to the fetus. It can result in hypoxia or death to the fetus if intervention is not initiated immediately. Stacy Ingalls A G2P1 at 38 weeks gestational age presents to Maternity unit from the Emergency department reporting that she has received no prenatal care in this pregnancy. She has no complaints of labor, or leakage of fluid, but feels she needs to “make sure the baby is okay” and states no fetal movements in a 2-day period. She states she is having “painless tightening of her uterus” irregularly but denies any bloody show or leakage of fluid vaginally. It is evident that a needs to be carried out immediately. Odelinda Baker A G1P0, 16-week gestational age patient presents to her certified nurse midwife’s (CNM) office with no complaints except “pink vaginal mucous”. The CNM examines her cervix and finds the cervix to be 4 cm dilated and 50% effaced with a bulging bag of membranes. The CNM is transferring the patient to the hospital for immediate treatment. Peg Smith A G2P3 at 38 weeks gestational age presents to the emergency department with a diagnosis of Placenta Previa. She is complaining of a large amount of bright red bleeding and she continues to actively bleed on the waterproof pad on the mattress. She has active, painful, regular contractions every 2-5 minutes for the last hour. The fetal heart rate is present at 120 beats per minute and variability is minimal and accelerations are absent. Michelle Davis A G1P0 at 30 weeks gestational age carrying a multifetal pregnancy has had a spontaneous rupture of membranes (SROM) when getting out of the elevator at the hospital and presents to the OB Triage with complaints that “something strange feels like it’s coming out.” The nurse can see when placing the woman in a stretcher that the umbilical cord has prolapsed out of the vagina. Rosie Holloway A G1P0 at 38 weeks is transferred to the Antepartum holding/testing area from her doctor’s office for monitoring and evaluation. In the office her cervix was 2-3 cm and 50% effaced. Earlier in the day, on admission, she had complained of irregular contractions and a persistent headache for the last 24 hours and decreased fetal movements as well as complaints of heart burn that had not been relieved with the OTC Tums. Blood pressures are 160-180/90-100. After 2 hours on the monitor the uterine activity monitor shows regular uterine contractions every 2-5 minutes apart, with the patient complaining of pain with a 7 out of 10 pain scale. The fetal heart rate of 130 has minimal to moderate variability and an absence of accelerations. Non-reassuring decelerations are currently ABSENT. Many of the patient’s blood tests are pending; however, the labs that have been received are showing a low platelet count, elevated (ALT, AST) liver enzymes. Urine test is 2+ for protein. The patient’s cervix is examined again and is now 3-4 cm dilated and 80%. HELLP Syndrome and Admit to Labor and Delivery Unit The breaking/leaking of what a patient refers to as their "bag of water" before natural labor has taken place at term (37-41 weeks gestation). Premature Rupture of Membrane (PROM) A maternal condition defined by the progressive dilation and effacement of the cervix that begins after 20 weeks and before term (the 37th week of pregnancy). This condition occurs because risk factors that are known or unknown cause uterine contractions and the cervix to dilate and efface prior to the time that the fetus is considered Term or 37-41 weeks. Many known and unknown causes for the condition exist. This condition is the leading cause of morbidity and mortality of newborns. Premature Labor An inpatient procedure whereby preexisting labor is assisted in its progress in strength and frequency of uterine contractions and/or dilation and effacement in the cervix by Artificial Rupture of the Amniotic Membranes (AROM), and/or cervical ripening agents and/or IV oxytocin. Augmentation of Labor A G2P1 at 38 weeks gestational age presents to the ER at 1:00 AM with complaints of decreased fetal movements over the last 3-4-hour period. She states that after emptying her bladder and returning to bed she noticed a small gush of vaginal fluid leaking down her leg. She states that the fluid was clear and colorless and denied foul odor. She states that the irregular tightening she usually feels every evening were absent tonight, and she currently feels no discomfort at all in her uterus. Premature Rupture of Membrane (PROM) and Admit to Antepartum testing/holding center as an outpatient Kathy Mann A G1P0 patient at 40 weeks gestational age has been contracting at home for 12 hours. In the last hour, the contractions have slowly decreased in intensity and are irregular in frequency. She reports that she had a spontaneous rupture of the amniotic membrane that occurred an hour ago and the color of the fluid was clear and was of a moderate amount and there was no foul odor. Her cervical exam was done in the doctor's office 2 hours ago and she was found to be 2 cm dilated and 80% effaced (she was 1 cm and 50% at her last prenatal visit a week ago). Augmentation of Labor and Admit to Labor and Delivery Unit Joann Rice A G2P1 at 38 weeks has been in the OB Antepartum testing area for the last 2 hours. Her Nonstress test was reactive and she has no contractions or abnormal discharge or fluid of any kind vaginally. Her blood glucose Accu- Check was within normal limits after lunch. Her fetus is active, and she has no complaints of any discomfort. She has a diagnosis regarding her glucose intolerance in pregnancy and is following an ADA diet and exercising regularly. She is currently having irregular Braxton-Hicks contractions and her cervix is <1 cm and 50% effaced. Gestational Diabetes Mellitus (GDM) Patricia Moore A G4P0 at 24 weeks presents to OB triage with complaints of lower back pain that comes “in waves from my low back wrapping around to just under my ribs” for the last 8 hours. She is afraid she may have a “yeast infection” because she noticed an increase in her vaginal discharge, but denies any vaginal burning, discomfort, itching or foul odor to the discharge. She admits that she has had “no prenatal care so far” and was told by her friend that the vaginal pinkish spotting she noticed about an hour ago isn’t normal. She has felt the baby moving today but noticed that her stool was looser than it has been in the past, her stomach is cramping, and she feared she may have gotten some food poisoning. Premature Labor and Admit to High Risk Antepartum Unit Chantel Foster A G4P2 at 38 weeks gestational age presents to the emergency department with active labor and a moderate amount of greenish fluid is noted leaking from the vaginal opening when her cervix is examined by the ER doctor and found to be at 5-6 cm. dilated and 80% effaced. Testing confirms that it is amniotic fluid. There is no foul odor to the fluid and the patient is afebrile. She is having regular 60-90 second contractions every 5 minutes and her pain is an 8 out of 10 at the peak of each contraction. The Fetal heart rate is 130 with moderate variability with few accelerations. Meconium Staining and Admit to Labor and Delivery Unit Ikesha Taylor A G2P1 at 36 weeks gestational age has been diagnosed with Gestational Diabetes at 26 weeks gestation. Her weekly antepartum surveillance exam is due. She presents to the maternity unit with no complaints of contractions or signs of labor. Nonstress Test and Admit to Antepartum testing/holding center as an outpatient Kristy Turner A G3P2 is presenting to the Maternity unit with complaints of “falling in her bathroom and hitting her abdomen on the bathtub.” She is 38 weeks and complains of persisting contractions that “don’t let up” and active fetal movements. She is having small amounts of bright red spotting for the last hour. Abruptio Placentae and Admit to High Risk Antepartum Unit Rita Ray A G1P0, 32-week gestational age patient presents to the ER with complaints of premature contractions for the last 6 hours. The patient had a cerclage placed at 16 weeks. Incompetent Cervix and Admit to High Risk Antepartum Unit Taryn Jones A G1P0 at 32 weeks presents to her obstetrician’s office with complaints of sudden increase in weight and generalized edema. She has 3+ pitting edema in her legs, 2+ deep tendon reflexes bilaterally and complains of “persisting indigestion” or epigastric pain. She has noticed that Tylenol taken every 4 hours has done little to relieve her headache over the last 24 hours. Her BP is 180/96, pulse 88, respiratory rate is 18/min, and oral temperature is 97.9 F. A urine specimen was taken in the office and showed 2+ protein. Preeclampsia Admit to High Risk Antepartum Unit A complication that occurs prior to, or during, delivery of the baby. This condition occurs when the “pulsing life-line” which connects the placenta to the fetus drops through the open cervix into the vagina ahead of the baby becoming trapped and totally or partially occluded against the baby’s body during delivery. This complication occurs in one in every 300 births and presents a great danger to the fetus. It can result in hypoxia or death to the fetus if intervention is not initiated immediately. Umbilical Cord Prolapse Sue Brown A G2P1 presents to the Emergency department with no previous history of prenatal care. She is having some spotting and uncomfortable contractions. She is unsure of her due date, but her gravid abdominal measurement is at 28 cm. She states that she thinks she has been pregnant for “about 7 months”. Placenta Previa and Admit to High Risk Antepartum Unit Carol Tanner A G2P1 patient at 38 weeks gestation presents to the Emergency Department with a persisting headache lasting >24hrs and "blurry vision". She states she feels very tired and "puffy" and noticed her feet and fingers are more swollen than the day before. Her face, hands, feet and legs are edematous. Her reflexes are brisk, bilaterally, and her blood pressure is 160/95 on the right arm and 158/98 on the left arm. She states that her baby has been actively kicking and moving regularly in the last hour and the monitor strip shows a Fetal Heart Rate baseline from 142-144 with moderate variability. She states she came to the Emergency department because she feels ill and complains of a persisting pain in the upper right quadrant of her abdomen. She continues to deny any sensation of uterine contractions or discomfort otherwise. Her uterus is soft, and she denies any complaints of "bloody show", abnormal discharge, or leakage of amniotic fluid vaginally. She has no fever, and denies vomiting, nausea or diarrhea. HELLP Syndrome and Admit to High Risk Antepartum Unit Karen Scott A G1P0 is admitted to the Antepartum holding area as an outpatient to be monitored for complaints of regular moderately uncomfortable uterine contractions lasting 60-80 seconds occurring every 2-5 minutes. Her cervix was examined for dilation and effacement and found to be 2-3 centimeters and 100% effaced. The patient complains of a “sudden large gush” of warm amniotic fluid between her legs following the vaginal exam. When the nurse is cleaning up the fluid on the bed and changing the waterproof pad a protrusion is visualized coming out of the patient’s vagina. The fetal heart rate has dropped suddenly to 40 beats per minute. The nurse quickly repositions the patient, does a vaginal examination and pushes the fetal presenting part away from the protrusion. Umbilical Cord Prolapse and Prepare for Surgical Intervention or Cesarean Section Precious Vines A G3P2 at 38 weeks with a diagnosis of intrauterine growth restriction has been sent over from her OB doctor’s office with orders for a biophysical profile. The patient denies any signs of labor currently. Contraction Stress Test (CST) and Admit to Antepartum testing/holding center as an outpatient Tina White A G2P0 16-week gestational age patient arrives in the antepartum triage with complaints of premature painless contractions coming in an irregular pattern for the last 12 hours. The nurse receives orders from her physician to check the patient’s cervix. The nurse finds that the cervix is dilated to 3-4 cm with a bulging bag of membranes. Incompetent Cervix and Prepare for Surgical Intervention or Cesarean Section Kathy Williams A G2P1 40-week gestational age has been in labor and delivery for more than 8 hours for induction of labor. The patient is receiving IV Pitocin to increase the strength and frequency of the contractions. She is 5-6 cm. dilated. Spontaneous rupture of membranes occurs as the nurse is checking for vaginal dilation. The nurse notices that the fetal heart rate abruptly decelerates in a “V” shaped pattern to 30-40 beats per minute. The nurse repeats the vaginal exam to assess for the cause of the deceleration and palpates a “pulsing protrusion” in the vaginal area. The nurse pushes the fetal head away from the cervix and the “pulsing protrusion” and elevates the mother’s hips and calls for additional medical help so that other immediate interventions can take place. Umbilical Cord Prolapse and Prepare for Surgical Intervention or Cesarean Section [Show More]
Last updated: 1 year ago
Preview 1 out of 8 pages

Reviews( 0 )
Recommended For You
*NURSING> CASE STUDY > OB CLINICAL 316 - Swift River OB day (All)
OB CLINICAL 316 - Swift River OB day
Swift River OB day 1 Chastidy Haswell A G1P0 at 40 weeks gestational age presents to OB Triage with complaints of a constant leakage of small amounts of clear fluid vaginally for the last 3 ho urs. Sh...
By A-PLUS GUIDENOTES , Uploaded: Aug 18, 2021
$10
*NURSING> CASE STUDY > OB CLINICAL 316 - Swift River OB day (All)
OB CLINICAL 316 - Swift River OB day
Swift River OB day 1 Chastidy Haswell A G1P0 at 40 weeks gestational age presents to OB Triage with complaints of a constant leakage of small amounts of clear fluid vaginally for the last 3 ho urs. Sh...
By STUDY-GUIDENOTES , Uploaded: Aug 18, 2021
$10
*NURSING> CASE STUDY > SWIFT RIVER OB DAY 1 OB CLINICAL 316 (All)
SWIFT RIVER OB DAY 1 OB CLINICAL 316
The breaking/leaking of what a patient refers to as their "bag of water" before natural labor has taken place at term (37-41 weeks gestation)." Premature Rupture of Membrane (PROM) Chastidy Haswell...
By destinyd , Uploaded: Jun 29, 2021
$10.5
*NURSING> CASE STUDY > Swift River OB day 1 OB CLINICAL 316 (All)
Swift River OB day 1 OB CLINICAL 316
Swift River OB day 1 Chastidy Haswell A G1P0 at 40 weeks gestational age presents to OB Triage with complaints of a constant leakage of small amounts of clear fluid vaginally for the last 3 hours. She...
By Grademaster , Uploaded: Nov 26, 2020
$10
*NURSING> CASE STUDY > Swift River OB day 1 OB CLINICAL 316 (All)
Swift River OB day 1 OB CLINICAL 316
Swift River OB day 1 Chastidy Haswell A G1P0 at 40 weeks gestational age presents to OB Triage with complaints of a constant leakage of small amounts of clear fluid vaginally for the last 3 hours....
By Good grade , Uploaded: Sep 06, 2020
$14
Health Care> CASE STUDY > NURS 316 / OB CLINICAL 316 - SWIFT RIVER OB (All)

NURS 316 / OB CLINICAL 316 - SWIFT RIVER OB
NURS 316 / OB CLINICAL 316 - SWIFT RIVER OB
By Mariebelle , Uploaded: Sep 21, 2022
$12
Business Law> CASE STUDY > COLLECTRO HUMAN RESOURCES ANALYSIS (All)
COLLECTRO HUMAN RESOURCES ANALYSIS
This assignment is designed to assess learning outcomes: 1. Critically evaluate the key issues involved in managing and developing people across cultural boundaries in the context of globalization,...
By Augustine , Uploaded: Oct 28, 2020
$10
Financial Accounting> CASE STUDY > SUSTAINABILITY ACCOUNTING AT OFFICEWORKS (All)
SUSTAINABILITY ACCOUNTING AT OFFICEWORKS
The Chief Executive Officer (CEO) of Officeworks has noticed an emerging and increasing trend of discussion about sustainability from businesses and some of Officeworks’s competitors are adopting va...
By Augustine , Uploaded: Oct 29, 2020
$10
Business> CASE STUDY > Analytics Mindset TechWear CASE ANALYSIS (All)
Analytics Mindset TechWear CASE ANALYSIS
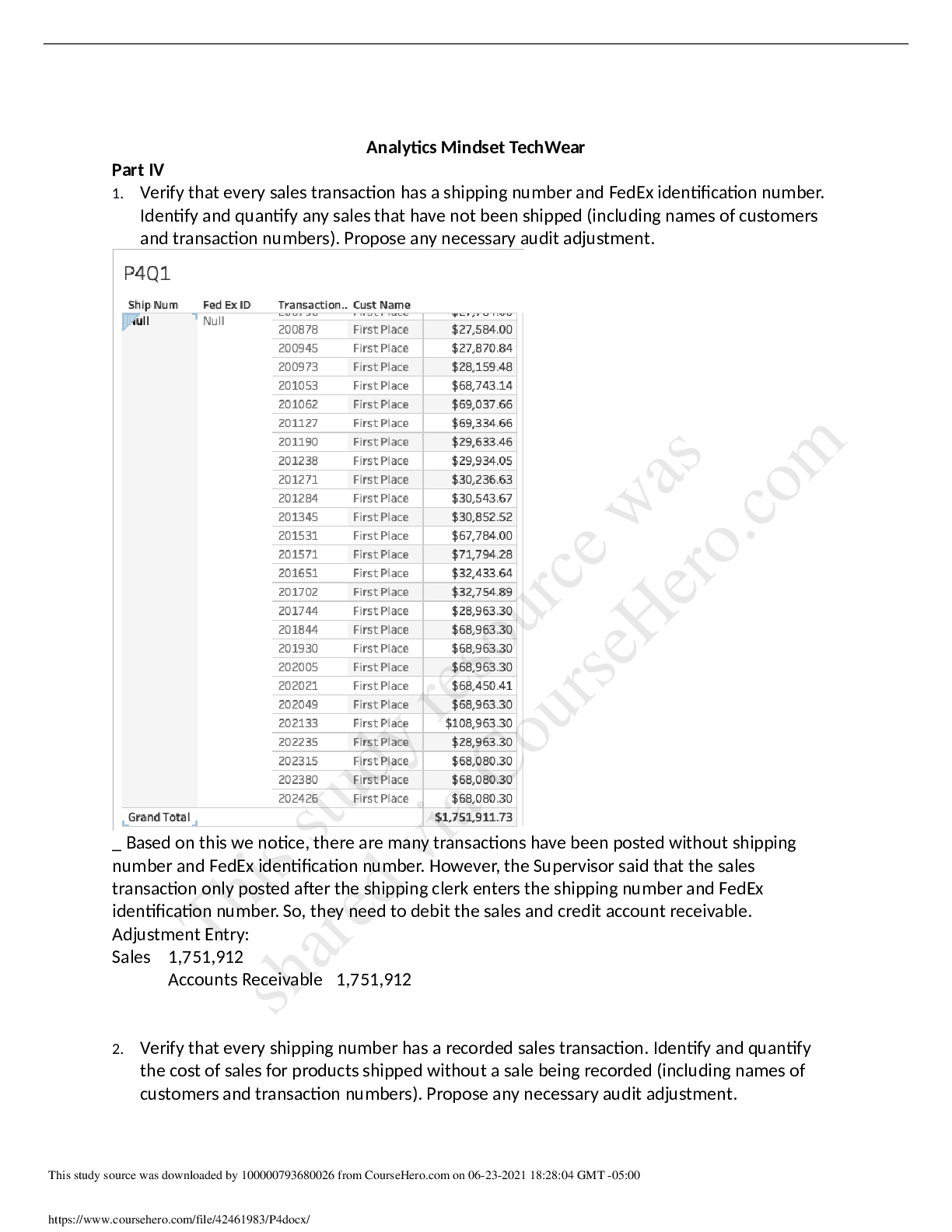
Analytics Mindset TechWear Part IV 1. Verify that every sales transaction has a shipping number and FedEx identification number. Identify and quantify any sales that have not been shipped (includin...
By Cheryshev , Uploaded: Jun 24, 2021
$9.5
*NURSING> CASE STUDY > Sara Daniels Hyperbilirubinemia Unfolding Reasoning_Case Study (All)

Sara Daniels Hyperbilirubinemia Unfolding Reasoning_Case Study
Hyperbilirubinemia UNFOLDING Reasoning Sarah Daniels, newborn infant Primary Concept Elimination Interrelated Concepts (In order of emphasis) • Clinical Judgment • Patient Education • Communic...
By Martin Freeman , Uploaded: Feb 28, 2021
$6
Document information
Connected school, study & course
About the document
Uploaded On
Nov 26, 2020
Number of pages
8
Written in

Additional information
This document has been written for:
Uploaded
Nov 26, 2020
Downloads
5
Views
3555