*NURSING > STUDY GUIDE > NR 566 Test Bank Questions For Weeks 5( Complete Solution Rated A)Top score (All)
NR 566 Test Bank Questions For Weeks 5( Complete Solution Rated A)Top score
Document Content and Description Below
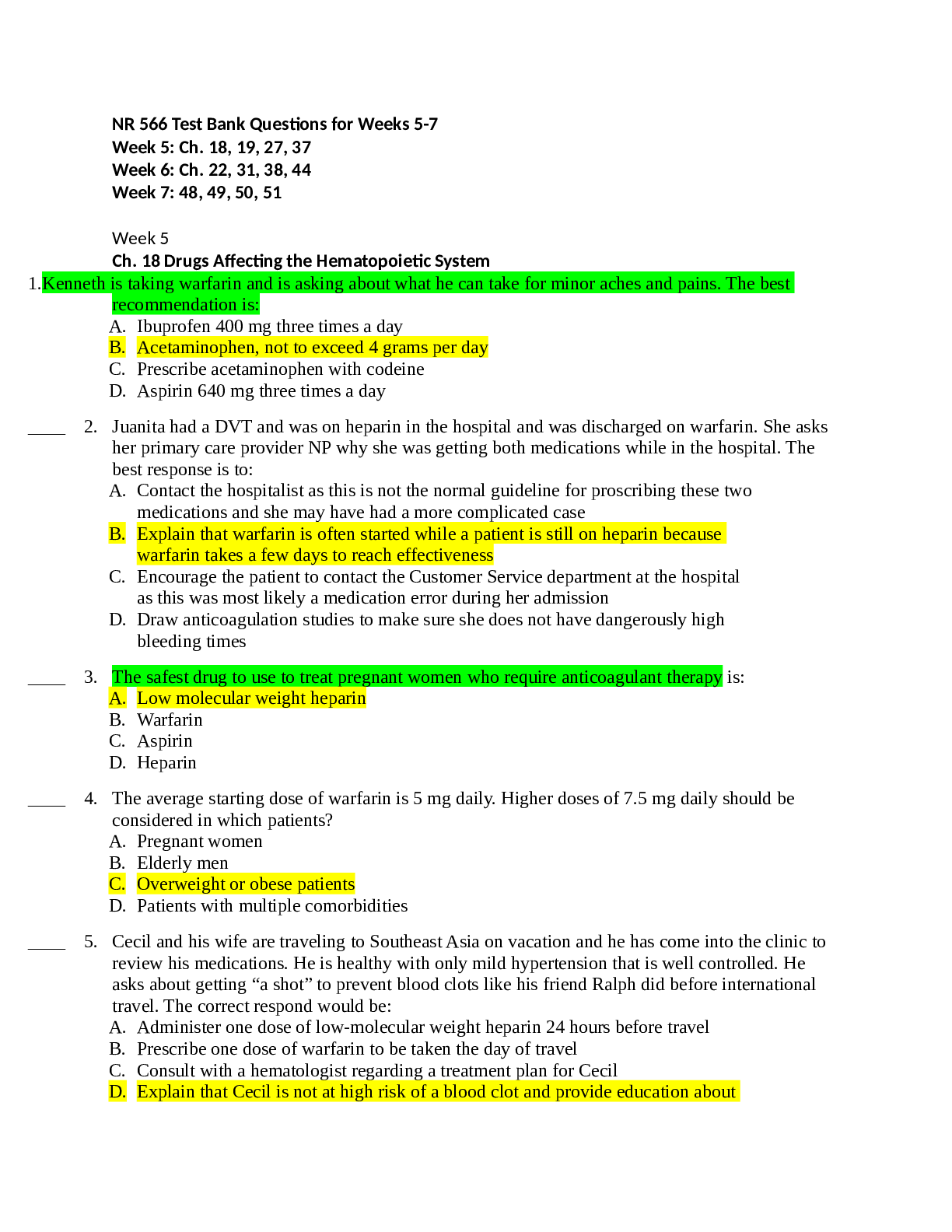
NR 566 Test Bank Questions for Weeks 5-7 Week 5 Ch. 18 Drugs Affecting the Hematopoietic System 1. Kenneth is taking warfarin and is asking about what he can take for minor aches and pains. The b est ... recommendation is: A. Ibuprofen 400 mg three times a day B. Acetaminophen, not to exceed 4 grams per day C. Prescribe acetaminophen with codeine D. Aspirin 640 mg three times a day 2. Juanita had a DVT and was on heparin in the hospital and was discharged on warfarin. She asks her primary care provider NP why she was getting both medications while in the hospital. The best response is to: A. Contact the hospitalist as this is not the normal guideline for proscribing these two medications and she may have had a more complicated case B. Explain that warfarin is often started while a patient is still on heparin because warfarin takes a few days to reach effectiveness C. Encourage the patient to contact the Customer Service department at the hospital as this was most likely a medication error during her admission D. Draw anticoagulation studies to make sure she does not have dangerously high bleeding times 3. The safest drug to use to treat pregnant women who require anticoagulant therapy is: A. Low molecular weight heparin B. Warfarin C. Aspirin D. Heparin 4. The average starting dose of warfarin is 5 mg daily. Higher doses of 7.5 mg daily should be considered in which patients? A. Pregnant women B. Elderly men C. Overweight or obese patients D. Patients with multiple comorbidities 5. Cecil and his wife are traveling to Southeast Asia on vacation and he has come into the clinic to review his medications. He is healthy with only mild hypertension that is well controlled. He asks about getting “a shot” to prevent blood clots like his friend Ralph did before international travel. The correct respond would be: A. Administer one dose of low-molecular weight heparin 24 hours before travel B. Prescribe one dose of warfarin to be taken the day of travel C. Consult with a hematologist regarding a treatment plan for Cecil D. Explain that Cecil is not at high risk of a blood clot and provide education about how to prevent blood clots while traveling 6. Robert, age 51 years, has been told by his primary care provider (PCP) to take an aspirin a day. Why would this be recommended? A. He has arthritis and this will help with the inflammation and pain. B. Aspirin has anti-platelet activity and prevents clots that cause heart attacks. C. Aspirin acidifies the urine and he needs this for prostrate health. D. He has a history of GI bleed, and one aspirin a day is a safe dose. 7. Sally has been prescribed aspirin 320 mg per day for her atrial fibrillation. She also takes aspirin four or more times a day for arthritis pain. What are the symptoms of aspirin toxicity she would need to be evaluated for: A. Tinnitus B. Diarrhea C. Hearing loss D. Photosensitivity 8. Patient education when prescribing clopidogrel includes: A. Do not take any herbal products without discussing with the provider B. Monitor urine output closely and contact the provider if it decreases C. Clopidogrel can be constipating, use a stool softener if needed D. The patient will need regular anticoagulant studies while on clopidogrel 9. For patients taking warfarin INRs are best drawn: A. Monthly throughout therapy B. Three times a week throughout therapy C. Two hours after the last dose of warfarin to get an accurate peak level D. In the morning if the patient takes their warfarin at night 10. Patients receiving heparin therapy require monitoring of: A. Platelets every 2 to 3 days for thrombocytopenia that may occur on Day 4 of therapy B. Electrolytes for elevated potassium levels in the first 24 hours of therapy C. INR throughout therapy to keep in the range around 2.0 D. Blood pressure for hypertension that may occur in the first 2 days of treatment 11. The routine monitoring recommended for low molecular weight heparin is: A. INR every 2 days until stable then weekly B. aPTT every week while on therapy C. Factor Xa levels if patient is pregnant D. White blood cell count every 2 weeks 12. When writing a prescription for warfarin it is common to write on the prescription. A. OK to substitute for generic B. The brand name of warfarin and Do Not Substitute C. PRN refills D. Refills for 1 year 13. Education of patients who are taking warfarin includes discussing their diet. Instructions include: A. Avoiding all vitamin K-containing foods B. Avoiding high vitamin K-containing foods C. Increasing intake of iron-containing foods D. Making sure they eat 35 grams of fiber daily 14. Patients who are being treated with epoetin alfa need to be monitored for the development of: A. Thrombocytopenia B. Neutropenia C. Hypertension D. Gout 15. The FDA issued a safety announcement regarding the use of erythropoiesis-stimulating agents (ESAs) in 2010 with the recommendation that: A. ESAs no longer be prescribed to patients with chronic renal failure B. The risk of tumor development be explained to cancer patients on ESA therapy C. Patients should no longer receive ESA therapy to prepare for allogenic transfusions D. ESAs be prescribed only to patients younger than age 60 years 16. When patients are started on darbepoetin alfa (Aranesp) they need monitoring of their blood counts to determine a dosage adjustment in: A. 6 weeks if they are a cancer patient B. 1 week if they have chronic renal failure C. 2 weeks if taking for allogenic transfusion D. Weekly throughout therapy 17. Jim is having a hip replacement surgery and would like to self-donate blood for the surgery. In addition to being prescribed epogen alpha he should also be prescribed: A. Folic acid to prevent megaloblastic anemia B. Iron, to start when the epogen starts C. An antihypertensive to counter the adverse effects of epogen D. Vitamin B12 to prevent pernicious anemia 18. Monitoring for a patient being prescribed iron for iron deficiency anemia includes: A. Reticulocyte count 1 week after therapy is started B. Complete blood count every 2 weeks throughout therapy C. Hemoglobin level at 1 week of therapy D. INR weekly throughout therapy 19. Patient education regarding taking iron replacements includes: A. Doubling the dose if they miss a dose to maintain therapeutic levels B. Taking the iron with milk or crackers if it upsets their stomach C. Iron is best taken on an empty stomach with juice D. Antacids such as Tums may help the upset stomach caused by iron therapy 20. Patients with pernicious anemia require treatment with: A. Iron B. Folic acid C. Epogen alpha D. Vitamin B12 21. The first lab value indication that Vitamin B12 therapy is adequately treating pernicious anemia is: A. Hematocrit levels start to rise B. Hemoglobin levels return to normal C. Reticulocyte count begins to rise D. Vitamin B12 levels return to normal 22. Patients who are beginning therapy with Vitamin B12 need to be monitored for: A. Hypertensive crisis that may occur in the first 36 hours B. Hypokalemia that occurs in the first 48 hours C. Leukopenia that occurs at 1 to 3 weeks of therapy D. Thrombocytopenia that may occur at any time in therapy 1. Week 5 Chapter 19: Drugs Affecting the Immune System Attenuated vaccines are also known as: A. Killed vaccines B. Booster vaccines C. Inactivated vaccines D. Live vaccines 2. Live attenuated influenza vaccine (FluMist) may be administered to: A. All patients over 6 months of age B. Patients between age 2 years and 49 years with no risk factors C. Patients with a URI or asthma D. Pregnant women 3. The reason that two MMR vaccines at least a month apart are recommended is: A. The second dose of MMR “boosts” the immunity built from the first dose B. Two vaccines 1 month apart is the standard dosing for all live virus vaccines C. If the two MMR vaccine doses are given too close together there is a greater likelihood of severe localized reaction to the vaccine D. Only 95% of patients are fully immunized for measles after the first vaccine, with 99% having immunity after two doses of MMR 4. MMR vaccine is not recommended for pregnant women because: A. Pregnant women do not build adequate immunity to the vaccine B. There is a risk of the pregnant women developing measles encephalopathy C. There is a risk of the fetus developing congenital rubella syndrome D. Pregnant women can receive the MMR vaccine 5. If the MMRV (measles, mumps, rubella, and varicella) combined vaccine is ordered to be given as the first MMR and varicella dose to a child the CDC recommends: A. Parents be informed of the increased risk of fever and febrile seizures over the MMR plus varicella 2 shot regimen B. Patients must also receive MMRV as the second dose of MMR and varicella in order to build adequate immunity C. Patients be premedicated with acetaminophen 15 minutes before the vaccine is given D. Patients should not be around pregnant women for the first 48 hours after the vaccine is given 6. The rotavirus vaccine (RotaTeq, Rotarix): A. Is a live vaccine that replicates in the small intestine, providing active immunity against rotavirus B. Should not be administered to infants who are or may be potentially immunocompromised C. Is not given to an infant who has a febrile illness (temperature greater than 100.5°F) D. All of the above 7. Varicella vaccine is recommended to be given to patients who are: A. HIV positive with a CD4+ T-lymphocyte percentage less than 15 percent B. Taking corticosteroids (up to 2 mg/kg/day or less than 20 mg/day) C. Pregnant D. Immunocompromised 8. Zoster vaccine (Zostavax) is: A. A live varicella zoster vaccine from the same strain used to develop the varicella vaccine B. Effective in preventing varicella zoster in patients of all ages C. Recommended for patients age 40 to 80 who have had chickenpox D. Administered at the same time as other live vaccines, as long as they are given the same day 9. True contraindications to diphtheria, tetanus, and acellular pertussis (DTaP or Tdap) vaccine include: A. Fever up to 104°F (40.5°C) after previous DTaP vaccine B. Family history of seizures after DTaP vaccine C. Adolescent pregnancy D. Anaphylactic reaction with a previous dose 10. Hepatitis B vaccine (HBV) is contraindicated in patients who: A. Were born less than 32 weeks gestation (give first dose at age 6 months) B. Are pregnant C. Are on hemodialysis D. Are allergic to yeast 11. Human papillomavirus (HPV) vaccine (Gardasil, Cervarix): A. Is a live virus vaccine that provides immunity to six strains of HPV virus B. Has a common adverse effect of syncope within 15 minutes of giving the vaccine C. Should not be given to males younger than age 12 years D. May be given to pregnant women 12. Influenza vaccine may be administered annually to: A. Patients with egg allergy B. Pregnant patients C. Patients age 6 weeks or older D. Patients with acute febrile illness 13. Immune globulin serums (IGs): A. Provide active immunity against infectious diseases B. Are contraindicated during pregnancy C. Are heated to above body temperature to kill most hepatitis, HIV, and other viruses such as parvovirus D. Are derived from pooled plasma of adults and contain specific antibodies in proportion to the donor population 14. Hepatitis B immune globulin (HBIG) is administered to provide passive immunity to: A. Infants born to HBsAg-positive mothers B. Household contacts of hepatitis-B virus infected people C. Persons exposed to blood containing hepatitis B virus D. All of the above 15. Rho(D) immune globulin (RhoGAM) is given to: A. Infants born to women who are Rh positive B. Sexual partners of Rh positive women C. Rh negative women after a birth, miscarriage, or abortion D. Rh negative women at 36 weeks gestation 16. Tuberculin purified protein derivative (PPD): A. Is administered to patients who are known tuberculin-positive reactors B. May be administered to patients who are on immunosuppressives C. May be administered 2 to 3 weeks after an MMR or varicella vaccine D. May be administered the same day as the MMR and/or varicella vaccine 17. Diane may benefit from cyclosporine (Sandimmune). Cyclosporin may be prescribed to: A. Treat rheumatoid arthritis B. Treat patients with corn allergy C. Pregnant patients D. Treat patients with liver dysfunction 18. Azathioprine has significant adverse drug effects, including: A. Hypertension B. Hirsutism C. Risk of cancer D. Gingival hyperplasia Week 5 Chapter 27 Anemia Pernicious anemia is treated with: A. Folic acid supplement B. Thiamine supplement C. Vitamin B12 D. Iron 2. Premature infants require iron supplementation with: A. 10 mg/day of iron B. 2 mg/kg per day until age 12 months C. 7 mg/day in diet D. 1 mg/kg per day until adequate intake of iron from foods 3. Breastfed infants should receive iron supplementation of: A. 3 mg/kg per day B. 6 mg/kg per day C. 1 mg/kg per day D. Breastfed babies do not need iron supplementation 4. Valerie presents to clinic with menorrhagia. Her hemoglobin is 10.2 and her ferritin is 15 ng/mL. Initial treatment for her anemia would be: A. 18 mg/day of iron supplementation B. 6 mg/kg per day of iron supplementation C. 325 mg ferrous sulfate per day D. 325 mg ferrous sulfate TID 5. Chee is a 15-month-old male whose screening hemoglobin is 10.4 g/dL. Treatment for his anemia would be: A. 18 mg/day of iron supplementation B. 6 mg/kg per day of elemental iron C. 325 mg ferrous sulfate per day D. 325 mg ferrous sulfate TID 6. Monitoring for a patient taking iron to treat iron deficiency anemia is: A. Hemoglobin, hematocrit, and ferritin 4 weeks after treatment is started B. Complete blood count every 4 weeks throughout treatment C. Annual complete blood count D. Reticulocyte count in 4 weeks 7. Valerie has been prescribed iron to treat her anemia. Education of patients prescribed iron would include: A. Take the iron with milk if it upsets her stomach B. Antacids may help with the nausea and GI upset caused by iron C. Increase fluids and fiber to treat constipation D. Iron is best tolerated if it is taken at the same time as her other medications 8. Allie has just had her pregnancy confirmed and is asking about how to ensure a healthy baby. What is the folic acid requirement during pregnancy? A. 40 mcg/day B. 400 mcg/day C. 800 mcg/day D. 2 gm/day 9. Kyle has Crohn’s disease and has a documented folate deficiency. Drug therapy for folate deficiency anemia is: A. Oral folic acid 1 to 2 mg per day B. Oral folic acid 1 gram per day C. IM folate weekly for at least 6 months D. Oral folic acid 400 mcg daily 10. Patients who are being treated for folate deficiency require monitoring of: A. Complete blood count every 4 weeks B. Hematocrit and hemoglobin at 1 week and then at 8 weeks C. Reticulocyte count at 1 week D. Folate levels every 4 weeks until hemoglobin stabilizes 11. The treatment of vitamin B12 deficiency is: A. 1,000 mcg daily of oral cobalamin B. 2 gm per day of oral cobalamin C. 100 mcg/day Vitamin B12 IM D. 500 mcg/dose nasal cyanocobalamin 2 sprays once a week 12. The dosage of Vitamin B12 to initially treat pernicious anemia is: A. Nasal cyanocobalamin 1 gram spray in each nostril daily x 1 week then weekly x 1 month B. Vitamin B12 IM monthly C. Vitamin B12 1,000 mcg IM daily x 1 week then 1,000 mg weekly for a month D. Oral cobalamin 1,000 mcg daily 13. Before beginning IM Vitamin B12 therapy, which laboratory values should be obtained? A. Reticulocyte count, hemoglobin, and hematocrit B. Iron C. Vitamin B12 D. All of the above 14. should be monitored when Vitamin B12 therapy is started. A. Serum calcium B. Serum potassium C. Ferritin D. C-reactive protein 15. Anemia due to chronic renal failure is treated with: A. Epoetin alfa (Epogen) B. Ferrous sulfate C. Vitamin B12 D. Hydroxyurea Week 5 Chapter 37: HIV The goals of treatment when prescribing antiretroviral medication to patients with HIV include: A. Prevent vertical HIV transmission B. Improve quality of life C. Prolong survival D. All of the above 2. A challenge faced with antiretroviral therapy (ART) is: A. Patients abusing ART B. Drug-resistant mutations of HIV C. Reduction of transmissibility of HIV D. Lack of efficacy data 3. Predictors for successful treatment with antiretroviral therapy (ART) in HIV-positive patients include: A. They respond to low potency treatment regimen B. They have demonstrated resistance in the past and should respond to newer ART drugs C. The patient is strictly adherent to the ART treatment regimen D. Lower baseline CD4 T-cell count at baseline 4. The goal of antiretroviral therapy (ART) in HIV-positive patients is: A. Maximum suppression of HIV replication B. Eradication of HIV virus from the body C. Determining a treatment regimen that is free of adverse effects D. Suppression of CD4 T-cell count 5. Pregnant women who are HIV positive: A. Are treated with AZT alone to prevent birth defects B. Are treated with a combination ART regimen C. Should not be treated with ART due to teratogenicity of the drugs D. Are at high risk of developing resistance to ART drugs 6. Antiretroviral therapy is recommended for HIV-positive patients with: A. A history of AIDS-defining illness B. Pregnant women C. Hepatitis B co-infection D. All of the above 7. If considering starting a patient on the nucleoside reverse transcriptase inhibitor (NRTI) abacavir, the following testing is recommended prior to prescribing: A. Renal function B. HLA B*5701 testing C. Pancreatic enzyme levels D. CYP 450 enzyme activity 8. [Show More]
Last updated: 1 year ago
Preview 1 out of 25 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Mar 16, 2022
Number of pages
25
Written in

Additional information
This document has been written for:
Uploaded
Mar 16, 2022
Downloads
0
Views
72


 (1).png)