*NURSING > EXAM > Rasmussen College :NUR2759 MDC3 Exam 1 Review - With NCLEX questions & extra notes, LATEST UPDATED,1 (All)
Rasmussen College :NUR2759 MDC3 Exam 1 Review - With NCLEX questions & extra notes, LATEST UPDATED,100% CORRECT
Document Content and Description Below
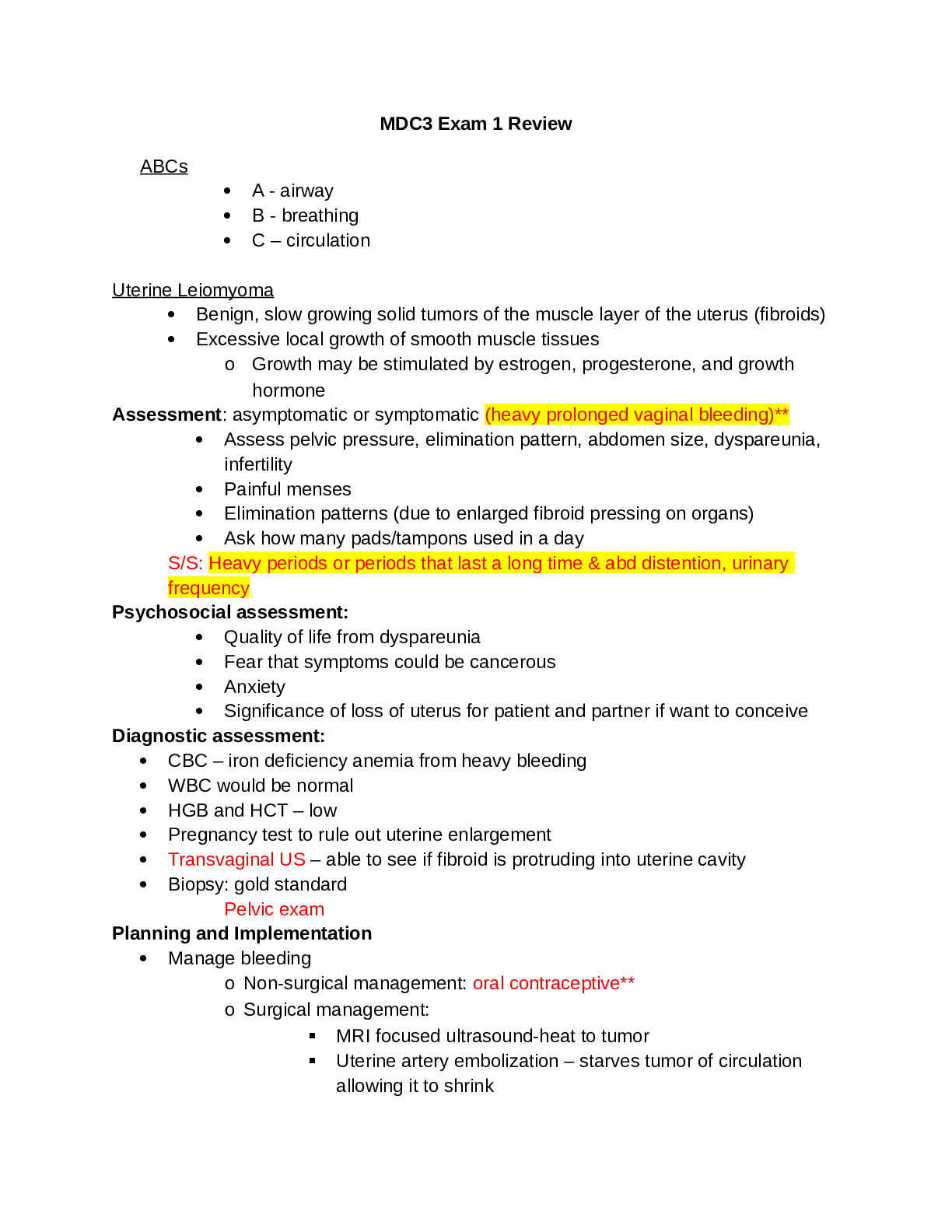
Rasmussen College :NUR2759 MDC3 Exam 1 Review - With NCLEX questions & extra notes, LATEST UPDATED MDC3 Exam 1 Review ABCs • A - airway • B - breathing • C – circulation Uterine Le... iomyoma • Benign, slow growing solid tumors of the muscle layer of the uterus (fibroids) • Excessive local growth of smooth muscle tissues o Growth may be stimulated by estrogen, progesterone, and growth hormone Assessment: asymptomatic or symptomatic (heavy prolonged vaginal bleeding)** • Assess pelvic pressure, elimination pattern, abdomen size, dyspareunia, infertility • Painful menses • Elimination patterns (due to enlarged fibroid pressing on organs) • Ask how many pads/tampons used in a day S/S: Heavy periods or periods that last a long time & abd distention, urinary frequency Psychosocial assessment: • Quality of life from dyspareunia • Fear that symptoms could be cancerous • Anxiety • Significance of loss of uterus for patient and partner if want to conceive Diagnostic assessment: • CBC – iron deficiency anemia from heavy bleeding • WBC would be normal • HGB and HCT – low • Pregnancy test to rule out uterine enlargement • Transvaginal US – able to see if fibroid is protruding into uterine cavity • Biopsy: gold standard Pelvic exam Planning and Implementation • Manage bleeding o Non-surgical management: oral contraceptive** o Surgical management: ▪ MRI focused ultrasound-heat to tumor ▪ Uterine artery embolization – starves tumor of circulation allowing it to shrink ▪ Myomectomy- laser removal ▪ Hysterectomy Erectile Dysfunction: causes & treatment • Common as one ages: reduced blood flow to penis Causes Medical causes: change in blood pressure Non-organic: increased stressor, illnesses Treatment • Medications that increase perfusion to penis (PDE- 5 inhibitors) • Vacuum pump • Pineal implant • Managing stress Education related to treatment for HPV/Cervical Cancer • Caused by HPV s/s of cervical cancer: o heavy bleeding in later stages o bleeding after sex o Most of the time asymptomatic Bleeding between periods Preventive screening: PAP smear, surgical biopsy (gold standard) to determine staging Treatment: • Early- ablation, laser • Late- chemotherapy/radiation Education: • No sticking anything up the vagina (tampons, douches) • May have bleeding • No sexual intercourse • No tub baths Breast cancer- preventative screenings, risk factors, diagnostic tests Preventative screenings • Mammography o Recommended to start screening at 45 o Women over 55 may switch to every 2 years • Breast self-awareness/self-examinations o >90% detected by patient • Clinical breast clinical Risk Factors o At least every 3 years for women in their 20s and 30s and every year for asymptomatic women at least 40 years old • Increased age • Family history • Early menarche, late menopause • Lack of breastfeeding • Postmenopausal obesity • Alcohol consumption • Mutations in BRCA1 or BRCA2 Diagnostic tests • Lab assessment: study of breast mass tissue and lymph nodes, liver enzymes, calcium, and alkaline phosphatase • Imaging assessment: o Mammogram o Ultrasound o MRI o Chest x-ray, CT for metastasis o Breast biopsy* Endometrial cancer- symptoms, risk factors, diagnostic testing • Most common gynecologic malignancy • Cancer of inner uterine lining • Grows slowly but vaginal bleeding usually leads to prompt evaluation and treatment = good prognosis • Most commonly associated with prolonged exposure to estrogen without its protective effects of progesterone Risk Factors: • Women in reproductive years • Family History • Diabetes Mellitus • HTN • Obesity • Uterine polyps • Late menopause • Nulliparity (no childbirths) • Smoking • Tamoxifen – given for breast cancer Symptoms: • Postmenopausal bleeding (how many pads/tampons a day)** • Watery, bloody vaginal discharge • Low back or abdominal pain • Low pelvic impaired comfort (describe exact location and intensity) • Pelvic exam may reveal palpable uterine mass** Diagnostic testing: o Transvaginal ultrasound* o Endometrial biopsy – gold standard “determine presence of endometrial thickening/cancer”** • Interventions o Pelvic exam Hysterectomies- what they are, who gets them, post-operative care, education • Total Hysterectomy -The entire uterus, including the cervix, is removed. The procedure may be vaginal or abdominal, with laparoscopic or robotic assistance. • Bilateral Salpingo-Oophorectomy (BSO)- Fallopian tubes and ovaries are removed. • Panhysterectomy - Total abdominal hysterectomy and BSO: The uterus, ovaries, and fallopian tubes are removed. • Radical Hysterectomy - The uterus, cervix, adjacent lymph nodes, upper third of the vagina, and surrounding tissues (parametrium) are removed. • Leiomyomas are the most common reason for hysterectomies Postoperative care • Assess vaginal bleeding • Abdominal bleeding at the incision site (a small amount is normal) • Intactness of the incision • Urine output per urinary catheter for 24 hours • Incisional or abdominal pain • Perineal care • Deep breathing exercises Education o Avoid sexual intercourse, douching o Report excessive bleeding or changes in discharge o Avoid heavy lifting or strenuous activity- can cause hernias or ruptures of sutures o hydrate Vulvovaginitis- s/s, causes, treatment, education • Inflammation of the lower genital tract resulting from a disturbance of the balance and hormones and flora Signs/Symptoms • Itching • Change in vaginal discharge, odor, or lesions Causes • Yeast • Bacterial vaginosis • Changes in normal flora Education • Teach wearing of cotton underwear • Avoiding tight clothing • Front to back wiping • No douching • Do not have sex if partner infected • Sitz baths, breathable cotton, avoid irritants Toxic shock syndrome • An infection caused by staph or strep (mainly staph) • Not necessarily from tampons o tampon is inserted into vaginal and causes micro-abrasions when inserted – if there for long period of time = more prone to bacterial growth Education: • Wear pads to bed • Change tampons every 4 hours • Do not use super absorbent tampons • Avoid sprays for hygiene, douching Treatment: • IVF • Antibiotics Prostate cancer- risk factors, s/s, lab tests, screening, metastases, post-op education, interventions, and complications • Prostate cancer screening is recommended to start discussion with provider at age 50* Risk Factors: Men over age 65 are at greatest risk & family history • If family history, screening starts at age 40* Lab tests: • PSA/digital rectal examination Signs/Symptoms: • Urinary symptoms (dribbling/incontinence) • Unexpected weight loss • Blood in urine BPH- s/s, treatment, education • Enlarged prostate tissue and compresses urethra Signs/symptoms • Difficulty urinating (maintaining or starting the stream) • Increased urination • Dribbling • Nocturia • Painful infection = UTI Treatment • Alpha blocker (doxazosin) – urinary retention and can also help with blood pressure • Reductase inhibitor (finasteride) – 1st line drug therapy Education Holistic care • Multidimensional care pieces: Mental, physical, psychosocial • Collaboration • Caring for the patient as a whole** • People can be scared about cancer MDC CARE o Address fear and anxiety Testicular cancer • Most at risk: people who have non-distended testes • Most common age its seen: Younger adults (age 15-30) • Most of time patient is going to recognize lump/bump themselves • Psychosocial assessment is important – anxiety, stress, fear Treatment/education: • Most common: remove the testes • Chemotherapy • Seeds? • Prior to getting testes removed = sperm banking so they can have kids down the road Genital herpes • Two types: 1 & 2 o One= oral o Two = genital • If symptoms are absent- viral shedding can still occur • Latex condoms are best to prevent contamination/transmission • Treatment: Valacyclovir (Valtrex) and Acyclovir • Nursing interventions: *** o Analgesics = NSAIDs and topical o Pt education about infection o Sexual transmission o Potential for recurrent episodes o Correct use of therapy Syphilis- s/s, treatment • STI Sign/symptoms • Chancre (primary clinical stage) – often goes undiagnosed • Flu-like symptoms (fever, body aches, headache) – 2nd stage Treatment • Drug of choice: penicillin Genital warts- risk factors, s/s, treatment • Caused by HPV Risk factors • Unprotected sex Signs/symptoms • Bleeding if disrupted • Small, white or flesh-colored papillary growths that may grow into cauliflower-like masses Treatment • Goal is to remove the wart • No current therapy eliminated HPV infection • Podofilox 0.5% cream or gel • Cryotherapy • Trichloroacetic acid or bichloroacetic acid may be applied weekly Chronic renal failure- causes, treatment Causes • Hypertension** • Diabetes** Prerenal (cause acute kidney injury/chronic kidney disease) - dehydration, decreased perfusion to the kidneys Intrarenal - clot in kidneys, glomerulonephritis Post renal - Urinary retention, prostate cancer, tumors, stones, BPH, bladder cancer Treatments • Maintain good blood pressure to avoid overuse of kidneys • Maintain blood sugars • Administer diuretics to remove excess fluids • ESKD – dialysis/kidney transplant • Fluid restrictions o Diet: low/no salt, no protein, renal diet, phosphorus Prevention Control hypertension & diabetes with medication & diet Acute kidney injury- causes, electrolyte imbalances, treatment Causes: perfusion reduction, kidney damage, urine flow obstruction Electrolyte imbalances: potassium Treatment: fluid supplementation, reduce exposure to nephrotoxic agents, diuretics Types of dialysis and nursing considerations related to dialysis Hemodialysis • Patient’s blood is removed and passes through an artificial semipermeable membrane to perform filtration and returned back to patient Peritoneal dialysis • Catheter is placed in peritoneal cavity due to high amount of capillaries • s/s of complication: o pain o increased in weight o signs of infection at catheter site • fluid returning from dialysis solution removed: cloudy solution indicates infection • Can depresss respiratory since fluid is compressing on lungs Nursing considerations • Assessment is nursing intervention-part of nursing process • Before treatment: Evaluate baseline vital signs, weight, laboratory tests • Continually monitor patient for respiratory distress, pain, discomfort • Monitor prescribed dwell time, initiate outflow • Observe outflow amount and pattern of fluid Chlamydia- s/s, treatment, education Signs/symptoms • Many women are asymptomatic • Mucopurulent vaginal discharge (yellowish and opaque) • Urinary frequency • Abdominal discomfort/pain • Cervical bleeding Treatment • Azithromycin or doxycycline Education • Mode of transmission • Incubation period • Possibility of asymptomatic infection • Need for abstinence until treatment is complete STD education • Using a latex or polyurethane condom for genital and anal intercourse • Using a condom or latex barrier (dental dam) over the genitals or anus during oral- genital or oral-anal sexual contact • Wearing gloves for finger or hand contact with the vagina or rectum • Abstinence • Mutual monogamy • Decreasing the number of sexual partners Diabetic nephropathy • HTN and DM are top causes of diabetic nephropathy • Vascular complication of type 1 or type 2 diabetes • Leading cause of ESKD • Severity is related to degree of hyperglycemia the patient generally experiences • Check glucose levels to make sure they maintain stable glucose levels o Know sugar levels (added in class) Nephrotic syndrome • Condition of increased glomerular permeability • Allows larger molecules to pass through the membrane into urine and be excreted o Massive loss of protein into urine, edema formation, and decreased plasma albumin levels o Most common cause is altered immunity with inflammation Signs/symptoms • Severe proteinuria • Low serum albumin levels, high serum lipid levels, fats in the urine, edema (especially facial and periorbital), and hypertension • Reduced kidney function May progress to end stage kidney disease (ESKD) Management based on what is causing disorder Treatment • Treat underlying cause o Immunosuppressive agents o ACE inhibitors ▪ Decrease protein loss in urine o Heparin ▪ Can reduce vascular effects o Dietary changes ▪ May need to decrease protein intake depending on GFR o Mild diuretics o Sodium restriction Incontinence- types, treatment, education • Stress o Most common – inability to retain urine when laughing, coughing, sneezing, jogging- cannot tighten urethra enough to overcome increased bladder pressure o Treatment: change diet, drug therapy – topical estrogen, lose weight, electrical stimulation magnetic resonance therapy o Education: keep a diary and perform Kegel exercises • Urge “overactive bladder” o Loss of urine for no reason after suddenly feeling the need to urinate o Treatment: anticholinergics, antihistamines, bladder training o Education: avoid caffeine and alcohol. Space fluids out throughout the day and limit fluids after dinner. Exercise • Overflow o The involuntary loss of urine associated with the detrusor muscle failing to contract and the bladder becomes overdistended • Mixed o Treatment: surgery, intermittent catheterization, bladder compression, drug therapy o A combination of stress, urge, and overflow • Reflex (detrusor) o when the bladder has reached its maximum capacity and some urine must leak out to prevent bladder rupture o Treatment: surgery, bladder compression and intermittent self- catheterization o Education: massage the bladder area to help manually empty bladder • Functional o incontinence occurring as a result of factors other than the abnormal function of the bladder and urethra. (ex. dementia) o Treatment: treatment of irreversible causes, urinary habit training, containment of urine Cystitis- s/s, treatment, education • Inflammation of the bladder o can be inflammation without infection Signs/symptoms • frequency • urgency • dysuria • hesitancy or difficulty in starting urine stream • cloudy/foul smelling urine • retention • fever • confusion in older adults Treatment • antiseptics or antibiotics • analgesics • Fluconazole is drug of choice* • Increase fluid intake • Comfort Education • Complete all antibiotics • Educate the patient that antibiotics may change color of urine • Avoid harsh soaps and douching • Wipe front to back • Pee after sex Urolithiasis (Kidney stones)- s/s, complications, treatment Signs/symptoms • **Urinary issues – frequency, dysuria, changes in urine • Severe pain • Renal colic – the stone is actually moving through urinary tract – PAIN** o N/V o Pallor Back and abd pain o Diaphoresis • Incomplete emptying of bladder • Hematuria - From irritation of urothelial lining Complications • PAIN – depends where the stones are Treatment • Comfort • Pain meds around clock • Opioid analgesics or NSAIDs Lithotripsy Considerations: Cardiac monitoring (EKG) Diagnostic testing KUB: if large enough CT scan/ultrasound Nursing interventions Education for diet changes Urine strain and send to lab Manage pain*** Flank, back, abd, testicular/scrotal pain Adequate amount of fluid intake 2-3 Ls Pyelonephritis- causes, s/s, treatment, complications • Most common organism – e.coli Causes • Bacterial infection in the kidney and renal pelvis (upper urinary tract) Signs/symptoms • Fever**/chills • Tachycardia • Tachypnea • Flank, back, or loin pain (CVA tenderness)* • Abdominal discomfort • N/V**, urgency, frequency, nocturia • Malaise/fatigue Treatment • Adequate fluid intake* (2-3L) • ECG monitoring • Antibiotics* Acute glomerulonephritis- s/s, diagnosis, complications The glomeruli are inflamed; often seen after strep throat Allow larger molecules to pass; will see blood and protein in the urine Signs/symptoms • Skin lesions • Edema • Hematuria o Difficulty breathing or SOB o Crackles o Changes in elimination – smoky, reddish brown, rusty, or cola colored urine o BP Diagnosis – kidney biopsy 24-hour urine collection *** Complications • Infection • Fluid overload Treatment Antibiotics (to clear strep throat) Polycystic kidney disease- pathophysiology, diagnosis, interventions and treatment Patho • Genetic disorder; fluid-filled cysts develop in nephrons • unilateral/bilateral • Associated with hypertension, abdominal fullness and pain, cyst bleeding, hematuria, kidney stone formation, infections, systemic disease Can cause a decrease in kidney function Cause Genetic disorder Diagnosis • Ask about pain, constipation, urine changes, hypertension, headaches • May have dysuria, nocturia, distended abdomen • Diagnostic assessment o Ultrasonography o MRI* o Urinalysis Interventions • Manage blood pressure • Manage pain • Prevent constipation • Slowing progression Treatment: no treatment will extend kidney function, ACE inhibitors, No NSAIDs Renal cell carcinoma- s/s, treatment options, post-op interventions, education • Most common type of kidney cancer • Most metastasizes to adrenal gland, liver, long bones, other kidney Signs/symptoms • Flank pain • Blood in urine • Kidney mass • Skin may be pallor, dark nipples • Weakness • Weight loss Swelling/abd distension Hematuria Treatment options • Microwave ablation or cryoablation -slow growth • Chemotherapy - not #1 choice • Kidney removal • Nephrectomy = #1 choice (unless they have 1 kidney) Post-op interventions • Monitoring for hemorrhage and adrenal insufficiency • Monitor VS - hypotension • Assess urine output • Manage pain • Prevent infection NCLEX QUESTIONS: ENDOMETRIAL CANCER: A 35 year old woman, with no previous childbirths, presents with a palpable uterine mass upon examination. She states that there is a sharp pain that is uncomfortable in her lower pelvic area. What test should the provider order to diagnose this patient? A. Transvaginal Ultrasound B. PSA levels C. Complete blood count (CBC) D. Test for HPV Which Patient below is NOT at risk for developing Chronic Kidney Disease? A. A 58 year old female with uncontrolled hypertension. B. A 69 year old male with diabetes mellitus. C. A 45 year old female with polycystic ovarian disease. D. A 78 year old female with an intrarenal injury. Questions from Buchanan’s powerpoints: The nurse is caring for four patients. Which patient does the nurse recognize being at the highest risk for development of breast cancer? A.28-year-old male with anorexia B.35-year-old female with four children C.44-year-old male with family history of colon cancer D.60-year-old female with ongoing menarche The nurse is caring for a patient who has been scheduled for a radial right mastectomy. When the patient states, “I’m afraid my partner will think I’m hideous after this surgery,” what is the appropriate nursing response? A. “I’m sure your partner understands” B. “Have you asked your partner about their feelings?” C. “Don’t worry about that now; just get through the surgery” D. “It sounds like you are concerned about the way you will look after surgery” The nurse is caring for a patient who has been recently diagnosed with fibrocystic breast condition. What teaching will the nurse provide? A. Analgesics may decrease pain B. Drink milk to increase calcium intake C. Increase salt intake at time of menses D. Avoid wearing a bra whenever possible Which expected post-surgical finding will the nurse teach the patient who is preparing to undergo a total abdominal hysterectomy? A. The patient will no longer have a period B. Vaginal drainage may be bloody for the first month C. Nutrition education to avoid weight gain D. No menopausal symptoms will be experienced A 52-year-old perimenopausal female broke her wrist after a fall from a ladder. She also reports no health concerns other than intermittent fatigue, insomnia, and hot flashes. What assessment questions should the nurse ask? (Select all that apply.) A. Do you engage in exercise? B. Why weren’t you using more caution on the ladder? C. Can you tell me about your diet? D. What medications are you currently taking? E. Do you have a family history of heart disease? The nurse is caring for four female patients. Which patient does the nurse anticipate may need a referral for hospice services? A. 29 y/o with painful periods B. 44 y/o with fibrous uterine leiomyoma C. 60 y/o with ovarian cancer D. 71 y/o with uterine prolapse An older male is being evaluated for hydronephrosis. What priority health history question will the nurse ask? A. Do you have high blood pressure? B. Have you had a recent urinary tract infection? C. Do you have a family history of kidney disease? D. Do you have difficulty starting and continuing urination? The nurse understands that the patient who has undergone a transurethral resection of the prostate (TURP) is at risk for developing which priority concern? A. Pain B. Infection C. Hemorrhage D. Bladder spasms The nurse is caring for four male patients with testicular cancer. Which does the nurse recognize that is at highest risk to die from testicular cancer annually? A. 54 y/o african american B. 58 y/o caucasian C. 60 y/o asian american D. 67 y/o american indian The nurse is meeting Brian Wayne, a patient whose natal sex is male. The patient reports identifying as a female named Brianne. How should the nurse address the patient? A. It’s nice to meet you, Brian B. How are you feeling today, Brianne? C. Mr. Wayne, I am happy to be your nurse today D. My name is Kris. How would you like me to address you? Which patient statement requires immediate nursing intervention? A. I’m becoming comfortable with my sexuality B. My girlfriend hits me when she’s mad C. I’m thinking about gender reassignment surgery D. My counselor and I are talking about my gender identity Which education regarding hormone therapy will the nurse provide to a female transitioning to male (FtM) patient? A. Avoid sharing needles, as this can transmit HIV or hepatitis B. Testosterone therapy will cause your voice to become higher C. The effects of testosterone therapy will be evident in about a month D. Do not wash your hands after applying testosterone it absorbs faster through your skin What does the nurse identify as the expected outcome when planning care for a patient being treated with antiviral drugs for genital herpes? A. Eradication of the infection B. No chance of transmitting the virus to a partner C. Decrease in the severity and frequency of recurrent outbreaks D. Prevention of viral shedding even when the patient is asymptomatic The nurse is assessing a female patient who reports small, flesh-colored growths in her groin that come and go. What condition does the nurse anticipate? A. Syphilis B. Gonorrhea C. Genital Warts D. Pelvic Inflammatory disease A 20-year-old sexually active male reports symptoms of a low-grade fever, headache, malaise, muscular aches, sore throat, and a rash on his hands and feet. What condition does the nurse anticipate? A. HIV B. HPV C. Syphilis D. Gonorrhea Which patient is most likely to experience renal compromise assessed by decreased urine production? A. A 10 year history of diabetes mellitus B. White blood cell count of 12,000/mm3 C. Recent history of myocardial infarction D. Blood pressure of 92/46 mmHg for 12 hours A patient with kidney failure reports dyspnea. The patient’s pulse oximeter reading is 95% on room air, but is visibly distressed with a respiratory rate of 32 breaths/min. What is the priority intervention? A. Notify the respiratory therapist B. Administer oxygen by nasal cannula C. Elevate the head of the bed to 90 degrees D. Administer a respiratory nebulizing treatment A patient with a history of kidney disease is admitted with acute shoulder pain. Which order should the nurse question? A. Digoxin 0.125mg by mouth daily B. Metoprolol 50 mg by mouth twice daily C. Pan cultures for a temperature over 38.5 D. Ibuprofen 800mg by mouth every 4 hours for pain as needed A 22-year-old male reports burning and difficulty with urination. What priority question will the nurse ask? A. Are you sexually active? B. Do you have low back pain? C. How long have you had these symptoms? D. Have you had a fever in the past 24 hours? The nurse is caring for four patients. Which patient does the nurse assess to be at greatest risk of developing a kidney stone? A. Caucasian male who is obese B. African-American female with family history of kidney stones C. Female with history of frequent urinary tract infections D. Hispanic/Latina female who eats animal protein at every meal The nurse has placed an indwelling urinary catheter via sterile technique. The nurse recognizes that it is how long before bacterial colonization begins? A. 12 hours B. 24 hours C. 48 hours D. 72 hours The nurse is caring for four patients. Which patient does the nurse identify as at highest risk for acute pyelonephritis? A. 19 y/o male with spinal cord injury B. 27 y/o female with urinary reflux C. 37 y/o male with HIV infection D. 44 y/o female with urinary tract stones The nurse is caring for a patient with polycystic kidney disease. Which assessment finding requires immediate nursing intervention? A. Temp of 99 Degrees F B. BP of 170/90 C. HR of 100 BPM D. Urine output less than 30cc/hr Which assessment finding does the nurse anticipate for a patient with chronic glomerulonephritis? (Select all that apply.) A. Increased urinary output B. Specific gravity of 1.010 C. Red blood cells in the urine D. Serum creatinine of < 6mg/dL E. Sodium level of <135 mEq/L Which clinical data requires immediate nursing intervention to prevent progression of acute kidney injury? A. HR of 120 BPM B. BP of 156/88 C. Urine Specific gravity of 1.001mmHg D. Intake of 2000 mL and output of 1500mL in the past 24 hours A patient with end-stage kidney disease (ESKD) has this serum laboratory analysis K+ 5.9 mEq/L Na+ 152 mEq/L Creatinine 6.2 mg/dL BUN 60 mg/dL A. Assess HR and rhythm B. Implement seizure precautions C. Assess the patient’s respiratory status D. Evaluate the patient’s acid-base balance More: Uterine Leiomyoma (Fibroids) Etiology/Patho: Develop from an excessive growth of smooth muscle cells and may be related to hormonal stimulation. They are benign, slow-growing solid tumors of the uterine muscle and are classified based on their position. Risks: Advanced age, nulligravida S/S: acute pain, heavy vaginal bleeding, constipation, urinary frequency/retention, ABD distention, dyspareunia (painful sex), infertility, uterine enlargement Tx/Prevention/Interventions: Manage bleeding, asymptomatic may not need tx, drug therapy or removal to assist with pregnancy, uterine artery embolization and hysterectomy for women who do not want pregnancy. Menopause may shrink unless taking HRT. Can be managed with oral contraception. MIS procedure to have myomectomy which spares the uterus. Complications from sx: Fluid overload, embolism, hemorrhage, perforation, irregular menstrual bleeding-> alert rapid response and to avoid teach post sx care such as use of IS, cough and deep breathing, TEDs..etc. Other complications: altered sexuality, grieving process-> address mental health and psychosocial needs ED Etiology/Patho: Can be organic ( reduction in function from DM, meds, or vascular dx) or functional (psychological reason such as stress) Risks: Inflammation, prostatectomy, pelvic fx, lumbosacral injury, vascular dx like HTN, neurologic condition, endocrine d/o’s, smoking/ETOH, meds like antihypertensives, poor overall health that prevents sex S/S: Inability to achieve/maintain erection Tx/prevention/interventions: Penile doppler ultrasonography determines anatomy/blood flow-> injection given to increase blood flow/no ED meds 2 days prior; cardio workup prior to tx; meds (PDE-5 and vasodilators); vacuum constriction device; penile implant; penile suppository Complications of tx: urethral/genital pain, HTN, s/e of meds (avoid ETOH, no nitrates) Cervical CA and HPV Etiology/Patho: Slow growing cancer can be detected early and treated with good results; however, early is often undetected. S/S do not occur until it is invasive. Risks: HPV (type 16 & 18), chronic cervical inflammation, HIV, immunosuppression, STIs, early sex, multiple sexual partners, male partner with previous partner with cervical cancer, socioeconomic factors, AA, smoking S/S: painless bleeding between periods, dysuria, hematuria, vaginal discharge, wt loss, pelvic pain, pain during/after sex, rectal bleeding, chest pain/coughing, leg pain or edema Tx/prevention/interventions: PAP and HPV testing, HPV vaccine, colposcopy with biopsy, leep, ablasion/laser, HPV typing, CXR, MRI, CT, PET, ABTs, removal of lesion, radiation, hysterectomy, exenteration, monitor bleeding, teach about wound care, assess for body image issues, manage drains, monitor skin, teach showers not baths, no heavy lifting/vaginal penetration/douches/tampons for 3 weeks Complications: infection, fistula development, kidney infection [Show More]
Last updated: 1 year ago
Preview 1 out of 37 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Feb 25, 2022
Number of pages
37
Written in

Additional information
This document has been written for:
Uploaded
Feb 25, 2022
Downloads
0
Views
51