*NURSING > STUDY GUIDE > NUR 2488 Mental Health Exam 1 Study Guide | Download To Score A (All)
NUR 2488 Mental Health Exam 1 Study Guide | Download To Score A
Document Content and Description Below
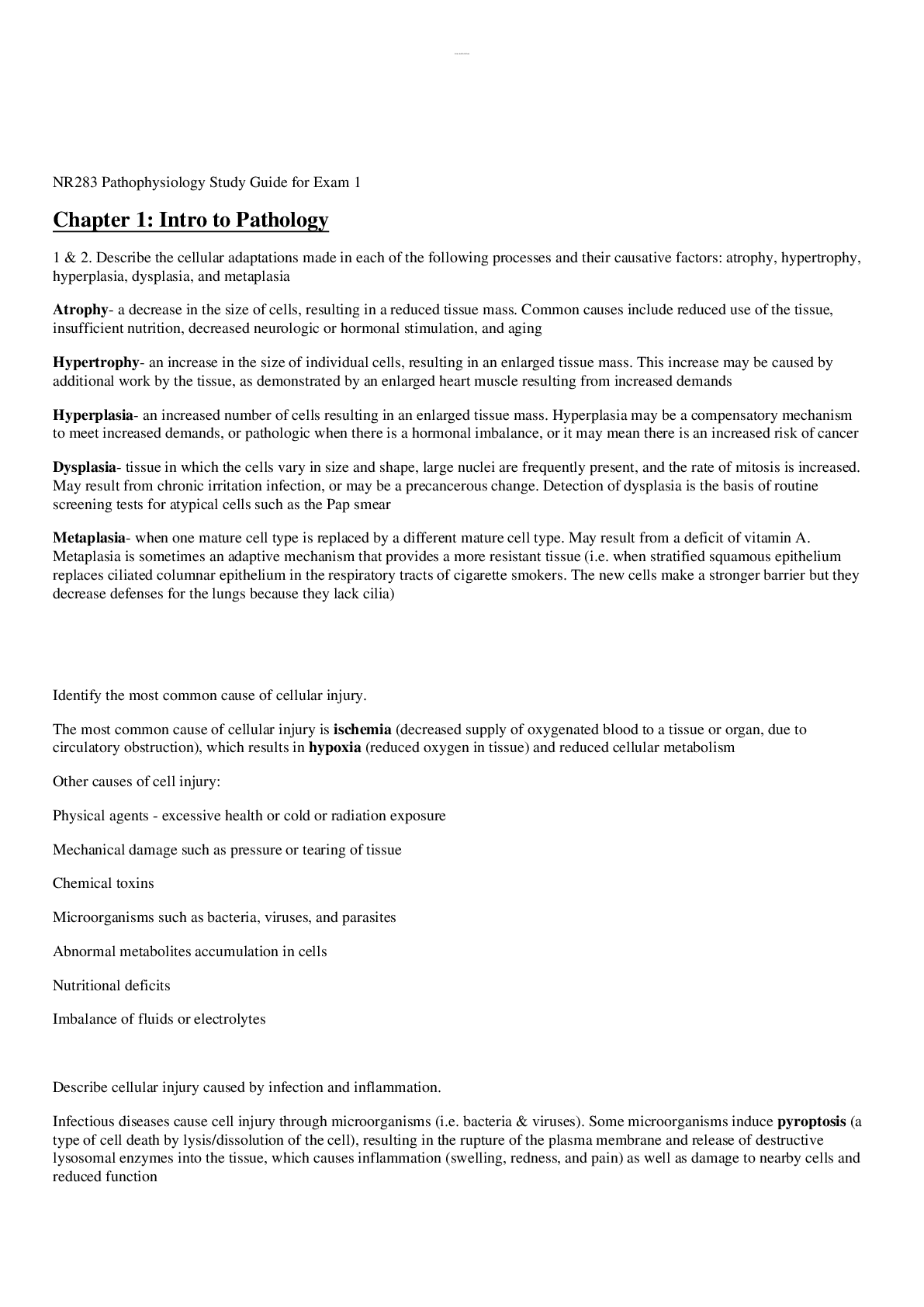
Mental Health Exam 1 Theorists: ❖ Freud ▪ Id: The primitive, pleasure-seeking part of our personalities that lurks in the unconscious mind. ▪ Ego: Our sense of self. Acts as an intermedi... ary between the Id and the world by using ego defense mechanisms, such as repression, denial, and rationalization. Engages in secondary process thinking, which is rational, realistic, and orientated towards problem solving. ▪ Superego: Assigned to those processes that Freud referred to as our conscience and is greatly influenced by our parents' or caregivers' morals and ethical stances. ❖ Maslow’s Hierarchy of Needs ▪ 1. Physiological- food, water, oxygen, elimination, rest, sex ▪ 2. Safety- protection, security, stability, order, structure, limits ▪ 3. Love and Belonging Needs- affiliation, affection, lover ▪ 4. Esteem- competency, achievement, esteem from others ▪ 5. Self Actualization- becoming everything one is capable of ❖ Erikson’s Stages of Development ▪ Infant: Birth - 1.5 yrs old o Trust vs. Mistrust o Task: develop a basic sense of trust and comfort and minimal fear and uncertainty. ▪ Early childhood (toddler) - 1.5-3 yrs old o Autonomy vs. Shame/doubt o Task: gain self-control and independence ▪ Preschooler 3-6 yrs old o Initiative vs. Guilt o Task: achieve sense of purpose and task mastery ▪ School age 6-12 yrs old o Industry vs. Inferiority o Task: self-confidence thru learning and competition ▪ Adolescent 12-20 yrs old o Identity vs. Role confusion o Task: differentiation from parents leads to fidelity, integrate all the above for sense of self ▪ Young adult 20-30 yrs old o Intimacy vs. isolation o Task: form intense long term relationships ▪ Adult 30-65 yrs old o Generativity vs. Self-absorption o Task: achieve life goals and obtain concern for future generation ▪ Older adult 65+ o Integrity vs. Despair o Task: derive meaning from life and sense of self worth Role of neurotransmitters as related disorders: ❖ Dopamine ▪ Increase: o Schizophrenia o Mania ▪ Decrease: o Parkinson's disease o Depression ▪ Functions: o Fine muscle movement o Integration of emotions and thoughts o Decision making o Stimulates hypothalamus to release hormones (sex, thyroid, adrenal) ❖ Serotonin ▪ Increase: o Anxiety states ▪ Decrease: o Depression ▪ Functions: o Mood o Sleep regulation o Hunger o Pain perception o Aggression and libido o Hormonal activity ❖ Norepinephrine ▪ Increase: o Mania o Anxiety o Schizophrenia ▪ Decrease: o Depression ▪ Functions: o Mood o Attention and arousal o Stimulates sympathetic branch of autonomic nervous system for "fight or flight" in response to stress ❖ GABA ▪ Increase: o Reduction of anxiety o Schizophrenia o Mania ▪ Decrease: o Mania o Anxiety o Schizophrenia o Huntington chorea (Huntington's disease) ▪ Functions: o Inhibitory neurotransmitter: o Reduces anxiety, excitation, aggression o May play a role in pain perception o Anticonvulsant and muscle-relaxing properties o May impair cognition and psycho motor functioning Nurse-Client Relationship: ❖ Orientation ▪ Can last for a few meetings or long period of time, the first time the nurse and patient meet. o An atmosphere is established in which rapport can grow. o The nurse's role is clarified, and the responsibilities of both the patient and the nurse are defined. o The contract containing the time, place, date, and duration of the meetings is discussed. o Confidentiality is discussed and assumed. o The terms of termination are introduced. o The nurse becomes aware of transference and countertransference issues. o Patient problems are articulated, and mutually agreed goals are established. ❖ Working ▪ Allows for the patient to experience increased levels of anxiety and demonstrate dysfunctional behaviors in a safe setting while experimenting with new and more adaptive coping behaviors. o Maintain the relationship o Gather further data o Promote the patient's problem-solving skills, self-esteem, and use of language o Facilitate behavioral change o Overcome resistance behaviors o Evaluate problems and goals, and redefine them as necessary o Promote practice and expression of alternative adaptive behaviors ❖ Termination phase ▪ The final, integral phase of the nurse-patient relationship. Termination is discussed during the first interview, and again during the working stage at appropriate times. Termination may occur when the patient is discharged or when the student's clinical rotation ends. o Summarizing the goals and objectives achieved in the relationship o Discussing ways for the patient to incorporate into daily life any new coping strategies learned during the time spent with the nurse o Reviewing situations that occurred during the time spent together o Exchanging memories, which can help validate the experience for both nurse and patient and facilitate closure of that relationship ❖ Nurse-client vs social relationship ▪ The therapeutic relationship between nurse and patient differs from both a social and an intimate relationship in that the nurse maximizes his or her communication skills, understanding of human behavior, and personal strengths to enhance the patient's growth. Patients more easily engage in the relationship when the clinician's interactions address their concerns, respect the patient as a partner in decision making, and use language that is straightforward. ❖ Boundaries with clients ▪ Patient needs separated from nurses needs ▪ Warning signs: over helping, controlling, narcissism ▪ Relationship is no longer helpful if boundaries are broken. ❖ Role of psych RN Nursing process: ❖ Developing plan of care ❖ Developing a goal/outcome ❖ Mental health vs mental illness The interview: ❖ Sections of the psychiatric assessment ▪ Establish rapport. ▪ Obtain understanding of the current problem. ▪ Review physical status and obtain baseline vital signs. ▪ Assess risk factors affecting the safety of the patient or others (suicide or homicide). ▪ Perform a mental status examination (MSE). ▪ Assess psychosocial status. ▪ Identify mutual goals for treatment. ▪ Formulate a plan of care. ▪ Document data in a retrievable format. ❖ Sections of the MSE ▪ Personal: age, gender, marital status, religion, race, ethnicity, employment, living ▪ Appearance: dress, grooming, pupils, expressions, height and weight, scars, tattoos, appearance vs age ▪ Behavior: body movements, peculiar (repetitive, scanning environment), abnormal (tardive dyskinesia), eye contact ▪ Speech: rate, volume, disturbances, cluttering ▪ Affect: flat, bland, animated, angry, withdrawn, appropriate ▪ Mood: sad, labile, euphoric ▪ Thought: organized, coherent, flight of ideas, delusions, obsessions ▪ Cognition: A&O x3, LOC, memory, attention, abstraction, insight, judgment ❖ How to assess ▪ Attention o Digit span test - patient is asked to repeat increasing lengths of numbers forwards, and then backwards. o Serial sevens - patient is asked to start at 100 and subtract 7, then keep subtracting 7 from each answer. ▪ Abstraction ▪ Insight o Insight is an understanding of their condition (including abnormal thoughts) o Tell me about your illness and if it is worse now? o What medications are you taking? ▪ Judgement o Judgment is an assessment of real life problem-solving skills o What should you do if you find a stamped (not canceled) and addressed envelope? ❖ Considerations that should be evaluated during an interview Communication: ❖ Empathetic vs sympathetic responses ▪ Empathetic o We UNDERSTAND the feelings of others. o "How upsetting this must be for you. Something similar happened to my mother last year and I had so many mixed emotions. What thoughts and feelings are you having?" ▪ Sympathetic o We FEEL the feelings of others. o "I know exactly how you feel. My mother was hospitalized last year and it was awful. I was so depressed. I still get upset just thinking about it." ❖ Examples of therapeutic communication techniques ▪ Using silence o Encourage a person to talk by waiting for the answers. ▪ Accepting o "Yes." "Uh-huh." "I follow what you say." ▪ Giving recognition o "Good morning, Mr. James." "You've combed your hair today." "I notice that you shaved today." ▪ Offering self o "I would like to spend time with you." "I'll stay here and sit with you a while." ▪ Offering general o "Go on." "And then?" "Tell me about it." ▪ Giving broad openings o "Where would you like to begin?" "What are you thinking about?" "What would you like to discuss?" ▪ Placing the events in time or sequence o "What happened before?" "When did this happen?" ▪ Making observations o "You appear tense." "I notice you're biting your lips." "You appear nervous whenever John enters the room." ▪ Encouraging description of perception o "What do these voices seem to be saying?" "What is happening now?" "Tell me when you feel anxious." ▪ Encouraging comparison o "Has this ever happened before?" "Is this how you felt when...?" "Was it something like...?" ▪ Restating o Patient: "I can't sleep. I stay awake all night." Nurse: "You have difficulty sleeping?" Patient: "I don't know ... he always has some excuse for not coming over or keeping our appointments." Nurse: "You think he no longer wants to see you?" ▪ Reflecting o Patient: "What should I do about my husband's affair?" Nurse: "What do you think you should do?" Patient: "My brother spends all of my money and then has the nerve to ask for more." Nurse: "You feel angry when this happens?" ▪ Focusing o "This point you are making about leaving school seems worth looking at more closely." "You've mentioned many things. Let's go back to your thinking of 'ending it all'." ▪ Exploring o "Tell me more about that." "Would you describe it more fully?" "Could you talk about how it was that you learned your mom was dying of cancer?" ▪ Giving information o "My purpose for being here is..." "This medication is for..." "The test will determine..." ▪ Seeking clarification o "I am not sure I follow you." "What would you say is the main point of what you just said?" "Give an example of a time you thought everyone hated you." ▪ Presenting reality o "That was Dr. Todd, not a terrorist stalking and trying to harm you." "That was the sound of a car backfiring." "Your mother is not here; I am a nurse." ▪ Voicing doubt o "Isn't that unusual?" "Really?" "That's hard to believe." ▪ Seeking consensual o "Tell me whether my understanding agrees with yours." ▪ Verbalizing the implied o Patient: "I can't talk to you or anyone else. It's a waste of time." Nurse: "Do you feel that no one understands?" ▪ Encouraging evaluation o "How do you feel about...?" "What did it mean to you when he said he couldn't stay?" ▪ Attempting to translate into feelings o Patient: "I am dead inside." Nurse: "Are you saying that you feel lifeless? Does life seem meaningless to you?" ▪ Suggesting o "Perhaps you and I can discover what produces your anxiety." "Perhaps by working together we can come up with some ideas that might improve your communications with your spouse." ▪ Summarizing o Have I got this straight?" "You said that..." "During the past hour, you and I have discussed..." ▪ Encouraging formulation of a plan of action o "What could you do to let anger out harmlessly?" "The next time this comes up, what might you do to handle it?" "What are some other ways you can approach your boss?" ❖ Examples of Non-therapeutic communication techniques ▪ Giving premature advice o "Get out of this situation immediately." ▪ Minimizing feelings o Patient: "I wish I were dead." Nurse: "Everyone gets down in the dumps." "I know what you mean." "You should feel happy you're getting better." "Things get worse before they get better." ▪ Falsely reassuring o "I wouldn't worry about that." "Everything will be all right." "You will do just fine; you'll see." ▪ Making value judgments o "How come you still smoke when your wife has lung cancer?" ▪ Asking ”why” questions o "Why did you stop taking your medication?" ▪ Asking excessive questions o Nurse: "How's your appetite? Are you losing weight? Are you eating enough?" Patient: "No." ▪ Giving approval; agreeing o "I'm proud of you for applying for that job." "I agree with your decision." ▪ Disapproving; disagreeing o "You really should have shown up for the medication group." "I disagree with that." ▪ Changing the subject o Patient: "I'd like to die." Nurse: "Did you go to Alcoholics Anonymous like we discussed?" Cultural Considerations: ❖ Ethnicity ▪ Define: Category of people who identify with eachother based on common language, ancestral, societal, cultural, or national experiences. ▪ Examples: African Americans, Asians, Hispanic ❖ Culture ▪ Define: The concept of culture is most often considered with racial or ethnic minority groups. However, the concept of culture also includes sexual orientation, age groups, physical abilities or disabilities, gender, religion, or socioeconomic status. ▪ Examples: traditions of thought and behavior, such as language and history that can be socially acquired, shared, and passed on to new generations. ❖ Impact of culture to patient care Ethics: ❖ Negligence ▪ Define ▪ Examples ❖ Autonomy ▪ Define: Respecting the rights of others to make their own decisions. ▪ Example: Acknowledging the patient's right to refuse medication. ❖ Justice ▪ Define: The duty to distribute resources or care equally, regardless of personal attributes. ▪ Example: An intensive care unit (ICU) nurse devotes equal attention both to a patient who has attempted suicide and to another patient who suffered a brain aneurysm. ❖ Beneficence ▪ Define: The duty to act so as to benefit or promote the good of others. ▪ Example: Spending extra time to help calm an extremely anxious patient is a beneficent act. ❖ Fidelity ▪ Define: Also called non-maleficence. Maintaining loyalty and commitment to the patient and doing no wrong to the patient. ▪ Example: Maintaining expertise in nursing skill through nursing education demonstrates fidelity to patient care. ❖ Veracity ▪ Define: One's duty to communicate truthfully. ▪ Example: Describing the purpose and side effects of psychotropic medications in a truthful and non-misleading way. ❖ Examples of how these are used in patient care ❖ Patient’s rights ▪ Right to treatment ▪ Right to refuse treatment ▪ Right to informed consent ▪ Freedom from unreasonable restraints ❖ Limited rights to involuntarily admitted clients ❖ Duty to Warn and how it is used in psychiatric nursing ▪ Must warn a patient's potential victim of potential harm ❖ HIPPA and how it is used in psychiatric nursing ▪ The psychiatric patient's right to receive treatment and to have confidential medical records is legally protected. The fundamental principle underlying the ANA Code of Ethics for Nurses on confidentiality is a person's constitutional right to privacy. Generally, your legal duty to maintain confidentiality is to protect the patient's right to privacy. ▪ You may not, without the patient's consent, disclose information obtained from the patient or information in the medical record to anyone except those individuals for whom it is necessary for implementation of the patient's treatment plan. Special protection of notes used in psychotherapy that are kept separate from the patient's health information was created by this HIPAA rule. ❖ When is it appropriate to use restraints/seclusion? ▪ Restraints o When the particular behavior is physically harmful to the patient or a third party o When alternative or less restrictive measures are insufficient in protecting the patient or others from harm o When the patient anticipates that a controlled environment would be helpful and requests seclusion ▪ Seclusion o Provides comfort and relief to patients who can no longer control their own behavior o When a decrease in sensory over-stimulation is needed o Reduces overwhelming environmental stimuli o Protects a patient from injuring self, others, or staff o Prevents destruction of personal property or property of others Psychopharmacology: ❖ Classes of medications used to treat psychiatric disorders (know generics) Antidepressants: ❖ SSRIs- Inhibit reuptake of serotonin (therefore increases it); used for depression, OCD, anxiety, panic disorder (used the most for depression because of the least amount of side effects) ▪ Medications: o fluoxetine (Prozac) o sertraline (Zoloft) o paroxetine (Paxil) o citalopram (Celexa) o escitalopram (Lexapro) o vortioxetine (Brintellix) ▪ Side effects: o Dry mouth o Blurred vision o Insomnia o Headache o Nervousness o Anorexia o N/V/D o Sexual dysfunction o Suicidal ideation ▪ Teaching: o Take in AM to avoid insomnia o Advise patient that it may take 3-4 weeks for the medication to work. ❖ Tricyclics- Inhibit reuptake of norepinephrine and serotonin (increasing their levels); Used for major depression. ▪ Medications: o amitriptyline (Elavil) o nortriptyline (Pamelor) (also used for nerve pain) o clomipramine (Anafranil) o protriptyline (Vivactil) o imipramine (Tofranil) (also used for nerve pain) ▪ Side effects: o Orthostatic hypotension o Sedation o Anticholinergic effects o Cardiotoxicity o Seizures ▪ Teaching: o Take at night due to sedation effect. ❖ MAOIs- Inhibits the enzyme MAO that breaks down norepinephrine and serotonin. Used as a second or third line for depression (last resort). Most dangerous! ▪ Medications: o isocarboxazid (Marplan) o phenelzine sulfate (Nardil) o tranylcypromine sulfate (Parnate) o selegiline HCl (Emsam, Eldepryl) ▪ Side effects: o orthostatic hypotension o hypertensive crisis if food containing tyramine is eaten o agitation o headaches o anticholinergic effects o photosensitivity ▪ Teaching: o Avoid tyramine foods! (cheese, cream, yogurt, coffee, chocolate, bananas, raisins, Italian green beans, liver, pickled foods, sausage, soy sauce, yeast, beer, and red wines). o Avoid Any drugs that are CNS stimulants or sympathomimetics (e.g., vasoconstrictors and cold medications containing phenylephrine and pseudoephedrine). o Take at night to avoid insomnia. ❖ Serotonin syndrome ▪ S/S: o Mild restlessness o Shivering o Diarrhea o Muscle rigidity o Fever o Seizures ▪ Nursing implications: Anxiolytics: ❖ Benzodiazepines- Enhance action of GABA. Depresses the limbic and subcortical CNS. Used for antianxiety. ▪ Medications: o diazepam (Valium) o clonazepam (Klonopin) o alprazolam (Xanax) o flurazepam (Dalmane) o triazolam (Halcion) o lorazepam (Ativan) ▪ Side effects: o High incidence of dependence, taper slowly o Drowsiness o Dizziness o Hypotension o respiratory depression ▪ Teaching: o Eat small, frequent meals o Rise slowly from sitting to standing o Don't drink alcohol o Don't discontinue abruptly o Don't drive Antipsychotics: ❖ Typical/conventional/first generation ▪ Medications: o chlorpromazine HCl (Thorazine) o fluphenazine HCl (Prolixin) o perphenazine (Trilafon) o thioridazine HCl (Mellaril) o haloperidol (Haldol) o loxapine (Loxitane) o molindone HCl (Moban) o thiothixene HCl (Navane) ▪ Side effects: o Sedation o EPS symptoms o orthostatic hypotension o headache o photosensitivity o dry mouth and eyes o blurred vision ▪ Teaching: ❖ Atypical/Second Generation ▪ Medications: o clozapine (Clozaril) o risperadone (Risperdal) o quetiapine (Seroquel) o olanzapine (Zyprexa) o iloperidone (Fanapt) o lurasidone HCl (Latuda) o ziprasidone HCl (Geodon) o aripiprazole (Abilify) o paliperidone (Invega) ▪ Side effects: o Sedation o Drowsiness o Weight gain o Weight loss o Headaches o Fatigue o Blurred vision o Photosensitivity o Alopecia o Peripheral edema o Amenorrhea o Hyperglycemia o Insomnia o Anxiety o Agitation o Constipation o N/V o Arthralgia o Dizziness o Sexual dysfunction ▪ Teaching: ❖ Identify potentially fatal side effects- recognize S/S ▪ Symptoms of agranulocytosis o Malaise o Fever o Sore throat o Decreased WBC count ▪ Symptoms of neuroleptic malignant syndrome (NMS) o Muscle rigidity o Sudden high fever o Altered mental status o Blood pressure fluctuations o Tachycardia o Dysrhythmias o Seizures o Rhabdomyolysis o Acute renal failure o Respiratory failure o Coma ▪ Symptoms of Extrapyramidal Syndrome (EPS) o Stooped posture o Masklike facies o Rigidity o Tremors at rest o Shuffling gait o Pill-rolling motion of the hand o Bradykinesia. [Show More]
Last updated: 1 year ago
Preview 1 out of 14 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Jan 11, 2022
Number of pages
14
Written in

Additional information
This document has been written for:
Uploaded
Jan 11, 2022
Downloads
0
Views
29


.png)

-3-168.png)