*NURSING > QUESTIONS & ANSWERS > Walden University - NURS 6501N Advanced Pathophysiology Knowledge Check 3 (Latest 2021) 100% Correct (All)
Walden University - NURS 6501N Advanced Pathophysiology Knowledge Check 3 (Latest 2021) 100% Correct Study Guide, Download to Score A
Document Content and Description Below
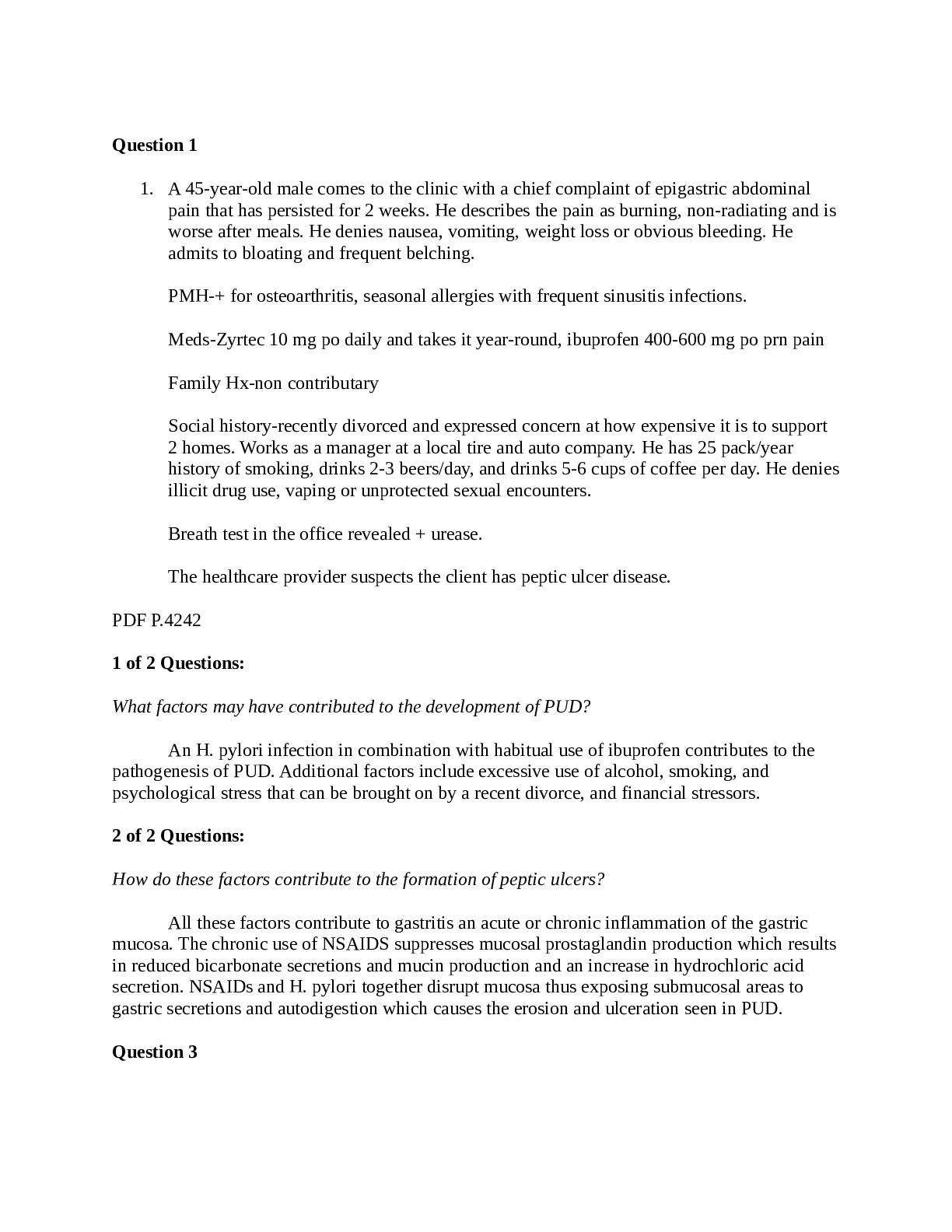
Question 1 1. A 45-year-old male comes to the clinic with a chief complaint of epigastric abdominal pain that has persisted for 2 weeks. He describes the pain as burning, non-radiating and is worse... after meals. He denies nausea, vomiting, weight loss or obvious bleeding. He admits to bloating and frequent belching. PMH-+ for osteoarthritis, seasonal allergies with frequent sinusitis infections. Meds-Zyrtec 10 mg po daily and takes it year-round, ibuprofen 400-600 mg po prn pain Family Hx-non contributary Social history-recently divorced and expressed concern at how expensive it is to support 2 homes. Works as a manager at a local tire and auto company. He has 25 pack/year history of smoking, drinks 2-3 beers/day, and drinks 5-6 cups of coffee per day. He denies illicit drug use, vaping or unprotected sexual encounters. Breath test in the office revealed + urease. The healthcare provider suspects the client has peptic ulcer disease. PDF P.4242 1 of 2 Questions: What factors may have contributed to the development of PUD? An H. pylori infection in combination with habitual use of ibuprofen contributes to the pathogenesis of PUD. Additional factors include excessive use of alcohol, smoking, and psychological stress that can be brought on by a recent divorce, and financial stressors. 2 of 2 Questions: How do these factors contribute to the formation of peptic ulcers? All these factors contribute to gastritis an acute or chronic inflammation of the gastric mucosa. The chronic use of NSAIDS suppresses mucosal prostaglandin production which results in reduced bicarbonate secretions and mucin production and an increase in hydrochloric acid secretion. NSAIDs and H. pylori together disrupt mucosa thus exposing submucosal areas to gastric secretions and autodigestion which causes the erosion and ulceration seen in PUD. Question 3 1. A 36-year-old morbidly obese female comes to the office with a chief complaint of “burning in my chest and a funny taste in my mouth”. The symptoms have been present for years but patient states she had been treating the symptoms with antacid tablets which helped until the last 4 or 5 weeks. She never saw a healthcare provider for that. She says the symptoms get worse at night when she is lying down and has had to sleep with 2 pillows. She says she has started coughing at night which has been interfering with her sleep. She denies palpitations, shortness of breath, or nausea. PMH-HTN, venous stasis ulcers, irritable bowel syndrome, osteoarthritis of knees, morbid obesity (BMI 48 kg/m2 ) Family history-non contributary [Show More]
Last updated: 1 year ago
Preview 1 out of 12 pages
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Dec 24, 2021
Number of pages
12
Written in

Additional information
This document has been written for:
Uploaded
Dec 24, 2021
Downloads
0
Views
79
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)
.png)

.png)
.png)
.png)
, (A Grade), Questions and Answers, All Correct Study Guide, Download to Score A.png)
, Latest Questions and Answers with Explanations, All Correct Study Guide, Download to Score A.png)
, Latest Questions and Answers with Explanations, All Correct Study Guide, Download to Score A.png)
, Latest Questions and Answers with Explanations, All Correct Study Guide, Download to Score A.png)
 110 OUT OF THE 160 TOTAL QUESTIONS FOR EACH VERSION AUTHENTIC Questions and Answers (latest Update), Correct, Download to Score A.png)
, Questions and Answers, All Correct Study Guide, Download to Score A.png)
 (LATEST-2021) CORRECT ANSWERS, DOWNLOAD TO SCORE A.png)
, Latest Questions and Answers with Explanations, All Correct Study Guide, Download to Score A.png)
 All Correct Answers, Download to Score A.png)
 (LATEST-2021) CORRECT ANSWERS, DOWNLOAD TO SCORE A.png)
, Latest Questions and Answers with Explanations, All Correct Study Guide, Download to Score A.png)
, Latest Questions and Answers with Explanations.png)
