*NURSING > TEST BANK > NR-511 Week 4 Midterm MyQBank (GRADED A) Questions and Answer Solutions | productive cough, cough-va (All)
NR-511 Week 4 Midterm MyQBank (GRADED A) Questions and Answer Solutions | productive cough, cough-variant asthma | 100% GUARANTEED.
Document Content and Description Below
NR-511 Week 4 Midterm MyQBank Questions Q bank questions Respiratory An adult has upper respiratory symptoms and cough for the past 14 days. What should be considered? (Pertussis) Pertussis shoul... d always be considered in adults who present with acute cough of greater than 5 days’ duration. The incubation period for pertussis is about 7-10 days. Patients present with URI symptoms for 1-2 weeks. The classic paroxysmal cough usually begins in the second week of the illness. The duration of symptoms and cough are about 3 months even when treated with antibiotics. This is highly infectious and is a reportable disease. Mycoplasma pneumoniae is: (a disease with extrapulmonary manifestations) Mycoplasma is an atypical pathogen and produces atypical pneumonia. It can be difficult to diagnose because symptoms can be varied and involve multiple body systems (extrapulmonary manifestations). Infection with Mycoplasma may present with a normal white blood cell count, maculopapular rash, GI symptoms, tender joints and aches, and, though rare, cardiac rhythm disturbances. Respiratory symptoms may not be pronounced. On chest X-ray there are some unique findings (peribronchial pattern) with Mycoplasma. These include thickened bronchial shadow, streaks of interstitial infiltration, and atelectasis. These are more likely to occur in the lower lobes. Which medication below is contraindicated in an asthma patient because it may increase risk of sudden death if used alone? (Long-acting bronchodilator) A long-acting bronchodilator can be used to treat asthma when it is used in combination with an inhaled steroid. Otherwise, using a long-acting bronchodilator like salmeterol is contraindicated. There is an increased risk of sudden death with asthma exacerbations when this class is used solo to treat asthma. The other choices can be used to treat asthma. Choices vary depending on the patient. A 75-year-old female with emphysema who has been treated with inhaled steroids for many years should: (should be screened for osteoporosis) Older females are at higher risk than others for osteoporosis. This female patient, who has used inhaled steroids and smokes, has multiple risk factors for osteoporosis. Additionally, she probably has emphysema because she smoked (or still smokes). If she is Asian or Caucasian, she has still another risk factor. Screening for osteoporosis should be considered when managing patients with multiple risk factors. A patient received the pneumonia immunization at age 60 years. He is 65 years old and presents to your clinic today. What recommendation should be made about the pneumococcal immunization? (He should receive another one today) This patient should receive another one today because he is 65 years old and at least 5 years has elapsed since his last one. The CDC does not recommend immunizing this patient every 5 years. Two immunizations are available, PCV13 and PPSV23. He needs both, but PCV13 should be administered today. PPSV23 should be administered at least 1 year later. Which of the following medications should be used cautiously in a patient who has asthma? (Timolol ophthalmic drops) Timolol is a beta blocker. This class of medications can precipitate bronchoconstriction in patients who have asthma. Even though timolol is being administered in the eye, it is absorbed through mucous membranes and can exert systemic effects. Beta blockers should be avoided in patients with asthma and used cautiously in patients with COPD. The other medications listed have no specific contraindications for patients with asthma. The most common symptom associated with acute bronchitis is: (Cough) Fever (temp > 101°F) is an unusual symptom associated with acute bronchitis. Cough is the most common symptom associated with acute bronchitis. Purulent sputum is identified in more than 50% of patients with acute bronchitis. The color imparted to the sputum is usually due to sloughing of epithelial cells, not bacterial infection. Concurrent upper respiratory symptoms are typical of acute bronchitis. Pharyngitis is common. Mild persistent asthma is characterized by: (symptoms occurring more than twice weekly) Mild persistent asthma is characterized by symptoms that occur more than twice weekly but not daily; or 3-4 nocturnal awakenings per month due to asthma. It is treated with an inhaled steroid daily, and a bronchodilator PRN for exacerbations. If symptoms occur more than twice weekly, therapy should be stepped up. Generally, a long-acting bronchodilator is added to the steroid when therapy is stepped up. The chest circumference of a 12 month-old is: (equal to head circumference) The chest circumference is not routinely measured at well-child visits, but is assessed if there is concern about the circumference of either the head or the chest. An exception to this observation can occur in premature infants where the head grows very rapidly. Normally, the head exceeds the chest circumference by 1-2 cm from birth until 6 months. Between 6 and 24 months the head and chest circumference should be about equal and by 2 years of age the chest should be larger than the head. The chest circumference is measured at the nipple line. A patient with cough and fever is found to have infiltrates on chest x-ray. What is his likely diagnosis? (Pneumonia) The finding of infiltrates on chest x-ray, in conjunction with clinical findings of fever and cough, should direct the examiner to consider pneumonia as the diagnosis. Other common clinical findings with pneumonia include chest pain, dyspnea, and sputum production. Though not common, some patients with pneumonia exhibit gastrointestinal symptoms like nausea, vomiting, and diarrhea. An uncommon symptom associated with acute bronchitis is: (temperature > 101°F) Fever is an unusual symptom associated with acute bronchitis. Cough is the most common symptom associated with acute bronchitis. Purulent sputum is identified in more than 50% of patients with acute bronchitis. The color imparted to the sputum is usually due to sloughing of epithelial cells, not bacterial infection. Concurrent upper respiratory symptoms are typical of acute bronchitis. Pharyngitis is common within the first 3 days of the illness. Patients who have cough-variant asthma: (all exhibit cough) One of the most common causes of cough in adults is asthma. Cough due to asthma is often accompanied by episodic wheezing or dyspnea, though some patients who have asthma only cough. This is termed “cough-variant asthma.” The clinical presentation of asthma varies but hyper-responsiveness of the airways is a typical finding. The most common cause of atypical pneumonia in adults is: (Mycoplasma pneumonia) In patients who have atypical pneumonia, Mycoplasma is the most common pathogen. M. pneumoniae is so named because of its atypical appearance on chest X-ray. This organism is responsible for “walking pneumonia” that is prevalent in a young adult population. This accounts for about 15% of pneumonia and is transmitted via respiratory droplet. Which patient might be expected to have the worst FEV1? (A 65-year-old with emphysema) FEV 1 stands for “forced expiratory volume in 1 second.” This is the volume of air that is forcefully exhaled in the first second of exhalation after a deep breath. Patients with emphysema are not able to do this efficiently because their alveoli are stretched, and mostly contain trapped air. FEV 1 is used to assess airway obstruction. An asthma patient in the green zone would be expected to have a normal (compared to himself) FEV1. An FEV1 measurement or pulmonary function tests would not be performed on a patient with pneumonia or bronchiectasis because he would have diminished respiratory capacity related to his infection. A patient who has asthma presents with chest tightness, wheezing, coughing, and fever. He has wheezing and diminished breath sounds in the upper right lobe. His cough is nonproductive, and he denies nasal symptoms. Which symptom is not likely related to his asthma? (Fever) Wheezing is typical of asthma, but one must consider pneumonia in any patient who presents with diminished breath sounds in only one lobe. Fever is not typical of asthma or an exacerbation. Ipratropium is very widely used in the treatment of COPD. Which of the following statements about ipratropium is correct? (It decreases parasympathetic tone and produces bronchodilation) Ipratropium is the most widely studied anticholinergic medication used to treat patients with COPD. It produces its helpful effects by reducing cholinergic tone in the lungs. It may be used with a beta agonist if shortness of breath is present. However, beta agonists increase side effects like tachycardia and tremor and do not improve efficacy. An 80-year-old has Stage 3 COPD. He is most likely to have concomitant: (anxiety or depression) About 40% of older patients who have COPD have concomitant anxiety and/or depression. It should be treated because it affects the overall management of COPD. COPD is characterized by airflow limitation and dyspnea. This may contribute to feelings of chronic anxiety. Additionally, many chronic diseases are associated with depression. This is the case with COPD. A 6-year-old child who has moderate persistent asthma is diagnosed with pneumonia after chest X-ray and laboratory studies. He developed a sudden onset of fever with chills. He is in no distress. What is the preferred treatment for him? (Amoxicillin) In children who are older than 5 years of age, the most common bacterial pathogen is an atypical pathogen. Because this child has asthma and uses an inhaled steroid daily, the most likely pathogen is Streptococcus pneumoniae. An abrupt onset of fever and chills is suggestive of Streptococcal pneumonia. Amoxicillin is usually chosen first for its efficacy, cost, and tolerability. The higher dose (80- 100 mg/kg/d) is chosen because of the prevalence of resistant Streptococcus pneumoniae. Azithromycin would be chosen if an atypical pathogen was more likely. Doxycycline is not an appropriate choice because it has poor Strep coverage and it is contraindicated in children younger than 8 years. What disease is usually managed with a short-acting or long-acting inhaled anticholinergic medication? (COPD) First-line treatment for patients with COPD who have intermittent symptoms of shortness of breath is an anticholinergic medication because it improves lung function. Alternatively, a short-acting beta agonist may be used. Anticholinergic medications are not used as a lone agents to manage symptoms of asthma; inhaled steroids usually are. Bronchitis is a viral infection that is self-limited and usually does not require an inhaled medication. Bronchiectasis is a disease in which the respiratory tubules are permanently enlarged. Symptoms include chronic production of purulent mucous. A patient with pneumonia reports that he has rust-colored sputum. What pathogen should the nurse practitioner suspect? (Streptococcus pneumonia) Clinical descriptions of mucus do not really help in clinical decision-making regarding pneumonia, but certain clinical characteristics are associated with specific types of pneumonia. Strep pneumonia, also known as pneumococcal pneumonia, is associated with rust-colored sputum. Scant or watery sputum is associated with atypical pathogens like Mycoplasma and Chlamydophila pneumonia. Thick, discolored sputum may be associated with bacterial pneumonia. A 44-year-old nonsmoker is diagnosed with pneumonia. He is otherwise healthy and does not need hospitalization at this time. Which antibiotic can be used for empirical treatment of pneumonia according to the most recent Infectious Diseases Society of America/American Thoracic Society guidelines? (Azithromycin) The guidelines recommend macrolide use or doxycycline for initial treatment of uncomplicated pneumonia in outpatients who are otherwise healthy and have not had recent antibiotic exposure. The initial choices can be any of these: azithromycin, clarithromycin, or doxycycline. These agents are chosen because they cover atypical pathogens, the most likely pathogen in this population. Fluoroquinolones are commonly used first line in these patients; however, the guidelines strongly recommend using fluoroquinolones for patients with comorbidities or patients who have recent antibiotic exposure. The gold standard for diagnosing pneumonia on chest X-ray is the presence of: (Infiltrates) The finding of infiltrates on chest X-ray, in conjunction with clinical findings of fever, chest pain, dyspnea, and sputum production on clinical exam, should direct the examiner to consider pneumonia as the diagnosis. An 83-year-old healthy adult is diagnosed with pneumonia. He is febrile but in no distress. What is the preferred treatment for him? (Levofloxacin) At age extremes, the most common pathogen is Streptococcus pneumoniae. Because of the age of the patient and the consequences of potential treatment failure, a respiratory quinolone should be considered. Quinolone antibiotics can produce QT prolongation and should be used cautiously in older adults. Azithromycin or doxycycline would be chosen if an atypical pathogen was suspected. This is unlikely in this patient because of his age. The pneumococcal immunization in infants has: (shifted the pathogenesis to fewer cases of S. pneumonia) The heptavalent pneumococcal conjugate vaccine (PCV13), Prevnar, protects children from 13 types of pneumococcal bacteria. It has reduced the incidence of ear infections caused by S. pneumo and has reduced the incidence of recurrent ear infections and tube placement by 10-20%. The pathogenesis of acute otitis media has shifted to more cases of H. influenzae, but this organism is less likely to become resistant, as Strep pneumo has. A 78-year-old adult who has a 50 pack year smoking habit asks the nurse practitioner about the benefits of quitting “at my age.” What should the nurse practitioner reply? (This will decrease your risk of all cause mortality 5 years after stopping) Smoking cessation at any age is beneficial to the person engaging in smoking cessation. Data demonstrates that after 5 years of smoking cessation, there is a significant decrease in the risk of death from coronary disease, cancer, and COPD. The patient already has COPD if he has a 50 pack year habit. All patients should be counseled to quit smoking regardless of age. M. pneumoniae and C. pneumoniae are respiratory pathogens that: (cause atypical pneumonia) These two organisms are common causes of pneumonia. They are called atypical pathogens because they produce atypical pneumonia. They are transmitted via respiratory droplets from the nose and throat of infected people. Prolonged close contact is probably needed for transmission to occur. Patients are usually contagious for 10 days or so. Most commonly, these infections occur in younger patients, but all ages may be affected. Generally, the atypical pathogens are eradicated with macrolide antibiotics or tetracyclines. An 18-month-old child is diagnosed with bronchiolitis. His respiratory rate is 28 breaths per minute. Which choice below is most appropriate for patient management? (Antipyretics) Bronchiolitis is a viral infection and antibiotics would be inappropriate for management. Since fever commonly accompanies bronchiolitis, antipyretics such as acetaminophen and ibuprofen are commonly used. Bronchiolitis is characterized by wheezing. A normal respiratory rate for an 18-month-old is 20-30 breaths/minute. Bronchodilators, especially nebulized, and inhaled/oral steroids are commonly employed to decrease respiratory effort. However, these interventions lack proven benefit, increase the cost of care, and have many side effects. How should a 20-year-old college age student who presents with cough, night sweats, and weight loss be screened for TB? (A TB skin test) Screening for TB in this patient should take place with a skin test known as the Mantoux. A chest X-ray is typically performed after a positive skin test. A sputum specimen is used for diagnosis, not screening. A questionnaire is used for screening patients who have had a history of a positive TB skin test. If symptoms are acknowledged on the questionnaire, a chest X-ray may be performed. The questionnaire is used to prevent inappropriate exposure to radiation in patients in whom regular screening is required, like healthcare providers. An example of a short-acting beta agonist is: (levalbuterol) An example of a short-acting beta agonist is albuterol or levalbuterol. These provide rapid dilation of the bronchioles and can give immediate relief for shortness of breath; hence the term for this class of medications: rescue medications. Salmeterol is a long-acting beta agonist. These should never be used without an inhaled steroid to treat a patient with asthma. Mometasone and beclomethasone are steroids commonly used to treat patients with asthma. A patient with asthma uses one puff twice daily of fluticasone and has an albuterol inhaler for PRN use. He requests a refill on his albuterol inhaler. His last prescription was filled 5 weeks ago. What action by the NP is appropriate? (Increase the dose of the inhaled steroid, refill the albuterol) The patient is using his short-acting bronchodilator excessively if he needs a refill of his inhaler in only 5 weeks. Inhalers typically contain 200 puffs. They should be used two or fewer times per week. His inhaled steroid dose should be increased and his albuterol inhaler should be refilled. In fact, he should not be without a prescription for the albuterol. Consideration could be given to prescribing a long-acting bronchodilator and increasing the steroid, but this is not the best choice because this does not include a refill of the albuterol and this patient cannot be without access to a rescue inhaler. Patients with asthma: (can cough or wheeze) The second leading cause of cough in adults is asthma. Cough due to asthma is often accompanied by episodic wheezing or dyspnea, though some patients with asthma only cough. This is termed “cough variant asthma.” The clinical presentation of asthma varies but hyper-responsiveness of the airways is a typical finding. A 26-year-old being treated for community-acquired pneumonia (CAP) has been taking azithromycin (standard dose) in therapeutic doses for 72 hours. His temperature has gone from 102° F to 101° F. What should be done? (Stop azithromycin and initiate a respiratory quinolone) A 26-year-old with CAP should show improvement in symptoms in 24-48 hours if he is on appropriate antibiotic therapy. Azithromycin treats atypical pathogens like Mycoplasma and Chlamydophila, but, has poor Streptococcus coverage. The most likely pathogen in this age group that causes pneumonia is an atypical pathogen, but at this point the most common typical pathogen, Streptococcus pneumoniae, must be considered. The best choice is to consider Streptococcus pneumoniae as the pathogen and treat with a respiratory quinolone. Specifically, this patient should receive a respiratory quinolone because of the increased incidence of resistant Streptococcus pneumoniae (DRSP). A 60-year-old patient newly diagnosed with COPD presents to your office. He would like to get the influenza immunization. He has no evidence of having had the pneumococcal immunization. What statement is correct? (He should receive both influenza and pneumococcal immunizations today) This patient has COPD. He should receive the pneumococcal immunization today. He belongs to a group of patients with chronic illness who are between the ages of 19 and 64 years and so, should be immunized for pneumonia. The flu immunization should be given to him annually. Which of the following is NOT part of the differential for a patient who complains of cough? (Obesity) All of the other conditions listed, heart failure, GERD, and asthma, are associated with cough. Obesity does not produce cough and is not associated with cough. A 65-year-old has been diagnosed with asthma. Older patients who have newly diagnosed asthma: (are more likely to cough) Asthma is usually diagnosed in children or young adults. Diagnosis after age 65 years is unusual, but 5- 10% of newly diagnosed asthma patients are part of this age group. The most common presentation is cough, not wheezing. Exacerbations are much less variable than in younger adults. This is often initially misdiagnosed because the patient presents with symptoms that seem more like heart failure or COPD. A 67-year-old patient with COPD presents an immunization record that reflects having last received the pneumococcal immunization (PPSV23) when he was 60 years old. Which statement below reflects the current standard of practice recommended by CDC for this patient? (He should be vaccinated today with PCV13) The recommendation by CDC is pneumococcal immunization once at age 65 years regardless of other diseases present. However, if the initial immunization was given prior to age 65 years and 5 years has elapsed since the initial one, he should be revaccinated today. Two immunizations are available, PCV13 and PPSV23. He needs both, but PCV13 should be administered today. PPSV23 should be administered at least 1 year later. A 24-year-old college student who does not smoke is diagnosed with pneumonia. He is otherwise healthy and does not need hospitalization at this time. What antibiotic represents the best choice for treatment for him? (Clarithromycin) A macrolide (like azithromycin or clarithromycin) or a tetracycline (like doxycycline) is used for initial treatment of uncomplicated pneumonia in outpatients who are otherwise healthy and have not had recent antibiotic exposure. These agents are chosen because they cover atypical pathogens (the organism most likely to have infected him) and provide coverage against nondrug-resistant forms of Streptococcus. Fluoroquinolones are commonly used first line in these patients. However, guidelines strongly recommend using fluoroquinolones for patients with comorbidities and/or those who have suspected macrolide resistant strains of Streptococcus. Inappropriate use of fluoroquinolones will promote development of fluoroquinolone-resistant pathogens. What does a peak flow meter measure? (Expiratory flow) A peak flow meter measures peak expiratory flow; that is, air flow out of a patient’s lungs. Peak flow is sensitive to changes in the respiratory tubules and so reflects narrowing of the airways. The utility of a peak flow meter is especially important for patients with asthma because of the rapid changes that occur prior to the onset of an asthma exacerbation. There is minimal to no benefit of measuring these airway changes in patients with COPD and pneumonia. The major laboratory abnormality noted in patients who have pneumococcal pneumonia is: (leukocytosis) An increased white count is typical in patients with bacterial pneumonia such as pneumococcal pneumonia. Eosinophils can be increased in patients who develop pneumonia secondary to exposure to a very irritating substance like a toxic gas. Gram stain can demonstrate gram-positive or negative pathogens. Leukopenia is an ominous finding, especially in older patients. This indicates a poor prognosis because it means that the immune system is not responding to a potentially fatal pathogen. Which drug class is never used to treat chronic obstructive pulmonary disease (COPD)? (Leukotriene blockers) There is no data to suggest efficacy in treating COPD patients with leukotriene blockers like zafirlukast or montelukast. A long-acting bronchodilator (used twice daily) like salmeterol is commonly used. The long- acting anticholinergic medication tiotropium can be used once daily. Systemic steroids may be used for exacerbations of COPD. A patient who has asthma presents with chest tightness, wheezing, coughing, and fever. He has wheezing and diminished breath sounds in the upper right lobe. His cough is non-productive, and he denies nasal symptoms. Which symptom is most likely related to pneumonia? (Fever) The presence of fever should trigger the practitioner to consider pneumonia. The other symptoms are most likely secondary to asthma. Coughing may be due to asthma and pneumonia. A patient with COPD has been using albuterol with good relief for shortness of breath. He is using it 3- 4 times daily over the past 4 weeks. How should the NP manage this? (Add a long-acting beta agonist) The patient is using albuterol too frequently. It should be used no more than twice weekly because it will lose its effectiveness over time (tachyphylaxis). Albuterol should be used as a rescue medication only. This patient’s medication regimen needs adjusting. The best choice is to consider adding a long-acting beta agonist (or long acting inhaled anticholinergic) and have him use albuterol as a rescue medication only. Which of the following may be used to diagnose COPD? (Pulmonary function tests or spirometry) Spirometry or pulmonary function tests (PFTs) are essential to diagnose COPD. The most important measures are the FEV1 (forced expiratory volume in one second) and FVC (forced vital capacity). Chest radiograph has a poor sensitivity in diagnosing COPD. Only about half of patients with moderately severe COPD can be diagnosed using chest radiography alone. CT scan is able to identify emphysema, but not chronic bronchitis. Arterial blood gases demonstrate hypoxia, but a specific cause is not able to be determined from this test alone. A patient with acute bronchitis was diagnosed at an urgent care center 10 days ago. He reports that he received an antitussive for nighttime cough, a steroid injection and oral steroids, and an antibiotic. Which of these interventions was of greatest benefit in resolution of his symptoms? (None of them) Acute bronchitis is almost always due to a viral infection. The antibiotic had no effect in symptom resolution. Unfortunately, antibiotics are commonly given for acute bronchitis. There is no evidence to support use of steroids as they do not result in quicker resolution of symptoms than placebo. In fact, multiple studies have failed to demonstrate benefit. Time is of greatest benefit in resolution of acute bronchitis symptoms. A 65-year-old patient has COPD. She receives a prescription for an albuterol inhaler. What medication information should be provided to this patient? (This may cause tachycardia) An example of an inhaled beta agonist is albuterol or levalbuterol. These agents stimulate the beta receptors in the lungs and in the heart. This helps the patient breathe better because it produces bronchodilation, but it potentially can produce arrhythmias or angina because beta receptors in the heart can become stimulated too. The dose for a patient with underlying cardiac problems is half the dose (and used with caution). Common side effects of these agents are jitteriness, tremor, nervousness, and potentially hypokalemia if used on a regular basis. A patient presents with symptoms of influenza during influenza season. He has not received the immunization against influenza. What should be used to help diagnose influenza in him? (A nasal swab) Influenza is diagnosed based on the results of a flu swab and the patient’s clinical presentation. A patient with influenza usually demonstrates influenza A (the most predominant strain during an outbreak) or influenza B (the strain identified occasionally during flu season but more often, throughout the rest of the year) if he is infected. The most common cause of pneumonia in people of all ages is: (S. pneumonia) Streptococcus pneumoniae (S. pneumo) is the most common pathogen in community-acquired pneumonia (CAP) worldwide. It is more common in age extremes (the very young and very old) and during winter months. Group A Strep can cause a fulminant pneumonia even in patients who are immunocompetent. Mycoplasma is the most common atypical pathogen that causes pneumonia. Staphylococcus pneumonia is more common postinfluenza in the very young and very old. A patient recently received levofloxacin for 7 days to treat pneumonia. His respiratory symptoms have resolved, but today he calls the office. He reports having severe watery diarrhea, abdominal cramping, and low-grade fever. What should be done? (Order a stool specimen) This history of recent antibiotic exposure suggests C. difficile. A stool specimen should be ordered to assess for infection with C. difficile. Some clinicians will initiate treatment for C. difficile based on this history, especially if the patient’s symptoms are severe or the patient is elderly/debilitated. A 20-year-old college age student has a positive TB skin test. Which choice listed below provides definitive diagnosis of tuberculosis? (A sputum specimen) Screening for TB is performed with a skin test known as the Mantoux. A chest X-ray is typically performed after a positive skin test, but is not diagnostic since TB can affect organs other than the lungs. A sputum specimen is used for definitive diagnosis. A questionnaire is used for screening patients who have had a history of a positive TB skin test. If symptoms are acknowledged on the questionnaire, generally, a chest X-ray is performed. The questionnaire is used to prevent too frequent exposure to radiation in patients in whom regular screening is required, like healthcare providers. A patient has cough, pharyngitis, nasal discharge, and fever. He has been diagnosed with acute bronchitis. Which symptom is least likely in the first 3 days of this illness? (Cough) Cough is the most common symptom associated with acute bronchitis and almost always appears after day 3 of the illness. In the first few days of acute bronchitis, upper respiratory symptoms predominate. In fact, it may be impossible to distinguish upper respiratory infection from acute bronchitis. Pharyngitis and nasal discharge/congestion are common on days 1-3. Acute bronchitis is suggested when cough lasts longer than 5 days. Fever is a relatively uncommon symptom of acute bronchitis. When fever appears along with cough, pneumonia should be strongly considered. Which of the following characteristics is always present in a patient with COPD? (Obstructed airways) COPD, chronic obstructive pulmonary disease, is characterized by obstructed airways. The obstruction is NOT completely reversible even with medication use. Productive cough is likely present in patients with chronic bronchitis but not necessarily emphysema. Shortness of breath does not have to be present (or perceived in patients with COPD). Hypercapnia is more prevalent in patients with emphysema since air trapping occurs. “Good control” of asthma is measured by the number of times weekly a patient uses a rescue inhaler. What choice below indicates “good control”? (Once weekly) Good asthma management is characterized by using short-acting bronchodilators (rescue medication) no more than twice weekly during daytime or twice monthly at nighttime. Using short-acting inhaled bronchodilators 2 times weekly necessitates use of prophylactic medications such as inhaled steroids and possible use of long-acting bronchodilators in conjunction with inhaled steroids. Mr. Smith has smoked for 45 years. Which of the following medications may worsen one of his diseases? (Propanolol) Propanolol is a nonselective beta blocker and might be potentially more harmful in a patient who has COPD than a cardioselective beta blocker. Metoprolol is a cardioselective beta blocker. Typically, cardioselective beta blockers exert their effect on the beta receptors in the heart, but not always. Sometimes there is effect on the beta receptors in the lungs. This could produce shortness of breath and would be described as a drug-disease interaction. Noncardioselective beta blockers like propanolol have a worse effect than cardioselective ones. In any event, beta blocker use should be avoided or used with caution in patients who have lower airway disease. The most common sequela of influenza in older adults is: (Pneumonia) More than 90% of deaths associated with influenza occur in older adults. Pneumonia is the most common cause of death and most common reason for hospital admission in older patients with influenza. Annual influenza immunization is recommended for all adults in the United States. A healthy 7-year-old child is diagnosed with atypical pneumonia. He is febrile but not in distress. What is the preferred treatment for him? (Azithromycin) In this age group (> 5 years), the most common atypical pathogens are Mycoplasma or Chlamydophila. Therefore, a macrolide antibiotic like azithromycin is the preferred agent. It is usually chosen first for its coverage of atypical pathogens. Doxycycline is not an appropriate choice because it is contraindicated in children younger than 8 years, however, it does provide coverage against the atypical pathogens. Amoxicillin provides no coverage of atypical pathogens and so it is a poor choice. A 30-year-old patient with intermittent asthma is using his “rescue” medication once daily. How should this be managed? He should receive a prescription for a(n): (an inhaled steroid) The patient is using his bronchodilator (“rescue” medication) more than twice weekly. This is a signal to the healthcare provider that the patient’s asthma is not well controlled and another medication needs to be used. The next step for this patient is a trial of an inhaled steroid. This should relieve his symptoms and decrease the use of his rescue medication. If an inhaled bronchodilator is overused, it will not continue to produce bronchodilation over time. Which choice below most appropriately differentiates acute bronchitis from pneumonia in a patient who has a productive cough? (Chest X-ray) Nearly all cases of pneumonia can be identified on chest X-ray by the presence of infiltrates. Patients with bronchitis have a normal chest X-ray unless there are other underlying pathologies. CBCs help distinguish bacterial from viral infections. Fever is not used to differentiate acute bronchitis from pneumonia. Sputum specimens are indicated when there is a need to identify organisms in the sputum. The most common cause of pneumonia in an otherwise healthy 3-year-old child is: (a viral infection) In children who are 6 months to 5 years of age, the most common cause of pneumonia is a viral pathogen. Rarely are studies performed to identify viral pathogens, however one of the most common viral pathogens is respiratory syncytial virus (RSV). S. pneumoniae is a common cause of pneumonia in very young children, it is also implicated in older adults as a causative agent in pneumonia. In young and middle adults, Mycoplasma is a common pathogen. Which medication below should be avoided in a patient with stage 3 COPD? (Cough suppressant with codeine) Codeine should be avoided (or used with extreme caution) because the sedative effect of codeine or any narcotic can potentially worsen respiratory depression and worsen hypercapnia. A patient with acute bronchitis and cough for 5 days calls to report that his cough is productive of discolored sputum. He has no other new symptoms. How should the nurse practitioner manage this? (Continue the original plan of care) This is the typical course of acute bronchitis. Acute bronchitis is characterized by cough lasting greater than 5 days, but usually less than 20 days. More than 50% of patients report discolored sputum. Since the overwhelming majority of cases of acute bronchitis are secondary to viral causes, antibiotics are not indicated. Discolored sputum is related to sloughing of epithelial cells and is the reason for the discoloration. Discolored sputum does not indicate bacterial infection. The CDC recommends treating acute bronchitis with antibiotics ONLY when the etiology is pertussis. In all other cases, the patient should be treated with supportive and symptomatic management only. A patient has received a prescription for lisinopril. Which side effect most commonly occurs with this medication? (Dry cough) A common side effect of ACE inhibitors is dry cough. Though estimates vary, 5-20% of patients who receive ACE inhibitors develop a cough. Angiotensin converting enzyme is believed to be responsible for metabolism of bradykinin in the lungs. Bradykinin is thought to be responsible for the cough because it induces production of arachidonic acid metabolites and nitric oxide. These substances may promote cough. The cough associated with ACE inhibitors appears to be a class effect. A 24-year-old presents with fever, rhinorrhea, and paroxysmal, high-pitched cough. This is: (Pertussis) Pertussis is also called “whooping cough.” This is a highly communicable respiratory disease caused by Bordetella pertussis. There are three recognized stages of pertussis: the catarrhal phase, the paroxysmal phase, and convalescence. More adults than children have contracted pertussis in the last decade. Since the outbreak of pertussis in Iowa in 2005, diminished titers were recognized and adolescents are being given a booster with TdaP at 11-12 years of age. A 60-year-old patient reports chronic cough and sputum production. He has a long history of exposure to secondhand cigarette smoke from his wife. What diagnosis is most likely? (COPD) This patient’s exposure to secondhand cigarette smoke from his wife represents a risk factor for COPD even though this patient does not smoke. COPD must be considered in anyone with a history of chronic cough and sputum production, dyspnea at rest or exertion, and history of exposure to tobacco smoke. A patient is diagnosed with asthma. Which question is most important to ask when deciding on medication management? (How often do your symptoms occur?) Diagnosis of asthma, as well as pharmacologic management of asthma, is based on frequency of occurrence of symptoms (wheezing, shortness of breath, cough, etc.). Bronchodilators, both short and long-acting, and inhaled steroids, represent the cornerstone of management of most patients who have asthma. Not all patients with asthma wheeze, therefore, asking that question might not be of great help. Severity of symptoms is subjective. Smoking cessation is important, but not a determinant in selecting medications for asthma management. Breath sounds auscultated over the periphery of the lung fields are quiet and wispy during the inspiratory phase followed by a short, almost silent expiratory phase. These breath sounds are considered: (Vesicular) The three normal breath sounds are vesicular, bronchovesicular, and bronchial. Vesicular breath sounds consist of a quiet, wispy inspiratory phase followed by a short, almost silent expiratory phase. They are heard over the periphery of the lung fields. Bronchial breath sounds consist of a full inspiratory and expiratory phase with the inspiratory phase usually being louder. They are normally heard over the trachea and larynx. Bronchovesicular breath sounds consist of a full inspiratory phase with a shortened and softer expiratory phase. They are normally heard over the hilar region. Crackles are adventitious sounds heard in the lungs and may be due to abnormalities in the lungs. GI The two tests that can indicate current infection with hepatitis B are: (presence of hepatitis B surface antigen and IgM) The earliest serologic marker that indicates acute hepatitis B infection is the presence of hepatitis B surface antigen. It becomes positive about 1-10 weeks after infection, but usually before symptom onset. A positive IgM indicates current infection. The presence of hepatitis B core antibody identifies hepatitis B infection (present or past) with certainty. It does not indicate timing of infection. A mother of a 4-week-old infant visits your office. She states that her baby is vomiting after feeding and then cries as if he is hungry again. What should the nurse practitioner assess? (His abdomen for an olive shaped mass) The symptoms likely reflect pyloric stenosis. The most common time for this to occur is 3-6 weeks. It rarely occurs after 12 weeks of age. Babies who have episodes of projectile vomiting and who demand to be refed are called “hungry vomiters” and a diagnosis of pyloric stenosis should be considered. The olive- shaped mass, if found, probably represents hypertrophy of the lateral edge of the rectus abdominus muscle. It is most easily felt immediately after vomiting. This diagnosis is made much earlier now than it used to be, so problems with dehydration are not as common as decades ago. A patient has the following laboratory value. (anti-HAV IgG: positive). What is the clinical interpretation? (He has immunity to hepatitis A) This patient is immune to hepatitis because he has a positive immunoglobulin G (IgG). This signifies immunity secondary to: (1) past infection, or (2) immunization. A negative IgG signifies absence of immunity to hepatitis A and susceptibility if exposed. The early signs and symptoms of appendicitis in an adult: (are subtle) The most consistent findings in adults with early presentation of acute appendicitis are subtle and difficult to identify. Symptoms may be as vague as indigestion, flatulence, and a feeling of ill-being. Initially, pain can be in the general abdomen, then become periumbilical, and finally localize to the lower right quadrant. Early symptoms are difficult to identify, especially in older adults. A 70-year-old presents to the nurse practitioner’s office for a well exam today. What medication probably has no effect on screening for occult blood in the stool? (Acetaminophen) The exam for occult blood is a screen for colorectal cancer. Aspirin, clopidogrel, NSAIDs, warfarin all decrease the positive predictive value of the test because they all can exacerbate bleeding if it is occurring in the colon secondary to a polyp or tumor. Ideally, the medications mentioned (except acetaminophen) would be stopped prior to the exam to increase the likelihood of test sensitivity, but this is not always possible. Symptoms of uncomplicated reflux disease in older adults should be treated: (with empiric treatment) In older patients without signs of complicated GERD (choking, cough, shortness of breath, pain with swallowing or in the chest), empiric treatment is appropriate. Empiric treatment can take place using proton pump inhibitors or H2 blockers. If H2 blockers are used, famotidine and nizatidine are preferred because of their efficacy and low risk of drug-drug interactions. If symptoms of GERD persist despite initial treatment, or if symptoms are severe, patients should have testing to rule out esophageal cancer, Barrett’s esophagitis, or other conditions of the esophagus and throat. Which symptom is INCONSISTENT with irritable bowel syndrome in older adults? (Onset after 50 years of age) Irritable bowel syndrome (IBS) is common in adults and lasts into older adulthood, but symptoms start prior to age 50 years. Typical symptoms of IBS are diarrhea and constipation intermittently, abdominal pain (one of the criteria for diagnosis), and bloating. Other symptoms that are inconsistent with IBS are associated weight loss, blood in the stool, rectal bleeding, and nocturnal diarrhea. These are more indicative of inflammatory disease or carcinoma of the bowel. A 20-year-old female patient presents with tenderness at McBurney’s point. Appendicitis is considered. What laboratory test should be done initially to determine the etiology of this patient’s abdominal pain? (Serum pregnancy test) A serum pregnancy test should be performed since this patient could have an ectopic pregnancy. Once pregnancy is ruled out, other etiologies can be evaluated. CBC with an elevated white count may indicate that an infection is present. It does not indicate a specific location of the infection. Urinalysis could help determine if the etiology is a urinary tract infection. Symptoms can mimic an appendicitis. Positive vaginal swabs could indicate pelvic inflammatory disease as the cause of the pain. A patient with a suspected inguinal hernia should be examined: (standing) The patient should be examined while he is standing. He should be asked to bear down, cough, or strain during the exam. Though hernias are far more common in males, they can be found in females too. In males, the patient should be asked to stand. The examiner should put his 2nd or 3rd finger through the scrotum and into the external ring. When the patient is asked to cough, a “silky” feel will butt up against the examiner’s finger, and the hernia can be easily felt. A healthcare provider (“the HCP”) was stuck with a needle from a patient suspected to be infected with HIV (“the patient”). A rapid HIV test was performed on the patient and found to be positive. This means that: (the HIV status of the patient requires further testing) The rapid HIV is always performed on the source patient (“the patient”). It is known as an ELISA (enzyme linked immunosorbent assay). In the patient suspected of being HIV positive, it is performed to establish whether or not he was positive at the time of the needle stick. In this case, it was found to be positive, but, this is a screening test, and false positives can occur. Therefore, a confirmatory test, the western blot, is routinely performed on the patient’s specimen to confirm the findings of the ELISA. The healthcare provider will usually be tested with a rapid HIV but it is done to establish HIV status at the time of the needlestick. The results of a rapid test can be performed in less than 20 minutes. A patient has had right upper quadrant pain that has lasted for the past 3 days, but the pain has become acute in the past 12 hours. He has low-grade fever. Which lab test(s) will be elevated if he has pancreatitis? (Serum amylase) Serum amylase levels begin to rise 6-12 hours after pancreatic insult and remain elevated for 3-5 days. The other tests described may be abnormal but are not specific for pancreatitis. A patient presents with complaints of bright red stools over the past week. This symptom could be consistent with: (cancer of the sigmoid colon) Bright red blood in the stools is more characteristic of left-sided colon cancer (descending and sigmoid colon) or rectal hemorrhoids. If blood occurs in the stool in right-sided colon cancers (ascending colon) or gastric ulcers, the stool will be black and tarry. A 24-year-old female presents with pain and tenderness in the right lower abdominal quadrant. Her pelvic exam and urinalysis are within normal limits. Her WBC is elevated and her urine pregnancy test is negative. What is part of the differential diagnosis? (Appendicitis) A CBC with a mild elevation in white cell count indicates that infection is likely. This finding is present in most patients who have acute appendicitis. Right lower quadrant abdominal pain, anorexia, and nausea/vomiting are considered classic symptoms of acute appendicitis. Pelvic inflammatory disease is characterized by cervical motion and adnexal tenderness on bimanual examination. Purulent endocervical discharge may be present. This is unlikely in the presence of a normal pelvic exam. Acute pelvic pain and a positive pregnancy test in women of childbearing age may suggest ectopic pregnancy. The patient’s pregnancy test is negative. Symptoms of a urinary tract infection (UTI) can mimic appendicitis, but this can be ruled out with the patient’s normal urinalysis report. What medication used to treat patients who have GERD provides the fastest relief of heartburn symptoms? (Calcium carbonate) Calcium carbonate is an antacid. It provides rapid changes in gastric pH. This provides relief that can be noticed immediately. The increase in pH lasts for about 30 minutes and corresponds with resolution of symptoms. However, as pH decreases within 30 minutes, symptoms may return. Ranitidine is an H2 blocker. It provides relief in 1-2 hours. This usually lasts for about 6-12 hours. Amantadine is an antiviral not used to treat GERD. Pantoprazole is a proton pump inhibitor. This provides relief after several hours or days of daily consumption. A patient with gall bladder disease has classic symptoms. Which symptom below is NOT classic of gallbladder disease? (Pain that occurs when the stomach empties) The pain associated with cholecystitis is usually constant and may or may not occur in relation to meals, but it rarely occurs after the stomach has emptied (takes several hours) or with fasting. Initial pain is usual after a fatty meal. The pain is usually in the upper right quadrant but is nearly as common in the mid abdomen. The pain can mimic a myocardial infarction and so it must be treated as cardiac pain until proven otherwise. The pain is usually caused by contraction of the gallbladder after a meal. The contraction may force a stone or sludge against the gallbladder outlet. Discomfort can last for several hours. Most patients who have acute hepatitis B infection: (have varied clinical presentations) Most patients with hepatitis B (70%) have subclinical hepatitis. Development of cirrhosis is rare following hepatitis B infection unless other systemic factors are present, such as ethanol abuse, HIV infection, hepatitis C infection, etc. There is no predilection for this disease by gender. When patients are symptomatic, they typically develop nausea, jaundice, and flu-like symptoms with fever, body aches, and fatigue. A patient has been diagnosed with hepatitis A. The most common reported risk factor is: (international travel) Traveling internationally is the most common risk factor. Hepatitis A (HAV) is spread via the fecal-oral route (and is highly contagious), though most people have no recollection of eating or drinking contaminated food/drink. Mexico, Central and South America are countries with the highest reported rates of HAV. Other risk factors are contact with infected family or close contacts and homosexual activity among men. Hepatitis A has declined since vaccination in the US has become widespread. A 6-week-old male infant is brought to the nurse practitioner because of vomiting. The mother describes vomiting after feeding and feeling a “knot” in his abdomen especially after he vomits. The child appears adequately nourished. What is the likely etiology? (Pyloric Stenosis) This scenario is typical of an infant with pyloric stenosis. It is more common in males (88%) and usually is diagnosed before the child is 12 weeks old. The classic presentation is an infant who vomits immediately after eating. The “knot” in the abdomen is the typical “olive-shaped mass” palpable at the lateral edge of the rectus abdominus muscle in the right upper quadrant of the abdomen. The mass is best palpated immediately after vomiting. The differential should include GER, but no mass is palpable. Munchausen syndrome by proxy is the fabrication or induction of an illness in a child in order for the caregiver to receive attention. Which of the following is NOT a risk factor for developing hepatitis B? (Consuming contaminated water) Hepatitis B can be contracted by any of the choices listed except drinking contaminated water. Drinking contaminated water increases the risk of hepatitis A. An 83-year-old patient is diagnosed with diverticulitis. The most common complaint is: (left lower quadrant pain) Diverticular disease is more common in older adults. About 70% of patients diagnosed with diverticulitis have left lower quadrant pain. Rectal bleeding may have varied etiologies, such as rectal carcinoma or hemorrhoids. Bloating and cramping are often found in patients with diverticular disease (diverticulosis) but not specifically diverticulitis. Belching and flatulence are not specifically associated with diverticulosis. Which medication listed below can exacerbate the symptoms of GERD? (Verapamil) Verapamil is a calcium channel blocker. Calcium is needed for muscle contraction. Since the lower esophageal sphincter is opened and closed by muscles, the contraction of these muscles will be less forceful. GERD can be exacerbated in this case. Calcium channel blockers should be avoided in patients with severe GERD or in patients in whom calcium channel blockers exacerbate GERD symptoms. Choose the number on the image that most closely approximates the location of a direct inguinal hernia. (Above pubic bone) Hesselbach’s triangle is the area through which direct inguinal hernias occur. The boundaries of Hesselbach’s triangle are formed by the inguinal ligament, the rectus abdominis muscle, and the epigastric vein and artery. Weakness in the floor of the inguinal canal results in the protrusion of direct inguinal hernias. This weakness is commonly the result of connective tissue abnormalities, but may occur due to a deficiency in the musculature of the abdomen from chronic over-stretching or injury. A 70-year-old patient states that he had some bright red blood on the toilet tissue this morning after a bowel movement. He denies pain. What is the LEAST likely cause in this patient? (Anal fissure) Nearly 1 in 3 patients in this age group with acute lower gastrointestinal bleeding have bleeding secondary to diverticulitis. Nearly 1 in 5 have colorectal cancer or polyps, though, polyps usually do not bleed. Patients who have anal fissures often complain of a tearing pain during bowel movements. Regardless of the etiology, this patient needs referral for a colonoscopy to identify the cause of bleeding. He is at high risk for colon cancer because of his age. The appropriate recommendation is referral to gastroenterology for colonoscopy. GERD (gastroesophageal reflux disease) and physiologic reflux have similar characteristics. However, physiologic reflux: (rarely occurs at nighttime) GERD is usually associated with symptoms that produce injury to the mucosa. This rarely occurs in physiologic reflux. Characteristics typical of physiologic reflux are that it occurs primarily postprandial (like GERD), is usually asymptomatic, rarely occurs nocturnally, and is usually short-lived. In contrast, GERD usually occurs nocturnally, especially when there is lower esophageal sphincter disease. A 56-year-old male patient has been diagnosed with an inguinal hernia. What symptom would make the nurse practitioner suspect an incarcerated hernia? (Pain) A hernia is a weakened area in the muscle where loop of bowel protrudes through the abdominal wall. Normally, hernias are not frankly painful, though they may be tender. A painful hernia should be suspected as one that has become incarcerated or strangulated. Incarceration means that the hernia cannot be reduced; it is trapped. A strangulated hernia means that it is incarcerated and ischemia is present. A strangulated hernia is a surgical emergency. Emergency surgery should be performed within 4-6 hours to prevent loss of bowel. Dilated scrotal veins should cause the examiner to consider varicocele. A 48-year-old patient has the following laboratory values. (anti-HCV: reactive, HCV RNA: detectable). How should they be interpreted? (The patient has hepatitis C) This patient has hepatitis C. He has a reactive HCV antibody (anti-HCV). This is a positive screen for hepatitis C. The HCV RNA level is detectable, which confirms infection. When both the anti-HCV and HCV RNA are positive, the patient can be diagnosed with hepatitis C. At this time, there is no immunization for hepatitis C. Choose the number on the image that most closely approximates the location of an indirect inguinal hernia? (Inguinal fold) The internal inguinal ring is the most common site for development of an indirect inguinal hernia. These can occur in men and women. Though most are probably congenital, symptoms may not be obvious until later in life. Indirect hernias are: more common on the right side. Direct inguinal hernias occur through Hesselbach’s triangle. A patient presents with right upper quadrant and upper abdominal pain. Acute cholecystitis is suspected because the pain radiates to the: (right scapula area) Acute cholecystitis presents with right upper quadrant and/or upper abdominal pain radiating to the right scapular area. The pain is usually steady and aching. Pain in the epigastric area could be associated with a peptic ulcer or dyspepsia. Cancer of the stomach presents with epigastric pain. Acute mechanical colon obstruction presents with pain in the lower abdomen. A 63-year-old male has been your patient for several years. He is a former smoker who takes simvastatin, ramipril, and an aspirin daily. His blood pressure and lipids are well controlled. He presents to your clinic with complaints of fatigue and “just not feeling well” for the last few days. His vital signs and exam are normal, but his liver enzymes are elevated. His hepatitis panel is negative for infectious hepatitis. What is the most likely cause of his elevated liver enzymes? (Daily grapefruit consumption for the past 10 days) Grapefruit is a potent inhibitor of the cytochrome P450 enzyme system. Statins and calcium channel blockers are two infamous drug interactions that occur with grapefruit and grapefruit juice. Because they inhibit metabolism of the statin, the patient continues to have statin in circulation because he cannot significantly metabolize the medication. When the next day’s dose is taken, its effect is coupled with the effect of the previous day’s dose. The effect is cumulative. Hepatoxicity can quickly develop. The simvastatin must be stopped immediately! The liver enzymes must be followed until they return to normal; which could take weeks, months or even longer. What is the simplest screen for nutritional adequacy in elderly patients? (Measure their weight) In older adults, serial weight is the simplest screen for assessment of nutritional adequacy. Weight loss in elderly patients is associated with greater mortality than weight maintenance. A 31-year-old patient is suspected of having hepatitis C. He reports possible exposure about a month ago. (anti-HCV: nonreactive, HCV RNA: not detectable). How should the nurse practitioner interpret his laboratory results? (The patient does not have hepatitis C) This patient does not have hepatitis C (HCV) infection. An HCV antibody test (anti-HCV) is recommended as the initial screen for infection. Development of detectable antibodies (anti-HCV) usually occurs between 2-6 months following exposure. The patient's HCV antibody test (anti-HCV) is nonreactive. Typically, subsequent evaluation to detect the presence of HCV RNA is not necessary following a nonreactive anti-HCV result. Because exposure occurred less than 6 months ago, he may lack detectible levels of anti-HCV antibodies, which warrants testing for HCV RNA. HCV RNA levels become detectible before reactive antibodies. HCV RNA was not detected in this patient. This confirms that this patient has a true negative screen for infection with HCV. A patient has been diagnosed with viral gastroenteritis. He has nausea and vomiting, and has started having lower abdominal cramps. What is the most effective intervention for him? (Oral rehydration) Patients with viral gastroenteritis should be treated symptomatically. The goal of therapy is to prevent dehydration and replace electrolyte losses. Antidiarrheals, antispasmodics, and antiemetics can decrease nausea, vomiting, abdominal cramping and symptoms of diarrhea, but should be used with extreme caution when given to older adults or children younger than 5 years of age. Clinical judgment should dictate when it is prudent to initiate these agents. A 35-year-old patient has the following laboratory values. How should they be interpreted? (HBsAG: negative, Anti-HBc: negative, Anti-HBs: negative) (The patient should consider Hepatitis B immunization) This patient has a negative hepatitis B surface antigen (HBsAg). Therefore, he does not have hepatitis B. The patient has a negative hepatitis B core antibody (anti-HBc). Therefore, he has never had hepatitis B. The patient has a negative hepatitis B surface antibody (anti-HBs). Therefore, he is not considered immune, and immunization should be considered. There is a remote possibility that this patient has been immunized but did not produce hepatitis B surface antibodies. If this were the case, he should consider immunization once again. An 85-year-old adult has chronic constipation. How should this be managed initially? (Avoid all constipating medications/foods when possible) Initially, all medications known to cause constipation should be stopped when possible. Symptoms should be reassessed. It is always preferable to stop a medication to correct a condition BEFORE adding a medication to correct a condition. If symptoms persist, a gradual increase in dietary fiber up to 25 grams daily should be added, along with increasing fluid intake. Physical activity should be increased as tolerated. Sorbitol solution and an oil retention enema could be initiated if other options mentioned were not helpful. Which is NOT an effective strategy for helping older adults gain weight? (Increase carbohydrate intake) When treating patients with weight loss, the goal is to increase the number of calories at each meal. Fats are more heavily laden with calories than carbohydrates. Carbohydrates (and proteins) provide only 4 calories per gram; fats provide 9 calories per gram. The addition of fats will increase calories much more quickly than increasing carbohydrate intake. All of the suggestions listed above will increase caloric intake. Daytime snacks should be offered too. Consider a vitamin B supplement because this can stimulate appetite. The relationship between duodenal ulcer disease and H. pylori infection is: (very likely) H. pylori is a gram-negative organism that is a major etiologic factor in development of duodenal ulcer disease, gastric adenocarcinoma and lymphoma of the stomach. Only about 10-15% of patients with H. pylori infection actually develop duodenal ulcer disease, but this is the largest contributor to duodenal ulcer development. Other etiologic factors in duodenal ulcer development are NSAID overuse and smoking. A 37-year-old has routine blood work performed during an annual exam. On exam he has a tender, enlarged liver. How should the nurse practitioner proceed? (Order a hepatitis panel) The differential for a patient with elevated liver enzymes can reflect many different etiologies. Since the liver is tender and liver enzymes are elevated, a likely etiology is hepatitis. The size and consistency of the liver should be ascertained. The spleen should be assessed. If it is palpable, it is enlarged also. Hepatitis panel should be performed and strong consideration given to referral to gastroenterology. Repeating liver enzymes might be considered if the rest of the exam was normal and the lab values were the only abnormal values. The results of a CBC will not change the differential. The patient’s abnormal labs and exam make this urgent, and waiting a week will delay diagnosis and possible treatment. A 19-year-old female presents with lower abdominal pain that began about 12 hours ago. She denies vaginal discharge. Which choice below is the least likely cause of her symptoms? (Renal stone) A renal stone can produce lower abdominal pain, but it is unlikely to produce fever. Low-grade fever might accompany appendicitis, UTI, or a ruptured ovarian cyst. Another diagnosis that must be considered because of her age is pelvic inflammatory disease. In this case, a pelvic exam should be performed. The most common place for indirect inguinal hernias to develop is: (the internal inguinal ring) The internal inguinal ring is the most common site for development of an indirect inguinal hernia. These can occur in men and women. Though most are probably congenital, symptoms may not be obvious until later in life. Indirect hernias are more common on the right side. Direct inguinal hernias occur through Hesselbach’s triangle. A 14 year-old male patient has an acute, painless groin swelling. Which tool would yield the most information to identify the etiology of the swelling? (Ultrasound of the scrotum) The patient has an acute swelling of the groin. Since the etiology could include several scrotal problems (inguinal hernia, hydrocele, or varicocele), an ultrasound will yield quick reliable information with a diagnostic accuracy of 93% for acute groin problems. The definitive treatment for inguinal hernia is surgical repair. Mrs. Lovely, an 84-year-old, complains of fecal incontinence. A likely cause is: (constipation) Underlying constipation is a common cause of fecal incontinence in older adults. However, typically it is multifactorial. Risk factors include: age > 80 years, impaired mobility, and neurologic disorders including dementia. Inactivity and poor fluid consumption may contribute to constipation but are not causes of fecal incontinence. A 40-year-old patient has the following laboratory values. How should they be interpreted? HBsAG: negative, anti-HBs: positive, anti-HBc: negative (The patient has been immunized) This patient has a negative hepatitis B surface antigen (HBsAg). Therefore, he does not have hepatitis B. The patient has a negative hepatitis B core antibody (anti-HBc). Therefore, he has never had hepatitis B. The patient has a positive hepatitis B surface antibody (anti-HBs). Therefore, he is considered immune. The patient is immune from immunization because his hepatitis B core antibody is negative. If the core antibody had been positive, he would be considered immune from the disease. This patient has been immunized. A patient has the following lab values. This indicates that he: (HBsAG: negative, anti-HBc: negative, anti-HBs: positive) (is immune to hepatitis B) This patient is immune to hepatitis B because he has a positive hepatitis B surface antibody. He does not need immunization. His immunity is due to immunization because he has a negative core antibody. The finding of a positive surface antibody and a negative core antibody in this patient indicates immunity from hepatitis B from immunization. If his immunity had been derived from infection, his core antibody would have been positive. A 3-day-old full-term infant has a bilirubin level of 16 mg/dL. How should this be managed? (Order phototherapy for the infant) There are several ways to determine how elevated the bilirubin level is. One measure is to use the Bhutani nomogram. It predicts bilirubin levels based on postnatal age. A level of 16 mg/dL is considered high intermediate. Since the bilirubin probably will rise a little more, phototherapy is probably appropriate. Which imaging study of the abdomen would be LEAST helpful in diagnosing an acute appendicitis? (X- ray) X-rays are usually not helpful in diagnosing appendicitis, however, some findings on radiograph can be associated with appendicitis: ileus, free air, right lower quadrant appendicolith or soft tissue density, or a deformity of the cecal outline. A CT scan is considered more accurate than an ultrasound, but ultrasound and CT are the most commonly used tests. The sensitivity and specificity with CT scan are 94 and 95%, respectively. With an ultrasound, the sensitivity and specificity are 86 and 81%, respectively, but it is the preferred diagnostic test in children because of an absence of radiation. MRI is generally not used because it is more expensive, takes more time to complete, and is not as readily available. A patient has the following laboratory values. What does this mean? (anti-HAV IgM: negative, anti-IgG: negative) (He has no immunity to hepatitis A) This patient does not have immunity to hepatitis A, as evidenced by the negative IgG. He is not currently infected, as evidenced by the negative IgM. This patient should be referred for immunization. The immunization consists of two immunizations given 6-12 months apart. They can be given to infants or adults. The most common cause of diarrhea in adults is: (viral gastroenteritis) Most cases of acute gastroenteritis are viral in origin. Severe diarrhea is usually caused by bacteria and usually lasts longer than 3 days. An 84-year-old presents with a stated involuntary weight loss. He states that he’s lost about 6 pounds in the last 6 or 8 weeks. What statement below is NOT part of the assessment? (Evaluate his upper and lower extremity muscle mass) Involuntary weight loss in older adults is often due to malignancy or disease. The initial assessment of an older adult who reports involuntary weight loss is to document the weight loss. If prior measurements are part of the patient’s chart, this would be helpful. Laboratory assessment should also be performed. Consideration should be given to performing a CBC, TSH, and metabolic panel. Also consider chest and abdominal X-rays. If all are normal, he should be monitored and reweighed on the same scale for comparison. A dietary consult should be ordered. However, even with negative initial findings, a significant number of patients are later found to have disease or malignancy. What choice below is most commonly associated with pancreatitis? (Gallstones and alcohol abuse) In adults, the most common causes of acute pancreatitis are gallstones and alcohol abuse. Pancreatitis in women is more often due to gallstones; in men, due to alcohol abuse. Hypertriglyceridemia can precipitate pancreatitis, but a serum amylase measurement may be normal. This can be a difficult diagnosis to make. The other conditions listed are not associated with pancreatitis. However, viral infections of the pancreas can produce pancreatitis. Most patients who have acute hepatitis A infection: (have a self-limited illness) Clinical presentation of patients infected with hepatitis A virus (HAV) is variable. However, most adult patients have a self-limited, uncomplicated course. There may be mild, flu-like symptoms or there may be a more acute and severe clinical manifestation. Rarely does HAV result in hepatic failure unless other complicating illnesses, like HIV or hepatitis B or C, are present. In children, most are asymptomatic. A 95-year-old male has lost muscle mass as he has aged. He does not have any underlying disease that has caused this loss. What is this termed? (Sarcopenia) Sarcopenia is the term used to describe loss of muscle mass related to aging. The actual definition is a decrease in appendicular muscle mass that is measured as a two standard deviation decrease. It is associated with increased falls, disability, and impairment. In males, this is due to decreased production of testosterone. A patient has the following lab results: (anti-HCV: reactive) This means: (more data is needed) The anti-HCV test is a screening test. A patient who has a reactive screen for hepatitis C may have the disease, but more data are needed to determine this. Once the screen is reactive, a confirmatory test should be performed. The confirmatory test is the HCV RNA. If it is detectable, it indicates past or current infection with hepatitis C. If undetectable, the HCV RNA indicates that the screen was a false positive. What medication may be used to treat GERD if a patient has tried over-the-counter ranitidine without benefit? (Pantoprazole) If a patient has been diagnosed with GERD and he is symptomatic on an H2 blocker like ranitidine, a proton pump inhibitor (PPI) should be considered. An example of a proton pump inhibitor is pantoprazole. Relief of symptoms after using a PPI does not indicate a benign condition. This patient could have esophageal erosions, Barrett’s esophagitis, or esophageal cancer. He should be screened for risk factors for these conditions and then a decision to refer this patient to gastroenterology can be made. Which set of symptoms is most likely in a patient infected with C. difficile? (Diarrhea, abdominal pain, nausea or vomiting) The classic symptoms that patients with C. difficile experience are diarrhea, abdominal pain, and nausea or vomiting. This patient should be treated because symptoms are present. If no symptoms or mild symptoms are present, treatment can be delayed until symptoms develop or worsen. All patients who are infected do not exhibit symptoms. They do not need treatment. Older adults frequently complain of constipation. Which medication listed below does NOT increase the likelihood of constipation in an older adult? (Metformin) Diarrhea, not constipation, is a common side effect of metformin. Constipation is a common complaint in older adults because of medications they routinely consume and many diseases they often have. Some examples of medications that can cause constipation are opiate analgesics, NSAIDs, and antacids. Some diseases and conditions that can produce constipation are hypothyroidism, colon cancer, electrolyte abnormalities, immobility, and change in diet due to inability to chew food properly. A 40-year-old patient has the following laboratory values. How should they be interpreted? (HBsAG: negative, anti-HBc-positive, anti-HBs: positive) (The patient had hepatitis) This patient has a negative hepatitis B surface antigen (HBsAg). Therefore, he does not have hepatitis B. The patient has a positive hepatitis B surface antibody (anti-HBs). Therefore, he is considered immune. The patient also has a positive hepatitis B core antibody (anti-HBc). Therefore, he is immune because he has had hepatitis B. A patient has suspected peptic ulcer disease. Her symptoms occur a few hours after eating. She probably has a: (duodenal ulcer) Symptoms have a poor correlation with disease found during endoscopy. However, duodenal symptoms tend to occur within 2-5 hours of eating. These patients derive relief from eating or taking antacids. This is in contrast to a patient with a gastric ulcer who has symptoms within minutes of eating. He tends to derive less relief from antacids. A patient has received a prescriptions for metronidazole for treatment of C. difficile. What should be avoided in this patient? (Alcohol) Patients should always be cautioned against alcohol ingestion (in any form) if they take metronidazole. Alcohol can (and usually does) produce a disulfiram reaction. This is characterized by abdominal cramps, nausea, vomiting, headache, and elevated body temperature. Precautions should remain until 72 hours after the last dose of metronidazole. A 5-year-old has been diagnosed with pinworms. He lives with his mother. There are no other members of the household. How should his mother be managed? (Perform the “scotch tape” test and look at the collection under the microscope) The diagnosis of pinworms (Enterobiasis) is made by using a piece of scotch tape on a tongue depressor. It is touched against the patient’s rectum. The greatest yield of eggs will occur during the nighttime or early AM. Eggs will be found here if they are present. Worms and eggs are rarely found in stool specimens, so this is not a good plan. When the scotch tape is examined under a low power microscope, the eggs will be easily visualized since they are large and bean shaped. The finding of an adult worm would confirm the diagnosis. These are large enough to be seen with the naked eye. If the mother is symptomatic, she should be treated with or without a rectal exam. It is very likely she is infected. Which of the following symptoms is typical of GERD? (Pyrosis) Typical symptoms of GERD include pyrosis (heartburn). The other symptoms listed are considered atypical symptoms of GERD. Patients who present with atypical symptoms of GERD, especially if older than 50 years, should be considered for endoscopy. An 82-year-old adult has constipation. A supplement known to cause constipation is: (Calcium) Calcium does produce constipation in many patients. If this is taken as a supplement for osteoporosis or osteopenia, the patient should be encouraged to increase fluids and fiber. An inguinal hernia is palpated on a male patient by an examiner. Which word below best describes what the hernia feels like when touched by the examiner? (Silky) Patients should be in the standing position when examined for a hernia. They are asked to strain, cough, or bear down after the examiner has inserted his fingertip within the external ring. The word used to describe the impulse of the hernia bumping into the finger is “silky.” Nodular might be the word used to describe a prostate gland. Bumpy implies an irregular surface on some object. This is not the case with a hernia. Hirschsprung’s disease is characterized by: (failure to pass meconium in the first 48 hours of life) Another name for this condition is aganglionic megacolon. The affected segment of colon is absent of ganglia that are responsible for producing peristalsis. The diagnosis cannot be made in the first 48 hours of life, but a suggestion of the diagnosis can be made because meconium is not passed in a timely manner. Consequently, most infants are diagnosed in the neonatal period. Patients usually present with emesis, abdominal distention, and failure to pass stool. An abdominal X-ray will demonstrate distal intestinal obstruction with dilated bowel loops. The patient should be referred for surgery to remove the diseased segment of colon. Many older adults have cachexia. What characterizes this? (Illness and loss of muscle mass) Cachexia is common in older adults and is associated with increased mortality. It is described as a syndrome of underlying illness that is accompanied by loss of muscle mass. Illnesses associated with cachexia are malignancies, renal disease, COPD, and chronic heart failure. Other matters are associated with cachexia and may contribute to loss of muscle mass. These include loss of appetite, insulin resistance, and increased catabolism of bodily proteins. What medication listed below could be used to increase appetite in an anorexic patient? (Megestrol) Megestrol acetate has a positive effect on weight in patients who are trying to gain weight. It increases appetite and may improve quality of life. Weight gain may take up to 3 months before it is measurable. Megestrol has the potential to cause edema and so should be used cautiously (or not at all) in patients with chronic heart failure. A patient has been diagnosed with hepatitis B. The most common reported risk factor is: (sexual exposure) Hepatitis B is transmitted by blood and body fluids. While exposure to infected blood or blood products would significantly increase risk of infection in unvaccinated people, this is much less likely than becoming infected via sexual exposure or IV drug use. Hepatitis A is transmitted via fecal oral routes. Drinking contaminated water and eating contaminated food implicate hepatitis A as the etiologic agent. Which of the following is an appropriate initial intervention for gastroesophageal reflux disease (GERD) in an 8-week-old? (Small, frequent thickened feedings) Two strategies should be tried initially. First, avoidance of overfeeding is recommended. Hence, small, frequent feedings. Second, milk thickening agents appear to improve symptoms in infants who experience gastroesophageal reflux disease (GERD). Thickened feedings significantly decrease frequency of reflux in most infants. Also, caloric content is increased and this may be helpful for patients who are underweight because of persistent GERD. Generally, when medications are used, proton pump inhibitors are preferred over an H2 blocker like cimetidine. Changing formula generally does not help, however, a milk-free diet may help since 40% of infants with GERD are sensitive to cow’s milk protein. Lateral positioning seems to be ineffective in relieving symptoms in infants. A 42-year-old patient was diagnosed with ulcerative colitis many years ago. What part of his routine health screenings should be stressed by the nurse practitioner? (He should have a colonoscopy every 1-5 years) A history of ulcerative colitis or Crohn’s disease is associated with an increased risk of colorectal cancer. Recommendations vary according to organization, but generally, screening with annual colonoscopy should take place 8-10 years after diagnosis in patients with pancolitis. Colonoscopy should be repeated every 1-5 years, depending on his level of risk. A 20-year-old female patient presents with tenderness at McBurney’s point. What laboratory test supports a diagnosis of appendicitis? (CBC with elevated white count) CBC with an elevated white count indicates that an infection is likely. It is not specific to location of the infection. Urinalysis should be performed to rule out a UTI. Symptoms can mimic an appendicitis. Serum hCG (pregnancy test) must be performed since this patient could have an ectopic pregnancy. Positive pelvic cultures could indicate pelvic inflammatory disease as the cause of the pain. A patient has elevated liver enzymes. What is the likely etiology of the elevation? (Hepatitis) These liver enzymes are elevated. In looking at the numbers, the ALT is grossly elevated compared to the AST. A diagnosis of hepatitis is far more common when the ALT is elevated. AST becomes the dominant liver enzyme when the patient has consumed a substance that causes the liver to be damaged. Examples of this are found in the choices suggesting acetaminophen, alcohol, and drug abuse. An 83-year-old patient is diagnosed with diverticulitis. Where is her pain typically located? (Left lower quadrant) Diverticular disease is more common in older adults. About 70% of patients diagnosed with diverticulitis have left lower quadrant pain; the location of the sigmoid colon. Pain may be present for several days prior to the acute episode. In addition to left lower quadrant pain, bloating and cramping are commonly described by these patients. Diverticulitis occurs secondary to perforations of a diverticulum. The initial step in the management of encopresis is: (client and family education) Encopresis is repetitive soiling of stool by a child who is 4 years of age or older who should be toilet trained. The patient and caregivers of a child with encopresis need education about the underlying cause, usually chronic constipation. The initial step is to remove negative connotations regarding soiling. The caregivers should be educated about changing the child’s chronic behavior patterns. The child should not be scolded. The next step after education is to relieve the constipation with a goal of one soft bowel movement daily. A 45-year-old patient has the following laboratory values. (HBsAG-positive, anti-HBc: positive, anti- HBs: negative) How should they be interpreted? (The patient has hepatitis) This patient has a positive hepatitis B surface antigen (HBsAg). Therefore, he has hepatitis B. A positive anti-HBc is found in patients who either have hepatitis now or who have had it. The surface antibody (anti-HBs) would be expected to be negative in a patient with positive surface antigen (HBsAg) because these two markers will not be positive at the same time. A patient has hepatitis B. He probably has a predominance of: (lymphocytes) Lymphocytes tend to be the predominant white cell present during viral infections. Hepatitis B is a viral infection. The total white count will likely be decreased. This often happens in the presence of viral infections. A bacterial infection is frequently evidenced by an elevated leukocyte count, an increased neutrophil count, and a decreased lymphocyte count. A 43-year-old female patient reports a possible exposure to hepatitis C about 4 months ago. Which statement is true about this patient? (HBsAG: negative, anti-HBc: negative, anti-HBs: positive, anti- HCV: nonreactive, HCV RNA: not detectable) (The patient does not have hepatitis C, but has immunity to hepatitis B) This patient does not have hepatitis C (HCV) infection. An HCV antibody test (anti-HCV) is recommended as the initial screen for infection. However, development of detectable antibodies (anti-HCV) usually occurs between 2-6 months following exposure. Although it is negative, she was exposed less than 6 months ago and thus a confirmatory test (HCV RNA) is necessary. Since the HCV RNA is negative, she does not have hepatitis C. Typically, subsequent evaluation to detect the presence of HCV RNA is not necessary following a nonreactive anti-HCV result. Because exposure occurred less than 6 months ago, she may lack detectible levels of anti-HCV antibodies, which warrants testing for HCV RNA. HCV RNA levels become detectible before reactive antibodies. HCV RNA was not detected in this patient. This confirms that this patient has a true negative screen for infection with HCV. A positive hepatitis B surface antibody (anti-HBs) in the presence of a negative core antibody (anti-HBc) indicates immunity to hepatitis B from immunization. A 5-year-old female’s playmate has been diagnosed with pinworms. The mother brings her child in for an exam. The 5 year-old denies rectal itching. How should the NP proceed? (Perform the “scotch tape” test and look at the collection under the microscope) The diagnosis of pinworms, Enterobiasis, is made by using a piece of scotch tape on a tongue depressor. It is touched against the child’s rectum. The greatest yield of eggs will occur during the nighttime or early AM. Eggs will be found here if they are present. Worms and eggs are rarely found in stool specimens, so this is not a good plan. When the scotch tape is examined under a low-power microscope, the eggs will be easily visualized since they are large and bean shaped. The finding of an adult worm would confirm the diagnosis. These are large enough to be seen with the naked eye. A 24-year-old male has recently returned from a weekend camping trip with friends. He has ulcerative colitis and history of migraine headaches. He reports a 2-day history of headache, nausea, and vomiting with weakness. Which of the following is not part of the differential diagnosis? (Exacerbation of ulcerative colitis) The patient presents with headache, nausea and vomiting. His symptoms could be due to migraine headache or acute gastroenteritis. Norovirus is a common cause of gastroenteritis. An exacerbation of ulcerative colitis would produce lower GI symptoms (diarrhea, flatulence, or bleeding), not nausea, vomiting, and headache. A mother presents with her 1-month-old infant. She reports that he cries inconsolably every evening after his first evening feeding. She asks for help. What should be done? (Provide education, parental reassurance, and encouragement) This describes colic. Colic is a symptom complex characterized by episodes of inconsolable crying accompanied by apparent abdominal pain. It typically occurs between 1-3 months of age and usually in a very predictable pattern, typically in the evening after feeding. Many different approaches are tried, but medication like ranitidine is not indicated; changing formula is not indicated either. Parents need education regarding colic, comfort measures like rhythmic rocking or frequent burping, much reassurance, and encouragement. A 50-year-old with a history of consumption of 3-4 alcoholic drinks daily and weekend binges has elevated liver enzymes. Which set of enzymes is most representative of this patient? (AST= 200, ALT= 75) The normal AST/ALT ratio in healthy subjects is 0.8. In patients with alcoholic hepatitis, the usual ratio (AST:ALT) is 2:1. When the ALT is very elevated, infectious hepatitis must be considered. Normally, both AST and ALT are less than 40 IU/L. The level of elevation does not correlate with the degree of damage in the liver and has no prognostic value in patients with non-acute liver disease. A 26-year-old female presents with concerns about possible hepatitis C (HCV) infection. She admits to IV drug use 2 months ago and sharing needles with several other people. Initial laboratory studies have been completed. How should this be managed? (anti HCV: reactive) (Order HCV RNA) An HCV antibody test (anti-HCV) is recommended as the initial screen for infection. Development of detectable antibodies (anti-HCV) usually occurs between 2-6 months following exposure. The patient's HCV antibody test (anti-HCV) is reactive. This indicates presumptive HCV infection. Subsequent evaluation to detect the presence of HCV RNA is necessary following a reactive anti-HCV result to confirm or rule out current infection. An older adult has suspected vitamin B12 deficiency. Which of the following lab indices is more indicative of a vitamin B12 deficiency? (Macrocytosis) A vitamin B12 deficiency can produce an anemia called pernicious anemia. This is most commonly found in older adults and is characterized by macrocytosis. In other words, the red cells are larger than expected. Microcytosis may be seen in iron deficiency anemia or thalassemia. Leukocytosis refers to large numbers of white cells in the blood stream. Thrombocytosis refers to an increased number of platelets in the blood stream. Which term does not characterize hemorrhoids? (Carcinogenic) Hemorrhoids are vascular structures in the anal canal. The classic symptoms of hemorrhoidal disease are bleeding, itching, burning. They are not carcinogenic, nor are they found with greater prevalence in patients with colorectal cancer. They are of equal prevalence in men and women. The most common age is 45-65 years. Which description is more typical of a patient with acute cholecystitis? (The patient is ill-appearing and febrile) A patient with acute cholecystitis usually complains of abdominal pain in the upper right quadrant or epigastric area. Many patients complain of nausea. The patient lies very still on the exam table because cholecystitis is associated with peritoneal inflammation that is worse with movement. Older patients are more likely to NOT exhibit Murphy’s sign and thus are more likely to experience complications of acute cholecystitis because diagnosis is delayed. Patients who are asymptomatic have cholelithiasis, not acute cholecystitis. Which patient has the least worrisome symptoms associated with his diarrhea? One with: (moderate amounts of watery diarrhea) Diarrhea is extremely common. Evaluation of diarrhea should take place when specific criteria suggest severe illness. In addition to those listed, some conditions which indicate further work-up are: profuse watery diarrhea with signs of hypovolemia, passage of > 6 unformed stools per 24 hours or a duration of illness > 48 hours, recent antibiotic use or recent hospitalization, and diarrhea in a patient > 70 years old. A 26-year-old female complains of pain at McBurney’s point. She feels nauseated. Her vital signs are provided. The most appropriate initial action by the NP is to: (order a CBC and pregnancy test) Patients with appendicitis usually have pain at McBurney’s point, the painful area in the right lower quadrant of the abdomen. However, because this patient is of child bearing age, pregnancy is part of the differential and must be ruled out initially. Once pregnancy status is determined, patient disposition can be determined. If pregnancy is ruled out, then workup for appendicitis can proceed. CT scan of abdomen has very high sensitivity and specificity for appendicitis (95 and 94%, respectively) and so it is the gold standard for diagnosis of appendicitis. A 7-year-old male presents with encopresis. The NP might expect: (Constipation) The underlying cause of encopresis, repetitive soiling of stool by a child who is 4 years of age or older who should be potty trained, is usually chronic constipation. The ultimate goal is to reverse the constipation and establish normal bowel habits by the child. Having the patient use daily laxatives reverses constipation. Once he is able to have one soft bowel movement daily and a routine has been established, the laxatives are slowly weaned off. Attention to dietary factors must be addressed so that the child’s diet will support a daily bowel movement. A 79-year-old with an appendicitis is unlikely to exhibit: (initial WBC elevation) Very young children and elderly adults are not likely to have initial WBC elevations. Consequently, appendicitis can be easily missed in these populations. Generalized abdominal pain is typical initially. UTI symptoms in older adults can manifest as lower abdominal pain and are a common presentation in this age group. Low-grade fever is common too. An 85-year-old adult has chronic constipation. What is the most likely cause of her constipation? (Medication-related) While all of these choices can contribute to constipation in an 85-year-old, she is on multiple medications that can increase her risk of constipation. Amlodipine, a calcium channel blocker, slows down motility in the gut. Oxybutynin has anticholinergic properties, which dry up mucus in the gut. Naproxen, an NSAID, increases the likelihood of constipation by inhibiting prostaglandins in the gut. Proton pump inhibitors and calcium supplements are commonly associated with constipation. A patient with diarrhea is tested for C. difficile. How soon should the enzyme immunoassay (EIA) yield results? (About 24 hours) The enzyme immunoassay allows detection of Clostridium difficile toxin, not the organism. It is the most commonly used assay in the US because it is easy to perform, and yields results in less than 24 hours. The assay has good specificity, but moderate sensitivity. More sensitive tests can be performed, but they are more expensive and take longer to yield results. What is true regarding older adults who are overweight? (Mortality in older adults related to overweight states declines over time) Overweight and obese states are not as important in predicting mortality in older adults as they are in their younger counterparts. After age 65 years (some studies demonstrate after age 70), weight is less significant in decreasing risk for mortality than in younger adults. There are some benefits to weight loss in the obese older adults. One of them is better balance and decreased risk for falls. Others include less sleep apnea, decreased risk of diabetes, and decreased rates of shortness of breath with respiratory and cardiac diseases. The relationship between colon polyps and colon cancer is that polyps: (have a slow progression to colon cancer) Colon polyps are usually slow growing and take a long time to progress to cancer. This is the reason that a colonoscopy does not need to be repeated annually. While not all polyps grow slowly, this is the usual progression. An older patient presents with left lower quadrant pain. If diverticulitis is suspected, how should the NP proceed? (CT scan of abdomen) CT scan of the abdomen is the diagnostic test of choice for this patient with suspected diverticulitis. The CT scan is able to demonstrate inflammatory changes in the colonic wall, colonic diverticula, thickening of the bowel wall, fistula formation, peritonitis, and other complications associated with diverticulitis. A chest and abdominal X-rays are commonly ordered and can help exclude other causes of abdominal pain, but they do not help diagnose diverticulitis. Barium enema would be contraindicated if there were a potential for perforation. Ultrasound is much less widely used than CT. A patient is in the clinic with a 36-hour history of diarrhea and moderate dehydration. Interventions should include: (oral rehydration with an electrolyte replenishment solution) The goal in managing a patient who presents with dehydration is rehydration. This is typically done with a commercially prepared electrolyte solution. Infamously, these are poor tasting. Patients usually prefer to rehydrate with fluids like tea, cola or a sports drink. However, these usually contain too much carbohydrate, too little potassium, and too much sodium for ideal fluid replenishment. Consequently, these are avoided when rehydration is needed. These are preferred by patients because of their good taste. The oral tract is always preferred for rehydration when it can be used. Resumption of the usual fluid and solid food intake should occur AFTER rehydration has occurred. Children with an inguinal hernia: (have a history of an intermittent bulge in the groin) Inguinal hernias are usually asymptomatic and absent on exam but can sometimes be elicited by increasing intraabdominal pressure such as occurs with straining or crying. The “silk sign” is infrequently appreciated but represents a silky thickening of the cord. If it is able to be palpated, it is done by placing a single finger next to the inguinal canal at the level of the pubic tubercle and gently moving the finger from side to side. Children with an incarcerated mass are often irritable but not constipated. A 10-year-old female presents with a 3-month history of abdominal pain. She has been diagnosed with recurrent abdominal pain. During the interview the nurse practitioner is likely to elicit a finding of: (school absenteeism) Recurrent abdominal pain can be diagnosed after three episodes of abdominal pain that severely affects the child’s usual activities and occurs over at least a 3-month period. No acute cause can be identified. Fewer than one in 10 children with recurrent abdominal pain attends school regularly. The goal in treating these children is a return to normal function and activities, not necessarily relief of pain. Caregivers must be coached to avoid reinforcement of pain behaviors with the child. A patient has the following laboratory values. (HBsAG: positive, IgM anti-HBc: positive) What does this mean? (He has acute hepatitis B) A positive hepatitis B surface antigen and positive IgM means that this patient has acute hepatitis B. The first serologic marker to be positive is the surface antigen. It can become positive as soon as 3-4 weeks after exposure to hepatitis B. A positive IgM indicates acute infection. A patient asks for advice about a medication that will produce rapid relief if he is having heartburn symptoms. What should the nurse practitioner recommend? (Calcium carbonate) Antacids, like calcium carbonate, produce the most rapid change in gastric pH and thus, the most rapid relief of symptoms. However, the increase in pH lasts 20-30 minutes and so may provide only short-lived relief. H2 blockers, like ranitidine, and proton pump inhibitors, like omeprazole, may take many hours before relief is realized and so are not the best choices for immediate relief of symptoms. Sucralfate does not affect gastric pH or acid output. Instead, it forms a viscous, adhesive substance that adheres to the surface of gastric and esophageal ulcers. Which of the following would be usual in a patient with biliary colic? (Pain in upper abdomen in response to eating fatty foods) Biliary colic refers to discomfort produced by contraction of the gallbladder. This occurs in response to eating. Typically, pain occurs in the upper right quadrant or chest, peaks an hour after eating, and then remains constant and finally subsides over the next several hours. Biliary colic usually lasts at least 30 min, but less than 6 hours. An episode of acute cholecystitis usually lasts greater than 6 hours. A positive Murphy’s sign is elicited when the gallbladder wall is inflamed. It can be elicited by palpating the gallbladder just beneath the liver as the patient takes a deep breath. A fecal occult blood test (FOBT) obtained during a rectal examination: (is inadequate to screen for colorectal cancer) This is not adequate to screen for colorectal cancer. Fecal occult blood tests have a much higher sensitivity if three consecutive stool specimens are used (applying two samples per card for each specimen). A single specimen is inadequate for screening purposes. Since polyps do not usually bleed, the fecal occult blood test is not a good screen for polyp identification. A patient has a positive hepatitis B surface antibody. This means he: (is immune to hepatitis B) The hepatitis B surface antibody indicates immunity to hepatitis B virus. Specifically, if this patient comes in contact with hepatitis B virus, he will not become infected with hepatitis B. The presence of hepatitis B surface antibody indicates immunity from immunization or actual infection. It also indicates recovery if the patient was infected. The most common reason that older adults develop peptic ulcer disease is: (H. pylori infection) The most common reason that older adults have peptic ulcer disease is infection with H. pylori. There are many regimens approved to treat H. pylori and most are well tolerated. NSAID use is the second most common reason older patients have peptic ulcer disease. A 15-year-old is about 10% below her ideal body weight. Laboratory studies were performed. Which complaint might be common in this patient? (Dizziness with standing) This patient does not meet the strict criteria for an eating disorder, but it should be suspected. The other laboratory values are not the cause of her dizziness with standing. This is likely due to a low hemoglobin. She needs treatment for a probable iron deficiency anemia and elicitation of history to help identify the cause of her low hemoglobin. The three most common causes of bacterial diarrhea in the US are Salmonella, Campylobacter, and: (Shigella) Shigella will be shed continuously in the stool and should be easily identified on stool culture. When bacterial gastroenteritis is suspected, a stool specimen could be ordered for confirmation. Generally, these three pathogens are easily identified if they are present. Enterovirus produces a viral form of diarrhea. Yersinia produces the deadly disease called bubonic plague. E. coli is a typical colonic pathogen. Which choice contains three medications that should have liver function tests measured prior to initiation of the medications? (Terbinafine, atorvastatin, simvastatin) Patients who take terbinafine and statins should have liver enzymes measured prior to initiation. Periodic monitoring of liver enzymes with the statins is no longer required. However, baseline values are prudent. There is no need to do this routinely with aspirin, cimetidine, propanolol, or iron in patients without risk factors. More than 600 commonly prescribed drugs can produce liver enzyme elevations. Care with prescribing is always warranted. The most common symptoms associated with gastroesophageal reflux disease (GERD) are heartburn and: (regurgitation and dysphagia) The three most common symptoms of GERD are heartburn (especially postprandial), regurgitation, and dysphagia (especially after longstanding heartburn). Other common symptoms are chest pain, nausea, and odynophagia (painful swallowing). EENT A patient has two palpable, tender, left preauricular nodes that are about 0.5 cm in diameter. What condition might this be associated with? (Conjunctivitis) The eyes are drained partly by the preauricular lymph nodes. These nodes may be palpated anterior to the ear. They can enlarge in response to eye infections like conjunctivitis, allergies, or foreign bodies in the eye. A 3-year-old has fluid in the middle ear that does not appear infected. The eardrum appears normal. This is referred to as: (middle ear effusion) Middle ear effusion refers to the presence of fluid in the middle ear. Since the eardrum appears normal and the fluid does not appear infected, there is no reason to suspect acute otitis media or purulent. A cholesteatoma is an epithelial growth in the middle ear. A contact lens wearer presents with an erythematous right conjunctiva. He denies blurred vision. There is scant drainage and crusting around the right eyelashes. He reports that crusting was present when he woke up this morning. How should the exam begin? (His visual acuity should be measured in each eye) This patient’s symptoms indicate that he could have conjunctivitis. Assessment of patients with eye complaints should always begin with assessment of vision in each eye. This should be documented. A 2-month-old is diagnosed with thrush. An exam of this patient’s saliva demonstrates all except: (spores) The visualization of yeast, hyphae, and pseudohyphae in saliva usually indicates Candida species. The diagnosis of thrush is usually made on clinical presentation and there is no need for KOH. Spores are a form assumed by some bacteria and fungi. They are resistant to heat and consequently are difficult to kill. A 6-month-old infant has a disconjugate gaze. The nurse practitioner observes that the 6-month-old tilts his head when looking at objects in the room. Which statement is true? (The infant will have an abnormal cover/uncover test) The cover/uncover test is used to assess strabismus, a common cause of disconjugate gaze. Strabismus represents a nonparallelism of the visual axis of the eyes. This results in the inability of both eyes to focus on the same object at the same time. At 6 months of age, a disconjugate gaze and tilting of the child’s head is a red flag. This child needs referral to ophthalmology. While an ocular tumor could be present, this is unlikely and not the action that should be taken today. A patient presents to your clinic with a painless red eye. Her vision is normal, but her sclera has a blood red area. What is this termed? (Subconjunctival hemorrhage) This represents leakage of blood out of the ophthalmic vasculature. It is usually painless and can be the result of coughing, sneezing, hypertension, or trauma. This will resolve without treatment, but aspirin or other agents that can produce bleeding should be discontinued until the etiology is determined. A nurse practitioner performs a fundoscopic exam. He identifies small areas of dull, yellowish-white coloration in the retina. What might these be? (Cotton wool spots) These are cotton wool spots. They are due to swelling of the surface layer of the retina. Swelling occurs because of impaired blood flow to the retina. The most common causes of cotton wool spots are diabetes and high blood pressure. A microaneurysm is the earliest manifestation of a diabetic retinopathy. These appear as small, round, dark red dots on the retinal surface. Exudates are an accumulation of lipid and protein. These are typically bright, reflective white or cream-colored lesions seen on the retina. At what age would it be unusual to see thrush? (At birth) Thrush is an infection in the oral cavity caused by yeast. Yeast grow in a warm, dark, moist environment. It is not unusual to see thrush in young infants who are breast or bottle fed. It would be unusual to see thrush in a newborn. In fact, this should cause concern regarding an immunocompromised state in the infant or hyperglycemia in the mother. Epstein-Barr virus is responsible for: (mononucleosis) Infectious mononucleosis is caused by Epstein-Barr virus (EBV). This commonly affects adolescents but can affect various age groups. The most prominent features of mononucleosis are fever, fatigue, pharyngitis, and lymphadenopathy. The posterior cervical lymph nodes are most commonly involved. A patient has been diagnosed with mononucleosis. Which statement is correct? (Cervical lymphadenopathy may be prominent) Mononucleosis is a common viral infection in adolescents and people in their early 20s. Splenomegaly occurs in about 50% of patients with mononucleosis. While it is not common, it is possible to be coinfected with Streptococcus in the throat. If this is the case, treatment with penicillin should be avoided because of the possibility of an “ampicillin” rash. The most prominent symptoms are fever, fatigue, pharyngitis, and lymphadenopathy. A 32-year-old patient is a newly diagnosed diabetic. She has developed a sinus infection. Her symptoms have persisted for 10 days. Six weeks ago, she was treated with amoxicillin for an upper respiratory infection. It cleared without incident. What should be recommended today? (Prescribe amoxicillin-clavulanate today) Amoxicillin is not indicated when a beta lactamase-producing organism is suspected. It should be suspected because she took an antibiotic 6 weeks ago. Amoxicillin-clavulanate is a good choice because it covers beta lactamase producers. A bacterial cause can be assumed since she’s had symptoms for 10 days. A viral infection likely would have run its course by now. This patient is diabetic and may be having blood sugar elevations that facilitate growth of the causative organism of the sinus infection. A decongestant could be added depending on her blood pressure and personal history of using decongestants. An NP examines a screaming 2-year-old. A common finding is: (pink tympanic membranes) The tympanic membrane normally becomes pink and can rarely become red when a child is screaming or crying. This is probably due to flushing and hyperemia of the face that occurs with crying. A distorted or erythematous tympanic membrane with decreased mobility is suggestive of otitis media. An infant is brought to the nurse practitioner because his gaze is asymmetrical. Which finding indicates a need for referral to ophthalmology? (He has persistent strabismus) Strabismus may be completely normal in the first few months of life. Persistent strabismus at any age likely indicates eye muscle weakness, cranial nerve abnormalities or a number of other pediatric eye diseases. The infant with a normal red reflex probably does not have retinoblastoma or congenital cataracts, but both of these conditions can result in strabismus. This infant should be referred to an ophthalmologist for evaluation if he has persistent strabismus. Which statement about serous otitis media is correct? (This can be diagnosed with pneumatic otoscopy) Serous otitis media (SOM) is also called otitis media with effusion (OME) or "glue ear." OME occurs when there is fluid (noninfectious) in the middle ear. This prevents normal mobility of the tympanic membrane and creates a conductive hearing loss. Pneumatic otoscopy is the primary noninvasive diagnostic method because it has a high sensitivity and specificity. It may be present before otitis media develops, or it may follow resolution of otitis media. OME is far more common than otitis media and is not associated with systemic symptoms like fever. Acute otitis media (AOM) describes infected fluid in the middle ear. Which of the following symptoms is more indicative of a bacterial sinusitis than viral? (Worsening of symptoms after initial improvement) There are no specific signs or symptoms that can clearly differentiate viral from bacterial sinusitis, including discolored nasal discharge. Facial pressure is present in both viral and bacterial infections, but facial pain is more likely to be associated with bacterial infection. However, rhinosinusitis symptoms lasting greater than 10 days and purulent nasal discharge, unilateral facial pain or maxillary tooth pain, and worsening of symptoms after initial improvement are suggestive of bacterial infection. A patient stated that his ears felt stopped up. He pinched his nose and blew through it forcefully. The nurse practitioner diagnosed a ruptured left tympanic membrane. What would indicate this? (Bright red blood in the left external canal) This patient ruptured his tympanic membrane (TM) traumatically from excessive pressure when he pinched his nose and blew out through it at the same time. It is common to find bright red blood (not clear fluid), but not active bleeding, in the external canal of the affected ear. He may experience pain in the affected ear, but this alone would not be indicative of a ruptured TM. Hearing may be diminished in the affected ear but should not be absent. Patients usually describe hearing as muffled. Arcus senilis is described as: (normal in people > 50 years of age) Arcus senilis describes an arc or circle around the cornea that is common in older adults. The circle is due to deposition of lipids in the cornea, but is not necessarily due to hypercholesterolemia. However, when this is seen in young adults, it is termed arcus juvenilis and is often associated with lipid abnormalities. Copper deposits in the cornea may be associated with Kayser-Fleischer rings. These may be associated with Wilson's disease, a genetic disorder in which copper is deposited in the brain and liver. Loss of central vision is associated with macular degeneration. A patient reports a penicillin allergy. What question regarding the allergy should the nurse practitioner ask to determine whether a cephalosporin can be safely prescribed? (What kind of reaction did you have?) The most important question to ask the patient is “what kind of reaction did you have?" Unfortunately, many patients who report penicillin allergy are not actually penicillin allergic. About 2-10% of patients who are penicillin allergic have cephalosporin allergy too. Cephalosporins should never be prescribed for penicillin-allergic patients if they report hives or anaphylaxis after taking penicillin. A 61-year-old male presents with a 12-hour history of an extremely painful left red eye. The patient complains of blurred vision, haloes around lights, and vomiting. It began yesterday evening. On examination, the eye is red, tender and inflamed. The cornea is hazy and pupil reacts poorly to light. The most likely diagnosis in this patient is: (acute angle glaucoma) The clinical presentation of a patient with acute angle glaucoma is as this patient has presented, age greater than 60 years, eye pain, and blurred vision. Nausea and vomiting are common. Pain is usually present when the intraocular pressure rises rapidly. This produces conjunctival redness. Symptoms are more common in the evening when light levels diminish and mydriasis occurs. In chronic angle closure, pressures rise slowly and pain is usually absent. Both can produce blindness. A patient presents with severe toothache. She reports sensitivity to heat and cold. There is visible pus around the painful area. What is this termed? (Pulpitis) The predominant symptom of patients who exhibit pulpitis is pain especially elicited by thermal changes, cold and hot. The pain can become severe and patients are ill appearing. Pus may be seen around the gum area or may be restricted to the pulp cavity. Caries and gingivitis do not produce pus. Periodontitis is characterized by gingival inflammation and pain. Pus is not present in this disease. A periodontal abscess produces pain and pus, but the pus is usually only expressed after probing. A patient who is 65 years old states that she has “hay fever” and has had this since childhood. What agent could be safely used to help with rhinitis, sneezing, pruritis, and congestion? (Nasal steroid) A nasal steroid is considered the gold standard for improvement of all symptoms associated with allergic rhinitis (hay fever). Ipratropium helps with rhinitis only. An antihistamine helps all symptoms listed but is not as effective at relieving symptoms of congestion as a nasal steroid. A decongestant is extremely effective at relieving congestion, but no other symptoms listed. A common complaint in older patients who have cataracts is: (sensitivity to sunlight) Loss of peripheral vision and eye pain is typical in patients with glaucoma, not cataracts. Patients with cataracts may be at higher risk for falls because they have difficulty seeing, however, this is not a common complaint of patients who have cataracts. Pain is not associated with cataracts. A 20-year-old-patient presents with complaints of a sore throat and cough that began this morning. His oral temperature is 101.2 °F. He has the following laboratory results. What is his most likely diagnosis? (Viral pharyngitis) The patient's CBC demonstrates a viral infection, not bacterial. Therefore, Streptococcal infection is an unlikely etiology with a negative rapid strep test. Mononucleosis is a possibility and it cannot be ruled out this early in the course of the illness, even with a negative Mono Spot. However, the "most likely diagnosis" is one of viral etiology. Swimmer’s ear is diagnosed in a patient who has right-sided tragal tenderness. What other symptom might he have? (Otic itching) Swimmer’s ear is termed otitis externa (OE). It is an infection of the external canal. This is characterized by tragal tenderness (pain with light touch of the tragus on the affected side). Fever does not occur because this is a superficial infection. OE is treated with a combination of topical agents: an antibiotic and steroid placed in the external canal. A patient who presents with a complaint of sudden decreased visual acuity has a pupil that is about 4 mm, fixed. The affected eye is red. What might be the etiology? (Glaucoma) This patient needs urgent referral to ophthalmology. While this is a relatively unusual patient in primary care, the primary care clinician must be able to recognize this patient and the need for urgent referral. In a patient with acute angle closure glaucoma, the patient is usually ill appearing and may have nausea and vomiting. This scenario should prompt urgent referral. On routine exam, a 15-year-old patient’s tympanic membrane (TM) reveals a tiny white oblong mark just inferior to the umbo on the surface of the TM. The patient has no complaints of ear pain and gross hearing is intact. What is this? (Scarring of the tympanic membrane) A white, chalky mark on the surface of the TM reflects scarring of the tympanic membrane (TM). This can occur secondary to TM rupture or tympanostomy tube placement. The normal color of the TM is pink or pearly gray, so this is not a variant of normal. A cholesteatoma is an abnormal growth found in the middle ear or mastoid, not on the surface of the TM. Foreign bodies typically reside in the external canal. A patient with mononucleosis would most likely have: (lymphocytosis) Mononucleosis (mono) is a viral infection. This is usually characterized by a predominance of lymphocytes. Eosinophilia is typical in parasitic infections and allergic reactions. Leukocytosis is a predominance of white cells but is not specific for mono. Monocytes can rise in mono, but their presence is not specific to mono. A patient with a bacterial sinusitis cannot spread this to others via: (urine or stool) Bacterial infections of the upper respiratory tract can be transmitted by direct contact with fomites, secretions, or by respiratory droplet. Fomites are inanimate objects where bacterial or viral particles live and are easily transmitted to others who touch the fomite. A doorknob is a common example. Infectious particles remain pathogenic for varying lengths of time depending on the organism, environment, and the fomite. Bacterial and viral particles are denatured once present in the digestive system and are no longer able to produce upper respiratory infection via stool or urine. A patient with allergic rhinitis developed a sinus infection 10 days ago. He takes fexofenadine daily. What should be done with the fexofenadine? (Continue the fexofenadine and prescribe an antibiotic) This patient should continue his fexofenadine. This treats his allergies and although he has a sinus infection, he still needs treatment for his allergies. A topical nasal steroid can be added if poor control of allergies exists, otherwise, this probably just increases the cost of treatment of during this sinus infection. If his sinus infection has been present for 10 days, an antibiotic seems prudent at this point. The nurse practitioner performs a fundoscopic exam on a patient who has recently been diagnosed with hypertension. What is the significance of AV nicking? (This is indicative of long standing hypertension) AV (arteriovenous) nicking can be observed as arteries cross veins when the arteries have narrowed secondary to hypertension. Generally, AV nicking takes time to develop and would be expected in patients with longstanding hypertension; especially when it is poorly controlled. Normally, veins are larger than arteries in the eyes. The vessels in the eyes are particularly susceptible to increased blood pressure. In severe hypertension, the retina can become detached. Which long-acting antihistamine listed below is sedating? (Cetirizine) Cetirizine (Zyrtec) is NOT non-sedating. In older adults, this medication should be avoided due to the sedative effect of cetirizine. In other age groups, it should be dosed at nighttime to minimize the initial sedative action. Fexofenadine is the least sedating of the oral agents listed. The hearing loss associated with aging involves: (sensorineural hearing loss) Hearing loss associated with aging is termed presbycusis and is a form of sensorineural hearing loss. This can be influenced by a number of factors, including heredity. Conductive hearing loss involves the external canal and the middle ear, preventing sound from traveling beyond the middle ear. The 8th cranial nerve and the inner ear are involved in sensorineural hearing loss. Noise damage can produce a sensorineural hearing loss. This usually occurs over time but is not necessarily associated with aging. A patient with diarrhea has a positive enzyme immunoassay for C. difficile. He is on clindamycin for a tooth abscess. How should he be managed? (Stop the clindamycin if possible, give metronidazole) The most important step in treating infection with C. difficile is stopping ingestion of the offending antibiotic. In this case, stopping the clindamycin, if possible, is the most important part of treatment. Metronidazole is recommended initially for nonsevere infection. If the antibiotic cannot be stopped, treatment for C. difficile should be continued as long as the patient must take the offending antibiotic. A patient has a penicillin allergy. He describes an anaphylactic reaction. Which medication class should be specifically avoided in him? (Cephalosporins) This patient should never have a cephalosporin prescribed for him because of the risk of cross-reactivity between the penicillin and cephalosporin classes. This could potentially give rise to another anaphylactic reaction to the cephalosporin prescribed. A good rule to follow if a patient has had an anaphylactic reaction to a penicillin is to NEVER prescribe a cephalosporin. Although the risk is small, it should not be taken. A 12-year-old complains of itching in his right ear and pain when the pinna is pulled or the tragus is pushed. Examination revealed slight redness in the ear canal with a clear odorless fluid. This could be suggestive of: (otitis externa) Otitis externa, swimmer's ear, is an infection or inflammation of the external ear or the ear canal. Symptoms include itching in the ear with an increase in pain when the pinna is pulled or the tragus is pushed. Slight redness appears in the ear canal, along with a clear odorless fluid. Otitis media is a middle ear infection and usually the tympanic membrane is bulging with fluid or pus behind it. Mastoiditis is an infection of the mastoid process (temporal bone adjacent to the middle ear) and generally results from inadequately treated otitis media. A ruptured tympanic membrane occurs more often in children. The infection causes pus or fluid to build up behind the eardrum and as the pressure increases, the eardrum may rupture. Ear pain decreases when the membrane ruptures and the discharge can be pus, bloody, or clear. A 3-year-old has been recently treated for an upper respiratory infection (URI) but drainage from the right nostril persists. What should the NP suspect? (Presence of a foreign body) Two clinical clues should make the examiner suspect a foreign body. First, the patient has continued drainage despite treatment. Second, the drainage is unilateral. Unilateral drainage from a nostril should prompt the examiner to visualize the turbinates. In this case, a foreign body could probably be visualized. What medication should always be avoided in patients with mononucleosis? (Amoxicillin) A generalized rash may be seen in patients with mononucleosis (mono) who are given amoxicillin or ampicillin at the time of the acute phase of the illness. The rash does not represent an allergic reaction, but instead probably represents a reaction between the Epstein Barr virus and the penicillin molecule. The rash is usually described as maculopapular and may be pruritic. The rash has also been described with other beta-lactam antibiotics, azithromycin, cephalexin and levofloxacin. At what age should oral health risk assessment begin? (6 months) Examination of the mouth may begin at birth, but oral health risk assessment should begin at 6 months of age. Part of the screening should be for the need for fluoride supplementation. Oral health risk assessment should take place at 6 months, and 9 months, and referral to a dental home should take place by 1 year of age. Oral health risk assessment should continue periodically at health screening visits at 18, 24, and every 6 months until a dental home is established. A 45-year-old patient describes a spinning sensation that has occurred intermittently for the past 24 hours. It is precipitated by position changes like rolling over in bed. During these episodes, he complains of intense nausea. Which choice best describes benign paroxysmal positional vertigo? (Symptoms precipitated by a position change) Vertigo is a symptom, not a disease. It may have either a peripheral or central (brainstem or cerebellum) etiology. The most common form of peripheral vertigo is benign paroxysmal positional vertigo (BPPV). It is usually due to calcium debris in the ear's semicircular canals. Symptoms can be reproduced by a position change and are usually assessed using the Dix-Hallpike maneuver. It is characterized by the sensation of moving, having objects around the patient move, or a tilting/swaying sensation. Spinning sensation is a typical description of a patient with BPPV. During acute attacks of vertigo, regardless of the etiology, nausea, vomiting and nystagmus are common. Attacks can be transient and last for days to weeks. Which of the following will decrease the risk of acute otitis media in a 6-month-old? (Breastfeeding) Breastfeeding is considered a negative risk factor for acute otitis media because it decreases the risk of otitis media. Exposure to cigarette smoke and sucking on pacifiers increases the risk of acute otitis media. It is unknown whether vitamin D supplementation increases or decreases the risk. Acute otitis media can be diagnosed by identifying which otic characteristic(s)? (Cloudy, bulging TM with impaired mobility) The best predictor of acute otitis media (AOM) is a cloudy, bulging tympanic membrane (TM) with impaired mobility. Decreased mobility of the TM can be a result of fluid behind the TM. This is known as a middle ear effusion (MEE). MEE is characterized by the presence of middle ear fluid (bubbles or an air fluid interface) or finding of TM abnormalities (opacity, impaired mobility, or color change). Redness of the TM alone does not constitute infection. The other finding that constitutes a diagnosis of AOM is the finding of acute, purulent otorrhea that is not due to otitis externa. This describes a ruptured TM from otitis media. A 58-year-old farmer presents with a wedge-shaped, pinkish, clear growth on the nasal side of his eye. He states that it has been present for a while, but only recently began to feel as if a foreign body was in his eye. This is probably a: (pterygium) Pterygia can occur in children, but it is more prevalent in older adults and is associated with chronic sun exposure. It is a benign growth of fibrovascular conjunctival tissue that usually appears on the nasal side first and extends laterally toward the iris. Although it is often initially asymptomatic, it can cause irritation and even visual impairment as it extends onto the cornea toward the pupil. A stye or hordeolum is a painful, self-limiting infection of a gland at the eyelid margin. Xanthelasma are typically associated with hyperlipidemia and appear as soft, yellow plaques on the medial aspect of the eyelids. A pinguecula is a benign, yellow, triangular nodule that does not affect vision. A 4-year-old child with otitis media with effusion: (probably has just had acute otitis media) Otitis media with effusion (OME) frequently precedes or follows an episode of acute otitis media. This condition should not be treated with an antibiotic since the middle ear fluid is not infected. However, the fluid acts as a medium for bacterial growth. This fluid may be present for months after an episode of acute otitis media. A patient diagnosed with Strep throat received a prescription for azithromycin. She has not improved in 48 hours. What course of action is acceptable? (A penicillin or cephalosporin with beta lactamase coverage should be considered) The patient should demonstrate improvement after 48 hours if an antibiotic with the appropriate antimicrobial spectra was prescribed. A macrolide would be a poor choice because there are high rates of Strep resistance to macrolide antibiotics. In light of this, strong consideration should be given to an antibiotic with different antimicrobial spectra. Since Strep was diagnosed and azithromycin was ineffective, the prescriber should consider that the causative agent has macrolide resistance and could be beta lactamase producing. An antibiotic with beta lactamase coverage should be considered. A penicillin or cephalosporin with beta lactamase provides this coverage. A 70-year-old presents urgently to the nurse practitioner clinic with angioedema. This began less than an hour ago. He is breathing without difficulty. What medication may have caused this? (Fosinopril) Angioedema is common in African American patients who take ACE inhibitors such as fosinopril. It is an unpredictable event but once it occurs, the culprit medication must be discontinued and never prescribed again. This reaction has occurred with many medications, but ACE inhibitors are classic culprits. Swelling that affects the lips, face, eyelids, tongue, and larynx characterizes angioedema. Not all reactions involve this severe a reaction, but any impairment in airway must be referred to the nearest emergency department. A 70-year-old patient has begun to have hearing loss. She relates that her elderly parents had difficulty hearing. Which complaint below is typical of presbycusis? (Inability to hear consonants) Presbycusis is age-related hearing loss. The significance of this patient’s parental hearing loss is important for history. Presbycusis is influenced by genetics as well as noise exposure, medications, and infections. Loss of ability to hear speech in crowded rooms or noisy areas, inability to understand consonants, and loss of high-pitched sounds is typical. Hearing loss is symmetrical. Asymmetrical hearing loss is a red flag, regardless of the age at which it occurs. Tinnitus is common and is an annoying sensation associated with presbycusis. A pulsatile noise in the ear raises suspicion of a tumor or arteriovenous malformation. A 6-day-old has bilateral mucopurulent eye discharge. Which historical finding explains the etiology of the discharge? (Mother has chlamydia) Infants born vaginally to mothers who have chlamydia have a 60-70% risk of acquiring C. trachomatis. Newborns may present with pneumonia and/or conjunctivitis. The most common clinical feature is conjunctivitis that occurs 5 to 14 days after delivery. It is characterized by swelling of the lids and a watery discharge that becomes mucopurulent. The conjunctivae are erythematous. This must be treated orally because topical treatment is not effective. The drug of choice in infants is oral erythromycin 50 mg/kg/day in divided doses for 14 days, whether treating pneumonia or conjunctivitis. Group A Strep pharyngitis: (can be accompanied by abdominal pain) Group A Streptococcus is usually characterized by multiple symptoms with an abrupt onset. Sore throat is usually accompanied by fever and headache. GI symptoms are common too; nausea, vomiting and abdominal pain are usual. Even without treatment, symptoms usually resolve in 3-5 days. A 14-year-old was diagnosed and treated for left acute otitis media 4 weeks ago. She presents today for a follow-up visit. There is an effusion in the left ear. She denies complaints. How should this be managed? (This should be monitored) About 40% of children have effusion 4 weeks after acute otitis media. This should be monitored and not treated with another antibiotic. Effusion is a stage in the resolution of otitis media. Pneumatic otoscopy will identify the presence of fluid or pus behind the TM, but it will not help in diagnosis or treatment once an effusion has been established. A tympanogram will establish that hearing is diminished, a fact that should be assumed since fluid is present in the middle ear. The patient presents with complaints of morning eyelash crusting and itchy red eyes. It began on the left and now has become bilateral. Based on the most likely diagnosis, what should the nurse practitioner tell the caregivers about this condition? (This usually begins as a viral infection) This image is consistent with conjunctivitis. Conjunctivitis or “pink eye” usually begins as a viral infection. As the conjunctiva becomes irritated, the eye is rubbed and fingers introduce bacteria. A secondary bacterial infection develops. Conjunctivitis produces a red (or pink) eye, but should never produce blurred vision. A patient with a red eye and blurred vision should be referred to ophthalmology. The preauricular nodes may be palpable when a patient has conjunctivitis; the anterior cervical nodes will not be. Pain is not common in conjunctivitis, but usually occurs with acute closed angle glaucoma. A patient presents with tragal pain. What is the most likely diagnosis? (Otitis externa) Otitis externa is “swimmer’s ear.” It is characterized by tragal tenderness. Otitis externa is an infection of the external canal. When the tragus is tender, it will be difficult to insert a speculum to examine the ear. A medication considered first line for a patient with allergic rhinitis is a: (topical nasal steroid) Allergy and asthma guidelines in the US recommend topical nasal steroids first line for management of symptoms of allergic rhinitis. A nonsedating antihistamine can be added to manage unresolved symptoms after a nasal steroid has been initiated. Antihistamines work well when the predominant symptoms are thin, clear nasal discharge. These can be safely used in combination for management. Decongestants are not recommended as lone agents because they have no effect on the underlying allergic mechanisms. They work well in combination with antihistamines and nasal steroids for congestion. Sedating antihistamines are usually avoided for allergic rhinitis because of safety concerns. A 17-year-old has a complaint of ear pain. If he has otitis externa, which complaint is most likely? (Tragal pain) A patient with otitis externa has swimmer’s ear, an infection of the external canal. The classic complaint is tragal pain or even pinnae pain. When significant edema exists in the external canal, hearing may be impaired, but the most common complaint is tragal pain. Systemic complaints do not accompany swimmer’s ear unless a second diagnosis is present simultaneously. Fever and upper respiratory infection are not likely. Which of the following is most likely observed in a patient with allergic rhinitis? (Exacerbation of symptoms after exposure to an allergen) Allergic rhinitis is usually diagnosed on clinical presentation and history. The diagnosis is appropriately made when allergic rhinitis symptoms are reproducible after exposure to the suspected allergen, like pollen. Nasal congestion, sneezing, postnasal drip and sore throat are not exclusive to allergic rhinitis. Finally, sinusitis does exacerbate allergic rhinitis symptoms. What is the usual age for vision screening in young children? (3 years) Initial vision screening should take place at 3 years of age. If the child is not cooperative, screening should be attempted 6 months later. If the child is still not cooperative at 3.5 years, it should be attempted at 4 years. Generally, children are cooperative at 4 years of age. The usual vision of a 3-year- old is 20/50. In a patient with mononucleosis, which laboratory abnormality is most common? (Lymphocytosis and atypical lymphocytes) Lymphocytosis, a predominance of lymphocytes, is the most common laboratory abnormality seen with infectious mononucleosis (mono). Atypical lymphocytes are a common finding too. An elevation in monocytes is often found, but it does not occur with as high frequency as lymphocytosis. The total white count often is increased and may lie between 12,000-18,000/microL. Elevated liver enzymes, ALT and AST, are noted in the majority of patients but is a benign finding. These usually return to baseline within several weeks of onset of acute symptoms. A 2-year-old has a sudden onset of high fever while at daycare. The daycare attendant describes a seizure in the child. The child is brought to the clinic; neurologically he appears normal. His body temperature is 99.9° F after receiving ibuprofen. He is diagnosed with otitis media. How should the nurse practitioner manage this? (Treat the otitis media and give education about fever management) The child may have had a febrile seizure at the daycare related to a sudden elevation of body temperature. The sudden rise (or even fall) of body temperature can precipitate a seizure in young children. The most common diagnosis associated with febrile seizures is otitis media. The mother should be advised about behavior to watch for that could indicate the child is having a seizure. If this behavior occurs again, the child should be brought for neurological evaluation. Information should be provided to the caregiver regarding management of elevated body temperature in the child. A tympanic membrane (TM) is erythematous. Which factor listed below is NOT the cause of an erythematous TM? (Coughing) Coughing does not produce an erythematous TM. The tympanic membrane (TM) can take on numerous colors depending on the condition or status of the patient. Under normal conditions, the TM is usually described as pearly gray or pink. When there is fluid behind the TM, it may take on a white, gray, or blue appearance. When pus is present behind the TM, it can appear white or yellow. An 80-year-old is having difficulty hearing. When the nurse practitioner examines him, she is unable to visualize the tympanic membrane because of cerumen impaction. This produces what kind of hearing loss? (Conductive) This is a conductive hearing loss provided he is able to hear when the cerumen is removed. Anything that inhibits the ability of sound to enter the external canal and middle ear will produce a conductive hearing loss. Sensorineural hearing loss can be produced by aging, Meniere’s disease, noise trauma, or cranial nerve VIII pathology. A 4-month-old infant has thrush. The mother is breastfeeding. She reports that her nipples have become red, irritated, and sensitive. What should the nurse practitioner advise the mother of this baby to treat thrush? (Treat the infant with an oral antifungal suspension and the mother’s nipples with a topical antifungal agent) If the infant has thrush, he should be treated with an oral antifungal suspension like nystatin. This is given four times daily after feedings. Since the mouth of the infant is in contact with the mother’s nipples during breastfeeding, and they appear infected too, the mother and infant should be treated simultaneously. Care should be given so that the mother gently washes her nipples and dries them before breastfeeding. This will minimize or eliminate ingestion of the topical antifungal in the infant. An older adult has cerumen impaction in both ears. His hearing is diminished. This type of hearing loss is: (conductive) A conductive hearing loss is one in which sound cannot enter the external canal or the middle ear. This is produced when fluid, cerumen or a foreign body prevents sound from entering the ear. A sensorineural hearing loss involves the inner ear or 8th cranial nerve. Presbycusis is the term used to describe hearing loss associated with aging. Hearing loss associated with presbycusis is usually more significant in the 6th decade. Cholesteatoma is a middle ear tumor. What symptom tetrad is most commonly associated with infectious mononucleosis? (Fatigue, fever, lymphadenopathy, pharyngitis) The tetrad includes fatigue, fever, pharyngitis, and lymphadenopathy (posterior cervical lymph nodes are most common). Approximately 50% of patients with mono have splenomegaly. Body aches are probably the effect of fever, but they do not characterize the disease. The etiologic agent of mononucleosis is the Epstein Barr virus. It is often spread by intimate contact between susceptible contacts. It is spread via saliva and has been called “the kissing disease.” A patient presents to clinic with a complaint of a red eye. Which assessment below rules out the most worrisome diagnoses? (Usual visual acuity) Visual acuity is a test that should be done on every patient who presents with an eye complaint, especially if the eye is red. It is not necessary to determine exactly what the visual acuity is; it is necessary to establish that vision is usual. If this is the case, the most worrisome diagnoses can be ruled out: infectious keratitis, iritis, and angle closure glaucoma. A rapid strep test was negative was negative in a 12-year-old female with tonsillar exudate, fever, and sore throat. Which statement is true regarding this? (A throat swab should be collected and sent to microbiology) An additional throat swab is sent to microbiology for culture if the rapid strep test is negative. The sensitivity varies in rapid Strep tests performed in the clinic setting. Some are as low as 50% and if negative then an additional throat swab should be collected. If beta-hemolytic Strep organisms are present, then the patient can be diagnosed with Streptococcal infection. A patient with environmental allergies presents to your clinic. She takes an oral antihistamine every 24 hours. What is the most effective single maintenance medication for allergic rhinitis? (Intranasal glucocorticoids) These agents are particularly effective in the treatment of nasal congestion and would be a good choice for the patient in this scenario. Intranasal glucocorticoids are effective in relieving nasal congestion, discharge, itching, and sneezing. A trial of stopping the oral antihistamine could be tried in this patient. Symptoms would determine whether the antihistamine should be resumed. A patient has nasal septal erosion with minor, continuous bleeding. There is macerated tissue. What is a likely etiology? (Cocaine abuse) The nasal septum separates the right from left nostrils. It is made of thick cartilage and is covered with mucous membrane. It can be injured by foreign substances that contact it, like cocaine. A nasal septal erosion or perforation should always be assumed to have been from sniffing toxic substances in the nose, not nasal steroids. A patient has been taking amoxicillin for 8 days for sore throat. Today, the patient has developed a pruritic full body rash and is diagnosed with penicillin allergy. What describes the skin manifestations of penicillin allergy? (There will be hives) The usual skin manifestation associated with an allergic reaction is hives. It is urticarial and of rapid onset. Hives are intensely pruritic, well circumscribed, raised, and erythematous. Penicillin is known to be allergenic and should be stopped immediately in these circumstances. An antihistamine should be administered. A patient has been diagnosed with acute rhinosinusitis. Symptoms began 3 days ago. Based on the most likely etiology, how should this patient be managed? (Decongestant and analgesic) The vast majority of patients who have acute rhinosinusitis have a viral infection. When bacteria are the causative agents, Streptococcus and Staphylococcus are common pathogens. Since the most likely pathogen is a virus, symptomatic treatment should occur unless a red flag such as fever, facial pain, purulent drainage, etc. is present. Typically, conservative measures should be used for 10 days prior to antibiotic use. In clinical practice, patients typically request antibiotics earlier than 10 days. An otherwise healthy 6-year-old male has been diagnosed with otitis media. His mother reports that he has not had an ear infection since he was 3 years old. How long should he be treated with an antibiotic? (5-7 days) The recommendations from the American Academy of Pediatrics are 5-7 days of antibiotic therapy for children 2 years or older who have mild to moderate acute otitis media (AOM). Children younger than 2 years of age should be treated for 10 days. Children 2 years and older may be treated for 5-7 days for AOM if they do not have a history of recurrent AOM. The single most effective maintenance therapy for allergic rhinitis is: (a topical nasal steroid) Many studies have shown that topical nasal steroids like budesonide, fluticasone, and mometasone provide relief of nasal stuffiness, nasal discharge, sneezing, and postnasal drip that is superior to antihistamines. Decongestants treat symptoms associated with nasal stuffiness. Currently, topical nasal steroids are the treatment of choice for relief of symptoms associated with allergic rhinitis (AR). Antihistamines and decongestants can be added to the regimen of a patient with AR. Nasal decongestant sprays are not recommended as monotherapy in the management of chronic allergic rhinitis. Use greater than 3-7 days may lead to downregulation of the alpha-adrenergic receptor, resulting in rebound nasal congestion. A 30-year-old male has been diagnosed with nonallergic rhinitis. Which finding is more likely in nonallergic rhinitis than allergic rhinitis? (Older age of symptom onset) Nonallergic rhinitis, often called vasomotor rhinitis, is common in the US. It is typically diagnosed and differentiated from allergic rhinitis by history. Although both conditions may coexist in patients, nonallergic rhinitis typically has onset after age 20 years. Allergic rhinitis typically presents prior to age 20 years. The most common symptoms associated with nonallergic rhinitis are nasal congestion and postnasal drip. It is predominantly reported in females. Common precipitants of nonallergic rhinitis symptoms can occur with exposure to spicy foods, cigarette smoke, strong odors, perfumes, and alcohol consumption. This is frequently treated with topical azelastine. A 70-year-old female states that she sees objects better by looking at them with her peripheral vision. She is examined and found to have a loss of central vision, normal peripheral vision, and a normal lens. This best characterizes: (macular degeneration) Macular degeneration presents most commonly with a loss of central vision. The macula is the central part of the retina. As it degenerates, central vision is lost. Questions should be asked about the rate of loss of vision. Reports of rapid vision loss require urgent ophthalmologic evaluation. Known risk factors are age greater than 50 years (greatest prevalence older than age 65), smoking, family history, and history of stroke, MI, or angina. In a patient who is diagnosed with mastoiditis, which of the following is most likely? (Displaced pinna) Mastoiditis is an infection of the mastoid process. The mastoid process is a honeycomb-like structure with air pockets. These become infected with Streptococcus or H. flu most commonly. It is seen in patients (usually less than age 6 years) with chronic otitis media or, less frequently, in adults with chronic tooth abscesses. Patients may present with recent history of acute otitis media, history of abscess in the teeth and jaw, fever, and a displaced and erythematous pinna or postauricular area. The tympanic membrane will usually be red and the patient can become ill very quickly. Nuchal rigidity is the term used to describe a stiff neck associated with meningitis. A 70-year-old patient in good health has a large, white plaque on the oral mucosa of the inner cheek. There is no pain associated with this. What is a likely diagnosis? (Leukoplakia) The etiology of this white plaque is unclear from the given information, but it cannot be cheilitis. This affects the lips. It cannot be an aphthous ulcer, because this is painful. Sjögren's syndrome does involve the mucous membranes but manifests itself as dry mouth, not a plaque or lesion. The differential diagnosis for a white oral plaque should include oral leukoplakia, a premalignant lesion. This is often related to human papillomavirus. Risk factors include smokeless tobacco. Others in the differential include oral hairy leukoplakia (seen almost exclusively in patients with HIV), squamous cell carcinoma, and malignant melanoma. It may also be a completely benign growth, but this can only be established after biopsy. A 39-year-old has a sudden onset of a painful right red eye. He reports sensitivity to light and the sensation of a foreign body, though his history for a foreign body is negative. He does not wear contact lenses. How should the NP manage this? (Refer to ophthalmology) While no clear diagnosis can be made from this scenario, there are several red flags. Collectively, the red flags necessitate referral to ophthalmology. First, the eye is red and painful. This patient is photophobic and has the sensation of a foreign body. There is no mention of eye discharge, but eye discharge with this scenario would cause the examiner to consider bacterial conjunctivitis or keratitis. The symptoms of photophobia and foreign body sensation are symptoms of an active corneal process. Glaucoma should also be considered in the differential. He should be referred to ophthalmology. How should the class effect of the nasal steroids be described? (There are no significant systemic effects with these) One reason nasal steroids are preferred agents in older adults (and young children) is that there are few systemic effects. The steroids are absorbed across the mucous membranes and are deposited in the area where they need to work. There is absolutely no sedation associated with their use. They are generally well-tolerated. The class is predictable. There is very little variation between agents. The most common complication of influenza is: (bacterial pneumonia) Pneumonia is the most common complication of influenza; bacterial pneumonia is the most common form. Streptococcus pneumoniae is the most common bacterial pathogen. 25% of deaths associated with influenza are related to pneumonia. Clinical presentation of pneumonia as a complication of influenza is characterized by worsening of symptoms after an initial period of improvement for 1-3 days. Fever, cough, and purulent sputum predominate. Cough is a symptom of influenza, not a complication. Bronchitis might be part of the differential of influenza, however, fever is uncommon in bronchitis. An older adult has a common cold. She calls your office to ask for advice for an agent to help her runny nose and congestion. What agent is safe to use? (Guaifenesin) This patient has hypertension and pseudoephedrine will increase her blood pressure. Oxymetazoline can be absorbed across mucous membranes and elevate blood pressure too. Diphenhydramine is a sedating antihistamine with anticholinergic properties. This would be contraindicated with glaucoma and in most older adults. Guaifenesin would be the safest agent to use. A 4-year-old was diagnosed and treated for acute otitis media in the left ear 4 weeks ago. She is here today for a well-child visit. There is an effusion in the left ear. She denies complaints. How should this be managed? (This should be monitored) About 40% of children have effusion at 4 weeks postacute otitis media. This should be monitored and not treated with another antibiotic. Effusion is a stage in the resolution of otitis media. Pneumatic otoscopy will identify the presence of fluid or pus behind the tympanic membrane (TM), but it will not help in diagnosis or treatment once an effusion has been established. A tympanogram will establish that her hearing is diminished, a fact that should be assumed since fluid is present in the middle ear. When does a child’s vision approximate 20/20? (5-6 years) A child’s vision should be screened beginning at age 3 years if he is cooperative. The vision of a 3-year- old should be about 20/50. A 4-year-old’s vision is usually 20/40. By 5 years of age, vision is usually 20/30. By 6 years of age, a child’s vision should be approximately normal, 20/20. A patient is diagnosed with thrush. What might be found on microscopic exam? (Budding yeasts, pseudohypha) The visualization of yeasts and/or pseudohypha in saliva indicates a fungal infection, often Candida species. Budding is a process by which yeasts reproduce. A 3-year-old has been diagnosed with acute otitis media. She is penicillin allergic (Type 1 hypersensitivity reaction). How should she be managed? (Clarithromycin) This patient experienced a Type I allergic reaction to penicillin. This is characterized by hives, wheezing, or anaphylaxis. It is NEVER considered safe to prescribe a cephalosporin like cefdinir. Macrolides, like clarithromycin, may be prescribed to patients with a true Type 1 reaction to penicillin. Since amoxicillin is a penicillin, it should not be prescribed. On examination of the tympanic membrane (TM), a cloudy, red, bulging ear drum with impaired mobility is detected. This is consistent with: (acute purulent otitis media) The best predictor of acute otitis media (AOM) is a cloudy, bulging TM with impaired mobility. Decreased mobility of the TM can be a result of fluid behind the TM. This is known as a middle ear effusion (MEE). MEE is characterized by the presence of middle ear fluid (bubbles or an air fluid interface) or finding of TM abnormalities (opacity, impaired mobility, or color change). Redness of the TM alone does not constitute infection. In acute otitis externa, the canal is swollen, narrow, moist and pale with tenderness on touching and the drum is intact. In chronic otitis externa, the skin of the canal is thickened, red, and itchy, and the drum is usually unaffected. With serous effusion, the drum appears amber and there usually is not a bulge. A patient with mononucleosis has pharyngitis, fever, and lymphadenopathy. His symptoms started 3 days ago. What is a likely finding in this patient? (He could have a negative Monospot) The “Monospot” detects the presence of heterophile antibodies in mononucleosis (mono). If the Monospot is performed too early in the course of the illness, it will be negative even though the patient has mono. If the patient has persistent symptoms suspicious of mono, a Monospot should be repeated. It is likely that several days after a negative result, a positive result will be obtained. Lymphocytosis characterizes mononucleosis; therefore, it is highly unlikely that a patient will not have a normal CBC if he has mono. A patient presents to a nurse practitioner clinic with paroxysmal sneezing, clear rhinorrhea, nasal congestion, and facial pain. Which symptom below is NOT associated with allergic rhinitis? (Facial pain) Facial pain is not associated with allergic rhinitis. In conjunction with nasal congestion, it is most likely a sinus infection. Patients with allergic rhinitis and nasal congestion are more likely to develop acute and chronic bacterial sinusitis because untreated allergic rhinitis results in impaired mucus flow. This increases the risk of infection. Symptoms of bacterial sinusitis include nasal congestion, purulent postnasal drip or rhinorrhea, facial pain and maxillary tooth pain. Bacterial sinusitis may be suspected if symptoms have been present for more than 10 days, however, no symptom can differentiate bacterial from viral sinusitis. What clinical finding necessitates an urgent referral of the patient to an emergency department? (A fiery red epiglottis) A finding of a fiery red epiglottis signals epiglottitis. Since airway obstruction can be rapid with epiglottitis, immediate referral to an emergency department is warranted. Sudden onset of hoarseness does not signal a specific emergency situation. Purulent drainage from the external canal may signify a ruptured tympanic membrane or otitis externa. Tragal pain is significant for otitis externa. When examining vessels of the eye, the: (arteries are smaller than the veins) The arteries are 2/3 to 4/5 the diameter of the veins. The arteries appear as light red in color; veins are darker red. Interestingly, the veins in the eyes pulsate; the arteries do not. Loss of venous pulsations can be identified in patients with head trauma, meningitis, or elevated intracranial pressure. A patient describes a sensation that "there is a lump in his throat." He denies throat pain. On exam of the throat and neck, there are no abnormalities identified. What is the most likely reason this occurs? (Globus) The term used to describe the sensation of "a lump in my throat," or the feeling that there is a foreign body in the throat, is globus. It is not associated with sore throat or pain. The most common cause of globus is GERD or other disorders of the upper esophageal tract. If there is no actual foreign body or abnormality, other etiologies may be psychologic or psychiatric disorders. A patient who is otherwise healthy states that he woke up this morning and has been unable to hear out of his left ear. The Weber and Rinne tests were performed. What is the primary reason for doing this? (It helps differentiate conductive from sensorineural hearing loss) The Rinne and Weber tests can help differentiate conductive from sensorineural hearing loss. Once it is determined that the patient's hearing loss is conductive or sensorineural, the differential can be better developed. Common causes of conductive hearing loss are cerumen impaction, otitis externa, and tympanic membrane rupture. Common causes of sensorineural hearing loss are presbycusis, Meniere disease, and acoustic neuroma. What are the most common signs and symptoms associated with mononucleosis? (Fatigue and lymphadenopathy) The most common symptoms associated with mononucleosis (mono) are lymphadenopathy (100%) and fatigue (90-100%). Pharyngitis occurs in 65-85% of patients. Cough occurs less than 50%; splenomegaly occurs 50-60%; fever 80-95%. The least common symptom of mono is rash. It occurs in only 3-6% of patients. A 93-year-old demented adult has been recently treated for an upper respiratory infection (URI) but drainage from the right nostril persists. What should the NP suspect? (Presence of a foreign body) Two clinical clues should make the examiner suspect a foreign body. First, the patient has continued drainage despite treatment. Second, the drainage is unilateral. Unilateral drainage from a nostril should prompt the examiner to visualize the turbinates. In this case, a foreign body could probably be visualized. AV nicking may be identified in a patient who has what disease? (Hypertension) Arteriovenous nicking (AV nicking), or nipping, is commonly seen in patients who have hypertension. It represents retinal microvascular changes. These are typically early changes and usually reflective of chronic hypertension. More severe damage can be seen when flame hemorrhages or cotton wool spots are identified. These often represent current blood pressure elevations, since these tend to be more acute evidence of elevated blood pressure. Most commonly, epistaxis occurs: (at Kiesselbach’s plexus) Most nosebleeds occur in men; 80% occur anteriorly. Kiesselbach’s plexus is the most common site for any epistaxis to occur because this site represents the anastomosis of branches of three primary vessels: the ethmoidal artery, the sphenopalatine artery, and the facial artery. Anticoagulants place patients at very high risk for nose bleeds, but patients who take anticoagulants do not constitute the majority of patients with nose bleeds. A patient presents with findings of pain, warmth, redness, and swelling below the inner canthus toward nose. Tearing is present and when pressure is applied to the lacrimal sac, a purulent discharge from the puncta is noted. This is suggestive of: (dacryocystitis) Dacryocystitis is infection and blockage of the lacrimal sac and duct. Symptoms include pain, warmth, redness, and swelling below the inner canthus toward nose. Tearing is present and when pressure is applied to the lacrimal sac, a purulent discharge from the puncta is noted. Red, scaly, greasy flakes and thickened, crusted lid margins are consistent with blepharitis. Symptoms include burning, itching, tearing, foreign body sensation, and some pain. Hordeolum is a localized staphylococcal infection of the hair follicles at the lid margin. A beady nodule protruding on the lid, chalazion is an infection or retention cyst of a meibomian gland and if infected, it points inside and not on lid margin. Which antihistamine is preferred for treating allergic rhinitis in an adolescent or adult? (Once-daily, nonsedating) The preferred antihistamines are long-acting (once-daily dosing) and nonsedating. These are second- generation antihistamines. Diphenhydramine and chlorpheniramine are first-generation antihistamines. The first-generation antihistamines are sedating and require frequent dosing. Consequently, they are not as desirable as the second-generation antihistamines. A 70 year-old male has a yellowish, triangular nodule near the iris. This is probably: (a pinguecula) Pinguecula are common as patient’s age. They usually appear on the nasal side first and then on the temporal side. This is a completely benign finding. A stye is also called a hordeolum. It is a tender, painful infection of a gland at the eyelid margin. These are self-limiting. A chalazion is a nontender enlargement of a meibomian gland. A subconjunctival hemorrhage is a blood-red colored area on the sclera that does not affect vision. It occurs and resolves spontaneously. A patient who is 52 years old presents to your clinic for an exam. You notice a yellowish plaque on her upper eyelid. It is painless. What should the NP assess? (Lipid levels) The description in the question describes a xanthelasma. It is slightly raised and is a well-circumscribed plaque, usually on the upper eyelid. One or both lids may be affected. These are often associated with lipid disorders but may occur independent of any systemic or local disease. These plaques do not affect vision. An elderly patient who has a red eye with tearing was diagnosed with conjunctivitis. What characteristics below most closely indicate viral conjunctivitis? (Profuse tearing) A patient with viral conjunctivitis typically has profuse tearing and minimal exudate. Patients with bacterial conjunctivitis have moderate tearing and exudate. Both are considered highly contagious. Patients should refrain from work or group activities for 48 hours until symptoms have subsided. The most common cause of acute pharyngitis in children is (respiratory viruses) The most common cause of acute pharyngitis is infection with viral agents. The most common viruses are adenoviruses, coxsackie A virus, and parainfluenza virus. The most frequent bacterial cause of acute pharyngitis is Streptococcus pyogenes. The most prevalent time of year for Streptococcus outbreaks is winter. Papilledema is noted in a patient with a headache. What is the importance of papilledema in this patient? (It could be an important finding in this patient) Papilledema represents swelling of the optic nerve head and disc secondary to increased intracranial pressure (ICP). It is not a common finding in patients with headaches, only those with headache secondary to ICP. The pressure disrupts fluid flow within the nerve and swelling results. The cardinal symptom of ICP is a headache; papilledema is a secondary finding. A patient is diagnosed with otitis externa. He complains of tragal pain, otic discharge, otic itching, and fever. What is the cardinal symptom of otitis externa? (Tragal pain) Otitis externa is “swimmer’s ear.” This is a superficial infection usually caused by Pseudomonas in the external canal. Fever, a typical systemic symptom, is inconsistent with otitis externa since the infection is superficial. The other symptoms listed are typical of patients who are diagnosed with otitis externa. However, the cardinal symptom is tragal pain. Mr. O has been diagnosed with hearing loss secondary to exposure to an ototoxic medication. Which one may be associated with ototoxicity? (Aspirin) Many medications are ototoxic in patients who are otherwise healthy. Some patients are at increased risk (for ototoxicity) when they consume ototoxic medications if they have impaired renal function. Renal impairment makes excretion of the ototoxic drug more difficult, and ototoxicity becomes more likely. Hearing loss secondary to use of the following medications should always be assessed: aspirin, aminoglycosides, vancomycin, erythromycin, loop diuretics (like furosemide), the antimalarial medications, sildenafil (tadalafil, vardenafil) and cisplatin. ACE inhibitors, digoxin, and beta blockers are not associated with ototoxicity. A teenager with fever and pharyngitis has a negative rapid strep test. After 24 hours, the throat culture reveals “normal flora." Which conclusion can be made? (The pharyngitis is of undetermined etiology) The patient has a preliminary culture that indicates the presence of normal flora, i.e. no finding of pathogenic organisms like beta hemolytic Strep. A final culture result generally takes longer than 24 hours to complete. It is premature to make a diagnosis at 24 hours with this culture report. The only conclusion that can be made at this time is "pharyngitis of undetermined etiology." He should be treated symptomatically with antipyretics and analgesics until a final culture is available to help with formulation of a diagnosis. Derm/skin A microscopic examination of the sample taken from a skin lesion indicates hyphae. What type of infection might this indicate? (Fungal) Under microscopic exam, hyphae are long, thin and branching and indicate dermatophytic infections. Hyphae are typical in tinea pedis, tinea cruris, and tinea corporis. A child with a sandpaper-textured rash probably has: (Strep infection) Streptococcal infections can present as a sandpaper-textured rash that initially is felt on the trunk. Rubeola, measles, produces a blanching erythematous “brick-red” maculopapular rash that begins on the back of the neck and spreads around the trunk and then extremities. Varicella infection produces the classic crops of eruptions on the trunk that spread to the face. The rash is maculopapular initially and then crusts. Roseola produces a generalized maculopapular rash preceded by 3 days of high fever. A 40-year-old female patient presents to the clinic with multiple, painful reddened nodules on the anterior surface of both legs. She is concerned. These are probably associated with her history of: (ulcerative colitis) These nodules describe erythema nodosum. These are most common in women aged 15-40 years old. They are typically found in pretibial locations and can be associated with infectious agents, drugs, or systemic inflammatory disease like ulcerative colitis. They probably occur as a result of a delayed hypersensitivity reaction to antigens. It is not unusual to find polyarthralgia, fever, and/or malaise that precede or accompany the skin nodules. A patient is diagnosed with tinea pedis. A microscopic examination of the sample taken from the infected area would likely demonstrate: (hyphae) Under microscopic exam, hyphae are long, thin and branching, and indicate dermatophytic infections. Hyphae are typical in tinea pedis, tinea cruris, and tinea corporis. Yeasts are usually seen in candidal infections. Cocci and rods are specific to bacterial infections. When can a child with chickenpox return to daycare? (After all lesions have crusted) Chickenpox is highly contagious and can be spread via respiratory secretions from an infected person or by direct contact from the vesicle fluid from lesions on the skin or mucus membranes. The usual incubation period is about 2 weeks but can be as long as 21 days or as short as 10 days. The greatest period of infectivity is 48 hours prior to the onset of the rash and until all the skin lesions have crusted over. A patient with a primary case of scabies was probably infected: (3-4 weeks ago) The incubation period for scabies is about 3-4 weeks after primary infection. Patients with subsequent infections with scabies will develop symptoms in 1-3 days. The classic symptom is itching that is worse at night, coupled with a rash that appears in new areas over time. The nurse practitioner examines a patient who has had poison ivy for 3 days. She asks if she can spread it to her family members. The nurse practitioner replies: (“No, transmission does not occur from the blister’s contents”) The skin reaction seen after exposure to poison ivy (or any other skin irritant), takes place because of contact with the offending substance. In the case of poison ivy, the harmful exposure occurs from contact with oil from the plant. The eruptions seen are NOT able to transmit the reaction to other people unless oil from the plant remains on the skin and someone touches the oil. The fluid found in the blisters is NOT able to transmit poison ivy to anyone; only the oil from the plant can do that. After oil has touched the skin, some time must pass for the reaction to occur. Therefore, reaction times vary depending on skin thickness and quantity of oil contacting the skin. Which chronic skin disorder primarily affects hairy areas of the body? (Seborrheic dermatitis) Seborrheic dermatitis causes flaking of the skin, usually the scalp. In adolescents and adults, when it affects the scalp, it is termed dandruff. When this occurs in young children or infants, it is termed “cradle cap”. The exact cause is unknown; however it has a propensity for hairy areas of the body such as the scalp, face, chest, and legs. It appears greasy and flaky. This may be seen in patients with Parkinson’s disease. A patient with diabetes has right anterior shin edema, erythema, warmth, and tenderness to touch. This developed over the past 3 days. There is no visible pus. What is the most likely diagnosis to consider? (Cellulitis) This description is one of cellulitis. Cellulitis involves an infection of the subcutaneous layers of the skin. It must be treated with an oral antibiotic. In a patient with diabetes, it is particularly important to identify, and aggressively treat cellulitis early, because elevated blood sugar levels will make eradication more difficult. Buerger’s disease involves inflammation of the medium-sized arteries and does not present on the anterior shin only. DVT seldom presents on the anterior shin, so this is not likely. Venous disease does not present acutely, as in this situation. The agent commonly used to treat patients with scabies is permethrin. How often should it be applied to eradicate scabies? (Once) A single whole-body application of permethrin is usually successful in eradicating infection with scabies. It is applied over the entire body from the neck down. The lotion is left on and then showered off 8-12 hours later. All contacts must be treated at the same time and all potential fomites (bed linen, mattresses, cloth furniture, etc.) must be treated as well. Permethrin can be sprayed on cloth fomites, or the fomite can be bagged for several days, washed and dried in a washing machine and dryer. Ironing clothes after washing them is acceptable. Impetigo is characterized by: (honey-colored crusts) Impetigo is a superficial bacterial infection of the skin characterized by honey-colored crusts. Another form of impetigo is characterized by the presence of bullae. These infections are treated with topical antibiotics, good hygiene, and frequent hand washing. It is usually caused by Staphylococcus or Group A Streptococcus. A 60-year-old patient is noted to have rounding of the distal phalanx of the fingers. What might have caused this? (Hepatic cirrhosis) Rounding of the distal phalanx describes clubbing. Clubbing of fingers is most often associated with chronic hypoxia as seen in cigarette smokers and patients with COPD or lung cancer. Other causes are cirrhosis, cystic fibrosis, pulmonary fibrosis and cyanotic heart disease. A patient has suspected scarlet fever. He likely has a sandpaper rash and: (a positive rapid Strep test) A patient with scarlet fever (scarlatina) has a common childhood disease that is characterized by sore throat, fever, and a scarlet “sandpaper” rash. The causative organism is Group A beta hemolytic Streptococcus pyogenes. The patient’s rapid Strep test will likely be positive. Diarrhea with abdominal cramps is not specific to scarlet fever. Petechiae represent an extravasation of blood under the skin and are not present with scarlet fever unless some other disease process is present. Petechiae should be considered to be a serious finding. A patient with a positive history of a tick bite about 2 weeks ago and erythema migrans has a positive ELISA for Borrelia burgdorferi. The Western blot is positive. How should he be managed? (He should receive doxycycline for Lyme disease) The first serologic test for Lyme disease is the ELISA. If this is positive, it should be confirmed. In this case, it was confirmed by a Western blot and it is positive. This patient can be diagnosed with Lyme disease. The appropriate treatment for erythema migrans is doxycycline, amoxicillin, or cefuroxime for 21 days. All three medications were found to be of equal efficacy. A patient will be taking oral terbinafine for fingernail fungus. The NP knows that: (terbinafine is an inhibitor of the CYP 2D6 enzymes) Many oral antifungal agents inhibit the 3A4 or 2D6 enzymes in the cytochrome P450 system. This is why they must be used with extreme caution (or not used) in patients who consume medications that need 3A4 or 2D6 enzymes for metabolism. And, liver enzymes must be monitored in patients who take oral antifungal medications and discontinued if elevations are >2.5 times the upper limits of normal. No oral agent has a 95% cure rate for fingernail fungus (tinea unguium). This can be a difficult infection to clear even if oral antifungal agents are utilized. A topical antifungal agent typically will not clear the infection if the nail matrix is involved. There is anecdotal evidence that menthol ointments or bleach may cause resolution when used topically. Generally, resolution of fingernail fungus occurs more rapidly than toenail fungus because toenails grow at slower rates than fingernails. A skin lesion that is a solid mass is described as a: (papule) A papule is an elevated solid mass up to 1.0 cm. in diameter. A macule is flat and small, like a freckle. A vesicle is filled with a serous fluid and less than 1.0 cm in diameter. A bullae is fluid filled and larger than 1.0 cm in diameter. The nurse practitioner is examining a 3-month-old infant who has normal development. She has identified an alopecic area at the occiput. What should be done? (Encourage the caregiver to change the infant’s head position) In a normally developing infant, an alopecic area at the occipital area generally develops because the infant has been placed in the supine position during sleeping and waking hours. Prolonged pressure on the occipital area can restrict hair growth. This is normal and will resolve when the infant begins to have better head control and movement; and she begins to have less pressure on the occipital area. Sometimes coarse, dry hair can be indicative of hypothyroidism; not necessarily alopecia. The most common form of skin cancer is: (basal cell carcinoma) Skin cancers are divided into two major groups: nonmelanoma and melanoma skin cancer. Basal cell carcinoma is considered nonmelanoma skin cancer and is the most common form of skin cancer in the US. It is most common in 40- to 60-year-olds, but can occur at any age if the skin is regularly exposed to sunlight or ultraviolet radiation. Basal cell carcinoma grows slowly, and if not treated it can spread to surrounding areas of tissue or bone. The nurse practitioner identifies satellite lesions in a 6-month-old infant. These are: (indicative of candidal infection) Satellite lesions are common in the diaper area of infants with a candidal diaper infection. They generally are associated with a beefy red rash. The skin creases are more commonly affected, but satellite lesions can be found anywhere that Candida can be found. A patient who is at high risk for skin cancer should: (examine his skin monthly for changes) Patients should be examined periodically for evidence of skin cancer by a professional examiner (NP, MD or PA). The frequency and type of examination depends on the risk level, and personal and family history of the patient. However, a patient should examine his own skin regularly for changes. Once he has begun to examine his skin, research demonstrates that he will identify early changes and can make his provider aware of them. An example of a premalignant lesion that develops on sun-damaged skin is: (actinic keratosis) Actinic keratoses (AK) are a result of solar damage to the skin. They are most common on the face, bald scalp, and forearms. Patients who present with AK usually have multiple of them. A characteristic that helps identification of AK is an area of erythema that surrounds the lesion. AK is sometimes easier felt than seen. Which of the following areas of the body has the greatest percutaneous absorption? (Genitalia) Genitalia have the highest percutaneous absorption across the entire body. This is important because low-potency creams will act with greater potency in this area. Low-potency creams/lotions should be used initially for treating skin conditions involving the genitalia. The sole of the foot has the lowest percutaneous absorption, followed by the scalp, forehead, and genitalia. Therefore, the sole of the foot will require more potent vehicles to enhance absorption. The main difference between cellulitis and erysipelas is the: (layer of skin involvement) Erysipelas and cellulitis both cause skin erythema, edema, and warmth. However, erysipelas involves the upper dermis and superficial lymphatics; cellulitis involves the deeper dermis and subcutaneous fat. Erysipelas is usually caused by Streptococcus; cellulitis may be caused by Staphylococcus and less commonly by Streptococcus. Most cases of atopic dermatitis exacerbation are treated with: (topical steroids) An exacerbation of atopic dermatitis is termed eczema. Under normal conditions, the skin should be kept well lubricated with emollients. These should be used liberally as often as needed to prevent skin from becoming dry. Dry skin is more prone to exacerbations. When an exacerbation occurs, topical steroids are very effective and are commonly used. The lowest potency steroid that resolves the exacerbation should be used. A 6-year-old patient with sore throat has coryza, hoarseness, and diarrhea. What is the likely etiology? (Viral etiology) This constellation of symptoms is typical of a viral infection. Group A Streptococcus is usually not accompanied by coryza. H. parainfluenzae is not a common cause of pharyngitis. Mycoplasma usually is associated with lower respiratory tract infections. A pregnant mother in her first trimester has a 5-year-old who has Fifth Disease. What implication does this have for the mother? (There is a risk of fetal death if she becomes infected) Pregnant mother should avoid exposure to patients with known Fifth Disease. However, the risk of transmission is very low. She should avoid exposure to aplastic patients who are infected because they are highly contagious. Infection during pregnancy is associated with a 10% risk of fetal death. There is no need for an ultrasound today. This pregnant patient does not have evidence of disease. She should be monitored for a rash which could indicate infection. A 74-year-old woman is diagnosed with shingles. The NP is deciding how to best manage her care. What should be prescribed? (An oral antiviral agent) An oral antiviral agent such as acyclovir, famciclovir or valacyclovir should be prescribed, especially if it can be initiated within 72 hours after the onset of symptoms. The addition of oral corticosteroids to oral antiviral therapy demonstrates only modest benefit. Adverse events to therapy are more commonly reported in patients receiving oral corticosteroids. There is no evidence that corticosteroid therapy decreases the incidence or duration of postherpetic neuralgia or improved quality of life. Corticosteroids should be limited to use in patients with acute neuritis who have not derived benefit from opioid analgesics. An adolescent has acne. The nurse practitioner prescribed a benzoyl peroxide product for him. What important teaching point should be given to this adolescent regarding the benzoyl peroxide? (Photosensitivity of the skin can occur) Benzoyl peroxide can produce sensitivity to the sun, so adolescents should be informed of this. This product can be used twice daily. It can cause peeling of the skin, but this is not a common occurrence. Hypersensitivity can occur with any topical product and is not specific to benzoyl peroxide. A 70-year-old is diagnosed with multiple cherry angiomas. The nurse practitioner knows that: (these may bleed profusely if ruptured) Cherry angiomas are mature capillary proliferations that are more common in middle-aged and older adults. They blanch with pressure and are usually 0.1-0.4 cm in diameter. They are commonly found on the trunk as multiple lesions. Because they are a proliferation of capillaries, they will bleed significantly if they rupture. The bleed is not life threatening, but in older adults who take aspirin, the bleeding will be worse. Pressure should be held over the ruptured area until bleeding stops. These are not precursors of skin malignancies. A patient has seborrheic dermatitis. Which vehicle would be most appropriate to use in the hairline area to treat this? (Foam) Seborrheic dermatitis affects the hairy areas of the body. In hairy areas of the body, foams are specifically used because they spread easily and are transparent. Lotions can be used in hairy areas because they provide a cooling, drying effect and are transparent. Lotions are the weakest of all vehicles. Creams and powders could be used, but patients prefer other vehicles and so adherence is less with these. A patient with eczema asks for a recommendation for a skin preparation to help with xerosis. What should the NP respond? (Use a petroleum-based product) Xerosis is dry skin. It is common in patients who have eczema. Using thick creams or ointments can prevent xerosis. Lotions should be avoided because they have high water content that promotes evaporation of water from the skin. Hypoallergenic refers to the allergenicity of a product. This is not related to the water content of products. A topical treatment for basal cell carcinoma is: (5-fluorouracil) Several treatments exist for basal and squamous cell carcinoma. The majority are simple procedures like cryotherapy, electrodessication, surgical excision, and a topical treatment like 5-fluorouracil (5-FU). The other agents listed are not used to treat basal or squamous cell carcinoma. 5-FU works by inhibiting DNA synthesis. It is effective if used for superficial basal cell carcinomas. It is available in cream and solution and is usually applied twice daily for 3-6 weeks. The most common place for basal cell carcinoma to be found is the: (Face) The most common presentation of basal cell carcinoma (BCC) is on the face. This is probably because BCC occurs secondary to sun damage. The most common sun exposure occurs on the face. In fact, 70% of BCC occurs on the face; 15% occurs on the trunk. An infant is diagnosed with diaper dermatitis. Satellite lesions are visible. This should be treated with a: (topical antifungal agent) The finding of satellite lesions associated with diaper dermatitis indicates a Candidal infection. This patient will be most effectively treated with a topical antifungal agent, allowing the lesions to be exposed to air for periods of time (like during a nap). A moisture barrier like zinc oxide is more beneficial when the diaper dermatitis is due to irritants like prolonged exposure to urine or feces. A low-potency steroid cream should be used with caution in an infant with a fungal infection. A low-potency steroid cream in conjunction with an antifungal can be helpful if there is a great amount of underlying inflammation, but it has the potential to worsen the infection. A 3-year-old female had a fever of 102° F for the last 3 days. Today she woke up from a nap and is afebrile. She has a maculopapular rash. Which statement is true? (The rash will blanch) This describes a patient with roseola or exanthem subitum. This is a common viral exanthem found in young children caused by human herpes virus 6. It is characterized by high fever for 3 days followed by the abrupt cessation of fever and the appearance of a maculopapular rash. This usually resolves in a few days. The child may return to school or daycare when he has been fever-free for 24 hours. A 71-year-old female presents with a vesicular rash that burns and itches. Shingles is diagnosed. An oral antiviral: (should be started within 72 hours of the onset of symptoms) This patient has been diagnosed with shingles. This can produce a painful neuritis. Shingles is treated with an oral antiviral agent, preferably within 72 hours of onset of the symptoms. Treating shingles with an oral antiviral agent shortens the severity and duration of shingles. It may also help decrease the incidence of post-herpetic neuralgia. A skin disorder has a hallmark finding of silvery scales. What word below describes this common condition? (Chronic) “Silvery scales” describes the hallmark finding in psoriasis. This is a chronic condition. It is not infectious, contagious, or acute. There are several variants, but “silvery scales” is the most common form. A child has 8-10 medium brown café au lait spots > 1 cm in diameter. The differential diagnosis should include: (neurofibromatosis) Neurofibromatosis (NF) is a common neurocutaneous disorder. The most common form is von Recklinghausen’s NF. Approximately 85% of patients with NF have this type. The incidence is about 1 in 2,600 people. Children with this disorder may have cognitive deficits, learning disabilities and other neurological related problems. They should be referred to neurology for diagnosis and treatment. A low-potency topical hydrocortisone cream would be most appropriate in a patient who has been diagnosed with: (atopic dermatitis) Low-potency steroid creams are almost never potent enough to treat psoriasis. Psoriasis requires higher- potency steroid preparation or systemic agents. Impetigo is a superficial bacterial infection, and a steroid cream would be contraindicated. Cellulitis is an infection of the subcutaneous layer of the skin and requires an oral or systemic antibiotic. Atopic dermatitis is a chronic inflammatory disorder of the skin that involves a genetic defect in the proteins supporting the epidermal layer. A patient with atopic dermatitis would be the most appropriate (of those listed above) to use a low-potency topical steroid cream. A patient is found to have koilonychia. What laboratory test would be prudent to perform? (Complete blood count) Koilonychia is the term that describes spoon-shaped nails. Spoon-shaped nails may be present in patients who have longstanding iron deficiency anemia. A CBC should be performed to assess for anemia. The most common symptoms of iron deficiency anemia are weakness, headache, irritability, fatigue, and exercise intolerance. A 23-year-old male appears in clinic with the following lesion on his trunk. This lesion is usually associated with: (pityriasis rosea) A herald patch is usually located on the trunk and associated with pityriasis rosea. It precedes the generalized Christmas tree pattern rash. Folliculitis is a superficial infection of the hair follicles. It presents as clusters of small, raised, erythematous lesions, not as a singular lesion as demonstrated in this image. Diabetes may be associated with acanthosis nigricans, a condition characterized by areas of velvety, hyperpigmented skin most commonly on the body folds and skin creases such as the neck and axillae. Hypothyroidism is not associated with this lesion. A 28-year-old has thick, demarcated plaques on her elbows. Which features are suggestive of psoriasis? (Silvery scales that are not pruritic) There are many different presentations of psoriasis. Plaque psoriasis, which is described in this question, is usually found in a symmetrical distribution on the scalp, elbows, knees, and/or back. The size of the lesions ranges from 1-10 cm in diameter. Usually the plaques are asymptomatic, but they may be mildly pruritic. Scaly lesions found on the scalp are not specific to psoriasis and could be seborrheic dermatitis. A scaly border around the plaque could describe the lesions associated with pityriasis rosea. Which of the following skin lesions in an older adult is a premalignant condition? (Actinic keratosis) Actinic keratosis is a premalignant condition of the skin and is considered an evolving carcinoma in situ. It is a precursor of squamous cell carcinoma. The lesions are usually multiple in occurrence and sit on an erythematous base. They appear dry, scaly, and flat and are usually secondary to sun damaged skin. Thus they are found on sun-exposed areas. The most common sites are the face, ears, lateral forearms, and tops of hands. A patient presents with plaques on the extensor surface of the elbows, knees, and back. The plaques are erythematous and thick, silvery scales are present. This is likely: (plaque psoriasis) Plaque psoriasis is seen initially in young adults and is characterized as described above. The thick, silvery scale is pathognomic and is usually asymptomatic, but some patients will complain of pruritus. A clinical finding that will help establish a diagnosis is pitting of fingernails. This occurs in about 50% of patients with psoriasis. The plaques are commonly distributed on the scalp, extensor surface of the elbows, knees, and back. This is a chronic skin disorder. A 15-year-old male has worked this summer as a lifeguard at a local swimming pool. He complains of itching in the groin area. He is diagnosed with tinea cruris. The nurse practitioner is likely to identify: (well marginated half-moon macules on the inner thigh) Tinea cruris, “jock itch” is common during warm months and in humid areas. It is a fungal infection that affects the scrotum and inner thighs, but never affects the penis and is never evidenced by scrotal swelling. He is probably at increased risk because he is working as a lifeguard and may wear damp or wet swim trunks during work. He should be treated with a topical antifungal cream, advised to dry off after swimming, and to put on dry swim trunks. A 68-year-old female adult with pendulous breasts complains of “burning” under her right breast. The nurse practitioner observes a malodorous discharge with mild maceration under both breasts. What is this? (Intertrigo) This is not unusual in adults with pendulous breasts. Intertrigo is common in areas between skin folds, under the breasts, between the scrotum and inner thigh, or between the toes. These are moist lesions that can be easily treated if the skin can be separated from touching the adjoining skin and the area can be kept dry. A topical powder with an antifungal would likely resolve this if used twice daily for 7-14 days. A diagnosis of diabetes should be considered if this is resistant to treatment or if it recurs. An example of a first-generation cephalosporin used to treat a skin infection is: (cephalexin) Two common first-generation cephalosporins used to treat skin and skin structure infections are cephalexin and cefadroxil. These are taken two to four times daily and are generally well tolerated. These antibiotics provide coverage against Staphylococcus and Streptococcus, common skin pathogens. A patient has a “herald patch” and is diagnosed with pityriasis rosea. Where is the “herald patch” most commonly found? (On the chest) The herald patch associated with pityriasis rosea is most commonly found on the trunk. It precedes the generalized Christmas tree pattern rash that is easily noted on the rest of the body. Because it appears round and has a darkened center, it looks like a ringworm. In fact, it is commonly mistaken for ringworm until the Christmas tree pattern rash appears. It would be unusual to identify the herald patch on a body part other than the trunk, but there are case reports of this. A 16-year-old has been diagnosed with Lyme disease. Which drug should be used to treat him? (Doxycycline) Doxycycline is frequently chosen first line to treat Lyme disease. However, numerous studies have demonstrated that amoxicillin and cefuroxime have equal efficacy as doxycycline in treatment of early Lyme disease. These drugs are recommended in patients who exhibit erythema migrans. Doxycycline is not recommended in children younger than 9 years of age. A 9-year-old female has presented to your clinic because of a rash on the left, upper area of her anterior trunk. She is embarrassed and very reticent to lift her blouse because her nipple will be exposed. How should the NP proceed? (Examine all other areas of the trunk, then ask the child to lift her blouse) The NP must visualize the area during exam so that an appropriate diagnosis can be made. Since the child is 9 years old, she should be given the opportunity to remove her blouse before allowing another adult to do this. Allowing the child to do this will put “control” in her hands. Hand-foot-and-mouth disease and herpangina: (are viral infections caused by Coxsackie viruses) These two common viral exanthems are caused by Coxsackie A viruses. Sometimes herpangina is caused by Coxsackie A or B. Ulcerations are produced on the mucous membranes, not pustules. Orchitis can occur in males infected with mumps. Herpangina typically occurs during summer and fall; hand-foot-and- mouth disease (HFM) occurs in late summer and fall. Both produce oral symptoms, but only HFM produces blisters on the palms of the hands and/or soles of the feet. Both are self-limiting viral illnesses A 74-year-old male patient has sustained a laceration to his foot. His last tetanus shot was more than 10 years ago. He has completed the primary series. What should be recommended? (Tetanus, diphtheria, and acellular pertussis (Tdap)) More than 10 years has elapsed since this patient’s last tetanus shot. He needs another one. Tdap is specifically indicated for adolescents, older adults, healthcare providers, and third trimester pregnant patients who have completed a primary series. Tetanus toxoid is indicated in the rare adult or child who is allergic to the aluminum adjuvant in the Td immunization. An adolescent takes isotretinoin for nodulocystic acne. She is on oral contraceptives. Both were prescribed by the dermatologist. The adolescent presents to your clinic with a sinus infection. Her temperature is 99.5° F and her blood pressure is 160/100 mmHg. How should this be managed? (Call the dermatologist to report the elevated BP) The nurse practitioner is responsible for treating the sinus infection but has also become aware of a potentially harmful situation involving the elevated blood pressure and oral contraceptive use. The safest and most professional action is to call the dermatologist to discuss your concerns regarding the elevated BP and concomitant oral contraceptive use since this potentially increases the risk of stroke in this adolescent. Care and professional courtesy should be exercised when discontinuing a medication that another provider has initiated. Professional courtesy is extended to the prescriber by calling them prior to discontinuing a medication they have ordered. Mr. Johnson is a 74-year-old who presents with a pearly-domed, nodular-looking lesion on the back of the neck. It does not hurt or itch. What is a likely etiology? (Basal cell carcinoma) Basal cell’s classic description is “a pearly-domed nodule with a telangiectatic vessel”. It is commonly found on sun-exposed areas like the head or neck. Sending the patient to dermatology (since these represent skin cancer) best treats these lesions. Sometimes these lesions can be treated with a topical agent like 5-fluorouracil if they are superficial; others require surgical removal. A 16-year-old male has nodulocystic acne. What might have the greatest positive impact in managing his acne? (Isotretinoin (Accutane)) Nodulocystic acne is the most severe form of acne vulgaris. Nodules and cysts characterize this disease. They can be palpated and usually seen on the skin, although they actually are under the skin’s surface. They develop when the follicle wall ruptures and leaks pus and cell contents into the dermis. The contaminated material infects adjoining follicles and the nodule develops. Isotretinoin is the only known effective treatment. Which of the following antibiotics may increase the likelihood of photosensitivity? (Ciprofloxacin) Many medications can produce a phototoxic reaction when a patient is exposed to sunlight. Antibiotics are especially notable for this. Common antibiotics associated with photosensitivity are tetracyclines, sulfa drugs, and fluoroquinolones. Ciprofloxacin is a fluoroquinolone. Amoxicillin and cephalexin are beta lactam antibiotics. Azithromycin is a macrolide antibiotic. Other common medications/classes that increase photosensitivity are hydrochlorothiazide, diltiazem, selective serotonin reuptake inhibitors, antihistamines, ibuprofen, and naproxen. Which of the following lesions never blanches when pressure is applied? (Purpura or petechiae) Blanching with pressure over spider angiomas always occurs. Spider veins and cherry angiomas usually blanch with pressure. Purpura and petechiae never blanch with pressure. Purpura and petechiae represent an extravasation of blood under the skin. These will not blanch when pressure is applied. This is usually observed in patients with thrombocytopenia or trauma. An older adult patient has been diagnosed with shingles on the right lateral aspect of her trunk. It initially appeared yesterday. It is very painful. How should she be managed? (An oral antiviral agent and pain medication) The primary goal of antiviral therapy in a patient diagnosed with shingles is to reduce the risk, or severity of postherpetic neuralgia. Since she has been identified within 72 hours of onset of lesions, she can be treated with most benefit with an oral antiviral agent. Studies do not demonstrate that patients have reduction of pain or resolution of symptoms faster if oral steroids are given. They should be avoided in older patients because there is no identified benefit. Shingles can be very painful, so treatment for pain should be priority. A young child has developed a circumferential lesion on her inner forearm. It is slightly raised, red and is pruritic. It is about 2.5 cm in diameter. This is probably related to: (the child’s new cat) This describes ringworm. It is a fungal infection that is common in children. A typical precipitant is a new animal like a cat. Since it appears on the inner forearm, it is likely the child got this from holding the cat. It should be treated with a topical antifungal agent. The primary therapeutic intervention for patients who present with hives is: (antihistamines) The primary cause of pruritus associated with hives is histamine release. Histamine is released from mast cells with other substances of anaphylaxis. Antihistamines are the primary therapeutic intervention. Topical steroid use is not helpful. Calcium channel blockers (nifedipine) are used as a “last resort” for refractory cases of urticaria. Steroids do not inhibit mast cell degradation and so are less helpful than thought. Steroids can be used for persistent attacks of acute urticaria if antihistamines are not helpful. The lesions seen in a patient with folliculitis might be filled with: (pus) Folliculitis is a superficial inflammation of hair follicles usually caused by bacteria. As a superficial infection, it involves only the epidermis. When this occurs, there are usually numerous pustular lesions. The composition of pus is dead white cells and other cellular debris. Which vehicle is least appropriate in a patient who has atopic dermatitis? (Lotions) Patients who have atopic dermatitis need continuous skin hydration. Lotions can worsen xerosis (dry skin) due to evaporation of water on the skin. In contrast to creams and ointments, lotions have a high water content and a low oil content. Creams have a lower water content. Ointments have no water and are excellent agents to use on dry skin as well as to prevent dry skin. A patient has been diagnosed with scabies. What is the medication of choice to treat this? (Permethrin) Scabies is eradicated by using permethrin and good hygiene. All household and personal contacts must be treated simultaneously, and meticulous care must be exercised to prevent transmission by cross contamination. All clothing, stuffed animals, linens, mattresses, and cloth furniture must be treated to prevent further transmission. The American Cancer Society uses an ABCDE mnemonic to help patients develop awareness of suspicious skin lesions. What does the “B” represent? (Border) The mnemonic is helpful when looking at skin lesions, but it is primarily used for patient education. The “A” represents asymmetry (asymmetrical lesions are worrisome), “B” is border (irregular borders), “C” is color (colored lesions have more melanin and may be associated with malignant melanoma), “D” is diameter (larger than a pencil eraser [6 mm] is concerning), and “E” represents enlarging or elevated (lesions that are actively enlarging are growing; elevated lesions are concerning). A “herald patch” is a hallmark finding in which condition? (Pityriasis rosea) Pityriasis rosea (PR) is a self-limiting exanthematous skin disorder characterized by several unique findings. It is more common in young adults. A characteristic finding is the “herald” or “mother” patch found on trunk. This looks like a ringworm and precedes the generalized “Christmas tree” pattern rash. The lesions associated with the rash are salmon-colored and oval in shape. Most cases clear in 4-6 weeks, but the plaques may last for several months. A patient has used a high-potency topical steroid cream for years to treat psoriasis exacerbations when they occur. She presents today and states that this cream “just doesn’t work anymore.” What word describes this? (Tachyphylaxis) Tachyphylaxis is the word used to describe a gradual and progressively poorer clinical response to a treatment or medication. This is particularly true of topical glucocorticoids, bronchodilators, nitroglycerine, and antihistamines when they are overused. The rebound effect describes a condition in which initial clinical improvement occurred, but worsening has occurred. Lichenification refers to a thickening of the skin. Drug-free intervals are important to prevent tachyphylaxis. A patient has been diagnosed with MRSA. She is allergic to sulfa. Which medication could be used to treat her? (Doxycycline) MRSA is methicillin-resistant Staph aureus. This is very common in the community and is typically treated with sulfa medications like TMP/SMX (Bactrim DS and Septra DS). If the patient is allergic to sulfa, this should not be used. A narrow-spectrum antibiotic that can be used is doxycycline or minocycline. It is given twice daily and is generally well tolerated. MRSA is resistant to the antibiotics in the other choices and so they should NOT be used to treat it. Topical 5-fluorouracil (5-FU) is used to treat: (basal cell carcinoma) 5-FU is a topical agent that can be used to treat basal cell carcinoma (BCC). It is most effective on rapidly proliferating cells. This treatment should only be used on superficial BCCs. If it is used on more invasive BCC, the cure rate is significantly lower. Therefore, 5-FU should be used only on superficial BCCs in noncritical locations. It is dosed as a 5% formulation twice daily for 3-6 weeks. A patient was burned with hot water. He has several 2-3 cm fluid-filled lesions. What are these termed? (Bullae) Bullae are fluid-filled lesions that are greater than 6 mm in diameter. These are common in patients who have a superficial partial-thickness burn. Vesicles are also fluid filled, but they are smaller than 5 mm in diameter. A cyst is enclosed in a sac that can contain fluid or gelatinous material. Wheals are erythematous, irregular raised areas on the skin. All of these are termed primary lesions. A child received a burn on his chest from a cup of hot coffee. On examination, the injured area appeared moist, red to ivory white in color, and features blisters. It is painful to touch. This burn would be classified as a: (superficial partial thickness burn) Types of burn injuries are chemical, electric, radiation, or thermal. They are classified by the depth of damaged skin. Symptoms of superficial partial thickness burns include: moist areas that are red to ivory white in color, immediate blister formation and painful to touch (pain receptors are intact). Superficial thickness burns appear erythematous without blisters and usually have local pain. Deep partial thickness burns have a dry, waxy, whitish appearance and resemble full thickness burns. Sometimes grafts are needed. Full thickness burns involve the destruction of all skin elements with coagulation of subdermal plexus, muscle, and or tendons. What finding is most characteristic of shingles? (Single dermatome affected) Shingles is herpes zoster. It characteristically affects a single dermatome. Grouped vesicles on an erythematous base may occur in some patients with shingles, but this is not unique to shingles. In fact, it is typical in many viral infections. Crusting may be seen with shingles, chicken pox, or impetigo. Pain, burning, and itching are symptoms that some patients have with shingles, but not all patients report itching with shingles. A patient reports that he found a tick on himself about 2 weeks ago. He presents today with a red circle and a white center near where he remembers the tick bite. He did not seek treatment at that time. Today he complains of myalgias and arthralgias. Which laboratory test can be used to help diagnose Lyme disease? (ELISA) A detailed history should always precede testing for Lyme disease. The red circle with the white center is likely erythema migrans (EM). EM is the characteristic skin lesion of Lyme disease (and other illnesses) and usually occurs within 1 month following the tick bite. Many learned authorities, including the Infectious Diseases Society of America, conclude that individuals should not be screened/tested for Lyme disease unless they have a high probability of having Lyme disease. In this case, historical features coupled with physical exam support the diagnosis, and thus screening. The most common initial serologic test for screening is an ELISA. If it is positive, it should be confirmed with a Western blot. Unfortunately, there are a large number of false positives and so a confirmation should be performed. The best way to evaluate jaundice associated with liver disease is to observe: (the sclera, skin, and lips) Looking at the sclera allows the examiner to see jaundice most easily and reliably. Jaundice may also appear in the palpebral conjunctiva, lips, hard palate, undersurface of the tongue, tympanic membrane, and skin. Jaundice in adults usually is a result of liver disease, but it can be due to excessive hemolysis of red blood cells. In infants, the usual cause is hemolysis of red blood cells, as is seen in physiologic jaundice. The term caput succedaneum refers to: (scalp edema) Caput succedaneum is a common finding in newborns. It is a result of pressure over the presenting part. This results in some ecchymosis of the scalp. While this may be disturbing to new parents who observe this in their newborn, it will resolve in a few days and is harmless. A 4-year-old has been diagnosed with measles. The nurse practitioner identifies Koplik’s spots. These are: (found on the inside of the cheek and are granular) Koplik’s spots are found in the oral cavity, especially on the buccal mucosa opposite the first and second molars. The spots are white and granular and are circled by an erythematous ring. The spots are pathognomonic for measles. The exanthem associated with measles is typically described as cranial to caudal in progression. The lesions become confluent and last for approximately 4 days before fading begins. A patient calls your office. He states that he just came in from the woods and discovered a tick on his upper arm. He states that he has removed the tick and the area is slightly red. What should he be advised? (No treatment is needed) Many factors must be present for a patient to develop Lyme disease from a tick bite. First, the tick must belong to Ixodes species. The tick must have been attached for at least 48 hours before disease can be spread. Time of year and stage of organism development affect transmission. There is no need for prophylactic treatment in this case because the tick has not been present long enough, though many patients will feel antibiotics are necessary. He could be checked to ensure that the entire tick has been removed. A wound has the following characteristics; partial thickness loss of dermis, a shallow open ulcer with red/pink bed, and no evidence of sloughing. What stage of pressure ulcer does this describe? (Stage II) Stage I is characterized by intact skin and nonblanchable redness of a localized area (usually over a bony prominence). Compared to adjacent tissue, the area may be painful, firm, soft, warmer or cooler. Stage II is characterized by partial-thickness loss of dermis presenting as a shallow open ulcer or a red-pink wound bed, absent sloughing. It may also present as an intact or open/ruptured serum-filled blister. Stage III is characterized by full-thickness tissue loss with or without visible subcutaneous fat; bone, tendon, and muscle are not exposed. Sloughing may be present but does not obscure the depth of tissue loss. The depth varies by anatomical location. Stage IV is characterized by full-thickness tissue loss with exposed bone, tendon, or muscle. Sloughing or eschar may be present on some parts of the wound bed. The depth varies by anatomical location. A patient has been in the sun for the past few weeks and has developed darkened skin and numerous 3-6 mm light-colored, flat lesions on his trunk. What is the likely etiology? (Tinea versicolor) Tinea versicolor is typically visualized during the spring and summer months when a patient has become darkened after sun exposure. The areas that are infected do not tan and so become very noticeable. The chest and back are common areas to observe tinea versicolor. There can be 100 or more in some infections. This can be treated with topical selenium sulfide or an oral antifungal agent. What advice should be given to a parent who has a child with Fifth Disease? (A parent may experience joint aches and pains) Fifth disease, erythema infectiosum, is a common viral exanthem seen in children 5-15 years of age. This produces a maculopapular rash that blanches easily. This rash is not pruritic but may last for several weeks before it completely goes away. Children are allowed to attend school as long as they have been fever free for 24 hours. Discomforts of this illness (fever, body aches, etc.) may be treated with acetaminophen or ibuprofen. Adults who are exposed to children with Fifth Disease may complain of arthralgias and myalgias for several weeks. A 6-year-old has been diagnosed with Lyme disease. Which drug should be used to treat him? (Amoxicillin) Amoxicillin, doxycycline, and cefuroxime have all been shown to have equivalent efficacy for treatment of Lyme disease. However, because this patient is 6 years old, he should not be given doxycycline as a first line treatment unless the other regimens are contraindicated. Macrolides like azithromycin should not be used first line because they are poorly effective at eradicating infection. They may be used in patients who are intolerant of penicillins and cephalosporins and who cannot take doxycycline. First- generation cephalosporins like cephalexin are poorly effective and should not be used. A patient presents with small vesicles on the lateral edges of his fingers and intense itching. On close inspection, there are small vesicles on the palmar surface of the hand. What is this called? (Dyshidrotic dermatitis) This dermatitis is intensely pruritic and involves the palms and soles and lateral aspects of the fingers. Over a couple of weeks, the vesicles desquamate. Recurrences are common. Seborrheic dermatitis affects only hairy areas of the body. The vesicles might raise suspicion of a viral infection, but this is not present in this case. A patient has 10 cm of well demarcated erythema on his lower leg that is raised and warm to touch. He had an abrupt onset of lower leg pain, and fever that began 36 hours ago. What is this? (Erysipelas) Erysipelas is characterized by an acute onset of symptoms as described in this scenario. Fever and chills are common. Patients with cellulitis tend to have a more gradual course, with development of symptoms over several days. The erythema noted in erysipelas is well demarcated and raised above the level of the skin. This elevation reflects that the more superficial dermis is involved. What is the proper technique to safely remove a tick from a human? (Pull it off with tweezers) Use tweezers to pull it off. If tweezers are not available, protected fingers should be used. The person removing the tick should take care NOT to crush the tick because it may contain infectious organisms. After the tick is removed, the skin should be washed well with soap and water. If mouth parts remain after the tick has been removed, they should NOT be removed. They will be expelled on their own and removal of these parts may cause significant skin trauma. The area should be monitored for 30 days for erythema migrans. A skin lesion fluoresces under a Wood’s lamp. What microscopic finding is consistent with this? (Hyphae) A Wood’s lamp emits ultraviolet light when turned on. If an area fluoresces under Wood’s lamp illumination, a fungal (and sometimes bacterial) infection should be suspected. Hyphae are associated with fungal infections. The test is most effectively performed in a darkened room so the fluorescence can be more easily identified. Deodorant, soap, and makeup may also fluoresce. About one-third of hyphae fluoresce. A 23-year-old male appears in clinic with the following nonpruritic lesion on his trunk. He first noticed this about 3 days ago. The lesion is probably: (a herald patch) Pityriasis rosea is a viral rash that is common in older children and young adults. It typically begins with a herald patch, a single round pink or salmon-colored, nonpruritic plaque on the chest, neck, or back. It is often mistaken for ringworm prior to the eruption of the Christmas tree pattern rash. The rash occurs within 1-2 weeks after the appearance of the herald patch. Scabies typically presents as a pruritic eruption characterized by small, erythematous, nondescript papules. Its prominent clinical feature is pruritus. Most cases of eczema initially occur by the age of five years, but can manifest in adults as an area of pruritic, thickened (lichenified), and excoriated skin in the flexural areas. Psoriasis may present as silvery scales or plaques. A patient presents to the minor care area of the emergency department after being bitten by a dog. The patient states that the dog had a tag around his neck and had been seen roaming around the neighborhood for days before the patient was bitten. The dog did not exhibit any odd behavior. How should this be managed? (Report the bite to animal control and administer appropriate medical care) All 50 states require reporting of animal bites to animal control or the state’s appropriate authority for reporting animal bites. It sounds unlikely that the dog could be infected with rabies, but rabies prophylaxis must be considered after all history and information has been gathered. Patients with atopic dermatitis are likely to exhibit: (itching) Atopic dermatitis is diagnosed on clinical presentation and includes evidence of pruritic skin. It is recurrent and often begins in childhood. For decades the "atopic triad" has been used to refer to patients with atopic dermatitis, asthma, and allergic rhinitis. This has recently been called into question. A similar triad, known as Samter’s triad, consists of asthma, aspirin sensitivity, and nasal polyps. Samter’s triad is not the same as the atopic triad. Which test is NOT suitable to diagnose shingles if the clinical presentation is questionable? (Complete blood count (CBC)) Herpes viruses are the causative agents in shingles, chickenpox, genital herpes, and oral fever blisters. Diagnosis is usually made on clinical presentation. However, in questionable cases, lab tests may be employed. A Tzanck preparation is a rapid test used to diagnose infections due to herpes viruses. Cells taken from a blister’s fluid are smeared on a slide and stained with a Wright’s stain, or the fluid can be used for other methods of testing. DFA is the most common test employed for shingles diagnosis because it can be rapidly performed and offers results in about 90 minutes. PCR may be performed on skin scrapings, serum or blood for herpetic diagnosis. CBC may indicate a patient with a viral infection, but it is nonspecific for herpetic infections. A patient exhibits petechiae on both lower legs but has no other complaints. How should the NP proceed? (Order a CBC) The presence of petechiae on the lower legs (or anywhere on the body) should prompt the NP to consider a problem that is related to a low platelet count. A CBC should be checked to assess the platelet count and for any evidence of anemia from blood loss. If the platelet count is found to be low, referral to hematology should be done. Blood cultures are of no value in this patient, who is otherwise asymptomatic. A 9-year-old has been diagnosed with chickenpox. A drug that should be avoided in him is: (aspirin) Aspirin should always avoided in the case of viral infections in children and adolescents. The incidence of Reye syndrome is increased if aspirin is given. This is especially true with varicella and influenza infections. The typical constellation of symptoms occurs during a bout of chickenpox and includes nausea, vomiting, headache, excitability, delirium, and combativeness with progression to coma. Since aspirin use has declined sharply, Reye syndrome has too. Professional/practice issues The nurse practitioner decides to study a group of patients who are trying to quit smoking. They all will be taking the same type of medication for 42 days to help them stop smoking. The patients have agreed to return to the clinic once weekly for the study’s duration. This type of study design is termed: (Cohort study) A cohort study describes an observational study that is prospective in nature, such as the case with this group of smokers. Cohort studies usually ask the question, “What will happen?” A case control study looks backward in time (retrospective). Case control studies usually ask the question, “What happened?” A controlled trial is an experimental study, not observational. The Framingham study of cardiovascular disease initiated in the early 1970s is an example of a: (Cohort study) The Framingham study was initiated in Framingham, MA in the early 1970s. The participants agreed to follow-up study (interviews and physical exam) every 2 years in a long-term study. This cohort study has examined what happens to disease over time. These are termed prospective studies because the events of interest occur after the study has begun. A nurse practitioner is taking care of a patient with health insurance and allergic complaints. The NP is aware that the patient is not using the prescribed allergy medication for her. Instead, the patient is giving the medication to her husband because he does not have insurance. What should the NP do? (Only prescribe the medication if the patient promises to use it) If the NP knowingly prescribes a medication for a patient other than the intended patient, the NP incurs medical liability and is deliberately diverting medications. This is illegal and constitutes theft in most states. The NP cannot legally continue to prescribe the medication if she knows that the intended patient is not the recipient of the medication. Certification: (validates competence) Certification is a process used to validate competence of an individual in an area of specialty. For example, certification exams are available for nurse practitioner graduates in the areas of family, pediatrics, women’s health, and adult-gerontological. While Medicare requires certification in order for a nurse practitioner to independently bill, it is not required for reimbursement by all organizations. Certification is not required by all states to practice as a nurse practitioner. Title protection is provided by licensure, not certification. The nurse practitioner is examining an older adult with dementia. She is noted to have bruises on her arms and on her posterior thoracic area. The nurse practitioner suspects elder abuse, but cannot be certain. The daughter of this older adult is her caregiver. The daughter is a patient of the nurse practitioner. What should the nurse practitioner do? (Report it to the appropriate authorities) Actual or suspected elder abuse is reportable in all 50 states, and healthcare providers are all mandatory reporters. Most older adults are abused by their caregivers, particularly when the elder has dementia. If the nurse practitioner asks the patient’s daughter if she is abusing her mother, it will likely result in a negative response by the daughter. Additionally, the daughter is not likely to seek this nurse practitioner’s help in the future because of fear of retribution. A nurse practitioner has worked for a large hospital as an RN. As a new nurse practitioner, she has developed a nurse practitioner managed clinic for hospital employees and is employed by the hospital. This nurse practitioner is described as a(n): (Intrapreneur) An intrapreneur is someone who is able to carve out a specialty role within an existing organization, healthcare setting, or business/industrial setting. An entrepreneur is someone who assumes the financial and personal risks of owning and operating a business. A nurse practitioner gives a patient 2 weeks of sample medications that will be taken once daily by the patient. The sample medications are packaged by the drug manufacturer. The nurse practitioner’s actions are an example of: (dispensing) Although definitions vary from state to state, a reasonable definition of dispensing is the legal right to select (as from stock) and/or label a medication to be self-administered by a patient. Most states allow registered nurses to dispense medications provided they are prepackaged. A registered nurse is not allowed to prescribe the medication being dispensed. Administering usually refers to the act of giving a single dose of a medication to a patient. Medication administration may be performed by nurses in all states. In a research study, the difference between the smallest and largest observation is the: (range) The range is the difference between the smallest and the largest observation in a group of values. What would be the study of choice to determine the cause of a cluster of adult leukemia cases found in an isolated area of a rural state? (Case control) A case control study would be ideal for discovering the cause of this situation. Case control asks the question “what happened”? It would identify subjects who have leukemia and would identify a control group of adults from the area who did not have leukemia. Both groups would be analyzed for characteristics or risk factors that were present in the “case” group but not the “control” group. This is an observational study. You are volunteering at a clinic that cares for homeless patients. What’s the most important aspect of a patient’s first visit? (Establish trust) The most important aspect of the initial visit is to establish trust. Many patients will not be willing to disclose a complete history to the examiner, especially one regarding alcohol or illegal drugs. A complete head-to-toe exam might be important, but most homeless patients are driven to care based on episodic illness. They will be interested in care for the problem that brought them in on the day of the exam. Additionally, resources may be limited, which would not allow for a complete head-to-toe exam on each patient, but instead, a focused visit. A nurse practitioner knows that she is HIV positive. She is employed in a private clinic and performs wellness exams on ambulatory adults. The nurse practitioner is: (is under no obligation to inform anyone) The nurse practitioner’s health information is protected health information. She is not obligated to inform her employer, patient, or state board of nursing as long as the performance of her job does not impose unnecessary risk to anyone. The Medicaid health program is: (funded by both state and federal governments) Medicaid is state run and specific to each state. The state programs are funded by a combination of state and federal funds. Most states have limits on the number of adult visits. Some states have no limits on visits for children. Participants generally do not pay premiums like Medicare recipients pay. The name given to subjects in a research study who do not have the disease or condition being studied, but who are included in the study for comparison are: (controls) Studied subjects are those members of a study who have a specific disease or condition of interest or who are receiving a specific treatment. Case series may refer to an observational study in which a group of patients with interesting characteristics are studied. Cross sectional is a type of observational study in which a particular characteristic is studied at one time rather than over time. Controls are commonly employed in many types of research studies. Mr. Bowers, a 97-year-old, is not able to make an informed decision due to mental incapacity. He does not have advanced directives, only a durable power of attorney (DPA). How should the nurse practitioner proceed? (Allow the DPA to make a decision based on the patient’s known values) An informed decision is determined by whether a patient is able to make and express personal preferences; comprehend risks, benefits, and implications; able to give reasons for alternatives; and has rational reasons for his choices. When an older adult is not able to make an informed decision, and a durable power of attorney is available, this makes the decision for direction of treatment. A durable power of attorney is an agent such as a trusted relative or friend. Standards of practice are established to: (regulate and control nurse practitioner practice) Standards of practice for all professionals (nurses, physicians, dentists, etc.) are established to regulate and control practice. They are intended to provide accountability for professionals and to help protect the public from unethical behavior and unsafe practice. Prescriptive authority: (varies from state to state) Prescriptive authority refers to the ability of a nurse practitioner to work and write prescriptions within the legal scope of practice in all 50 states. Although nurse practitioners are allowed to prescribe in all 50 states, there is great variability in how this occurs. Some states allow broader prescriptive authority, others much narrower authority. Who certifies nurse practitioners? (A nurse practitioner certifying body) The 2 certifying bodies for adult-gero and family nurse practitioners in the United States are American Nurses Credentialing Center (ANCC) and American Association of Nurse Practitioners (AANP). State boards of nursing grant a license to nurse practitioners in the state where they practice. Most states require certification in order to become licensed. A nurse practitioner examined a patient who had been bitten by her husband during an assault. There were numerous bite marks and lacerations on the patient’s forearms. The nurse practitioner sutured the lacerations, but this was contraindicated because of the highly infectious nature of human bites. The patient suffered no ill effects after suturing. How can this be described? (This is negligence) This is not malpractice. This is negligence. Negligence occurs when one fails to exercise the care that a reasonable person would exercise. Injury does not have to occur for negligence to occur. Human bites, known to be dirty bites with high probability of infection, should not be sutured. Malpractice is usually described as having multiple elements that all must be satisfied for malpractice to occur. There must be a duty, a breach of the duty, and a subsequent injury due to the breach. Comparison of performance is based on the standard of care delivered by nurse practitioners. Which study listed below is considered an experimental study? (Meta-analysis) Observational studies are studies in which subjects are observed. No intervention takes place with them. Examples of these are found in the first three choices. A meta-analysis takes published information from other studies and combines the information to arrive at a conclusion. Although a meta-analysis can use observational studies, these should be reported separately. A nurse practitioner has agreed to participate in the Medicare health insurance program. Medicare paid 80% of the charges billed for a clinic visit. What can be done about the other 20% that is owed? (The NP can bill the patient for a percentage of the remainder) The NP is a “participating” provider because he agreed to accept assignments. An assignment is an agreement between Medicare and the NP to accept the Medicare Approved Amount (MAA) as payment in full and not charge Medicare recipients a higher rate. The NP can bill the patient for a percentage of the remaining bill that was not paid by Medicare. The NP may opt out of participating. The NP can be reimbursed 100% if billed incident to the MD. A liability policy that pays claims only during the period that the policy is active is termed: (claims made policy) Liability insurance that covers the holder only during the time of the active policy is known as a claims made policy. This kind of policy is usually less expensive than other policies that will protect the policyholder against claims not known about at the end of the policy period. Tail coverage is more expensive than other policies because it protects the healthcare provider for an extended period of time after the incident occurs. An older adult male with moderately severe dementia presents with his caregiver daughter. His BMI is 18. His clothes have food stains on them and he looks as though he hasn’t been bathed in days. How should the nurse practitioner handle this? (The NP should report this as potential elder abuse) This patient presents as though he is being poorly cared for and mistreated. This occurs in about 3-8% of the adult population in the United States. There is no evidence that the patient has been physically abused, but he obviously suffers from neglect. This is a form of elder abuse, just as physical, sexual, psychological, or financial abuse is. Older adults with dementia often suffer abuse most frequently. A patient you are caring for in your clinic has Medicare Part B. What does this mean? (His medicare benefit covers outpatient services) Part B pays the examiner (NP, PA, MD, etc.). Part B of Medicare pays for outpatient care, ambulatory surgery services, X-rays, durable medical equipment, laboratory, and home health. Part B is an option that Medicare recipients can pay for with a monthly option. This charge is based on income. Since there is an initial copay, the federal government’s insurance plan may NOT pay for his visit to your clinic today. A patient you are examining in the clinic states that he has Medicare Part A only. What does this mean? (Only hospital visits are covered) Part A of Medicare refers to the hospital insurance program. There is no enrollment fee for most patients, and they are charged a monthly premium based on the number of eligible quarters they or their spouse contributed. This benefit also covers some skilled nursing facilities. A nurse practitioner examined a patient who had been injured by a cat. A 4-centimeter gaping laceration was present on the patient’s forearm. The nurse practitioner sutured the laceration. The patient subsequently became infected, needed hospital admission, and required IV antibiotics with incision and drainage. How can this situation be characterized? (The act of suturing this type of wound represents malpractice) This is malpractice. Cat bites, known to be dirty bites with high probability of infection, should not be sutured. Malpractice is usually described as having multiple elements that all must be satisfied for malpractice to occur. There must be a duty, a breach of the duty, and subsequent injury due to the breach. Comparison of performance is based on the standard of care delivered by nurse practitioners. A nurse practitioner’s scope of practice is influenced by a number of factors. Which one does not influence scope of practice? (Court of law) The scope of practice for nurse practitioners is established legally, ethically, and by boards of nursing and professional organizations. Scope of practice sets the boundaries and indicates what is permitted legally, etc. Scope of practice is not influenced by court of law. Scope of practice is determined by state statutes, state nursing boards, common practice in a locale, educational preparation, and others. Scope of practice can vary from state to state. An older adult was screened for colorectal cancer and had a positive screen. She went on to have a colonoscopy that was normal. She does not have colorectal cancer. The screen was a: (false positive) The screen was a false positive. Unfortunately, one of the hazards and great expenses of screening tests is the cost associated with false positives and false negatives. All screening tests have inherent costs associated with them. A nurse practitioner is working in a minor care clinic. She realizes that a patient with a minor laceration does not have insurance and is using his brother’s insurance information today so that his visit will be covered. How should she proceed? (She should let the clinic's business office know what is happening) The nurse practitioner cannot ignore the fact that this patient is attempting to defraud the clinic and insurance company in order to receive free care. If she does not let the business office know, she is a party to the fraud. She should let the business office know what is happening and have the patient present documents verifying that he is who he states that he is. If he cannot, he can still receive care if he is willing to pay for it. An alternative care site should be offered to him. A nurse practitioner is working in a minor care area of an emergency department. An illegal immigrant has a puncture wound caused by an unknown sharp object in a trash container. A dirty needle is suspected. The nurse practitioner: (should prescribe appropriate medications for HIV exposure even though the nurse practitioner knows the patient can’t afford them) The standard of care followed by the nurse practitioner should not depend on whether the patient has insurance or not. It is unethical to not properly inform the patient of risks he may have been exposed to from the puncture wound. Offering to buy the medications for the patient is noble but is not a sustainable practice. The nurse practitioner should prescribe the medications as for anyone with possible HIV exposure and refer to social services or a community referral agency that can help this patient acquire the appropriate medications. Licensure is: (used to establish a designated level of professional competence) Licensure is used by many states to protect the public and establish a minimal level of professional competence. Licensure and competence are two distinct recognitions and are conveyed by different organizations/bodies. Licensure and reimbursement are not usually related; however, reimbursement and certification are commonly related. A liability policy that pays claims even after the policy is no longer active is termed: (tail coverage) This is termed tail coverage because it extends beyond the time that the policy is active. This type of insurance is important for protection against claims that may come in after the healthcare provider has left the practice or retired. These are generally more expensive than claims-made policies. How would you create a therapeutic relationship with a patient? (Ask open-ended questions) A therapeutic relationship with a patient can be established in many ways. One way is to ask open-ended questions. This allows the patient to discuss what is most important to him; personal concerns may be vocalized by the patient. Telling the patient that he can trust you probably does little to establish trust. Actions that establish trust are more therapeutic than this statement. Touching the patient during the interview may be perceived as inappropriate by many patients. In contrast, touching the patient during the exam is different. Finally, telling the patient that you enjoyed taking care of him (if this were true) does little to establish trust. The research design that provides the strongest evidence for concluding causation is: (randomized controlled trials) A randomized clinical trial (RCT) is the epitome of all research designs. Subjects are randomly assigned to treatment groups. This type study provides the best evidence that the results were due to the intervention and not something else. A RCT is an experimental design, not an observational one. A nurse practitioner is volunteering in a homeless clinic to gain clinical experience. Which statement is true about this? (Malpractice insurance is needed by the nurse practitioner) Malpractice insurance is needed in any situation where patients are treated by a nurse practitioner. Some states have a Good Samaritan law that protects professional volunteers from being sued. Unless this is specifically provided by state law, a nurse practitioner should have professional liability insurance in the event the NP is sued. The legal authority to practice as a nurse practitioner in any state is determined by: (state legislatures) The authority to practice as a nurse practitioner is determined by each state’s legislature. Rules and regulations may be promulgated by state boards of nursing that reflect scope of practice of nurse practitioners specific to that state. Certification boards like ANCC and AANP “certify” that a nurse practitioner has met the requirements set by the certifying body. A nurse practitioner is working in a minor care area of an emergency department. A patient without insurance arrives with a puncture wound caused by an unknown sharp object in a trash container. A dirty needle is suspected. The nurse practitioner: (should prescribe a tetanus shot if needed and appropriate medications for HIV exposure even if he can’t afford them) The standard of care followed by the nurse practitioner should not depend on whether the patient has insurance or not. It is unethical to improperly inform the patient of risks he may have been exposed to from the puncture wound. Offering to buy the medications for the patient is noble but is not a sustainable practice. The nurse practitioner should prescribe the medications as for anyone with possible HIV exposure and refer to social services or a community services agency that can help this patient acquire the appropriate medications. A nurse practitioner (NP) works in an HIV exclusive practice. In talking with a patient, the NP learns that the patient’s sister lives next door to the NP. When the NP sees her neighbor (the patient’s sister), the NP states that she met her sister in the clinic today. The neighbor replies, “Don’t you work in an HIV clinic?” How can this situation be characterized? (This is a breach of confidentiality) This is a breach of the patient’s confidentiality. The neighbor’s sister is the NP’s patient. The NP is bound to confidentiality regarding protected health information for any of her patients. Even though the NP did not acknowledge that her sister was a patient, she breached patient confidentiality by telling the patient’s sister that she had met her in the clinic. This is different from telling her sister she met her at the grocery store. [Show More]
Last updated: 1 year ago
Preview 1 out of 74 pages
Instant download
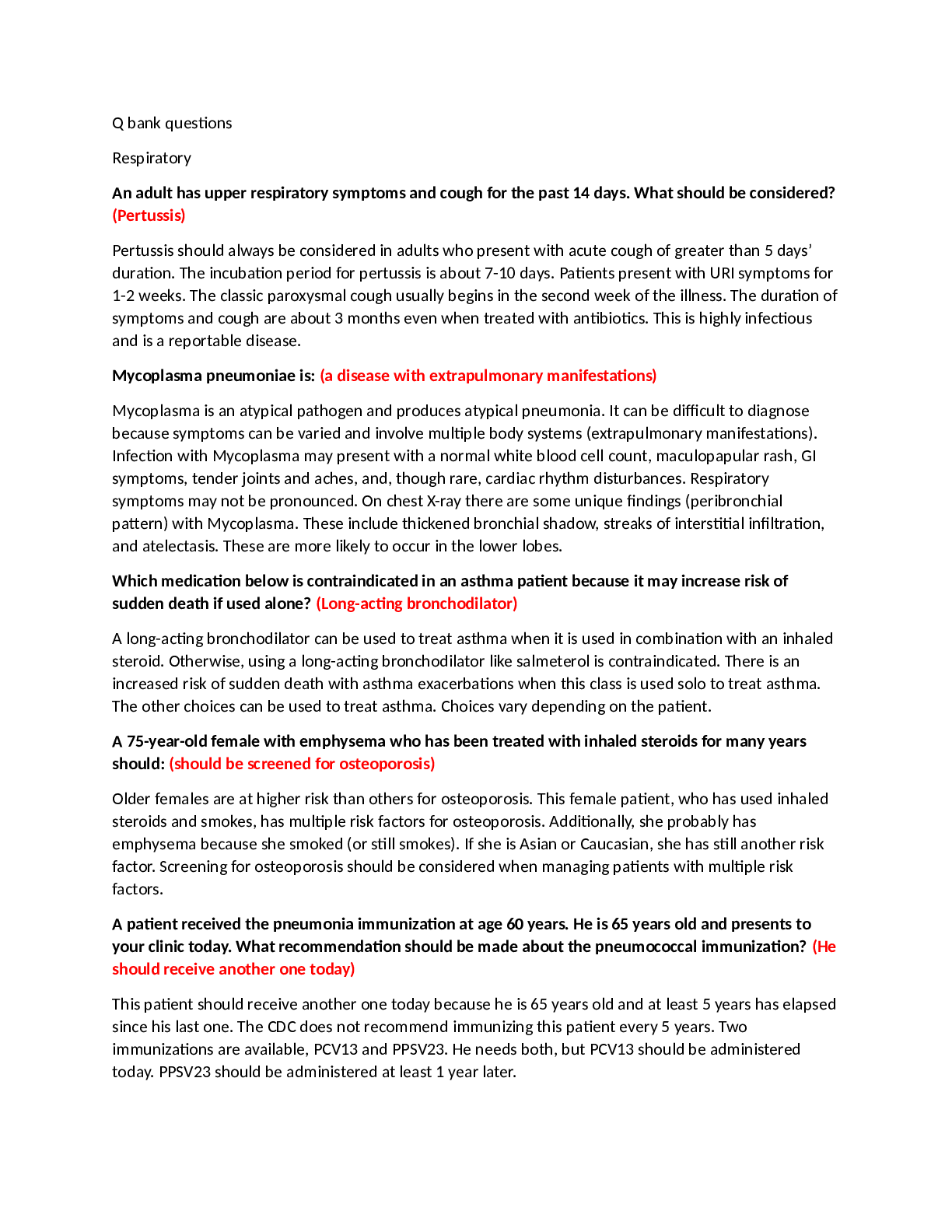
Instant download
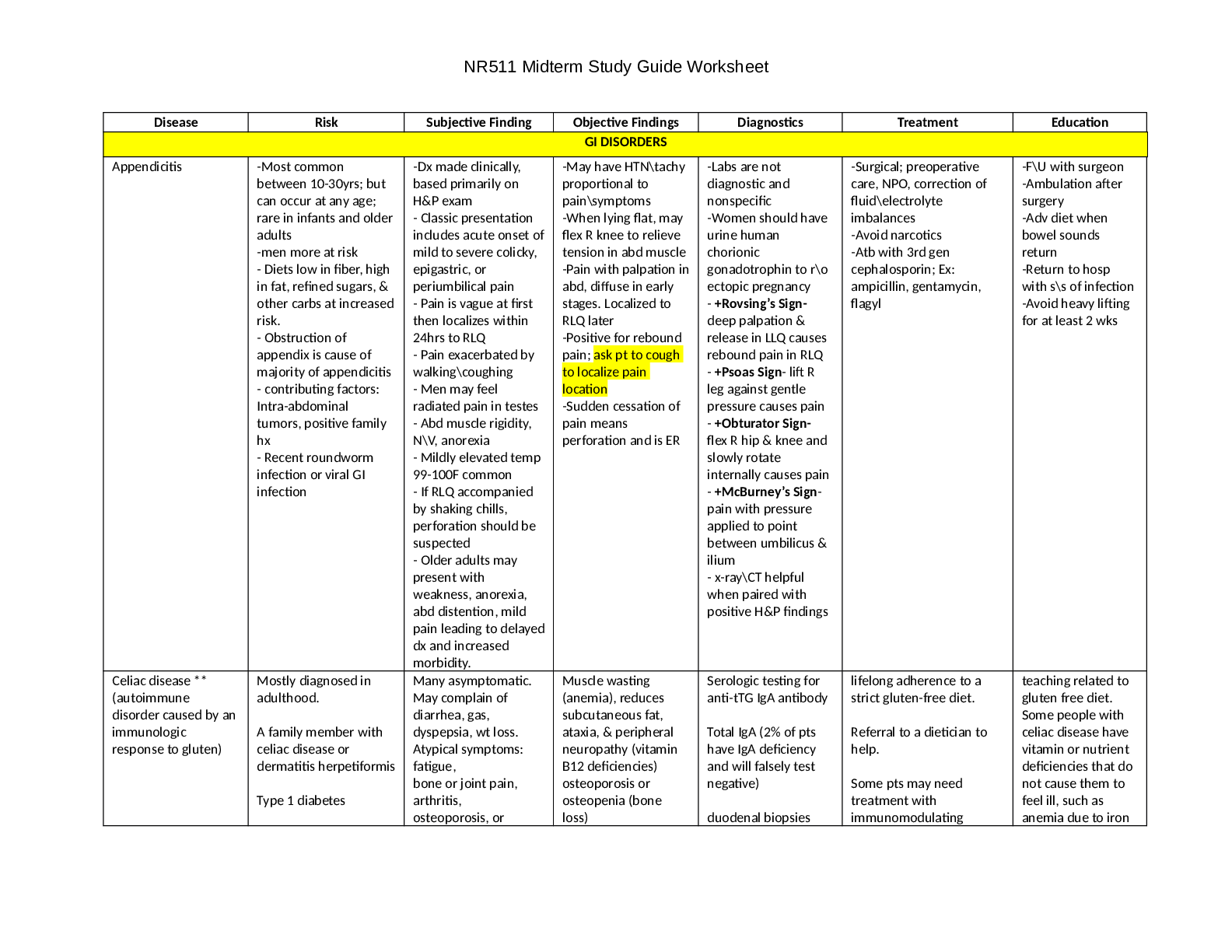
Reviews( 0 )
Document information
Connected school, study & course
About the document
Uploaded On
Dec 08, 2021
Number of pages
74
Written in

Additional information
This document has been written for:
Uploaded
Dec 08, 2021
Downloads
0
Views
156
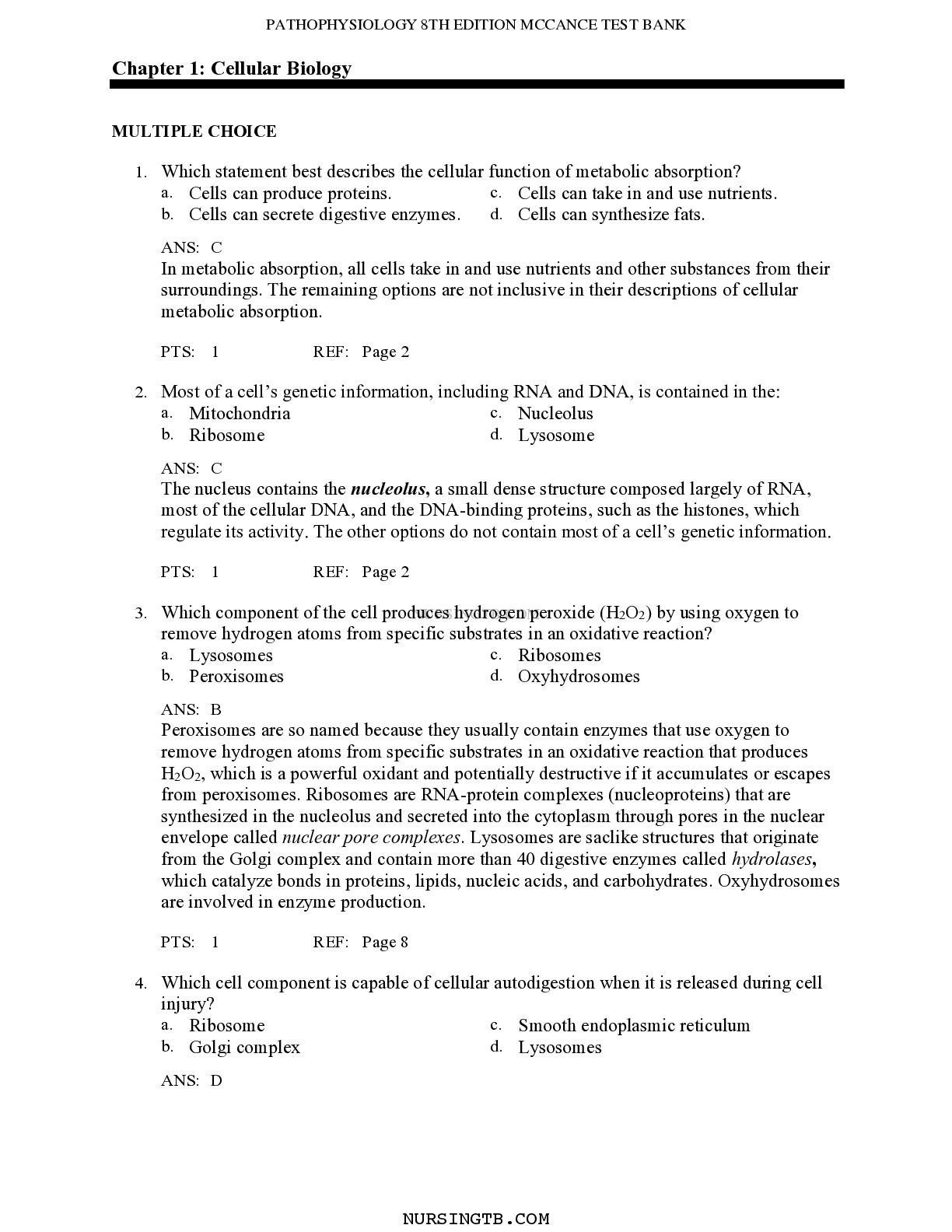

.png)


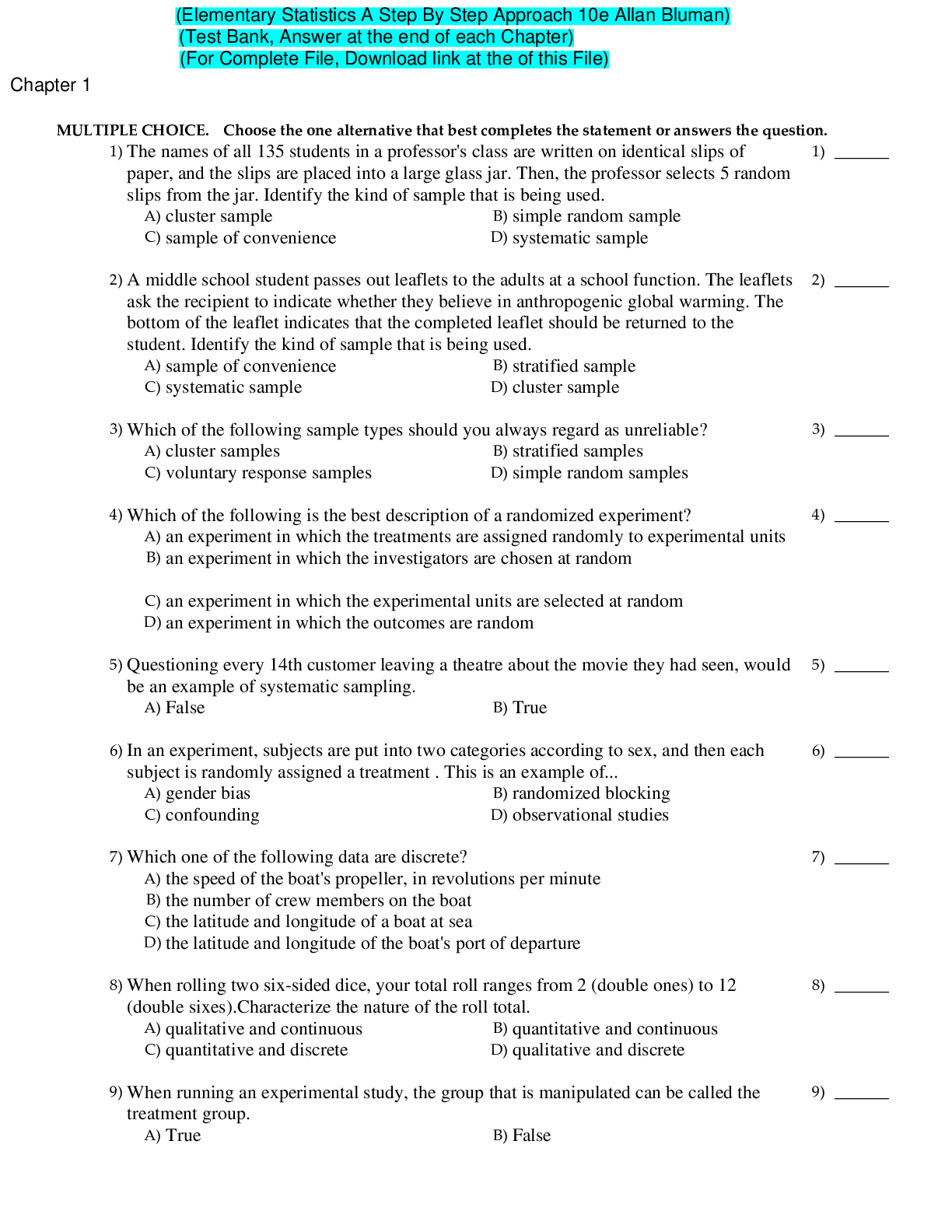
 Ken Leo, Jeffrey Knapp, Susan McGowan, John Sweeting (Test Bank).png)
